
Abstract
This article presents health information-seeking behaviour of immigrant women, their challenges in seeking health information and the potential socio-cultural factors influencing those challenges. It contributes to the field of information behaviour and helps in designing better information services for immigrants. Twelve semi-structured interviews were carried out with South-Asian immigrant women living in Finland. The study illustrates that participants seek physical and mental health information through family, friends, doctors and online sources. The main challenges in health information seeking are the lack of information about health services, fear from information seeking and sharing and not satisfied with information from the doctors in Finland. The potential socio-cultural factors are the cultural and language differences and the perception about the Finnish healthcare system and doctors’ behaviours. The study has strong practical implications for health centres and health professionals dealing with immigrants’ health matters in designing better health services and communication strategies for immigrants in Finland.
Keywords
1. Introduction
Immigrants often face significant difficulties when settling in a new country, such as adapting to a new culture, learning the language and navigating unfamiliar systems [1,2,3]. These challenges can make it hard for them to find stable housing, secure employment and build social networks [4]. In addition, immigrants also face barriers when seeking health information [5]. Language barriers, cultural differences and a lack of understanding of the local healthcare system can make it difficult for them to access reliable health information and make informed decisions about their health [4,6]. The growing immigrant population in Finland necessitates enhanced health and well-being services for these individuals and their families [7,8]. Promoting the health of immigrants and their access to healthcare services is one of the main goals of the Finnish Integration Plan [9]. Immigrants’ health is impacted by many factors, such as country of origin, reason for immigrating, age of immigration and the length of time spent in the host country [10]. Cultural differences, language barrier and lack of social networks are some major influencers for poor mental and physical health of immigrants in Finland [11]. Unemployment is one of the key challenges the immigrants face [12] and especially women immigrants are more vulnerable to unemployment challenges in Finland [13]. Unemployment results in various issues for immigrants, including economic hardship, loss of self-esteem and reduced social and leisure opportunities, leading to poor mental and physical health and diminished chances of integrating into the Finnish society [11,12,13]. These phenomena show that immigrants clearly need health information to improve their overall well-being in Finland. According to a survey about the health and well-being of immigrants in Finland, women immigrants feel the need for mental health services and general doctor’s reception services more often than men in Finland [9]. Immigrants face certain challenges in accessing health information in Finland due to some flaws in the Finnish healthcare system, such as long queues for treatment, high customer fees and lack of a common language with a health professional as key challenges in accessing the healthcare services in Finland [14]. In addition, immigrants struggle with accessing health information due to a lack of knowledge about service locations, their functions, operational procedures and the unavailability of interpreters [8,10,11].
Health information-seeking behaviour is the way in which individuals go about obtaining information about their health, health promotion activities and risks to one’s health and illness [12]. A growing number of scholars have examined the health information-seeking behaviour of immigrants, refugees and asylum-seekers in the past [8,13,6,15]. Very few scholars, however, have examined the health information-seeking behaviour of immigrant women [16,17,18]. These previous studies lack in explaining the challenges women might face in health information-seeking process from a socio-cultural perspective and how these challenges may help/hinder the integration of women in the host society. Socio-cultural factors such as language, cultural backgrounds, cultural beliefs, religious beliefs, social values and traditional communication styles have an impact on health information-seeking behaviour of immigrants [8,18,19,20]. Thus, this study aims to understand the health information-seeking behaviour of South-Asian immigrant women in Finland – from the socio-cultural perspective. It examines the challenges they might face in seeking health information and how these challenges may help/hinder the integration of immigrant women into the Finnish host society. The study intends to answer the following research questions:
RQ1. What kind of health information do they seek and how?
RQ2. Are there any challenges they face during the health information-seeking process? If yes, what are those?
RQ3. What and how do socio-cultural factors influence the challenges in the health information-seeking process?
2. Conceptual framework
This article uses the concept of everyday life information seeking (ELIS) by Savolainen (1995) to understand the health information-seeking behaviour of immigrant women in Finland [21]. In Library and Information Science (LIS), there are certain theories and models that explain ELIS in different contexts such as Dervin’s Sense-Making Theory [22], Interest-Concern-Caring [23], ELIS in the context of Small World [24] and information ground [25]. However, this particular paper focuses on the concept of ELIS by Savolainen (1995) because it emphasises problem-specific information seeking [21], where information is sought to address concrete, everyday issues. For immigrant women, health-related information is often sought in response to immediate, practical problems – such as understanding a medical condition, finding healthcare services or coping with language barriers. Savolainen (1995) introduced the concept of ELIS, emphasising that it refers to information seeking that is problem-specific and arises in the context of everyday life situations [26]. According to Savolainen, people engage in information-seeking behaviours to address specific, practical problems they encounter in daily living. These problems might range from solving a personal dilemma to obtaining information for decision-making. In the case of immigrants, they usually tend to have problem-specific information-seeking behaviour in their everyday life context, for instance, seeking a job, health problems, looking for housing, education or learning a language [1,27,28]. The concept emphasises that information-seeking behaviour is influenced by both situational and contextual factors, which are shaped by an individual’s life circumstances, social roles and cultural environment [29,15]. Various studies have investigated the ELIS behaviour of immigrants in the past and found that immigrants rely on different information sources to meet their needs or to solve the problems and face various challenges in seeking everyday life information [30,31,32]. In Martzoukou and Burnett’s (2018) study about Syrian refugee families in Scotland, it is examined that everyday life information about various matters such as health and domestic issues, well-being and community engagement is required, and language barrier is the huge challenge for accessing the information [33]. Thus, the main information need revolved around the learning of English language to meet everyday life information needs [33]. Khoir et al. [30] studied the everyday information behaviour of Asian immigrants in South Australia and found the difference in information needs of newcomers and longer-established immigrant. The newcomers’ information needs are referred to as personal, general and official needs, while the longer-established information needs are more about full participation. The popular information sources for immigrants were the Internet, mass media, people and formal organisations [30]. However, by focusing on ELIS, this article identifies the kind of health information they seek and how, and whether there are any challenges in seeking everyday life information in health matters.
3. Literature review
3.1. Health information-seeking behaviour of immigrants
Health information-seeking behaviour refers to the methods by which individuals consciously search diverse resources for information regarding their health, the risk, diseases and manners of health preservation [11,21]. Many previous studies have focused on health information-seeking behaviour of different groups of people such as cancer patients [26,22], students [23], teachers [24], seniors [25], adults [15] and athletes [27]. This particular study focuses on health information-seeking behaviour of immigrant women in Finland; hence, it is worth mentioning previous studies focusing on immigrants’ health information-seeking behaviour. Health information is one of the main concerns of immigrants upon arriving in a new host country [34]. Immigrants require health-related information for themselves and their families, including details on accessing medical services in the city and understanding the procedures for using these services in the host country [19,35]. In a study on health information-seeking behaviours of immigrants, asylum-seekers and refugees in Europe, it is shown that information about mental health, sexual health and HIV, dental, pregnancy and childbirth services is needed [19]. Immigrants also seek information about diet and nutrition, gastrointestinal issues, injuries, musculoskeletal problems and infections [36,37]. Immigrants need health-related information to manage the cultural shock and stress they get from a new place [38]. The psychological distress from leaving their home countries forces immigrants to seek health-related information for their mental well-being [19]. Some studies show that immigrant women need specific health-related information such as stress-management, pregnancy, childbirth, menstrual issues, physiotherapy and cardiovascular diseases [19,39,40,41]. Particularly about South-Asian immigrants, there are few studies focusing on health information seeking of this particular group, such as it is noticed that South-Asian immigrants were less probably to have used the Internet when compared to whites to seek health information in America [42]. Low-income South-Asian immigrants face barriers in accessing family health information due to lack of computer and Internet access in Canada, while those university going were more probably to use the Internet for health information seeking [43]. Similarly, in another study, the Indian immigrants preferred complementary and alternative medicines and home remedies to address their health needs rather than relying on health services [44]. In a study about health-seeking behaviour of Nepalese immigrants in Japan, it was found that the Internet was the most common source of information for those who had a high education level [45]. In another study, Bangladeshi migrant workers face difficulties in accessing information on health services in Malaysia due to lack of medical insurances and not having proper legal statuses in the country [46]. In a systematic review, it is noticed that Pakistani immigrants residing in high-income countries prefer to use traditional medicines as a first-line approach to cure illness due to cultural beliefs [47]. This previous literature shows that South-Asian immigrants, in general, have different information experiences to seek health information and face certain barriers in accessing the information in different countries [48,49]. However, the influence of socio-cultural factors on health information-seeking behaviour of South-Asian immigrants is not much focused on previous studies [47]. Therefore, there is a need for detailed understanding of what and how health information-seeking behaviour of this particular group of immigrants get influenced by certain socio-cultural factors in a new host country.
3.2. Sources of health information seeking for immigrants
Health information-seeking behaviour is an action taken to fulfil certain health information needs through certain sources [50]. The Internet has become a popular source of obtaining health information and to overcome obstacles in healthcare experiences for immigrants in different countries [51]. Immigrants face linguistic barriers in obtaining health information and healthcare services in a new country which leads them to use the Internet as an alternative [52]. Immigrants can use their native language or the language of the host country to search for health information [52]. Some studies show that immigrants use general websites such as general portal websites, search engines and country’s health-specific websites for health information [53]. Social media is considered the most popular source of health information among many people including immigrants [37]. For instance, a study on health information seeking by Pakistani female patients with chronic conditions reveals that they frequently use Internet sources and social networking sites like WhatsApp, YouTube, Twitter and Facebook to find information on hypertension and diabetes-related issues [54]. The main advantages for online health information seeking have been found to include easy access, social support, the potential of connections and anonymousness [53]. Few studies reveal that women seek online health information due to various benefits such as timeliness, interactivity, availability and vast amounts of information [55,56]. However, there is a need to study women immigrants’ usage of online health information sources further and the motivations behind using those sources. The challenges associated with certain health information sources and the consequences of those challenges on their integration process are also an interesting perspective to study. In this way, we can understand the needs for improvement in health information services for immigrant women which previous studies lack.
Besides the use of the Internet and social media, studies have found that immigrants prefer to use the healthcare professionals, traditional media and personal networks as their primary source of health information [57]. Family, friends, relatives and co-workers are a source of health information for some immigrants, especially Asian people who trust informal sources more than other sources [6,19].
3.3. Factors influencing health information-seeking behaviour of immigrants
Studies show that several factors such as migration status, educational background, economic situation, length of residency and socio-cultural factors have significant influence on the immigrants’ health information-seeking behaviour [58]. Socio-cultural factors refer to language, cultural norms, traditional values, thoughts and behaviours [59]. Language has a strong influence on health information seeking of immigrants [20]. It is noticed that immigrants seek health information mostly in their own national language. For example, in a study about health information-seeking behaviours of Korean immigrants in America, language has a high influence on choosing the information source, for example, immigrants find magazines and newspapers published in Korean language more helpful than other languages [60]. Furthermore, cultural background effects on beliefs about medication, for example, people with Asian cultural background believe in taking medication more often that should be avoided otherwise [61]. Past experience of taking medication and some religious beliefs are associated with the Asians’ health practices [61]. In another study, it is noticed that Pakistani immigrant mothers rely on self-medication and bring medicines from Pakistan to treat their health problems while living in New Zealand. Because they trust their own medication culture and find the medicines readily available on the counter in most of the pharmacies in Pakistan. [62]. Thus, these cultural beliefs about health and medication have an impact on information-seeking behaviour of immigrants. Furthermore, literacy and education also have an influence on the information-seeking behaviour of immigrants [63,64]. For example, studies have found that highly educated and literate immigrants are more probably to use the Internet as a source of health information and are more aware of avoiding misinformation [51]. In spite of several studies explaining about the factors influencing the immigrants’ health information-seeking behaviour, there is a lack of explanation on how these socio-cultural factors impact on health information-seeking behaviour of women immigrants. This study specifically intends to explore the potential socio-cultural factors influencing the South-Asian women immigrants in Finland and how these factors encourage/discourage the better integration into the host society.
3.4. Challenges in health information seeking of immigrants
Immigrants who arrive in a new country face various challenges in accessing different health-related information due to language barriers, cultural differences, lack of social networks and socio-economic situations [19,53]. Long wait times, lack of appointments, delayed access to the healthcare system, difficulties in accessing specialists, and diagnostic and acute care services are some challenges immigrants face during integration in a new country [65]. Lack of information about the healthcare services and how to navigate those services is a major challenge for immigrants [66]. The unfamiliarity with the new healthcare system of the host country is causing confusion and frustration for immigrants, and they often misunderstand the system and face difficulties in accessing needful information [6,65]. Immigrants are more probably to have a poor therapeutic relationship with their providers due to language difficulties, lack of trust in the services and experience of racism and discrimination [67,68]. The patient–doctor communication relationship is also seen as disturbing for immigrants in some studies, for example, rushed appointments, inadequately explained treatment plan, inadequately explained test results, lack of interpreters, and confidentiality and privacy concerns are mentioned as negative experiences resulting in poor integration into the host society [47,69]. Moreover, the challenge of overusing the Internet and social media for health information seeking may lead to several problems such as difficulties in navigating the right information, information overload, disorganised information, misinformation, too much negative and depressing information, overly technical medical language, lack of user friendliness and quality of online health information [53,63]. Studies show the risk of inaccurate, misleading, incomplete and dangerous information on the Internet may lead to hazardous health decisions [70,71].
Some studies show that women immigrants face more socio-cultural barriers in accessing health information than men [32,55]. For example, a study focused on health-seeking behaviour of Afghan women immigrants found that Afghan women are at high risk of poor physical and mental health because of difficulties in accessing the information, dependence on their husbands and cultural taboo [17]. However, this study adds to this literature by studying the health information-seeking behaviour of South-Asian immigrant women living in Finland which is a significant group of minorities in the country.
4. Context of the study
4.1. Healthcare system and immigrants’ situation in Finland
In Finland, the public healthcare is universal and taxation-based, mainly provided by municipality-arranged healthcare centres. Many private enterprises and non-governmental organisations also provide health services in Finland. The immigrants who hold resident permits in Finland are entitled to the same health services and benefits as the Finnish citizens [72]. According to the Finnish Health Care Act, a patient’s need for non-emergency treatment in public healthcare must be evaluated by healthcare professionals within 3 days of initial contact, and this is usually made by nurses [73]. For outpatient care in primary healthcare for non-urgent examinations is generally 3 months for both physical and mental health treatments in Finland. Waiting times to see specialists are even longer from 3 to 6 months [74]. According to the Finnish Institute for Health and Welfare, long wait times are a special challenge in the Finnish healthcare system and are associated with employee shortage in healthcare [74]. The institute reported that Finland has fewer doctors than the European Union (EU) average but more nurses. Longer waiting times are leading to problems of poor access to health services for many people in Finland including Finns, immigrants, refugees and asylum-seekers [75].
The number of immigrants has increased in Finland in recent years. In 2022, immigration increased Finland’s population by almost 35,000, and in 2023, by well over 50,000 [76]. According to Finnish Statistics, the number of South-Asian immigrant women from Pakistan, India, Bangladesh and Nepal has increased from 2019 till 2022. In 2019, the number of immigrant women was Pakistan (174), India (614), Bangladesh (162) and Nepal (196), which increased in 2022 to Pakistan (358), India (1,228), Bangladesh (415) and Nepal (349) [76]. According to the Finnish Institute of Health and Welfare, the health and well-being of immigrants are ensured at different stages of immigration and integration [77]. In Finland, there is a special rehabilitation service department which provides rehabilitation services to immigrants and their children and families such as mental health, treatment of disabilities or finding employment [77]. It is noticed that working-age immigrants generally have health challenges such as inability to cope, poor mental and physical health and difficulty in committing to studies or work, due to many reasons of being away from family, lack of social networks or unemployment [77]. In spite of the health challenges, immigrants may use rehabilitation services less often than the average citizen. There are few studies in Finland which show that many rehabilitation services such as psychological treatments, sports and fitness services and other mental health treatments are not known to immigrants [78,79]. However, these studies lack a detailed explanation of why immigrants underuse the mental health services in Finland. There might be socio-cultural factors, language barriers, a lack of information about the services or personal reasons behind not/less using the mental health services.
Some factors such as unemployment and discrimination lead to poor mental health conditions for immigrants in Finland [80]. For example, women immigrants are more vulnerable to unemployment challenges in Finland [13]. According to an Organisation for Economic Co-operation and Development (OECD) report on ‘Faces of joblessness in Finland’, poor physical or mental health can lead to poor work performances and may lead to job loss, and at the same time, job loss and longer unemployment periods can lead to health concerns. Hence, a positive association between unemployment and health is common in many countries including Finland [81]. Moreover, discrimination towards immigrants is noticed in the Finnish healthcare system to some extent. A recent Finnish, YLE news report revealed medical staff using racist and discriminatory language for non-white skin immigrants and Muslim foreigner patients in a Facebook group – which shows what is experienced on a daily basis in hospitals and health centres in real life [82]. According to YLE’s informants, it is very common that the medical staff is of the opinion that dark-skinned people are more dramatic by nature and exaggerate the extent of their pain than native Finns [82].
5. Methodology
In this study, a semi-structured interview approach is employed as a qualitative method. Given the complexities associated with human behaviour, especially within migrant communities, utilising this interview technique is suggested to gain deeper insights into the perspectives, behaviours and social environments of the research participants [83].
5.1. Participants of the study
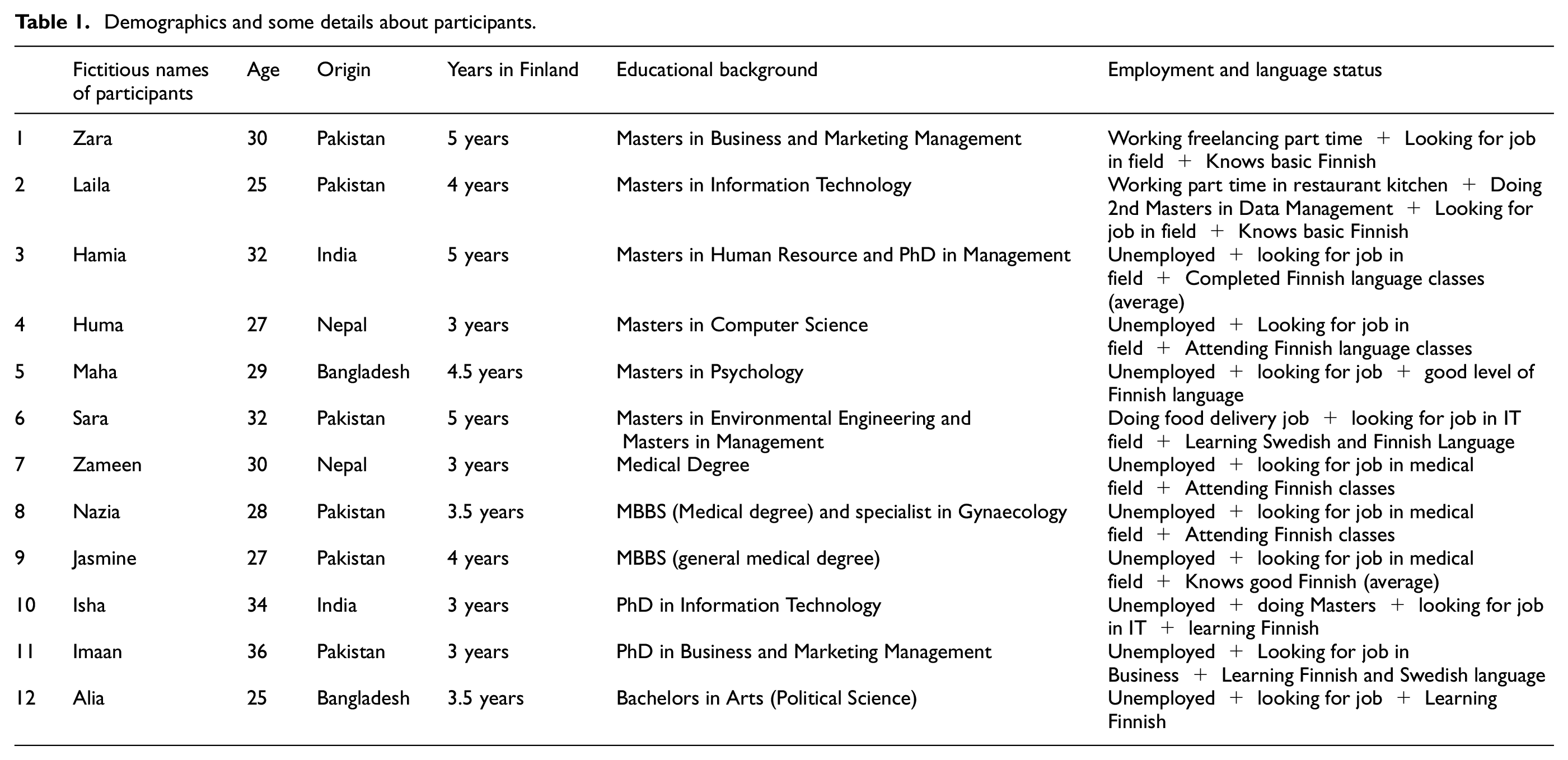
The study involves interviewing 12 adult immigrant women aged 25 to 36 years from South-Asian countries (comprising 6 from Pakistan, 2 from India, 2 from Bangladesh and 2 from Nepal) who have resided in Finland for a minimum of 3 to 5 years. The study particularly focuses on South-Asian immigrants because of the increasing number of immigrants coming to study, work and rejoin the families in Finland from Pakistan, India, Nepal and Bangladesh and this growing community can be a good representation of different cultures in the society. Recently, Finland experienced a historic high number of immigrants moved to Finland in 2023 – due to the war in Ukraine and many other factors. According to the Statistics Finland data, 71,918 individuals have migrated to the country in 2023 [84]. This number breaks the record of the year 2022 (21,920 individuals) [85]. Figure 1 shows the increasing trend of immigration to Finland during 2013–2022. Immigrants from several Asian countries (India, Bangladesh, China, Sri Lanka, Philippines) are a noticeable group of people who migrated to Finland in 2023 for family reunion, study and work purposes [84]. Due to the growing interest in the Finnish Education system, Finland has received a significant increase in international students and their families [86]. Recently, in late 2022, most of the study applications were submitted by citizens of India, Pakistan, Bangladesh, Sri Lanka and China [87]. The trend of immigrants from certain South-Asian countries (i.e. India, Pakistan, Bangladesh, Nepal) has increased in the last few years. Figure 2 shows the trend of increasing numbers of immigrants from certain South-Asian countries (i.e. India, Pakistan, Bangladesh and Nepal).
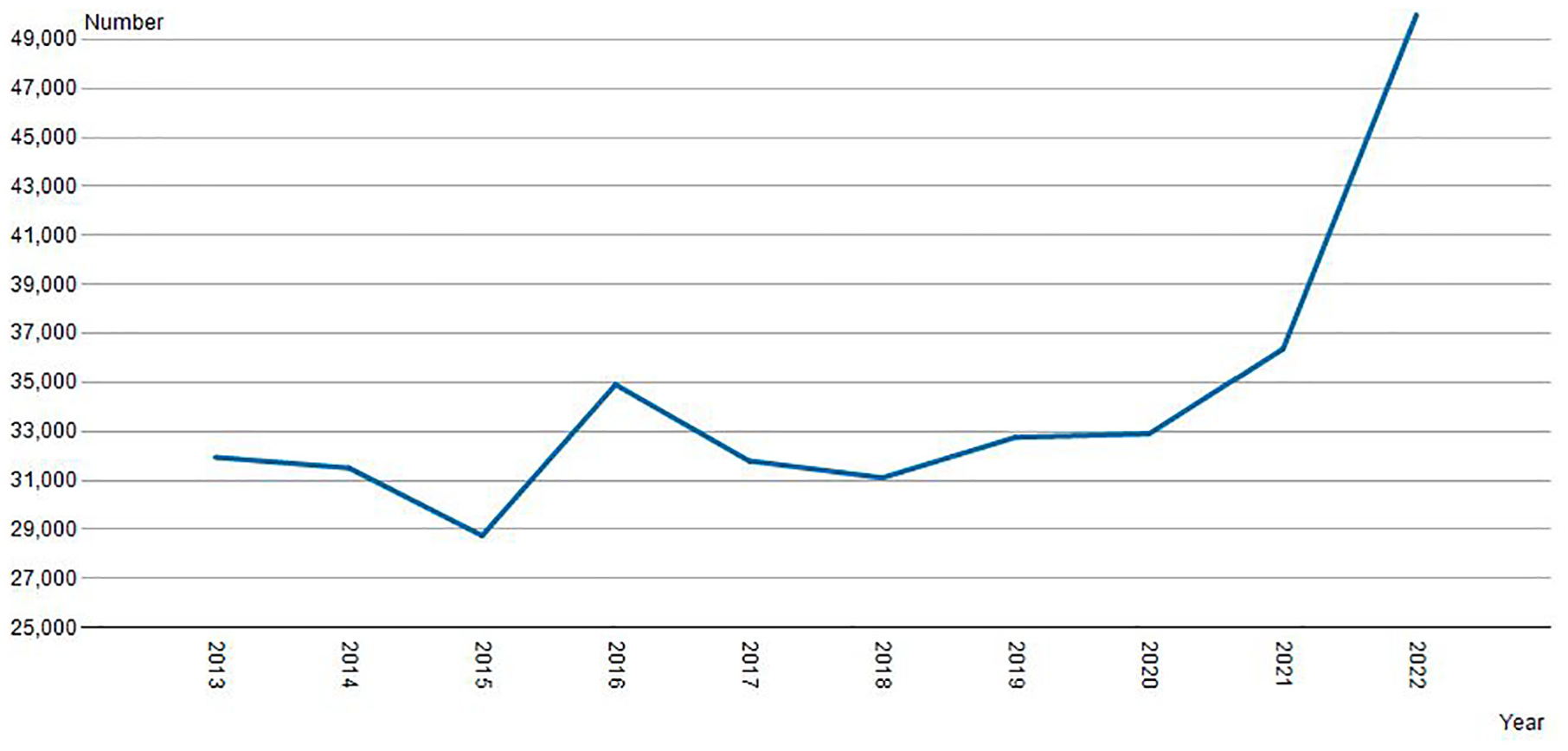
Immigration to Finland 2013–2022 [87].
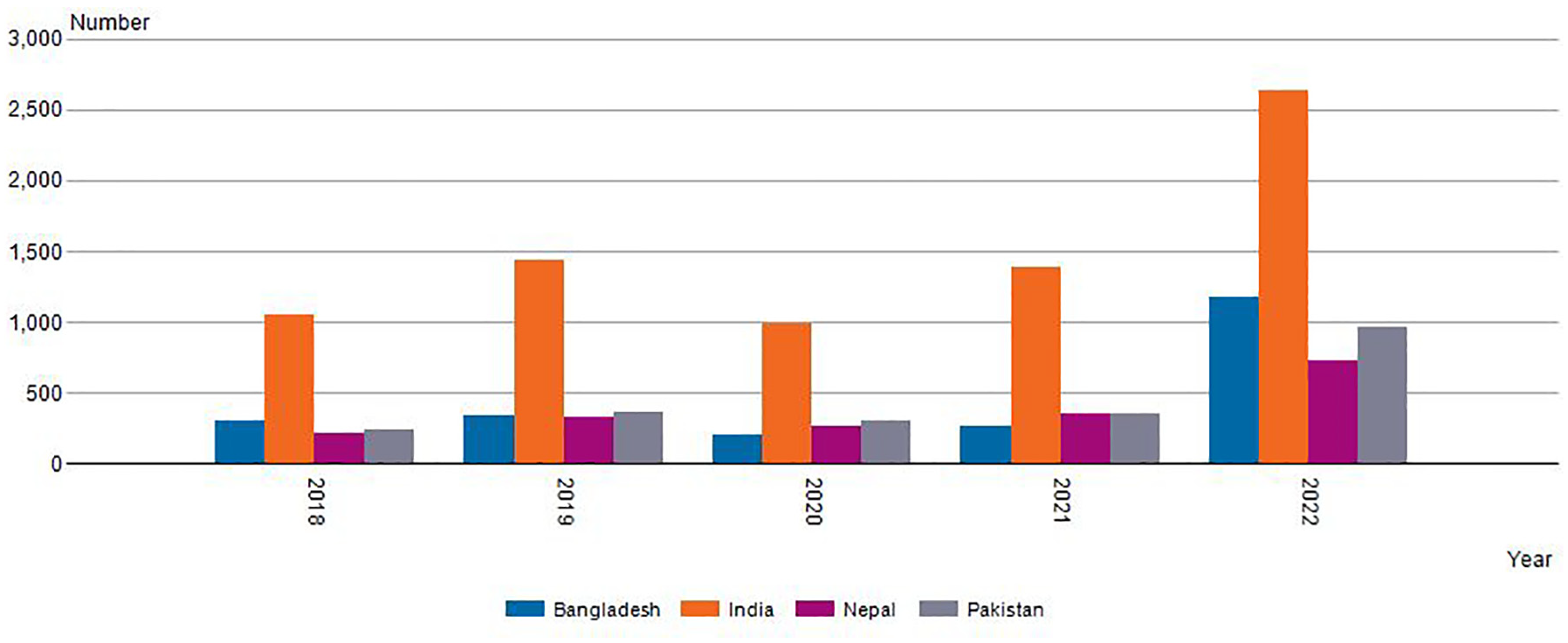
South-Asian immigrants in Finland 2019–2022, statistics from the Finnish Immigration Service [87].
South-Asian immigrants, like any group, are diverse, and cultural norms can vary significantly depending on factors such as country of origin, religion, region and socio-economic background [88]. However, there are several common cultural norms that tend to be shared among South-Asian immigrants (Pakistan, India, Bangladesh, Nepal) such as people understand Hindi almost in all four countries while they also speak Urdu, Bengali and Nepali languages. Most of the cultural festivals such as Diwali, Eid and Holi are celebrated in these countries which show the cultural heritage [89]. There are many similarities in traditional cuisine, art, music, social customs, etiquette and family values in these four South-Asian countries [90]. Moreover, looking at the socialisation patterns, South-Asian people are often characterised as collectivist, meaning they prioritise group harmony, interdependence and social cohesion [91]. Studies show that, in a collectivist culture, individuals may rely heavily on their social networks for information-seeking purposes, seeking advice, recommendations and referrals from trusted family members, friends or community members [92,93]. Similarly, looking at the communication style of South-Asian people, they tend to be more indirect and nuanced, where messages may be conveyed subtly or implicitly. Non-verbal communication such as gestures, facial expressions and body language can vary between east and west [94,95]. Information may be shared through interpersonal channels rather than formal sources in a collectivist culture [96]. These cultures may prefer face-to-face interaction than the virtual ones for comfortability and trust issues [97]. Moreover, the role of gender is also associated with the cultural background of people. In South-Asian cultures, women often face expectations and responsibilities that are influenced by traditional gender roles, cultural norms and societal expectations [98,99]. While these expectations can vary based on factors such as region, religion and socio-economic status, there are some common themes in the roles assigned to women in these cultures such as household duties, taking care of family and extended family, childcare and preserving cultural traditions [90,99].
The selection criteria for the participant in this study were that the participants must be immigrant women from any country, with the legal immigrant status living in any city of Finland. Participants must have been living in Finland for the minimum of 3 or more years, in order to get the integration experiences faced in the last 3 or more years living in Finland. In terms of age, adults above 18 years were included in the selection criteria for interviews.
All participants entered Finland via the spousal route, either accompanying their husbands or joining them shortly after their arrival. Some participants migrated to Finland with their children, while others gave birth to children after arriving in the country. All participants hold resident permits based on spousal permits, granting them the right to study and work. They are at various stages of Finland’s integration plan. The study population exhibits diversity in terms of occupation and educational background, all possessing strong educational backgrounds and proficient command of English alongside their native languages. Upon arrival, most began learning Finnish through courses offered by the Employment office (TE-office) designed for foreigners seeking full-time Finnish language instruction. Table 1 shows some demographic details about the participants where their original names are substituted with fictitious names to keep their identity anonymous.
Demographics and some details about participants.
5.2. Data collection
The author conducted semi-structured interviews, including pilot and expert interviews. In April 2023, two pilot interviews were conducted with immigrant women from Pakistan and India. The aim of these pilot interviews was to assess the suitability of the subjects for the interview questions. These pilot interviews helped in designing the interview questions about health information seeking of participants in Finland. Some of the interview questions were related to the theme such as challenges in health information seeking, sources for health information and kinds of health information needs. A total of 20 women were contacted through convenience sampling, and 12, comprising 2 from the pilot group and 10 new participants, agreed to participate voluntarily. Interviews are conducted face-to-face. English was used as the language of interviews, as all participants were proficient in communicating in English.
The author initiated interviews using convenience sampling, as it offered an efficient and straightforward method of participant recruitment. Being actively involved in the Pakistani Women Association within the city facilitated access to volunteers from Pakistan. In addition, personal connections with immigrant women from Bangladesh, India and Nepal, formed during previous employment, enabled access to volunteers from these South-Asian countries for interviews. Cultural and linguistic similarities, as well as shared gender, were helpful factors in engaging participants. For instance, the author, herself an immigrant woman originally from Pakistan residing in Finland, possesses fluency in Urdu, the mother tongue of Pakistani women, and understands Hindi, commonly spoken by individuals from India, Nepal and Bangladesh. The author acknowledges the potential influence of her personal background on the research but employs self-reflection to manage her positionality as an outsider.
5.3. Data analysis
The data analysis follows the four stages outlined by [100]. (1) The initial stage involved becoming acquainted with the data and making detailed notes. (2) After that initial codes were generated to identify themes such as codes related to the health information-seeking process and challenges in health information seeking. (3) Then, the codes were combined into the potential themes, for example, language barrier, cultural differences, Finnish healthcare system and doctors’ behaviours were collected under the information challenges. Similarly, all experiences related to sources of health information seeking are collected under the information sources theme. Some sources are mentioned such as family, friends, Internet and social media. (4) Ultimately, the themes underwent a thorough examination in connection with the complete data set, leading to the finalisation of themes. Subsequently, all themes were presented in the final phase as part of the findings, with Nvivo12 utilised in the comprehensive analysis.
5.4. Limitations of the study method
The sample size of this article consists of 12 participants that may limit the generalisability of the findings. The sample size of 12 participants raises some important considerations. While this sample size may not allow for generalisability in a statistical sense, it is not uncommon in qualitative research, particularly when the focus is on depth rather than breadth. Qualitative studies typically aim to achieve rich, contextualised insights rather than generalising findings to a larger population [100]. Therefore, the small sample size can be justified by the depth of data it provides. Twelve participants can offer a detailed understanding of the complexities and variations in information-seeking behaviours, particularly if the participants are chosen based on specific criteria that ensure diversity in their experiences and perspectives.
The study is conducted with the help of convenience sampling, which means that the study is able to reach only a limited population of immigrant and refugee women living in certain parts of Finland and Sweden, and therefore, the study is not generalisable to the larger population of immigrants and refugees.
5.5. Ethical considerations
The research adheres to the ethical guidelines established by the Finnish National Board on Research Integrity, which align with broader EU standards. The author obtained approval from the Research Ethics Board at Åbo Akademi University, Finland, following all research protocols. Participation was entirely voluntary, with participants provided comprehensive information about the study before interviews and asked to sign a consent form. The interview guide was meticulously crafted to avoid asking any invasive questions regarding participants’ cultural values or backgrounds.
6. Findings
6.1. Health information-seeking behaviour
This section exhibits the health information-seeking behaviour of participants by mentioning what kinds of information they seek and how. According to the findings, the kinds of health information seeking can be categorised in two main categories: (1) information related to physical well-being and (2) information related to mental well-being – during the participants’ integration process in Finland. Each category also explains how participants seek particular information.
6.1.1. Information related to physical well-being
The first main kind of health information seeking occurs among participants is about physical well-being during their integration process in Finland. According to the participants, physical health is somehow associated with mental health, for example, one participant, Hamia, mentioned that she got stress-belly – after living in Finland for four years – due to a longer period of stress about different matters including finding a job and learning Finnish language. She started searching for information about stress-belly such as What causes stress-belly? How to lose particular fat? What are the diet and exercise routine for fat reduction? The immediate source of searching for this information was YouTube and Instagram for Hamia. She found YouTube videos useful because the videos were in Hindi language which she understood well and the YouTubers were from India, the same origin as Hamia, which made her feel that they have the same physical pattern as her. Similarly, another participant mentioned ‘I gained body weight within two years of coming to Finland. I did not know the reason because I generally eat healthy. I went to the doctor and she said that it may be because of stress and sleeping disorders’ (Jasmine). She searched on Google and read many health blogs about weight loss, stress management, exercise and diet. She also searched on YouTube about exercises for beginners and diet plans for weight loss. She mentioned that her stress was mainly related to the cultural shock and pressure of applying for hundreds of jobs and receiving negative responses from employers. Similarly, Sara shared her experience when she had a miscarriage a year ago due to high levels of stress from the hectic routine at her previous workplace and the eagerness to change her job. She started seeking information about post-miscarriage care and precautions during her next pregnancy. She consulted her healthcare doctor in Finland in person and also watched videos on YouTube.
Some participants searched for information about how to start an active lifestyle such as joining a gym, yoga, swimming or sports in the city. They consulted other women in the WhatsApp group of Indian women in Turku and on Facebook groups of general immigrant women in Turku about any available opportunities to join gym, yoga or other sports. They feel comfortable in communicating with other women through chatting on these social media channels. Matters regarding womens’ sexual health including period problems, hormonal imbalance and family planning are also searched online by the participants.
6.1.2. Information related to mental well-being
The second important kind of health information seeking is regarding the mental well-being of participants during the integration process. The mental health of participants is impacted by the stress related to many different aspects such as coping with a new culture, learning a new language, lack of social network and finding a job. During the interviews, it was clear to notice that participants are vulnerable to migration-related stress and the feeling of loneliness. Even though most of the participants have their husbands and children with them in Finland, they still miss their parents, siblings and friends in their home countries.
Unemployment is mentioned as one of the main reasons for many psychological problems in participants – which leads them to seek health-related information through different sources. Participants mentioned that they feel hopelessness and disappointment in the Finnish recruitment system because they do not get any interview call after applying for hundreds of job applications. They associated the need for a job with the feeling of self-confidence and independence. For example, Alia mentioned: ‘The first thing I wanted to do in Finland was to get a good job and be independent and help my husband for a better life. But I did not get any job yet. I think my past experience and degrees are just useless’. While most of the participants did not know about the psychological services available at the health centres, one participant, Nazia, searched for the need of a psychologist to talk about her unemployment situation and stress and got the appointment through a general health centre. Nazia mentioned she got an appointment with a psychologist at the local health centre once and the session was 30 minutes long. She complained after the session that the psychologist only talked about general things about her life but not particularly about her feelings and depression. Later, she searched on Google and found online paid sessions with psychologists from Pakistan. She managed to find an online psychologist from Pakistan with whom she is discussing her matters in Urdu on Skype once a month. She is happy with the online sessions because she believes the psychologist from Pakistan understands her culture well and guides her accordingly.
Most of the participants’ behaviour shows the frustration from the long waiting time in getting appointments with the psychologists in Finland, and therefore, they turned to other digital solutions such as some participants joined yoga and meditation sessions on YouTube to overcome the stress in their lives. They seeked help mostly from YouTube, Instagram, online video sessions with psychologists, chatting with psychologists and WhatsApp calls to family.
7. Health information-seeking challenges
7.1. Lack of information about health and fitness services
Participants mentioned that they were not aware of most of the health services available in the city when they arrived in Finland. And, even after living in the country for several years, they still do not have information about many of the health services. For example, rehabilitation services for mental well-being and sports and fitness services for immigrants. Zara mentioned: When I came to Finland, I only knew about the local health centre (Terveyskeskus) near my home but did not know what kind of services I could get in this centre besides seeing a general doctor. I never heard of psychological treatment available at the centre and neither our teachers at schools ever mentioned it.
Similarly, Huma mentioned: I wish I knew about the work psychologist option available for me at my occupational health centre before when I was new in Finland and needed help. Nazia said: I was only referred to a psychologist by a doctor after three years of checkups and failed treatments for my fertility issue. I wish I knew about it before.
She added that she was not aware of learning swimming opportunities available from the city of Turku for all adult immigrants unless she met another Pakistani girl in the community.
7.2. Fear from information seeking and information sharing
The behaviour of fearing from information seeking is seen in the interviews. The participants highlighted this fear in various forms such as fear of seeking information from a doctor because of long waiting time. For example, Zara mentioned that she is scared of the long waiting time for the appointment to see the doctor for her disease that she does not even want to call the health centre and rather look for other options online. Another form of fear is associated with wasting the time for a doctor’s appointment. Most of the participants mentioned that in many cases, the doctor tells the same thing as discussed in the earlier appointment already and this wastes their time by travelling to the health centre. For example, Jasmine said: I had to cancel a very important meeting with my colleague to see the doctor. This was the second time with the same doctor about my indigestion problem and he did not tell me anything new. He repeated the same advice which I already had from the previous appointment. He asked me to change my diet plan once more.
Fear of information seeking is also associated with discrimination that participants face in the healthcare system. In this study, only two participants mentioned that they felt discrimination based on language skills. One said: The moment I entered the door, the doctor asked me Finnish or English? And I replied, English. She asked me how long I have been living in Finland and I replied, four years. She made a strange face and said why I do not know Finnish even after living in Finland for four years. Anyhow, the doctor managed to speak English with me but I personally feel that she did not handle my matter with care and referred me for another doctor in future. Now, I am scared to see any other doctor in Finland unless I learn good Finnish language.
Another said: the doctor refused to tell me about my reports because I did not know Finnish and asked to bring my husband who can understand Finnish. And my husband was not in the country at that time. I felt bad that the doctor did not explain the reports to me just because I do not understand Finnish or he did not want to speak English. I am afraid that I must have my husband with me in future appointments with me unless I learn sufficient Finnish.
The behaviour of fearing from information sharing is also obvious in different statements of interviewees. First, fear of information sharing because of cultural differences is mentioned by some participants. For example, Isha mentioned that she was not comfortable sharing information about her financial issues with her psychologist, imagining that she might not understand the situation well. Because the situation is different in Finnish culture. She felt fear that the psychologist might judge her that she is not earning independently but depending on her husband which is normal in Isha’s culture. Similarly, Nazia faced a situation where she had fear of sharing information about her food habits with her physician, imagining that the physician might laugh or make a joke of the type of Indian food she eats. She said: ‘My Indian food is too oily and fatty, which is totally different from Finnish food. So the doctor might make fun of my food. Therefore, I was afraid to share this with her’. Second, fear of information sharing because of lack of trust in psychologists is also mentioned by the participants. For instance, Hamia mentioned: I did not tell my psychologist about my personal matters with my spouse because how can I trust her that she will keep it secret. Afterall, she is an outsider. But I am confused that if I will not tell her the whole situation, how would she help me.
Third, fear of information sharing due to gender restrictions is also mentioned by one participant. Participants refused to share the complete information about her mental and physical situation with the male doctor because of uncomfortability.
7.3. Not satisfied with the information
There are several statements and situations where participants mentioned how they are not satisfied with the information they receive and the behaviours of doctors. For example, Laila mentioned: I was not satisfied with the appointment with the doctor because she told me that all of my physical problems are related to stress. I should not take stress. But I believe that we all have some extent of stress in our lives but not everyone has the same physical problems like me. And how can I control my stress? It’s not in my hand. I think the doctor did not take my situation seriously or she did not have enough knowledge about the disease.
Another situation where Zara explained her dissatisfaction with the doctor: The doctor started typing all what I was saying into her computer and spent almost fifteen minutes. And, in the end she talked to me for only five minutes. I think the doctor could stop typing and listening to me carefully. It seemed that she was more focused on keeping records in her system than talking to me and understanding my situation.
Zara faced another situation where she saw a doctor for her indigestion problem and she doubted that she might be allergic to gluten and wanted some examinations to confirm. But the doctor asked her to wait for one more month before examination. She was not satisfied with the doctor’s information and searched on YouTube for other solutions.
8. Socio-cultural factors influencing the challenges in health information-seeking process
In the following, there are certain socio-cultural factors that influence the challenges the participants face during health information-seeking process in this study.
8.1. Cultural and language similarities
Participants seek health-related information from people from their own ethnic culture such as their spouses, friends, relatives and doctors. Participants mentioned that it is easy to communicate with people from their own home country because of language and cultural similarities. For example, Sara had a stressful situation regarding her family structure and she consulted about the matter initially with her friends from Pakistan on WhatsApp because they are aware of a Pakistani family structure and understand the situation more easily than any other persons from other cultures. Similarly, Hamia mentioned: I have some Finnish friends but when I had irregular menstrual cycle problem, I rather consulted some friends from India, living in Finland, because I feel we have the same psychology. And, I can explain my problem more easily in Hindi.
Some participants mentioned that they are seeking health-related information from YouTube and Instagram and mostly subscribe and follow YouTubers and Instagrammers from their own country, because of cultural and language similarities. Isha mentioned: I went to a Finnish gym instructor once and she told me many different tips for diet plan and exercise and asked me to stop the oily Indian food. But she does not understand that I cannot stop my cultural food. I love it. Then, I watched some Indian YouTubers explaining about weight loss and diet plans and they suggested some modifications to Indian food to lose weight. And not completely stop it.
Imaan added: I follow Pakistani and Indian YouTubers and instagrammers for exercise, yoga and diet plans because of Urdu and Hindi language. And, I think they explain tips particularly for an Asian body.
8.2. Participants’ perception about Finnish healthcare system and doctors’ behaviour
In this study, participants’ perception about the Finnish healthcare system and doctors’ behaviour is associated with several challenges they face in the health information-seeking process. The perception about the Finnish healthcare system is mostly associated with negative remarks by the participants. They complained about long waiting times for appointments with doctors and nurses as the gateway between patients and doctors. They mentioned that they first need to see the nurse for their medical situation, and the nurse decides if the patient needs to refer to the doctor or not. ‘There is a lack of freedom in deciding to see the doctor or specialist in Finland’, mentioned by one participant. Another complaint was about delaying the tests for the patients, for instance, a participant was not sent for the blood test unless she got very sick. One of the most highlighted problems in the Finnish healthcare system was the culture of not prescribing antibiotics for normal bacterial infections. Participants compared the Finnish system with their own country’s culture of medication where it was easy to get antibiotics for bacterial infections even without doctors’ prescriptions.
The perception about doctor–patient communication style causes dissatisfaction with the information they get from the doctor. For example, one participant is found upset with the behaviour of the doctor writing down her problems in her computer and spending much time on keeping records then talking to her in person. In another situation, lack of physical touch by a physiotherapist during examination is shown as a dissatisfied session. In addition, the participants got the perception from the Finnish doctors that they take health situations (e.g. stomach issues, weight gain and hormonal imbalance) less serious unless it is a very risky situation (e.g. injuries, bleeding, accidents and pain). ‘It’s normal’ is the frequent phrase that participants heard from the doctors in most situations. For example, some statements participants heard from the doctors are: ‘it’s normal in this age, it’s normal to have weight gain if you have moved to a new country, it’s normal to have certain health issues due to stress, it’s normal to have stress because of workload’. Participants feel that the doctors try to normalise the situation instead of giving solutions such as medication, tests or referral to the specialists. Another perception about doctors’ behaviour is that they mostly prescribe the same pain-killer (i.e. Burana) for different health problems such as headache, body pain, fever or migraine. While participants expect more treatments than just having a pain-killer such as X-ray or blood test for clarifications. Moreover, doctors’ unwillingness to speak English or lack of English language proficiency is also mentioned as a barrier to information seeking for the participants.
The perception about the Finnish healthcare system and doctors’ behaviour is somehow influenced by socio-cultural beliefs and practices of participants’ own home country. It is noticed that the participants were comparing the Finnish healthcare system and doctors’ behaviour to their own countries’ system. For example, one participant mentioned that: it is a social trend of people in Pakistan or India to get antibiotics so easily, even without the prescriptions, and on the counter with a small price that we are used to taking antibiotics even for the normal bacterial infections such as flu.
Another mentioned: In Pakistani culture, the attitude of a doctor is considered positive if he/she listens to the patient, asks questions to the patient and touches the body for examination when required.
Some participants also mentioned that they do not need to go through a nurse to see a doctor in Pakistan or India which saves their time and makes it easier to access the medical care. Similarly, the doctors do not delay the tests or examinations and do prescribe multiple medications for a single disease in certain cases in Pakistan or India.
9. Discussion
The overall aim of the study is to understand the health information-seeking behaviour of South-Asian immigrant women in Finland – from the socio-cultural perspective. It is important to study particularly the women’s aspect of health information seeking to fill the gap in previous research and to improve the health services in their everyday lives for the better integration of this particular group in the society.
9.1. Health information sources
The findings reveal that participants seek health information from sources including family and friends, health professionals in Finland and doctors and psychologists in their home country. Both physical and mental health-related information is mainly accessed by online sources such as health e-blogs, WhatsApp calls to family, YouTube videos, Instagram hashtags and videos and Facebook groups. Some of the participants attend online sessions with psychologists from their home country rather than attending in-person appointments with a Finnish psychologist. The heavy dependence on online health information seeking is noticed in this study – because of the challenges they face in accessing offline health information in Finland [51]. However, one can discuss that the heavy dependence on online health information sources may lead to several challenges which is not a focus in this study. The challenges such as information overload, misinformation, privacy concerns and risks of negative and depressing information [53,63].
9.2. Reasons for poor physical and mental well-being of participants
The ELIS concept by Savolainen (1995) suggests that individuals seek information to address specific problems in their daily lives [21], which can span areas like health, work or studies. In this study, the findings demonstrate that participants seek information to resolve health-specific problems illustrating the problem-specific information-seeking behaviour described by Savolainen [21]. This study aligns with many previous studies where immigrants tend to have problem-specific information-seeking behaviour in their everyday lives to seek a job, to solve health problem and to look for housing, education or learning a language [1,27,28]. This study shows that the problems, related to the physical and mental well-being, are the significant concerns of South-Asian immigrant women in Finland. Physical well-being refers to seeking information about healthy lifestyle, weight management, healthy cooking options, hormonal issues, family planning, diet plans, exercise and sleeping disorders. Mental well-being refers to seeking information about coping with stress, meditation, yoga, motivational videos and quotes about life and coping with Finnish weather and culture. It is also shown that the physical well-being of participants is influenced by their mental well-being, for example, most of the physical challenges of weight gain and sleeping disorders are the results of mental stress. The main reasons for poor mental health of the participants are associated with the challenges in learning a new language, lack of social networks, new to Finnish culture, discrimination and unemployment [13,80]. These reasons align with the results of other studies [101,6,80]. This shows that participants need special support from Finnish rehabilitation services available for immigrants’ mental and physical well-being. But according to the Finnish Institute for Health and Welfare [61], immigrants underuse the rehabilitation services because most of the services are not known to them [78,79]. This highlights the fact that the Finnish healthcare system lacks in disseminating the information about rehabilitation services for immigrants such as psychological treatments, sports and fitness services and other mental health treatments [75]. The Finnish healthcare system needs to make improvements to access the immigrants more easily and timely – which can improve their overall well-being resulting in better integration into the host society.
9.3. Challenges in health information seeking and the impact of socio-cultural factors
The ELIS concept emphasises that information-seeking behaviour is influenced by both situational and contextual factors, which are shaped by an individual’s life circumstances, social roles and cultural environment [21,29,15]. Align with previous ELIS studies [21,29,15], this study shows that participants face some challenges in their everyday life health information-seeking process and these challenges are influenced by certain socio-cultural factors. The main challenges mentioned by the participants are lack of information about health services, fear from information seeking and sharing and not satisfied with information from the doctors in Finland. The main socio-cultural factors mentioned by the participants are cultural and language similarities [20] and perception about Finnish healthcare system and doctors’ behaviour. The participants fear from information seeking and sharing with the Finnish doctors because of long waiting times in getting appointments, discrimination based on language skills, cultural differences, lack of Finnish language skills of participants, lack of English language skills of Finnish doctors or unwillingness of Finnish doctors to communicate in English with foreigners, lack of trust in Finnish doctors and gender restrictions. These phenomena can be related to the concept of information avoidance where people intentionally avoid certain information causing mental discomfort, causing anxiety and increasing uncertainty [102,103]. The information avoidance behaviour is notably evident in the context of health information-seeking behaviour towards preventable diseases and unhealthy habits in previous studies [104]. However, in this study, the participants seem to avoid information to save their time, to ignore the repetitive information from doctors and to avoid the discrimination. Similarly, the unsatisfactory behaviour of participants is associated with their perception about the Finnish doctors’ behaviours. Most of these perceptions are negative and are influenced by the socio-cultural background of participants, for example, in participants’ home country, it is easy to access the doctors and specialists without any gateway of nurses, antibiotics and other medications are readily available without doctors’ prescriptions and no restrictions to have examinations. In a study by Akhtar and colleagues [62], similar results are shown where Pakistani female patients can get antibiotics without doctors’ prescription in Pakistan and it is normal in Pakistani culture. Thus, aligned with other studies [62,65], this study also finds that immigrants’ socio-cultural backgrounds shape their perceptions about certain medical systems and doctors’ behaviours which in result impacts their health information-seeking endeavours.
9.4. Integration problems
It is interesting to see that socio-cultural factors such as cultural and language similarities help some participants seeking health information, especially the psychological help from psychologists from their own country in their own mother language. However, this behaviour also indicates the lack of trust in Finnish doctors and inaccessibility and unavailability of needful health services in Finnish local healthcare. This behaviour has a negative impact on immigrants’ integration. The Finnish Integration plan is lacking in providing the necessary health services to immigrants and unable to build trust. Moreover, poor mental and physical health of immigrants reduce the ability of immigrants to pursue activities key to integration such as studies, work and socialising in the host country [13,6].
9.5. Theoretical and practical contributions
This study makes an important contribution to the LIS literature [23,25,105,106] in general and more specifically to Savolainen’s (1995) ELIS concept, particularly in the context of immigrant women and their integration into host societies [21]. These contributions extend and refine the ELIS framework by incorporating socio-cultural dimensions and exploring the specific challenges faced by migrant women during the information-seeking process. Savolainen’s (1995) ELIS concept is a concept used to understand how people seek and use information in the context of their everyday lives, more specifically problem-specific information [21]. The concept emphasises that information-seeking behaviour is influenced by both situational and contextual factors, which are shaped by an individual’s life circumstances, social roles and cultural environment [26,107]. While Savolainen’s concept acknowledges the role of social and cultural factors, this study delves deeper into how specific socio-cultural factors – such as cultural and language similarities and perception about local healthcare system and doctors’ behaviour – directly influence the information-seeking behaviour of immigrant women. This nuanced understanding enriches the ELIS concept by emphasising the importance of socio-cultural contexts in shaping information behaviour, particularly in diverse and multicultural settings. In this way, this thesis broadens the perspectives of looking at ELIS, the concept of Savolainen [21,26] from socio-cultural and gender-specified angels which is not explicitly discussed in previous literature. Moreover, this study adds on to the health information-seeking literature from the socio-cultural perspective and from the gender-specific (i.e. women) aspect of immigrants [15,108,51,53] and guides about their challenges in health information-seeking journey and the potential socio-cultural factors impacting those challenges. Thus, the study offers insights for information science, public health and migration studies which broadens the scope of the study.
Practically, the study provides guidance for health centres, health professionals and organisations dealing with immigrants’ health matters in Finland. Based on findings, this study provides some suggestions for the Finnish healthcare system to reduce the waiting time for appointments with doctors and specialists, disseminate information about health services more effectively to immigrants, encourage anti-discriminatory behaviours towards immigrants and offer healthcare professional culturally sensitive training and information about the special needs of immigrant women. For example, public health strategies can include training for healthcare professionals on cultural competence, language sensitivity and the specific health needs of immigrant populations. Building trust through better communication and actively involving patients in decisions about their care could improve immigrant women’s satisfaction with healthcare services and encourage more proactive health-seeking behaviours. In addition, Finnish health centres can consider hiring foreign doctors with diverse cultural experience and multilingual skills to help immigrants discuss their medical issues in multiple languages. Furthermore, health information materials, such as pamphlets, websites or apps, should be available in multiple languages and be sensitive to cultural variations in health perceptions. The study also highlights that many immigrant women fear seeking or sharing health information due to concerns about privacy, stigma or perceived judgement, especially regarding mental health. This fear can create a barrier to accessing necessary care. Public health campaigns should focus on reducing stigma, promoting confidentiality and educating immigrant communities about the rights and protections available within the Finnish healthcare system. Moreover, government or public health organisations could develop or enhance multilingual, user-friendly health websites and apps that provide accurate, culturally appropriate information about physical and mental health services, available healthcare options and how to navigate the system. Moreover, mobile health apps could include features like real-time language translation or virtual consultations with culturally competent healthcare providers, making health information more accessible and less intimidating.
10. Conclusions and future directions
This is one of the few studies in Information Studies which highlights the health information-seeking behaviour of immigrant women from a socio-cultrual perspective. Physical and mental health information is the main concern of the immigrants, and they consider family, friends and doctors for seeking information. However, online sources are the most popular information sources for health information seeking in this study. Lack of information about health services, fear from information seeking and sharing and not satisfied with information from the doctors in Finland are the main challenges. Participants face these challenges due to socio-cultural factors such as cultural and language differences and the perception about the Finnish healthcare system and doctors’ behaviours.
Future studies may consider studying the outcomes of heavy dependence on Internet and social media and understand the role of information overload and misinformation in the health information-seeking journey of immigrants in a new country. Future studies may also consider studying the relationship between unemployment and mental health and how it impacts on health information-seeking behaviour of immigrant women. In addition, future researchers may consider studying the influence of religious factors on health information-seeking behaviour of immigrants, because this current study did not focus on religious factors but socio-cultural factors precisely. Moreover, the participants’ age of this current study was 25–36 years, while future researchers may consider studying immigrant women who belong to older age groups such as above 60 years, to get an understanding of older immigrant womens’ health information-seeking behaviours.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.