
Abstract
Introduction
Accurate determinations of the cause of death are crucial for public health, crime investigations, and social justice. In the Netherlands, cause-of-death determinations rely heavily on external examinations, which can miss substance-related deaths. This study investigates the added value of toxicological blood testing in the determination of the cause and manner of death by forensic physicians in the Netherlands.
Methods
Collected blood samples of 642 decedents that were examined by a forensic physician in Amsterdam and surrounding regions underwent toxicological testing. Findings and concluding remarks from the external examination and toxicological testing were compared using descriptive statistics.
Results
Blood samples of 69% of cases tested positive for one or more pharmaceuticals, and 36% tested positive for illicit drugs and/or alcohol. In 55% of cases, toxicological testing revealed substances that were not indicated by the external examination. Its findings also prompted a revision of the initial cause and manner of death in 18 cases (3%).
Discussion
Key limitations in this study include that not all detected substances were quantified and a verification bias of the included cases, which may have led to an underrepresentation of unsuspected detections. Nonetheless, despite the constraints of (routine) screening capabilities and the effects of post-mortem degradation and redistribution, this study presented the importance of toxicological blood testing within a multifaceted approach that combines toxicological findings with scene evidence, medical history and the external examination, which is essential for improving the accuracy of cause-of-death determinations by the forensic physician.
Keywords
Introduction
The determination of the cause of death is of great importance for monitoring trends in health and disease, having a pivotal role in (inter)national public health interventions and the identification of crime-related deaths. Moreover, accurate determinations of the cause of death contribute to social justice by ensuring that deceased individuals receive a correct classification of their death, providing clarity and accountability to both bereaved families and society at large. In the Netherlands, the cause of death is commonly determined by forensic physicians, who perform an external (post-mortem) examination when no attending physician is available, when the attending physician is not convinced of a natural death, or when there are indications of an unnatural death. They inform the Public Prosecutor when they are not convinced of a natural death, after which further judicial investigations can be pursued, including an autopsy. The Dutch medicolegal system relies heavily on external examinations by attending physicians and forensic physicians, and both clinical and forensic autopsies are rarely performed.1–3 In contrast, countries such as the UK and Nordic countries more often involve coroners or medical examiners, and autopsies are more routinely conducted.4–6 Nevertheless, autopsy rates have been declining globally over the past few decades.2,3,6–10 Explanations for this decline include changes healthcare systems, social and cultural factors, lack of financial incentives, and the assumption that the cause of death is already known.2,3,8,11 As a result, concerns exist about the reliability of cause-of-death determinations across the world, including the Netherlands. External examinations do not always provide conclusive evidence for the manner and cause of death, and discrepancies are commonly discovered when compared to autopsy findings.12–15 The identification of intoxications is particularly challenging, as the external examination often does not reveal anything remarkable in these cases. The complementary role of toxicological testing in the forensic investigation on the manner of death is increasingly acknowledged, as it establishes whether drugs and/or other substances contributed to a death. In addition to fatal poisonings that can be confirmed, revealed or excluded, post-mortem toxicological results may provide information on the contributing factors and general circumstances of the death. An American study of 1180 medical examiner cases found that history and scene investigation alone were ineffective at predicting the presence of intoxicating substances, as half of the positive cases were missed. 16 Another study revealed that toxicological testing in initial cases of natural death without autopsy resulted in an amendment of the cause and manner of death in 5.7% of cases. 17 Additionally, toxicology results were identified as the most common reason for the amendment of death certificates. 18 This underscores its relevance further, especially given recent reports by the Dutch National Drug Monitor 19 and the European Union Drug Agency, 20 indicating a rise in both substance use and substance-related mortality across Europe.19,20 In Amsterdam, post-mortem examinations conducted by the forensic physician routinely include post-mortem toxicological testing for alcohol and a range of common illicit and prescription drugs since 2007. This first-line toxicological testing aims to provide rapid, broad-spectrum substance screening in cases where the cause of death is unclear, contributing to a broader investigative scope that supports the forensic physician’s assessment before the body is released. This differs from toxicological analyses performed within a strictly forensic context, where the primary aim is to support legal proceedings in cases. Each year forensic physicians in Amsterdam perform approximately 1100 external examinations in Amsterdam and neighbouring regions (∼1.8 million residents). Previous research demonstrated that toxicological urine screening during the external examination in the Dutch medicolegal context provided new insights into the circumstances of death. 21 However, post-mortem urine drug testing also has several limitations. Urine concentrations do not necessarily reflect serum concentrations and the presence of drug in the urine may not correlate with the actual effects of the drug on the body during the onset of death. 22 Currently, the extent to which post-mortem toxicological blood testing enhances cause-of-death determination by the forensic physician in the Dutch medicolegal context remains unexamined. Therefore, the current study aims to investigate the added value of toxicological blood testing in the determination of the cause and manner of death by the forensic physician in the Netherlands. Our primary objectives were to (1) identify the most frequently found substances in post-mortem blood samples collected by the forensic physician during the external examination, (2) determine how often toxicological analyses in post-mortem blood samples confirm, invalidate or discover new substances compared to information obtained during the external examination and (3) determine how often a (non-)toxicological contribution to the death was concluded after toxicological analyses and how it compared with the conclusion of the forensic physician and vice versa.
Methods
Study population
This prospective cross-sectional study focused on the post-mortem toxicological blood testing in cases of deceased adults that were examined by forensic physicians working for the Public Health Service Amsterdam (GGD Amsterdam) in Amsterdam and surrounding regions between January 2017 and December 2018. Cases were eligible for toxicological testing when a death occurred outside of the hospital or if a death occurred in the emergency room of a hospital.
Data collection
In this study, data from external examinations conducted by forensic physicians and toxicological testing performed by OLVG hospital were assessed. During the external examination, the body of the deceased, scene of death and the medical history were examined by the forensic physician according to the guideline of the Dutch Forensic Medical Society. 23 Forensic physicians recorded their observations and conclusions on the cause and manner of death, compiling their findings into an external examination report. Additionally, for the current study a questionnaire was created and filled in by the forensic physician to gather detailed information for the evaluation of post-mortem toxicological screening on-site. This included questions about signs that might have contributed to the death, including indications for recent drug use (e.g. based on witness accounts or the presence of drugs, drug paraphernalia, injection marks) or a history of drug abuse (e.g. based on the deceased’s medical records or statements from acquaintances). During the external examination, forensic physicians drew blood samples from a peripheral vein, typically the femoral or jugular vein. These samples and the corresponding external examination report were then sent to OLVG hospital for toxicological testing. For the studied cases, no autopsies were performed for the collection of blood samples or determination of the cause of death.
Toxicological analysis
After blood samples were taken by the forensic physician, they were stored as soon as possible at −80°C. Toxicology analyses were generally started < 12 h after external examination and blood sampling by the forensic physician. Fluoride was added to the collection tubes as a preservative. The chain of custody was guaranteed by labelling of all samples with a unique code, referring to an individual sample collection according to the Dutch national guideline. The laboratory of clinical and post-mortem toxicology of OLVG hospital was ISO-17025 and ISO-15189 certified.24,25 Qualitative, confirmatory and identification analyses and quantitative analyses were validated according to GTFCh and SWGTOX guidelines.26,27 For toxicological analyses, the Toxtyper (LC-MS) (Toxtyper™ (Bruker, Bremen, Germany)) was used to identify over 900 drugs and metabolites using Liquid Chromatography-Mass Spectrometry (LC-MSn). Sample pretreatment was done by addition of acetonitrile to post-mortem blood. In specific cases, at the request of the forensic physician or on the initiative of the hospital pharmacist-toxicologist, the concentration of a detected substance was determined (quantification). This was carried out whenever quantification was deemed relevant, especially when the substances that were found could be linked to a toxicological contribution to death, such as an overdose. Furthermore, using Gas Chromatography-equipped with a flame ionization detection (GC-FID), alcohol, several other volatile substances (including acetone and methanol) and gamma-hydroxybutyric acid (GHB) were quantified in the blood samples. Detected substances and conclusions on a toxicological contribution to a death were compiled in a toxicology report by the hospital pharmacist-toxicologist.
Data analysis
Information from the external examination recorded by forensic physicians on indications of (specific) drug use was divided into four subgroups: a positive indication (i.e. recent drug use or history of drug use) for specified substance; positive indication but not specific (e.g. ‘white substance found’); positive indication but different drug mentioned and; no indication. For identified medications, the corresponding substance group at the ATC (Anatomical Therapeutic Chemical) classification level 2 was assigned. The ATC classification system categorizes medications into different groups based on the organ or system they affect, as well as their chemical, pharmacological, and therapeutic properties. 28 In this system, the first level consists of a letter indicating the anatomical main group, while the second level consists of two digits representing the therapeutic or pharmacological subgroup. This classification is widely used internationally in pharmaceutical research.
Statistical analysis
Descriptive statistics like frequency distributions were used to summarize the data. Characteristics of included cases, including demographic characteristics, types of causes of death as well as found substances were summarized. Additionally, it was examined whether the presence or absence of substances assessed by toxicological blood analyses resulted in new insights into the circumstances surrounding death. Therefore, indications for drug use from external examination reports and detected substances from toxicological reports were collected and compared, as well as concluding remarks from both the external examination reports and toxicology reports on the manner and cause of death. Statistical analyses were performed with SPSS for Windows version 26.0 (SPSS Inc, Chicago, Illinois).
Results
Characteristics of cases
Forensic physicians from the Public Health Service Amsterdam performed 2080 external examinations between January 2017 and December 2018. Of these, for 643 cases a post-mortem blood sample was sent to OLVG hospital for comprehensive toxicological testing.
Characteristics of deceased individuals examined by the forensic physician (n = 2080), and those for whom blood samples were analyzed for toxicological blood testing (n = 642).


Overview of included cases and performed toxicological analyses.
Detected substances
Detected pharmaceuticals
Top 20 detected pharmaceuticals in post-mortem blood samples (n = 642).
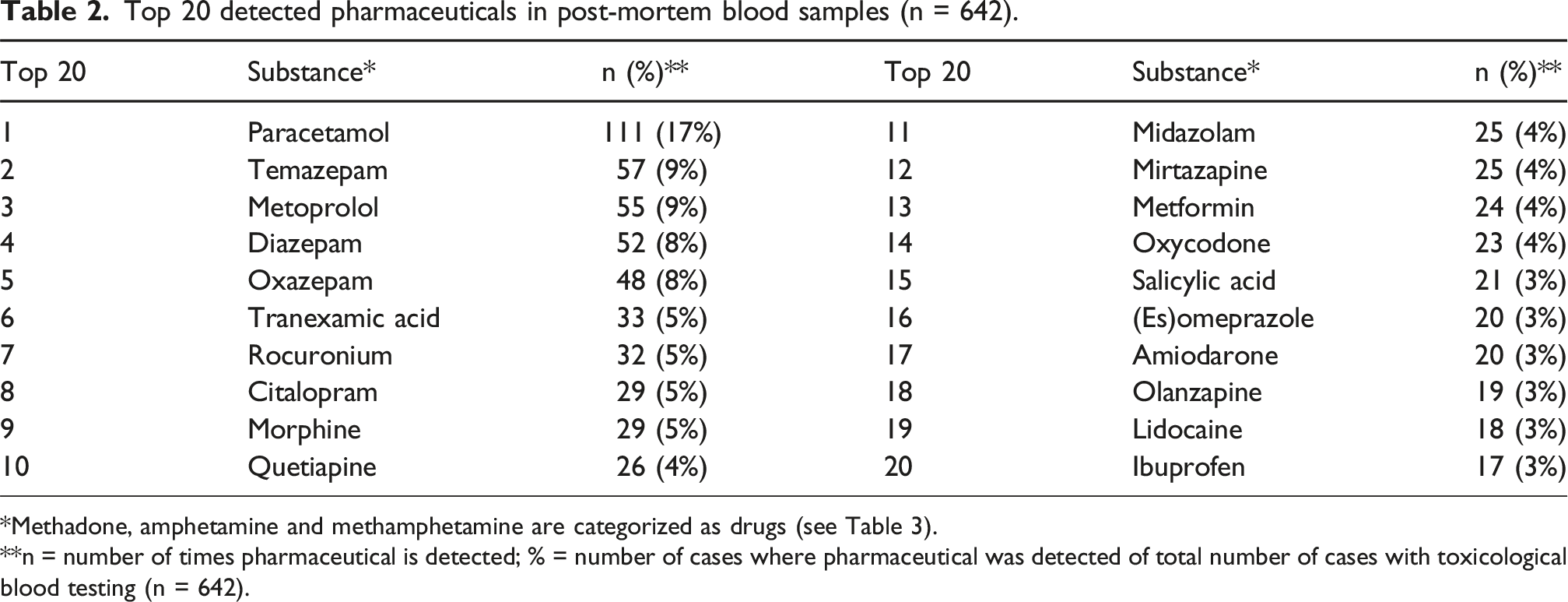
*Methadone, amphetamine and methamphetamine are categorized as drugs (see Table 3).
**n = number of times pharmaceutical is detected; % = number of cases where pharmaceutical was detected of total number of cases with toxicological blood testing (n = 642).
Detected (illicit) drugs and alcohol
Detected drugs in post-mortem blood samples of deceased individuals (n = 642).

*including metabolites.
**n = number of times drug is detected; % = number of detected drug of total number of cases with toxicological blood testing (n = 642).
Detected ethanol concentrations in post-mortem blood samples of deceased individuals (n = 150).

*n = number of cases where alcohol was detected; % = number of cases where alcohol was detected of total number of cases with toxicological blood testing (n = 642).
**Only the presence of a metabolite of ethanol (ethyl sulfate) was detected.
Findings from toxicological testing compared to findings from the external examination
Findings from the external examination for deceased with a positive toxicological outcome for alcohol and commonly found drugs and pharmaceuticals.

na = not applicable. *including metabolites.
**n = number of cases where substance was detected; % = of total number of cases where substance was detected.
1 recent drug use (based on heteroanamnesis or i.e. presence of drugs or paraphernalia) and/or indications of a history of drug use or addiction for the specific substance 2 recent drug use (based on heteroanamnesis or i.e. presence of drugs or paraphernalia) and/or indications of a history of drug use or addiction, but a specific substance was not mentioned.
§ Pharmaceuticals classified under Anatomical Therapeutic Chemical (ATC)-code N02 (various analgesics).
# Pharmaceuticals classified under Anatomical Therapeutic Chemical (ATC)-code N05 (psycholeptics, including sedatives, other tranquilizers, antipsychotics, and barbiturates).
$ Pharmaceuticals classified under Anatomical Therapeutic Chemical (ATC)-code N06 (psychoanaleptics, including antidepressants).
Findings from the external examination compared to findings from toxicological testing
Findings from toxicological testing for deceased with a positive indication of specified substance use from the external examination, for alcohol and commonly found types of drugs and pharmaceuticals.
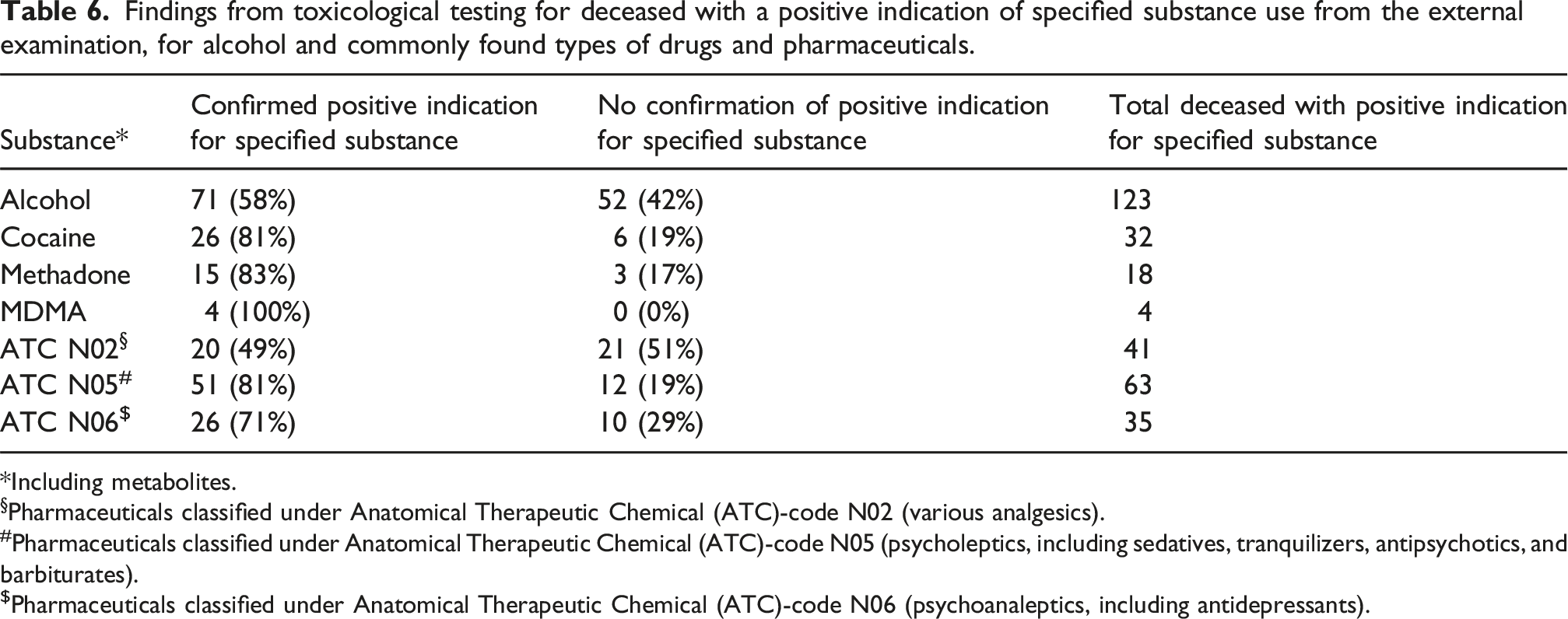
*Including metabolites.
§Pharmaceuticals classified under Anatomical Therapeutic Chemical (ATC)-code N02 (various analgesics).
#Pharmaceuticals classified under Anatomical Therapeutic Chemical (ATC)-code N05 (psycholeptics, including sedatives, tranquilizers, antipsychotics, and barbiturates).
$Pharmaceuticals classified under Anatomical Therapeutic Chemical (ATC)-code N06 (psychoanaleptics, including antidepressants).
Concluding remarks on toxicological contribution compared to manner and cause of death determined by the forensic physician
Based on the concluding remarks of the hospital pharmacist on the toxicological contribution to the death of an individual, in 66 (10%) of the 642 cases a toxicological contribution to the death was very likely. In 11 cases the conclusion of the forensic physician was a probable non-toxicological cause of death while toxicological testing revealed a fatal intoxication. For 6 cases the conclusion of the forensic physician on the manner of death was natural while a toxicological contribution and therefore unnatural cause of death was found based on the toxicological test. In total, for 11 cases (17%) of the 66 cases for which a toxicological contribution to the death was very likely, conclusions on the cause and manner of death needed to be revised.
Additionally, cases in which a toxicological contribution to the death was unlikely were compared with conclusions on the cause and manner of death from the external examination. Of 642 cases, for 429 (67%) a toxicological contribution to the death was unlikely based on the results of toxicological testing. After comparing the external examination report with the toxicological findings, it was determined that in 7 (2%) cases, the conclusion of the external examination report needed to be revised, as no toxicological evidence was found to support the suspected intoxications. In 10 cases, the toxicological analysis was insufficient to assess the forensic physician’s conclusion (among which 3 cases of suspected insulin intoxication and 3 cases of suspected helium intoxication).
Discussion
This study investigated the added value of post-mortem toxicological blood testing in medicolegal investigations performed by the forensic physician in a large metropolitan area in the Netherlands. It is the first study to provide insights in the extent to which rapid and broad-spectrum toxicological testing is of added value in the Dutch medicolegal system, in which cause-of-death determinations heavily rely on external examinations. The findings from this study demonstrate a high prevalence of pharmaceuticals (69%) and (illicit) drugs and/or alcohol (36%), reflecting a widespread use of substances in the studied population. Importantly, toxicological testing revealed the unsuspected presence of specific substances in the majority (55%) of cases and toxicological testing prompted a revision of the conclusion on the cause and manner of death in 18 (3%) cases. This demonstrates that the external examination by the forensic physician itself presents limitations with regards to predicting the presence of intoxicating substances and a toxicological contribution to the death, as was demonstrated by previously mentioned studies.16,17,21 This study shows that reliance on the external examination alone risks missing critical evidence of substance involvement, affecting the accuracy of cause of death determinations. Moreover, without toxicological testing, opportunities are missed to support public health efforts for drug surveillance. As mentioned before, European trends show substance use and substance-use related mortality is rising.19,20 Specific concerns exist regarding an increase in polysubstance use and the rise of new psychoactive substances (NPS or ‘designer drugs’), as well as the availability of very potent substances. This evolving landscape highlights the importance of vigilance and the integration of toxicological testing in the medicolegal investigation by the forensic physician. However, post-mortem toxicological blood testing comes with its limitations. First, toxicological analysis only identifies substances that are included in the routine panel and present in the laboratory’s analytical library. While these libraries are continuously updated and specific tests can be requested based on indication, emerging substances such as NPS or other non-routine compounds may go undetected. 29 Second, although toxicological blood testing aims to reflect the concentration and potential physiological impact of substances at or near the time of death, interpretation is complicated due to redistribution of substances in the body after death, degradation over time, and influences such as individual metabolic differences and interactions between substances and their metabolites.30–34 Moreover, the increasing medicalization of the population, along with the growing prevalence of polysubstance use pose additional interpretative challenges, as current knowledge on the prevalence, mortality and mechanisms of specific interactions between (illicit) substances remains limited. More research on these factors is necessary in order to increase the accuracy of toxicological interpretations, improve the overall reliability of cause-of-death determinations and guide prevention strategies. These factors also highlight the importance of a combined approach, in which toxicological testing can serve as a crucial tool to extend the scope of the post-mortem examination beyond what is externally observable. Combining toxicological findings with the decedent’s medical history, scene investigation, and external examination can lead to more accurate conclusions about the cause and manner of death.
Policy implications
The findings of this study provide important evidence on the added value of toxicological testing in medicolegal investigations by forensic physicians, offering data that can inform policy decisions. This research highlights the potential benefits of more systematic integration of toxicological analyses within the Dutch medicolegal framework. However, implementation requires careful consideration, as forensic physicians in the Netherlands operate within a complex context. They must balance limited resources, legal responsibilities, and a wide variety of cases, ranging from clearly unnatural deaths to sudden, seemingly natural fatalities in elderly individuals. Moreover, while the possibility to perform post-mortem toxicological blood testing as part of the external examination is now available nationwide, its actual use varies depending on local policies and practices. These realities underscore the need for evidence-based guidance to support clinical judgment and enable selective, yet effective, testing strategies, as is presented in this study. Ultimately, the integration of toxicological testing into routine practice should be shaped by informed dialogue within the field, weighing accuracy and justice against feasibility and sustainability. This dialogue is currently taking place for the development of a national guideline for external examinations by the forensic physician, including post-mortem toxicological blood testing.
Study limitations and strengths
The current study has several limitations. First, not all detected substances were quantified. While quantification was performed for all cases and substances where this was deemed relevant, especially for substances that could be involved in a toxicological contribution to a death, some fatal intoxications might have been missed. Currently, quantification is limited not only by high costs but also by the lack of validated reference frameworks for interpreting post-mortem concentrations, especially for substances with a narrow therapeutic index affected by redistribution and degradation.17,19 To support more routine quantification and further improve the detection of potentially lethal intoxications, future research should focus on further developing such reference frameworks and exploring semi-quantitative methods that allow differentiation between high and low concentrations, even without prior suspicion.
Secondly, cause and manner of death were determined solely based on external examination and toxicological analysis. As no autopsies were performed, internal findings could not be considered, introducing uncertainty in the determined cause and manner of death. Additionally, a potential source of selection bias in this study is that toxicological analyses were only conducted when requested by the forensic physician. This introduces a form of verification bias (workup bias), as cases in which the forensic physician might not suspect toxicological relevance were not tested. As a result, our dataset may overrepresent cases where toxicological findings align with initial forensic assessments while underrepresenting instances where unexpected substances could have been detected. This limits our ability to present a comprehensive view of the overall added value of toxicology in medicolegal investigations by the forensic physician, as it remains unknown what might have (not) been missed in cases that were not tested. Also, the chain of toxicological testing and therefore the information used in this study is based on the documented findings by the forensic physician. When their findings have not been documented properly, information used by the hospital pharmacist as well as the researchers might have been missed. Nevertheless, this study found a high level of documentation and digital accessibility, with all reviewed cases containing clear and well-documented reports. Since this information also serves as the foundation for external examination reports—a core responsibility of the forensic physician—it further supports the likelihood that this data is reliable and comprehensive. However, this study did focus on the city of Amsterdam and surrounding regions, a large metropolitan area that houses more students, tourists and drug users in comparison with other regions in the Netherlands. As a result, an extrapolation of our results for other regions is limited. However, the findings remain relevant, as they illustrate the diagnostic value of toxicological testing in a high-prevalence setting, where substance use is common but not always apparent from external examination alone, highlighting the broader importance of routine toxicological screening. Strong points of this study include the epidemiological approach by reviewing large numbers in routine forensic medical practice, providing robust insights in the contribution of post-mortem toxicology in determining the cause and manner of death by the forensic physician. Another strength of this study is the comprehensive toxicology screen with GC-FID and LC-MS. The use of the Toxtyper™ with iontrap LC-MSn is a state-of-the-art method for identification of drugs in body fluids, recommended for forensic analyses. LC-MS/MS is widely used with applications in medical laboratories covering a broad range of substances and analytes in toxicology and therapeutic drug monitoring.35–37
Conclusion
This study presents the valuable contribution of post-mortem toxicological blood testing in the medicolegal investigation by the forensic physician in the Netherlands. According to this study, various key recommendations are presented.
Key recommendations
• Acknowledge the limitations of the external examination in identifying the involvement of substances without toxicological testing • Promote discussion on ethical, legal and practical implications of routine versus selective post-mortem toxicological testing • Recognize the value of rapid and broad-spectrum (first-line) post-mortem toxicological testing not only for cause-of-death determination, but also for public health surveillance of trends in drug use • Research challenges regarding current testing methods, including the scope of routine screening and the complexities of interpreting post-mortem blood concentrations • Emphasize a multifaceted approach that combines toxicological findings with the external examination including scene evidence and medical history, as this remains essential for improving the accuracy of manner and cause-of-death determinations
Footnotes
Acknowledgements
The authors would like to thank Marijke de Vries for her contributions to the data collection and analyses.
Ethical considerations
This study used anonymized data collected under the statutory mandate of forensic physicians according to Dutch law (Article 7, Wet op de lijkbezorging, Wlb), the professional standard as formulated by the Dutch Society of Forensic Medicine (Forensisch Medisch Genootschap) and the Dutch Code of Conduct in Health Research (‘Gedragscode Gezondheidsonderzoek’, sections 5.4.1 and section 5.5), and therefore did not require separate institutional ethical approval.
Author contributions
M. Ceelen, A. Kadhim and E.J.F. Franssen conceived the study. M. Ceelen, A. Kadhim and N.C. Eckhardt collected and analyzed the data and wrote the manuscript. V.N. Slev, U.J.L. Reijnders and E.J.F. Franssen contributed to the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data were anonymized prior to analysis and handled according to GDPR requirements. Data are not publicly available due to confidentiality. Requests for data and materials should be addressed to the corresponding author.