
Abstract
This study evaluated standard toxicology screening by forensic physicians during external post-mortem examination. Collected urine samples of decedents were screened on-site for the presence of 10 commonly used drugs by means of a rapid multidrug test. Urine samples of 53% of the cases appeared to be positive for one or more compounds. Importantly, several cases were revealed which were positive for toxicology screening without indications for use of these drugs at the scene of death or from medical history. Based on these (preliminary) results, further action to incorporate routine post-mortem toxicology as a tool in forensic death investigation is recommended.
Introduction
The use of autopsy is declining in most developed countries since the latter half of the 20th century. 1 In The Netherlands, less than 7% of the decedents were autopsied in 1998. 2 Major limiting factors are the increased focus on cost control within both the public and private healthcare sectors and advances in pre-mortem diagnostic techniques. 3 Although autopsy is still considered the golden standard to assign cause and manner of death, nowadays diagnoses on death certificates are predominantly based on external examination conducted by the attending physician or the medical examiner.
However, the accuracy of cause of death determination by means of external examination has been questioned frequently. The population-based study of Modelmog et al., consisting of essentially all deaths occurring over a 1-year period in inhabitants of a German city, compared full autopsy findings with cause of death determined by the attending clinician. 4 Overall, 47% of diagnoses on death certificates differed from those based on autopsy and for 30% of the subjects, the difference crossed a major disease category. Other studies also reported significant discrepancies in underlying cause of death between death certificates and autopsy findings. 5 –8 It is of great importance to determine the precise cause of death as non-natural deaths have to be reported to the public prosecutor or coroner, who assesses the need for further investigation. Furthermore, cause of death reported on the death certificate is used for statistical purposes in epidemiological studies.
Less invasive techniques such as toxicological screening in small urine or blood samples are suggested to contribute to the evaluation of death cause. Besides confirming, revealing or excluding fatal poisonings, post-mortem toxicological results may provide information on the contributing factors and general circumstances of the death. 9 Toxicology results have been found to be a common reason to amend death certificates. 10 Furthermore, Gruszecki et al. demonstrated that clinical history, death scene investigation and physical findings identified only half the cases positive for intoxicating substances in decedents. 11 Especially in non-natural deaths, toxicology findings merited inclusion on the death certificate as a cause of death or contributing factor in approximately half of the cases where initial investigation did not suggest the presence of intoxicants.
Since April 2008, forensic physicians in Amsterdam, The Netherlands, performed toxicological urine screening during their external post-mortem examinations on-site. The goals of the present study were to determine (1) how frequently a toxic substance was detected using on-site post-mortem urine screening in decedents, (2) assess the concordance of two analytical methods (on-site test and laboratory test) and (3) whether the presence or absence of intoxicants determined by these toxicology tests provided new insights into the circumstances of death.
Methods
Study population
This study was conducted at the Forensic Medicine Department of the Municipal Public Health Service in Amsterdam, The Netherlands. Forensic physicians of this department act as the medical examiner for each (potentially) unnatural death in Amsterdam and neighbouring regions (~1.25 million residents). They annually examine approximately 1100 decedents. The main goal of the external examination is to clarify the cause and manner of death. The cause of death relates to a specific disease, injury or abnormality that initiated physical and biological events that directly led to death. 12 The manner of death, which explains how the cause of death arose, can be either natural or unnatural.
In the present study, post-mortem urine screening was performed in adult decedents that were examined in Amsterdam by the forensic physicians between April 2008 and April 2009. Violent deaths (n = 24), euthanasia and physician-assisted suicide (n = 188), deaths during hospital or nursing home admissions (n = 198) and deaths with a post-mortem interval of 7 days or more (n = 66) were not eligible for the study. Cases were included in the study if the death occurred outside the hospital or if death was confirmed in the emergency room of a hospital, before the patient was admitted. The forensic physicians were instructed about the study procedures by the principal researcher (MC).
Data collection
During the external examination, the decedent, scene of death and the medical history were examined by the forensic physician according to the guideline of the Dutch Forensic Medical Society to identify signs that might have contributed to death. Attention was paid to physical signs suggestive of recent use of intoxicants such as injection marks on the body and the presence of drugs/medication or drug paraphernalia. Based on all these findings, the cause and manner of death were established.
Subsequently, a post-mortem urine sample of the decedent was collected by means of suprapubic puncture or urethral catheterisation for toxicological screening on-site. A rapid on-site multidrug test was used to screen the urine samples for the presence of the following commonly used drugs classes: amphetamine, barbiturates, benzodiazepines, cannabis, cocaine, 3,4-Methylenedioxymethamphetamine (MDMA), methadone, methamphetamine, morphine and tricyclic antidepressants (TCA) (DrugControl© type 008A410, DeltaSigma) at cut-off concentrations shown in Figure 1 . This test contains a specific arrangement of different lateral flow chromatographic immunoassays using mouse monoclonal antibody-coupled particles and drug-protein conjugates. Goat antibodies are employed in the control line systems. The multidrug test was considered positive if both the test line and control line were visible and negative if only a control line appeared. The shade of red in the test line appeared to vary, but the test was considered negative whenever there was even a faint pink line. Finally, the urine samples were sent in a polypropylene test tube without preservative to ATAL Medical Diagnostic Center in Amsterdam for immunoassay validation. Here, the Thermo Fisher/Microgenics type Cedia test was used on an Olympus 2700 analyser for the detection of amphetamines, cocaine, methadone and benzodiazepines, whereas the Thermo Fischer/Microgenics type DRI was used for opiates and cannabis. For ethanol, the DRI-ethyl alcohol homogenic enzyme reaction was used. The following cut-off values for screening mentioned in the European Laboratory Guidelines for Legally Defensible Workplace Drug Testing were used: alcohol (ethanol): 0.2 mg/mL, amphetamines (d-methamphetamine): 1000 ng/mL, benzodiazepines (after glucuronidase treatment, calibrated on nitrazepam): 200 ng/mL, cocaine (benzoylecgonine): 300 ng/mL, cannabis (delta-9-THC-carboxylic acid): 50 ng/mL, methadone (EDDP): 100 ng/mL and opiates (morphine): 300 ng/mL. In addition, all test results were interpreted in perspective of the case (PZ).

Cut-off concentrations of the on-site multidrug test.
Furthermore, cocaine, metamphetamine, amphetamine, MDMA and cannabis were considered drugs of abuse, as were opiates except medicinal opiates that were used for pain relief (i.e. oxycodone, tramadol and paracetamol mixed with or combined to codeine). According to the level of toxicity, drugs of abuse were subsequently categorized as ‘low-risk drugs of abuse’ (cannabis) and ‘high-risk drugs of abuse’ (other above-mentioned drugs of abuse). Medicinal opiates as well as benzodiazepines, barbiturates and TCA were classified as medications.
Information about the presence at the scene of death of drugs or paraphernalia, use of drugs shortly before death or history of drug abuse was extracted from the electronic registry used by the forensic physicians to extensively document the findings of the external examinations. Moreover, a questionnaire was filled in by the forensic physician to gather detailed information for the evaluation of post-mortem toxicological screening on-site including the urine sample collection and drug screening results. Indications for drug use from these sources were divided in indications for recent drug use (based on heteroanamnesis or i.e. presence of drugs or paraphernalia) and indications of a history of drug use or addiction (based on heteroanamnesis or medical records). Heteroanamnesis was defined as an interview with family members, bystanders and/or physicians like the family doctor. Indications for medication use were all classified as recent use.
Statistical analysis
Descriptive statistics like frequency distributions were used to summarize the data. Furthermore, the concordance of urine test results obtained with the multidrug test on-site and the laboratory instrumental immunoassay tests were examined by determining their sensitivity, specificity and efficiency. 13 Sensitivity was calculated as true positives/sum of true positives and false negatives. Specificity was calculated as true negatives/sum of true negatives and false positives. Efficiency was calculated as sum of true negatives and true positives/total urine samples tested. Kappa statistics (κ) for levels of agreement between the multidrug test and the laboratory tests were used. This statistic provides values of +1 (perfect agreement) via 0 (no agreement above that expected by chance) to −1 (complete disagreement). 14 In addition, it was examined whether the presence or absence of intoxicants assessed by toxicological analysis resulted in new insights into the circumstances surrounding death. Therefore, we determined how frequently analysis of urine results strengthened, revealed or did not indicate drugs use in relation to scene examination and heteroanamnesis. Statistical analysis was performed with SPSS for Windows version 17.0 (SPSS Inc, Chicago, Illinois, USA).
Results
Characteristics of decedents
In total, 200 of 380 eligible death cases examined by the medical examiners during the study period were included in the present study. The main reasons for non-inclusion were other priorities of the forensic physician during the shift and non-availability of toxicology equipment. Subsequently, 113 of the 200 attempts of the forensic physicians to collect post-mortem urine samples were successful. The characteristics of the eligible decedents with and without toxicological urine screening are listed in Table 1 . Compared with those cases without a urine sample (n = 267), cases with a urine sample (n = 113) were more likely to be examined <24 hours after death and to have indications of drugs of abuse, medication and alcohol use.
Characteristics of external examination cases a

a Cases with a urine sample (US+) and those without a urine sample available (US−) were compared on demographics and characteristics provided by the external examination using independent t-test and chi-square test. The sample size was slightly less for some variables.
b Time interval between death and external examination.
c Cocaine, heroin, amphetamine, methamphetamine, MDMA, methadone.
d Benzodiazepines, barbiturates, morphine-related medication, and tricyclic antidepressants (TCA).
Urine collection and drugs screen on-site
Urine samples of 113 decedents examined in the present study were collected by means of suprapubic puncture (n = 57), catheterisation (n = 46) or other methods/method unknown (n = 10). One out of 113 multidrug tests gave an invalid test result. Urine samples of 30 cases (27%) were positive for one of the tested compounds, 26 cases (23%) for two or three compounds and three cases (3%) for four or more compounds. Most frequently detected drugs include in descending order benzodiazepines (n = 37), cannabis (n = 18), morphine (n = 16), cocaine (n = 13) and methadone (n = 12; Table 2). Although the low number of cases in some of the subclasses hamper statistical comparison, decedents with a positive urine test for cocaine and cannabis were significantly younger at death compared with decedents with a negative test (p = 0.003 and <0.001, respectively). In addition, urine tests for benzodiazepines were more often positive in female decedents (40% female versus 20% in the negative test group, p = 0.01).
Drug test results on-site of 112 post-mortem urine samples according to age and gender a
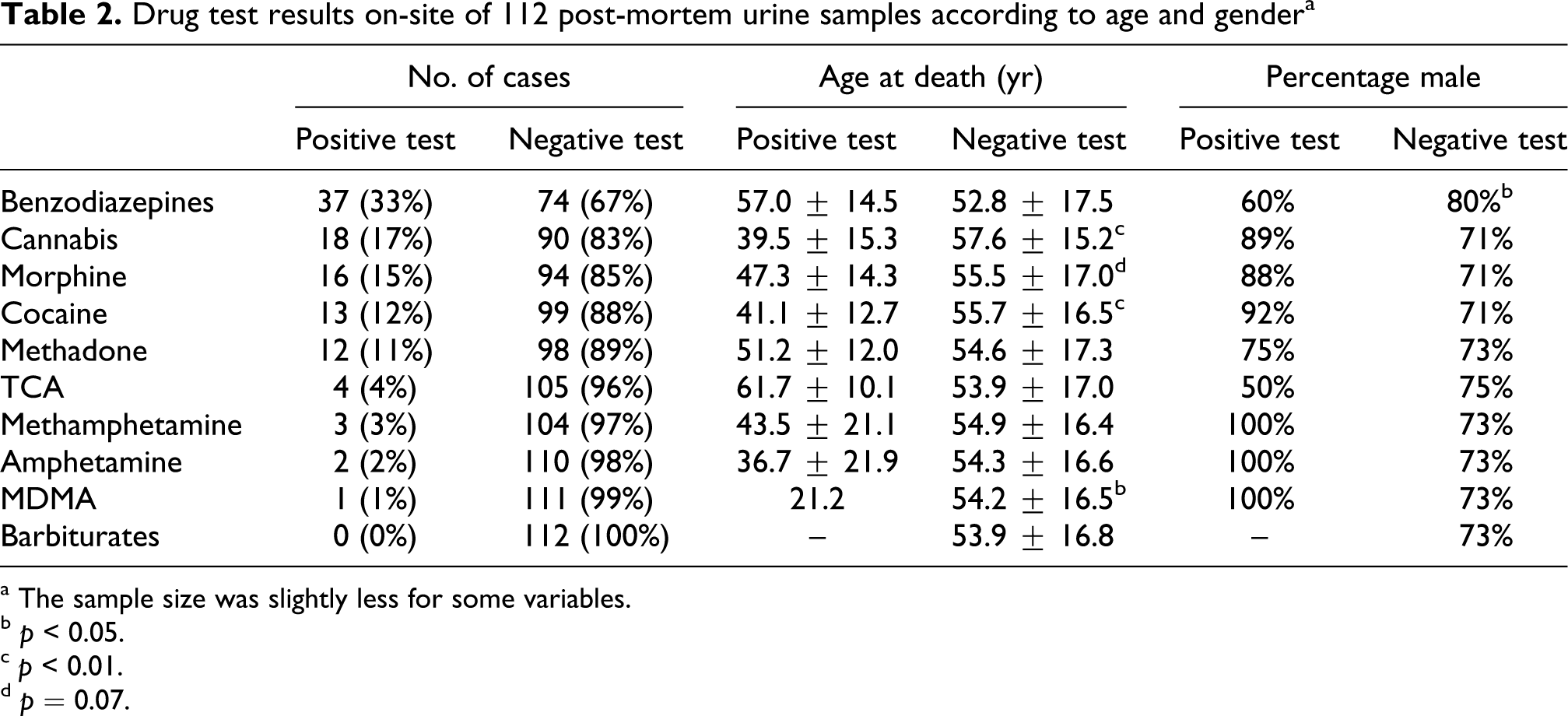
a The sample size was slightly less for some variables.
b p < 0.05.
c p < 0.01.
d p = 0.07.
Concordance analysis
Results for the analytical sensitivity, specificity and efficiency for the multidrug test compared to the laboratory tests are shown in Table 3 . Sensitivity was demonstrated to vary from 79% for benzodiazepines to 100% for amphetamine and related compounds. Furthermore, the concordance between the test results obtained by the multidrug test and the laboratory tests measured by Kappa can be considered as substantial (0.61–0.80) for two drugs classes and almost perfect (>0.80) for five other drugs classes.
Comparison between the multidrug test results and the analyses in the laboratory a
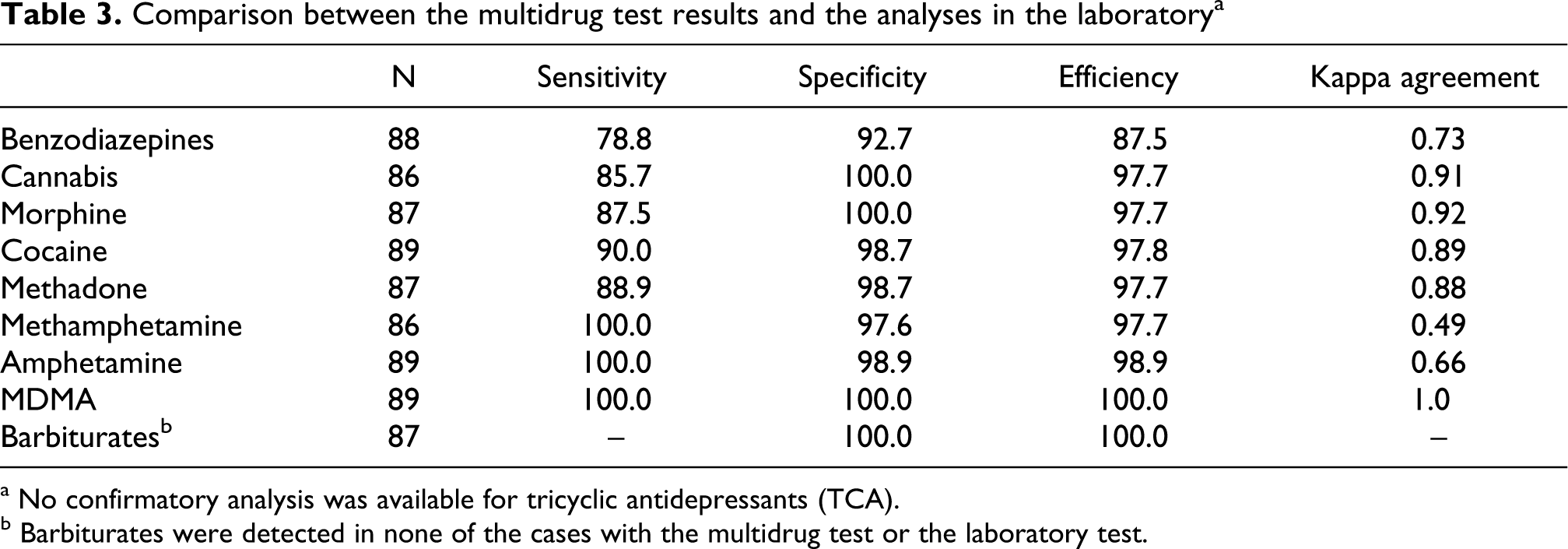
a No confirmatory analysis was available for tricyclic antidepressants (TCA).
b Barbiturates were detected in none of the cases with the multidrug test or the laboratory test.
Drug test results in relation to heteroanamnesis and scene investigation
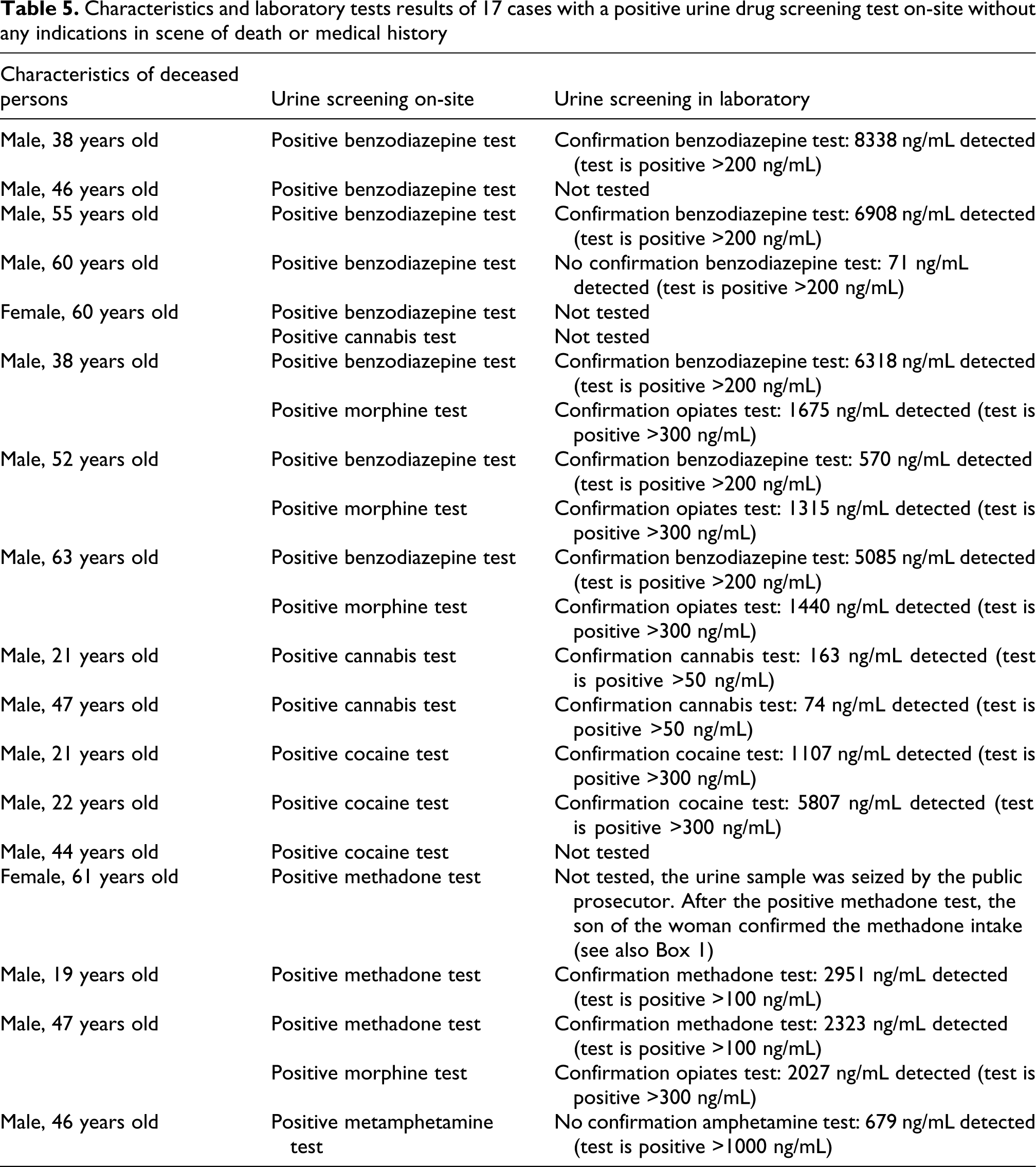
Table 4 demonstrates how frequently toxicological analysis results revealed, strengthened or made drug use unlikely in relation to scene examination and heteroanamnesis. The majority of the cases with indications for recent use or abuse of drugs were strengthened by toxicology screening. Similarly, most cases without indications for recent use or abuse of drugs were followed by a negative toxicology screening result. Nevertheless, in several cases without indications for drugs use, positive multidrug tests were found. For instance, urine of 7 out of 89 cases without indications in scene of death or heteroanamnesis for use of high-risk drugs of abuse were found positive for this type of drugs. One of these cases is presented in Box 1 in more detail. In Table 5 , main characteristics of all revealed cases are summarized.
Indications from the scene of death or the medical history of the decedent for drugs use in relation to urine screening results a

a Above-mentioned urine screening results were based on the multidrug test, except for alcohol, which was based on the laboratory test.
b Indications for history of use, abuse, or addiction, without indications for recent use.
c Cannabis.
d Cocaine, non-medicinal opiates, amphetamine, methamphetamine, methadone.
e Benzodiazepines, barbiturates, medicinal opiates and tricyclic antidepressants (TCA).
Characteristics and laboratory tests results of 17 cases with a positive urine drug screening test on-site without any indications in scene of death or medical history
Discussion
This study evaluated a standardized toxicology screening by means of immunoassay on-site during the external examination in the field of forensic medicine. Urine samples of approximately half of the decedent cases were found to be positive for one or more compounds. Importantly, several cases that were positive for toxicology screening were revealed without indications for use of these types of drugs in the scene of death or medical history. Furthermore, toxicology screening was also useful with respect to the confirmation or unlikeliness of recent drug use.
To our knowledge, the present study is the first to use a commercially available immunoassay as screening procedure for the detection of 10 classes of drugs in urine specimens of decedents examined by forensic physicians. Immunoassay devices for on-site drug testing represent a rapidly growing segment in the drug screening market and are currently used in several settings, including a variety of clinical applications. 15,16 These types of immunoassays, which are based on ligand/receptor technology, have been compared to laboratory-based screenings system and are found to be equally effective, less costly and more rapid. 17 We also found that the concordance between the results obtained by the two analytical methods (immunoassay on-site and laboratory immunoassay) was good. Nevertheless, it is important to keep in mind that for validation of any analytical procedure, a method using a completely different analytical principle should be used. Results of immunoassays (either on site or in a laboratory) should be considered presumptive due to the possibility of false negative or false positive test results until confirmed by an analysis that is recognized as confirmatory (e.g. gas chromatography-mass spectrometry (GC-MS) and liquid chromatography-mass spectrometry (LC-MS)). 18
Our study revealed several unexpected positive drugs screens in urine samples of deceased persons. However, the interpretation of such test results is complicated. Although urine has been considered to have the greatest potential of any specimen to provide qualitative ante-mortem drug-exposure information, 19 urine samples do not necessarily reflect the amount of substance the subject was influenced by at the time of death. A positive urine test does not essentially mean that the drug of abuse caused the death. Many drugs can be detected in urine several days following use, especially in heavy users. A high drug concentration in post-mortem urine cannot be specifically linked to a drug overdose. Therefore, post-mortem urine screening can be very useful to detect the presence of various substances, although it should be followed by quantitative, confirmatory blood tests in order to determine whether the detected substance did cause or contributed to death.
It is also important to take into account that forensic physicians examine a distinct subpopulation of deaths. Only cases where the cause of death is not obviously natural are brought to the attention of the forensic physician. In addition, in the present study, death cases with a urine sample available for toxicology screening differed from those cases without a urine sample. Therefore, our findings cannot be directly generalized to all deaths occurring in Amsterdam and may also differ from the total number of decedents examined by forensic physicians. Nevertheless, our findings demonstrate that in more than 50% of the decedents examined by the forensic physician, one or more substances were detected in the urine sample. This is in line with a non-forensic study by Gruszecki et al. with low non-inclusion rates. 11
In view of an adequate determination of the manner and cause of death, it is important to have an accurate idea whether the decedent was under the influence of certain drugs shortly before death, since drugs can cause or contribute to death. However, the majority of drugs do not produce visible characteristic pathological changes on the body. Therefore, the forensic physician is dependent on other indications that can be apparent during death investigation. The forensic physician attempts to acquire the medical history of the deceased and the circumstances surrounding death through interviews with family members, bystanders and physicians like the family doctor and investigation of the body and scene of death. However, heteroanamnesis and scene investigation are not always effective at predicting the presence of intoxicating substances within decedents, as was demonstrated by ours and other studies. 11 Post-mortem toxicological analysis can be considered an essential tool in addition to heteroanamnesis and scene investigation in forensic cause of death determination. The specific detection of many compounds and their metabolites in various matrices have improved substantially over the years. 19 Routine drug screening would be useful in the diagnosis of fatal intoxications. On the other hand, such a strategy could be time consuming, costly and inefficient. Due to a lack of research, it is currently unclear which cases should be subject to universal toxicological screening. More insight into these aspects could be gained from a study that we are currently preparing, which will investigate both urine and blood samples in a large representative number of deceased persons examined by forensic physicians.
In conclusion, post-mortem toxicological screening can easily be conducted on-site, shows good agreement with laboratory screenings techniques and can reveal the presence of several types of drugs which were used shortly before death. This information is relevant for adequate cause of death determination. Further action to routinely integrate post-mortem toxicology as part of death investigation performed by forensic physicians in close cooperation with forensic toxicologists is recommended.
Footnotes
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.