
Abstract
Background
The mechanism of emamectin benzoate (EMB—a macrocyclic lactone insecticide like abamectin) action involves the disruption of glutamate-gated chloride channels and GABA receptors in insects, leading to paralysis and death. EMB overdose can breach the blood–brain barrier, resulting in severe poisoning and altered consciousness.
Aim
Review EMB poisoning presentations in patients and reevaluate clinical manifestations.
Materials and Methods
This retrospective study reviewed (August 31, 2008–August 31, 2023) medical university hospital records. We analyzed symptoms, patient characteristics, vital signs, Glasgow Coma Scale scores, laboratory findings, and outcomes.
Results
Ten patients (males: 6, females: 4, median age = 64.5 years) experienced EMB poisoning. Common symptoms included sore throat, gastrointestinal distress, dyspnea, and altered consciousness; two patients showed laryngeal corrosive injuries. Management involved activated charcoal administration, gastric lavage, and intensive care unit admission.
Discussion
Sore throat and corrosive injuries were distinctive presentations of EMB poisoning, warranting vigilance. Potential mechanisms of corrosive injury include skin and eye irritation effects of EMB, the solvents of which might exert corrosive action.
Conclusion
EMB poisoning manifests as diverse symptoms, including sore throat, gastrointestinal symptoms, central nervous system depression, and potential aspiration pneumonia. Recognizing and promptly managing EMB poisoning are crucial for enhancing patient outcomes and minimizing complications.
Introduction
Emamectin benzoate (EMB) is a macrocyclic lactone insecticide akin to abamectin. Introduced for use on cole crops in the United States in 1997, its mechanism involves augmenting the opening of glutamate-gated chloride channels in the nervous system and stimulating gamma-aminobutyric acid (GABA) receptors. This action incapacitates insects, causing paralysis and eventually death.1,2 Although perceived as having low human toxicity due to its restricted ability to penetrate the blood–brain barrier, high doses might overcome this limitation. 2 Typically, EMB poisoning presents as gastrointestinal upset, central nervous system (CNS) depression, and aspiration pneumonia. In extreme instances, altered consciousness and respiratory failure can ensue.2–7 According to the National Center for Biotechnology Information, EMB has been linked with the potential for corrosive injury. 8 To our knowledge, there are no published reports detailing corrosive injuries in humans due to EMB poisoning. Beyond individual case reports and one cohort study,3–6,9 we have not identified any case series or cohort studies that describe patients affected by EMB poisoning. Owing to the scarcity of detailed information on EMB poisoning, this study investigated the cause of sore throat in patients who underwent EMB poisoning, suggesting a potential for corrosive injury. By meticulously examining all relevant cases and studies in the literature, we aim to gain a comprehensive understanding of the potential effects of EMB poisoning and to identify effective management strategies for such cases.
Materials and Methods
This retrospective chart analysis was conducted at the Medical University Hospital in Taichung, Taiwan, from August 31, 2008, to August 31, 2023. It focused on patients diagnosed with EMB poisoning found through medical records. The keyword ‘Emamectin’ guided our search of the hospital’s poisoning database. Individuals younger than 20 years of age and pregnant women were excluded from the study. According to the laws of our country, individuals under the age of 20 years are considered vulnerable; therefore, we excluded them based on ethical considerations.
Our analysis primarily evaluated the symptoms and management approaches for EMB poisoning. We considered various factors, including age, gender, co-ingestion incidents, quantity of exposure, reasons for exposure, vital statistics, Glasgow Coma Scale (GCS) scores, laboratory findings (especially blood gas, lactate, and potassium), patient disposition (discharge, observation, admission to ward or intensive care unit), and the duration of hospitalization. For each case of EMB poisoning, we meticulously documented demographics, specific details of EMB exposure (such as concentration and volume), treatment strategies, and patient outcomes. Treatment strategies for patients with EMB poisoning included supportive care, airway protection, and decontamination (such as gastric lavage and administration of activated charcoal if exposure to EMB occurred within 1 h, as deemed necessary by the attending physician). Additionally, antibiotics were administered to patients complicated with aspiration pneumonia.
The study was approved by the China Medical University Hospital Institutional Review Board with the exemption code CMUH112-REC3-140. This exemption was based on the retrospective nature of the study and the minimal risk posed to the participants.
Results
Cases of emamectin benzoate ingestion: clinical features, treatments, and outcomes.

Figure 1 illustrates the range of symptoms observed in our cohort after EMB exposure. Seven (70%) patients reported experiencing a sore throat. Gastrointestinal disturbances, including nausea, vomiting, diarrhea, and abdominal discomfort, were reported in 60% (n = 6) of the cohort. Five patients (50%) showed dyspneic symptoms characterized by a respiratory rate exceeding 20 breaths per minute or clinical notes of dyspnea. Additionally, 40% (n = 4) developed aspiration pneumonia and 20% (n = 2) presented with atrial fibrillation. Notably, one patient experienced acute respiratory failure. In terms of neurological impact, 40% (n = 4) of the patients displayed altered levels of consciousness, with initial Glasgow Coma Scale scores of 3, 7, 11, and 13. Biochemical analysis revealed hypokalemia in several cases, with potassium levels of 2.8 mmol/L, 3.2 mmol/L, and 3.4 mmol/L. Shows the symptom prevalence in patients. The most common is a sore throat in roughly 70%, followed by gastrointestinal symptoms at around 60%. Dyspnea affects 50%, CNS depression and aspiration pneumonia both affect 40% of patients. Respiratory failure is the least frequent, affecting just 10%.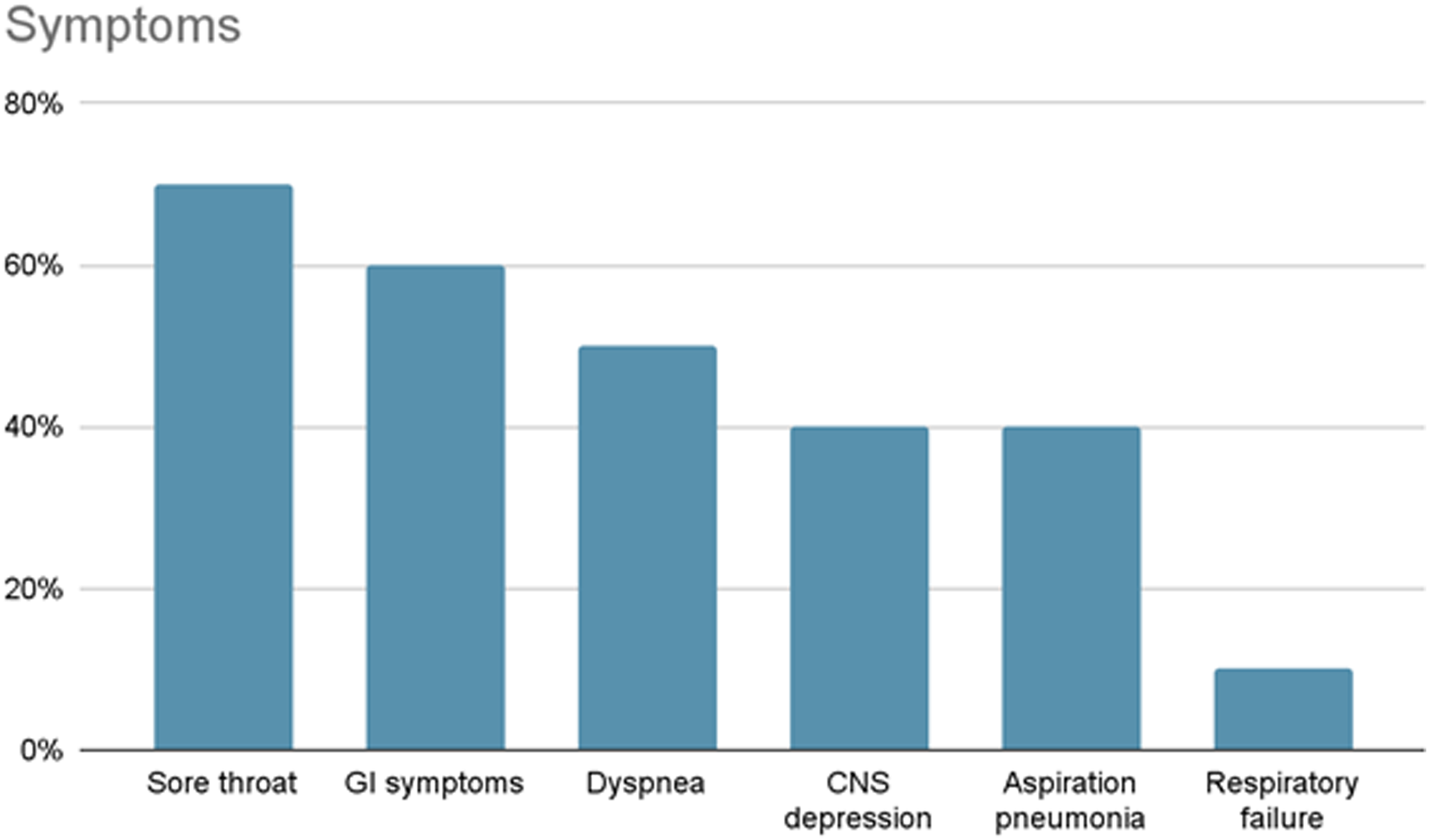
In the emergency management of these cases, activated charcoal was administered to 70% of the patients (n = 7), while gastric lavage was performed on 80% (n = 8). Regarding diagnostic and therapeutic interventions, esophagogastroduodenoscopy was conducted on one patient, revealing gastroesophageal reflux disease, erythematous gastritis, and an ulcer. Flexible fiberoptic laryngoscopy was performed on three patients, yielding diverse findings: mild laryngeal erosion, possibly related to corrosive damage, was noted in one patient; a second patient showed grade II corrosive injury to the oropharynx, larynx, and hypopharynx; and the third patient exhibited edematous mucosa over the bilateral hypopharynx and larynx, also suggestive of corrosive injury. Furthermore, endotracheal intubation was necessary for a patient who presented with respiratory distress and desaturation. No fatalities occurred among the study cohort. One individual with a history of alcohol consumption developed pancreatitis, while another experienced ruptured hepatocellular carcinoma.
Patient disposition: half of the patients (n = 5) necessitated ICU admission, while the remaining went to the general ward for continued care and observation.
Outcome: One patient experienced severe respiratory failure. Furthermore, five patients required admission to the ICU, while the rest had a favorable prognosis. No fatalities occurred among the study cohort.
Aspiration pneumonia was apparent in patients who presented with changes in consciousness. Respiratory failure was attributed to laryngeal edema resulting from caustic injury.
Discussion
The study cohort predominantly presented with sore throat, with two patients showing signs of corrosive laryngeal injury, a unique aspect prompting speculation about EMB as a contributing factor. This hypothesis underscores the need for heightened vigilance in EMB poisoning cases presenting with sore throat, potentially indicating underlying corrosive injury. However, the exact mechanism behind such injuries remains unclear, requiring further research.
EMB has been associated with skin and eye irritations, suggesting potentially harmful effects upon exposure.8,10 Notably, the 2.15% EC formulation of EMB involved in poisoning cases comprises over 97% of solvents, including methanol, 2,6-bis(1,1-dimethylethyl)-4-methylphenol, and 1-hexanol,3,9 and surfactants (sodium 2-[methyloleoylamino]ethane-1-sulphonate and naphthalenesulfonic acid, bis(1-methylethyl), 11 and nonylphenol). 12 2,6-bis(1,1-dimethylethyl)-4-methylphenol exhibits corrosive properties. Additionally, sodium 2-[methyloleoylamino]ethane-1-sulfonate and naphthalenesulfonic acid, bis(1-methylethyl), have been identified as corrosive substances.13,14
These solvents and surfactants may have been responsible for the corrosive injuries seen in our patients. Based on these observations, it is crucial to be vigilant and consistently monitor patients who present with sore throat due to EMB poisoning. Further research is vital to better understand the mechanisms underlying corrosive injury and the possible impact of solvents in EMB formulations. Gaining this insight will help improve patient care and minimize potential complications associated with this caustic insecticide.
In our study, most patients presented with mild injuries, consistent with the findings of earlier studies.2,3,6 The most common clinical manifestations observed in our cohort were sore throat, gastrointestinal disturbances, and mild CNS depression. However, there was a significantly more severe case in which the patient experienced respiratory failure. This case was attributed to a combination of corrosive injury, aspiration pneumonia, and CNS depression.
Traditionally, EMB has been considered nontoxic to humans (mammals) because of its limited capacity to penetrate the blood–brain barrier, the absence of glutamate-gated chloride channels in mammals, and its minimal affinity for mammalian chloride channels. 1 However, significant exposure to EMB can lead to serious poisoning incidents. Patients presenting with CNS depression in our study may have concurrently administered BZD. Caution is warranted when managing cases of EMB poisoning in combination with BZD, considering the insecticide’s interaction with GABA receptors. Concurrent administration of BZD and EMB may aggravate symptoms, given the capacity of EMB to potentiate GABAergic effects. 15 This interaction may result in more pronounced CNS complications. The recognition of these pharmacological interactions is crucial for effective patient management.
Other literature studies documented two fatal cases of EMB poisoning.4,5 One patient died of asphyxia owing to pulseless ventricular tachycardia triggered by vomiting. 5 Another case involved fatality attributed to seizures and severe metabolic acidosis. 4 These incidents have raised concerns about the lethal toxicity of EMB, which is potentially linked to its solvent components, as discussed in several research papers.4,5 In our group of patients, metabolic acidosis was evident in only one case, which coincided with alcohol intake. Although none of our patients exhibited ventricular rhythm disturbances, two presented with poisoning-induced atrial fibrillation. Additionally, three patients displayed hypokalemia, consistent with earlier case reports.5,7 A particularly notable case highlighted a patient who experienced seizures, bilateral aspiration pneumonia, and hypokalemia, leading to ICU admission. 7
Within our cohort of 10 patients, all required hospitalization; notably, half (five patients) required care in the ICU. This observation is consistent with the findings of previous studies. 9 Specifically, a retrospective analysis of intentional poisonings involving avermectin pesticides, such as emamectin and abamectin, indicated that 42% of cases required ICU admission, with 78% requiring hospitalization. 9 Another retrospective analysis which focused on avermectin poisoning cases that involved abamectin and ivermectin, reported a 37% rate of ICU admissions. 16 In this study, ICU care was necessary for 7 out of the 19 documented cases. 13 Wu et al. highlighted a significant correlation between disturbances in consciousness and dyspnea, with both symptoms being indicative of severe clinical outcomes. 9 Upon examining our data, the distribution of ICU admission rates was as follows: among patients exhibiting disturbances in consciousness, 50% (2 out of 4) required ICU care; for those experiencing dyspnea, the rate was 25% (1 out of 4); patients presenting with a sore throat saw an ICU admission rate of 33% (2 out of 6); and notably, a substantial 50% (2 out of 4) of those diagnosed with aspiration pneumonia necessitated ICU admission. Although EMB poisoning typically presents with a low mortality rate, emerging evidence suggests that its toxicity may be more severe than previously understood. 9 Particularly, in cases of significant EMB exposure, a considerable number of patients require not only hospitalization but also intensive care in the ICU, underscoring the potential severity of such poisonings.
Analogous to other macrocyclic lactones, EMB is primarily excreted through the gastrointestinal (GI) tract. 2 Consequently, the management of EMB poisoning frequently involves decontamination methods such as gastric lavage and the administration of activated charcoal, which are typically complemented by supportive care. 2 However, utmost caution is essential in performing gastric lavage or administering activated charcoal in cases of EMB poisoning. This caution is due to the frequent incidence of caustic injury, aspiration pneumonia, and CNS depression seen in these patients. Prioritizing the protection of the patient’s airway is critical before initiating decontamination procedures in cases of EMB poisoning. Ensuring a secure airway is crucial in mitigating the risk of aspiration-related complications, a concern that becomes pronounced when CNS depression has compromised the patient’s protective reflexes. Guaranteeing airway protection and adhering to precautionary protocols enables healthcare professionals to conduct decontamination procedures more safely and effectively in cases of EMB poisoning.
Gastric lavage and activated charcoal are contraindicated in cases involving corrosive agents because re-exposure of the esophagus to these substances may result in further injury. 17
Gastric lavage should only be considered if a potentially life-threatening quantity of poison has been ingested and if the procedure can be started within 60 minutes. However, there is insufficient evidence to support the routine use of gastric lavage. 18
EMB poisoning leading to impaired consciousness can pose a significant risk to patients’ lives, hence gastric lavage is commonly employed in such cases. However, the necessity of gastric lavage may be subject to debate. According to the study “Intentional avermectin pesticide ingestion: a retrospective multicenter study,” evidence suggests that gastric lavage or activated charcoal administration does not significantly affect clinical outcomes. 9 Similarly, in our study, there was no clear benefit observed from gastric lavage or the administration of activated charcoal.
Summary: In our study, many patients with EMB poisoning experienced sore throat and corrosive laryngeal injuries. Despite assumptions of safety, EMB exposure can cause severe adverse effects, such as respiratory failure, especially when combined with substances like BZD. Fatalities associated with EMB poisoning underscore concerns about its heightened toxicity, often requiring ICU admission. Management includes careful use of decontamination methods like gastric lavage and administration of activated charcoal to prevent worsening injuries. Prompt intervention and supportive care are essential for minimizing adverse effects.
Limitations
This study’s small sample size, involving only 10 patients from a single medical university hospital in Taichung, Taiwan. Consequently, this limited dataset might not fully represent the diverse range of EMB poisoning cases and their varied outcomes. Additionally, the absence of a control group in our research design may introduce potential biases, as other confounding factors cannot be ruled out. Factors such as the possibility of missing data, inconsistencies in record-keeping, and variations in the documentation of information might affect the robustness of our findings. Another limitation is our failure to determine EMB or its metabolites in biological samples.
Moreover, our study included patients who had co-ingested EMB with other potentially toxic substances. The simultaneous presence of EMB, BZD, and alcohol could potentially alter consciousness. However, it is unlikely that BZD, alcohol, or carbon monoxide poisoning alone would directly cause symptoms, such as sore throat or corrosive injury.
Our research presents an intriguing hypothesis regarding the potential of corrosive injuries following EMB poisoning. However, these insights are based on a limited number of cases. Owing to this, the precise mechanism underlying this observation remains speculative. Comprehensive, large-scale studies are essential to establish a definitive causal relationship and clarify the underlying mechanisms.
Conclusion
Patients with EMB poisoning may exhibit various symptoms, with sore throat and corrosive injuries as notable presentations. In addition, GI symptoms, CNS depression, and aspiration pneumonia are commonly observed. This diverse array of symptoms underscores the importance of recognizing and promptly managing EMB poisoning to improve patient outcomes and reduce the risk of complications.
Footnotes
Author contributions
Chi-Syuan Pan contributed to the study conception, data collection, methodology, analysis, interpretation, and manuscript writing; Jiun-Hao Yu contributed to the study conception, data collection, methodology, analysis, and interpretation; Chi-Chan Lee contributed to the study conception, data collection, methodology, analysis, interpretation, and manuscript writing; Dong-Zong Hung contributed to the study conception, data collection, methodology, analysis, interpretation, and manuscript writing; Chun-Hung Chen contributed to the study conception, data collection, methodology, analysis, interpretation, and manuscript writing.
Patient Consent
Written informed consent was waived by the Institutional Review Board due to this study posing minimal risk to the participants and all data was fully de-identified to ensure patient confidentiality.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.