
Abstract
Drug-induced liver injury (DILI) is the leading cause of compound attrition during drug development. Over the years, a battery of in-vitro cell culture toxicity tests is being conducted to evaluate the toxicity of compounds prior to testing in laboratory animals. Two-dimensional (2D) in-vitro cell culture models are commonly used and have provided a great deal of knowledge; however, these models often fall short in mimicking natural structures of tissues in-vivo. Testing in humans is the most logical method, but unfortunately there are ethical limitations associated with human tests. To overcome these limitations better human-relevant, predictive models are required. The past decade has witnessed significant efforts towards the development of three-dimensional (3D) in-vitro cell culture models better mimicking in-vivo physiology. 3D cell culture has advantages in being representative of the interactions of cells in-vivo and when validated can act as an interphase between 2D cell culture models and in-vivo animal models. The current review seeks to provide an overview of the challenges that make biomarkers used for detection of DILI not to be sensitive enough during drug development and explore how 3D cell culture models can be used to address the gap with the current models.
Introduction
The liver is a major organ with a vital role in maintaining normal physiologic state, metabolic homeostasis, and detoxification, 1 which makes it highly susceptible to toxic agents/medications/concoctions. 2 Drug induced liver injury (DILI) is caused by overdose or continuous intake of drugs over prolonged periods1–6 and is the main cause of liver failure in patients on chronic medication. 7 Antineoplastic and tuberculostatic agents have been found to be the main offending drugs with approximately 1 in 1000 patients admitted to a health facility developing DILI. 7 DILI has a huge potential of causing clinical challenges when one considers the hepatotoxic potential of some drugs currently on the market, such as non-steroidal anti-inflammatory drugs, antibiotics, antiepileptics and tuberculostatics that has been missed during the early stages of drug development. DILI has been reported as one of the leading causes of drug development attritions, post-marketing withdrawals and boxed warnings (warning put on labels of some medicines for purposes of bringing consumers’ attention to the fact that studies have indicated that the medication has potential to cause significant risk or serious side effects).2,3 Since DILI is a leading cause of drug development attritions and post-marketing withdrawals, it is crucial that sensitive and robust methods are developed to detect DILI as early as possible during drug testing and development.
Published literature reviews on DILI focus on advantages and limitations of available in-vitro models.8–12 Soldatow et al. described various traditional and novel in-vitro liver models, providing a perspective on the challenges and opportunities afforded by each individual test system. 12 Langhans reviewed common approaches to 3D cell culture, discussing the significance of 3D cell culture models in drug resistance and addressed some of the challenges of applying 3D cell culture models to high-throughput drug discovery. 11 Milner et al. compared 2D and 3D hepatic models and assessed their pros and cons. 8 Llewellyn et al. focused on the benefits, limitations, and adaptations of specific in-vitro approaches to assess DNA damage in the liver, whilst identifying critical advancements required to support a multitude of biochemical endpoints for genotoxicity. 10 Miranda et al. reviewed the drug-induced hepatotoxicity mechanisms and the available 3D liver in-vitro models focusing on characteristics, advantages, and limitations for human hepatotoxicity assessment. 9 Kulsharova and Kurmangaliyeva discussed the liver micro physiological platforms from the perspective of drug metabolism studies and highlighted the liver on a chip platform and multi organ systems integrating liver on a chip device used for drug metabolism mimicry in-vitro. 13 The present literature review differs to currently published reviews on the same topic in that we provide an overview on the traditional models for detecting DILI and challenges associated with biomarkers used to detect DILI. In addition, focus is given to the DILI endpoints for 3D liver in-vitro technologies and their advantages compared to traditional in-vivo biomarkers.
To identify relevant articles for this literature review, we did an extensive assessment of currently published research available on online databases such as MEDLINE, Scopus, and Google Scholar. We searched for English articles published up to August 2021 focusing on the pathogenesis of DILI, traditional biomarkers used for detecting liver injury, cell culture models for detecting DILI and animal models for early detection of DILI. This literature search has a limitation in that we may have missed some relevant studies due to time constraints or due to the exclusion of studies published in other languages that are not English.
In the remainder of the article, we present the pathogenesis of DILI, DILI biomarkers and why traditional biomarkers are not specific and sensitive enough for early detection of DILI. We also review the current literature on new biomarkers like the microRNA-122 that have been discovered and how serum levels of these compare to traditional biomarkers in detecting DILI. We provide a synopsis of in-vitro models used for detecting DILI, their classification and properties that make them suitable models as well as end-point assays used for early detection of DILI. We discuss the limitations of 3D cell culture technology in detecting DILI such as limited cell permeability and short cell lifespan. Lastly we explores the future of 3D cell culture technology in drug development, and we conclude by acknowledging that 3D cell culture technology still needs to be validated for in-vitro detection of DILI biomarkers.
Pathogenesis of DILI
The human liver is located on the right upper abdomen and is vital for metabolism occurring in hepatocytes that are segregated into metabolic zones. 14 Xenobiotics that overwhelm the metabolic zonation cause changes in zonation patterns leading to DILI. 14 DILI is classified into three types based on clinical presentation (hepatocellular, cholestatic, or mixed), mechanism of hepatotoxicity (dose dependent or idiosyncratic) and histologic presentation (hepatitis, cholestasis, or steatosis).1,6
The exact mechanism for DILI pathogenesis is not fully elucidated, however, several studies have divided the mechanism into direct or indirect toxicity.1–6 Direct toxicity occurs when drugs or their metabolites directly damage the cytoplasm membrane, endoplasmic reticulum, or organelles of liver cells.1,2,5 Indirect toxicity occurs when toxins first interfere with the metabolic pathways or metabolism of macromolecules, resulting in changes in cell structure due to metabolic disorders.1–6 Direct toxicity is further classified as intrinsic or idiosyncratic DILI. Intrinsic DILI occurs when drugs induce toxicity in a predictable dose-related manner whilst idiosyncratic DILI is caused by agents with little or no intrinsic toxicity (no dose-toxicity relationship). 3 Although mechanisms of toxicity are distinct, the effects of toxins on the liver cannot be practically separated; for example, initial hepatocyte destruction due to direct drug toxicity may be further enhanced by the subsequent inflammatory reaction.3,15 The earliest event in DILI is the inhibition of the mitochondrial respiratory chain, which leads to increased reactive oxygen species (ROS) and depletion of adenosine triphosphate (ATP). 4 A combination of ROS generation, ATP depletion, and mitochondrial insult may induce intracellular hepatocyte damage and death.2,15–17 Hepatocytes apoptosis requires ATP which may not be available due to mitochondrial dysfunction and depleted ATP stores.5,6,15 When there is mitochondrial dysfunction and ATP depletion, hepatocyte death occurs through the necrotic pathway, which may enhance hepatic inflammation.5,6,15
The first step during drug metabolism (phase I reaction) is mediated by the cytochrome p450 (CYP 450) system where intermediate bioactive products are generated. The CYP450 is a superfamily of metabolic enzymes found in the liver endoplasmic reticulum. 3 The intermediate bioactive products (drugs and their metabolites) generated by the CYP 450 are inactivated through glucuronic, glutathione or sulpha-conjugation in phase II reactions. 2 If the phase II glucuronic, glutathione or sulpha-conjugation pathways are overwhelmed, the intermediate bioactive compounds interact with various cellular organelles (e.g. mitochondria) leading to hepatotoxicity.2,15 Most of the therapeutic dose (>90%) is metabolized by glucuronidation and sulphation before being excreted from the body whilst the remaining undergoes CYP 450 metabolism to form the reactive intermediate N-acetyl-p-benzoquinone imine (NAPQI).1,17,18 NAPQI is then detoxified by conjugating with glutathione (GSH).17,18 In acetaminophen (APAP) overdose, the GSH pathways is saturated leading to excess NAPQI that will subsequently bind covalently to liver proteins causing toxicity. 1 Covalent binding of the intermediate bioactive compounds (e.g. hydralazine, tienilic acid) to CYP 450 has been reported to lead to the formation of anti-CYP antibodies and result in immune-mediated DILI.19,20 The anticancer drug bortezomib has been found to lower the levels of the hepatocyte nuclear factor−1a-induced promoter activation of CYPP450 2E1 giving rise to endoplasmic reticulum stress, thereby lowering the rate of CYP2E1 expression with subsequent alleviation of APAP induced DILI in mice. 21
Immune-mediated DILI is characterized by prolonged intervals between drug administration and recognized liver toxicity. 15 Drug metabolites bind to cellular proteins and major histocompatibility complex triggering an immune response directed against the hepatocyte, for example, halothane triggers the generation of antibodies directed against CYP 450 CYP2E1. 2 Immune-mediated DILI may be much more pronounced and severe after repeated exposures to the drug.
DILI biomarkers
Numerous biomarkers for DILI have been explored, but only a few are adopted or qualified as valid by the US-FDA. 22 DILI biomarkers can be individual or a panel of proteins, nucleic acids or metabolites leaking into circulation from the injured liver.23,24 The elevation of biomarkers in blood circulation is often delayed which makes it difficult to interpret the actual extent of hepatic damage. 23 Around 40% of human DILI cases are not detected in preclinical toxicity studies, 25 possibly due to the delay in elevation of biomarkers in blood circulation.
The recommended traditional biomarkers for the assessment of hepatocellular injury in animal models such as rats, dogs, and non-human primates (NHPs) are alanine aminotransferase (ALT), aspartate aminotransferase (AST), gamma-glutamyl transferase (GGT), alkaline phosphatase (ALP) and total bilirubin (TBILI). 26 ALT is considered a more specific and sensitive indicator of hepatocellular injury than AST in rats, dogs, and NHPs. In most cases, ALT increase is usually greater than AST, when both enzymes are increased due to hepatic injury. 27 This is mainly because ALT has a longer half-life, and a greater proportion of AST is usually bound to mitochondria. Hepatocellular necrosis, injury, or regenerative activity causes increased serum ALT activity, with or without increased AST activity. 26 Decreases in ALT activity has been observed with concurrent hepatic microsomal enzyme induction in the rat. 28 Increased ALT activity has been reported with concurrent hepatic microsomal induction in the dog and rat but were not considered indicative of hepatic injury as there was no change in liver histology or weight. 28 Increased serum ALT activity can be affected by extra hepatic factors for example muscle injury can cause increases in serum transaminase activity, but AST is generally higher than ALT when both are concurrently increased. 27 The restraint method can result in increased AST activity with or without increases in ALT activity in mice and NHPs; therefore, type of restraint and extent of handling should be considered in the evaluation of increased AST activity, with or without increased ALT activity. 26 Sorbitol dehydrogenase (SDH) is frequently the most sensitive and specific indicator of hepatocellular toxicity in rats. 29 The determination of SDH activity requires rapid processing of samples from blood collection to chemistry analyzer, unlike the more stable analytes, AST, and ALT. SDH interpretation is not confounded by compound interference owing to modification of pyridoxal phosphate cofactor interaction, as occurs with transaminases. 28 Recently, glutamate dehydrogenase (GLDH) has been studied as a potentially superior biomarker of hepatocellular toxicity in rats than ALT, AST, or SDH. 30
Alkaline phosphatase and total bilirubin (TBILI) are recommended for the assessment of hepatobiliary injury in rats, dogs, and NHPs. 26 In laboratory animals, hepatobiliary pathology and bone growth/disease are the 2 most common causes of increased serum ALP activity. 27 Increases in ALP activity due to hepatobiliary pathology generally precede increases in TBILI concentration in most species. Increased ALP activity from the liver in the absence of cholestasis has been reported in dogs with increased endogenous or administered glucocorticoids in rats and dogs with concurrent microsomal enzyme induction. 26 In rats, intestinal ALP is the major circulating isoenzyme, so a transient increase in serum ALP may occur postprandially, whereas fasting can result in a decrease in serum ALP. Decreases in ALP activity has been reported in rats with concurrent microsomal enzyme induction in the absence of changes in food consumption. Bilirubin, although not very sensitive or specific, is a readily available test and is used for determination of cholestatic processes. 27 Bilirubin may be increased under conditions of hemolysis; this decreases the specificity of this parameter. 31
Gamma-glutamyl transferase is an enzyme found in serum and originates from various organs such as the liver, pancreas, intestine, lungs, and kidneys,32,33 which makes it not specific enough for early detection of DILI. Serum GGT has been used as a biomarker for liver injury, however, studies have shown that elevated serum GGT is not specific for liver injury as it is also associated with cardiovascular disease, diabetes mellitus, hypertension, and metabolic syndrome.32,33
Although traditional biomarkers for liver injury have been applied to the diagnosis of DILI, the lack of specific and sensitive biomarkers poses a major limitation 3 and thus accurate prediction of drugs causing DILI during early drug development. These drawbacks prompt the investigation and discovery of more effective biomarkers (such as microRNA-122, microRNA-192, Keratin 18, High-mobility group box-1, Glutamate dehydrogenase and Cytokeratin-18) for use in the early phases of drug development to prevent pursuing the development of toxic drugs.
Recent attention in literature has focused on the development of microRNA biomarkers of liver injury.23,24,34–36 Because of their abundance and stability in biofluids, circulating microRNAs such as the microRNA-122 and microRNA-192 have emerged as favourable biomarkers for DILI.23–25 mircoRNA-122 represent noncoding RNA that is exclusively expressed by hepatocytes and represents 75% of the total hepatic miRNA content.24,34 These micro-RNAs exhibit drug dosage and treatment duration dependent changes in plasma levels correlating with the levels of ALT and liver degeneration histopathology. 25 Clinical, preclinical, and in-vitro studies have demonstrated an early rise in mir-122 levels before any changes in traditional markers (AST; ALT) detected.23,34 A pilot study conducted by Bakshi et al. concluded that anti-tubercular (isoniazid, rifampicin, pyrazinamide) DILI is associated with decreased expression of liver specific microRNAs (miR-192 and miR-122) which can be considered as potential targets to further understand the mechanism of hepatotoxicity. 25
Keratin-18 is an intermediate type-1 filament mainly found in the epithelium and provides cytoskeletal support to cells. 37 The full-length fragment of Keratin-18 is released during hepatic necrosis and the caspase-cleaved fragment released during apoptosis.23,37 The fragment of keratin-18 or the caspase cleaved keratin-18 form has been demonstrated in APAP-DILI, reflecting total cell death and apoptosis. 23 Keratin-18 rises earlier than comparative rise in serum AST in these studies.
High-mobility group box-1 (HMGB1) is a key DAMP candidate with proposed functions in the regulation of inflammation following tissue injury, LPS-induced shock, and UV irradiation. 24 HMGB1 functions as a DNA-binding protein inducing bends in the DNA helix allowing interactions between DNA and proteins such as p53 in healthy organisms. 38 HMGB1 is passively released from necrotic cells and actively secreted by inflammatory cells, with signature post translational modifications characteristic of the respective release mechanism.34,38 Specific HMGB1 isoforms (e.g. acetyl form) have been demonstrated on patients surviving or requiring liver transplantation secondary to APAP overdose. 23 Inhibition of HMGB1 in rodent models has been found to attenuate paracetamol toxicity indicating its role as a mediator of injury.38,39
Glutamate dehydrogenase (GLDH) is an enzyme found in the matrix-rich mitochondria of the liver, kidney and brain but absent in cristae-rich cardiac and skeletal mitochondria.24,34 The difference between GLDH released by the brain/kidney and liver is that after cellular injury, brain/kidney GLDH enters the cerebrospinal fluid and tubular lumen respectively whilst liver GLDH is released into systemic circulation.24,34 This makes GLDH circulating in blood liver specific as it indicates leakage of liver mitochondrial contents into circulation. 24 Systemic circulation of GLDH has been shown to rise in healthy volunteers treated with heparins and cholestyramine 40 whilst in rats subjected to hepatic injury (including partial hepatectomy and exposure to methapyrilene, dexamethasone, cyproterone, isoniazid and lead nitrate) indicated that GLDH increased 10 times greater than ALT elevations. 41
Cytokeratin-18 (CK18) is an intermediate filament protein found in the liver and functions as a major cellular structural component.42–44 CK18 has a potential to be used as a DILI biomarker because it is readily abundant in hepatocytes. Full length and cleaved forms of CK18 have been used in clinical research as DILI biomarkers and were found to be accurate and sensitive in diagnosing DILI as well as providing valuable information into the mechanism of hepatocellular injury when compared to traditional DILI biomarkers. 43 The challenge with CK-18 as a DILI biomarker is that very little research has been conducted to validate CK18 in preclinical DILI models. 43
A prospective study by Dear et al. analysed 2 clinical patient cohorts with acute liver injury concluding that a combined model of mirRNA-122, HMGB1, and K18 predicted risk of acute liver injury better than traditional biomarkers currently being used. 39 An exciting proposition and direction for future studies to aid causality assessment in human DILI would be a combination approach of predictive in-vitro cell systems with the novel mechanistic and hepatic selective prognostic biomarkers to be used in parallel with current tests. 23
In-vitro models for detecting DILI
The use of animals for toxicity testing has been criticized by organizations like the People for the Ethical Treatment of Animals (PETA) arguing that not all data collected from animal studies can be translated to humans. With arguments against the use of animals in preclinical toxicity testing, 3D cell culture models become a good interphase between 2D cell culture models and in-vivo animal models thereby reducing the number of animals used in toxicity testing. Although hundreds of in-vitro cell culture models (primary human hepatocytes (PHH), human liver microsomes, human cell lines, human liver slices, isolated perfused livers and human pluripotent stem cells derived hepatic cells, 45 have been developed, only a small group have been sufficiently validated to be accepted by national and international regulatory bodies necessitating the urgent need for conducting rigorous studies to validate in-vitro cell culture models supported by mechanistic evidence as animal alternatives. 46 In-vitro model for detecting DILI should be able to mimic the physiological environment of the liver, remain functionally stable over longer periods of time to support different toxicity testing scenarios such as single or repeated toxicity, low-dose chronic exposures or the addition of multiple cell types. 10 Advanced multicellular 3D in-vitro models have been developed to recapitulate the complex, intricate organ structure and active metabolic function that help to understand the pathophysiology leading to DILI in a natural exposure scenario. 10 There are a wide range of 3D in-vitro liver models available in the arena as described below.
Classification of 3D culture methods
3D cell culture models can be broadly classified into different categories i.e. scaffold-based technique (using hydrogels or structural scaffolds), scaffold-free technique (using freely floating cell aggregates, such as spheroids) and the hybrid system (includes scaffold base characteristics and external physical support).
Scaffold-based 3D technique
Scaffolds are cell culture technologies designed to support cell adhesion, cell-biomaterial interactions, adequate transport of gases and nutrients for cell growth and survival avoiding cell toxicity, 47 as well as providing physical support by using structures mimicking extra-cellular matrix (ECM) composition simulating the native cellular microenvironment enabling cells to aggregate, proliferate, and migrate. 48 The aim of a scaffold technology is to produce characteristics for the native cell function within the ECM that is biocompatible and characterizes the shape and function of the assimilated cell structure. 49 Scaffolds are manufactured from natural (fibrin, collagen, hyaluronic acid, silk, and gelatin) and synthetic materials (polymers, titanium, bioactive glasses, and peptides).50–53 The fabrication technique for scaffold synthesis depends on the size and surface properties of the material and recommended role of the scaffold. The relevant fabrication techniques for a particular target tissue must be identified to facilitate proper cell distribution and guide their growth into 3D space. Various techniques are used for scaffolds fabrication such as melt molding, gas foaming, fiber bonding, freeze drying, electrospinning, fiber mesh, micro molding, and solvent casting. Despite the tissue type, important factors to consider when designing the scaffold are biocompatibility, bioactivity, biodegradability, mechanical response, and scaffold architecture.54–56 Scaffold-based 3D technique can further be divided into solid-state scaffolds and hydrogels as described below.
Solid state scaffolds
Solid state scaffolds are made from materials such as ceramics, metals, glass, and polymers and are used for their ability to create organized positioning of cells in-vitro in a controllable and reproducible manner. 57 Cell adhesion, growth and behaviour in solid scaffold depends on factors such as scale and topography of the internal structure, material used for its construction, the surface chemical properties, permeability, and mechanical properties. 58
Hydrogels
Hydrogels are hydrated and hydrophilic polymer networks with pores mimicking natural ECM structure that is important for cell survival, proliferation, differentiation, and migration. 59 Hydrogels are one of the most used scaffolds substituting natural tissues, 60 mainly due to their potential to mimic natural ECM structure, soft and rubbery consistence, low surface tension and high-water content. 61 Hydrogels are made from natural materials such as collagen (most widely used), gelatin, alginate, fibrin, hyaluronic acid, agarose, chitosan, and laminin.62–64 Hydrogels made from natural materials have an advantage of having adhesive properties, high cell viability, controlled proliferation, and differentiation. Polyacrylic acid, polyethylene glycol (PEG), polyvinyl alcohol, polyglycolic acid (PGA) and poly (2-hydroxy ethyl methacrylate are some of the synthetic materials used to make hydrogels.65–67 Synthetic hydrogels mimic biological properties of ECM a property ideal for 3D scaffolds since they have well defined chemical, physical and mechanical properties to achieve stiffness and porosity. 68 Synthetic hydrogels have an advantage in that they have a long-life span, high gel strength and water absorption capacity. 69
Scaffold free technique
Scaffold-free systems have cells aggregating and self-assembling similar to what happens in a natural process of organogenesis. 70
Organoids
Organoids are in-vitro 3D multicellular aggregates capable of self-renewal, self-organization, and mimicking corresponding in-vivo organ functionality. 71 Organoids are used for studying aspects of corresponding in-vivo organ in a cell culture dish. 71 Organoids are produced from stem cells or primary tissues by providing suitable physical and biochemical signals. 72 Organoids are classified based on how the organ buds are created into tissue organoids (e.g. intestine, prostate, mammary and salivary glands) and stem cell organoids (e.g. embryonic stem cells or induced pluripotent cells). 73 Presently, different in-vitro organoids have been set to simulate numerous tissues such as functional organoids for pancreas, liver, intestine, kidney, and lung etc. Organoids can be obtained by culturing cells as a monolayer on an ECM coated surface with organoids being produced after the cells differentiate. The second is a mechanically supported cell culture to provide further differentiation of primary tissues. The third approach is to produce embryoid bodies through hang drop culture or on the low adhesion plates. 74 The main disadvantages of organoids are the lack of vasculature, lack of key cell types found in-vivo, and some organoids only replicate early stages of organ development. 71
Spheroids
Spheroids are 3D cell cultures arranged into sphere-like formations, deriving their name from hamster lung cells grown in suspension observed to be arranged in a nearly perfect spherical form. Spheroids naturally mimicking aspects of solid tissues, establish ideal physiological cell-to-cell interactions, cells form their own ECM components and better cell-ECM interactions and excellent gradient for efficient diffusion of growth factors as well as the removal of metabolic waste. 75 Spheroids have an advantage in that they can be analyzed by imaging using light fluorescence and confocal microscopy. There are different approaches for culturing spheroid as described below.
Hanging drop method co-culture used to generate tissue-like cellular aggregates for molecular and biochemical analysis in a physiological suitable model. The hanging drop method became the basis of the non-scaffold method for the formation of multicellular spheroids. In hanging drop method, cells are cultured in a drop of media suspended on the lid of a cell culture dish, which is carefully inverted and placed on top of the dish containing media to maintain a humid atmosphere. Suspended cells then come together and form 3D spheroids at the apex of the droplet of media. 76 This method has many advantages such as cost effectiveness, controlled spheroid size, and various cell types can be co-cultured and produced into spheroids.77,78 Moreover, it has been reported that 3D cell culture generated with hanging drop method have 100% reproducibility. 75 Due to limited volume of droplets generated with this technique, it is difficult to maintain spheroids and change the medium.
Low adhesion plates are spheroid microplates with round, V-shaped bottoms, and very low attachment surfaces to generate self-aggregation of cells and spheroid formation designed with hydrophilic or hydrophobic coating, which reduces cell from attaching to the surface. 79 Low adhesion plates are cost effective highly reproducible culture method, 80 with a potential to produce one spheroid per well making it appropriate for medium-throughput screening, as well as creating defined geometry suitable for multicellular culture. 81 These plates have initial higher volume capacity than hanging droplets and there is no need to manipulate the spheroids.
Spheroids cultured using bioreactors under specific dynamic conditions, 82 can be generated by stirring or rotating using spinner flask or National Aeronautics and Space Administration rotating wall vessel, respectively. 83 Bioreactors provide greater spheroid production control and reproducibility. 84 However, production of spheroids through this method requires expensive instruments and high-quality cell culture medium.
An overview of 3D hepatic cell-based models previously used for studying drug induced liver injury.
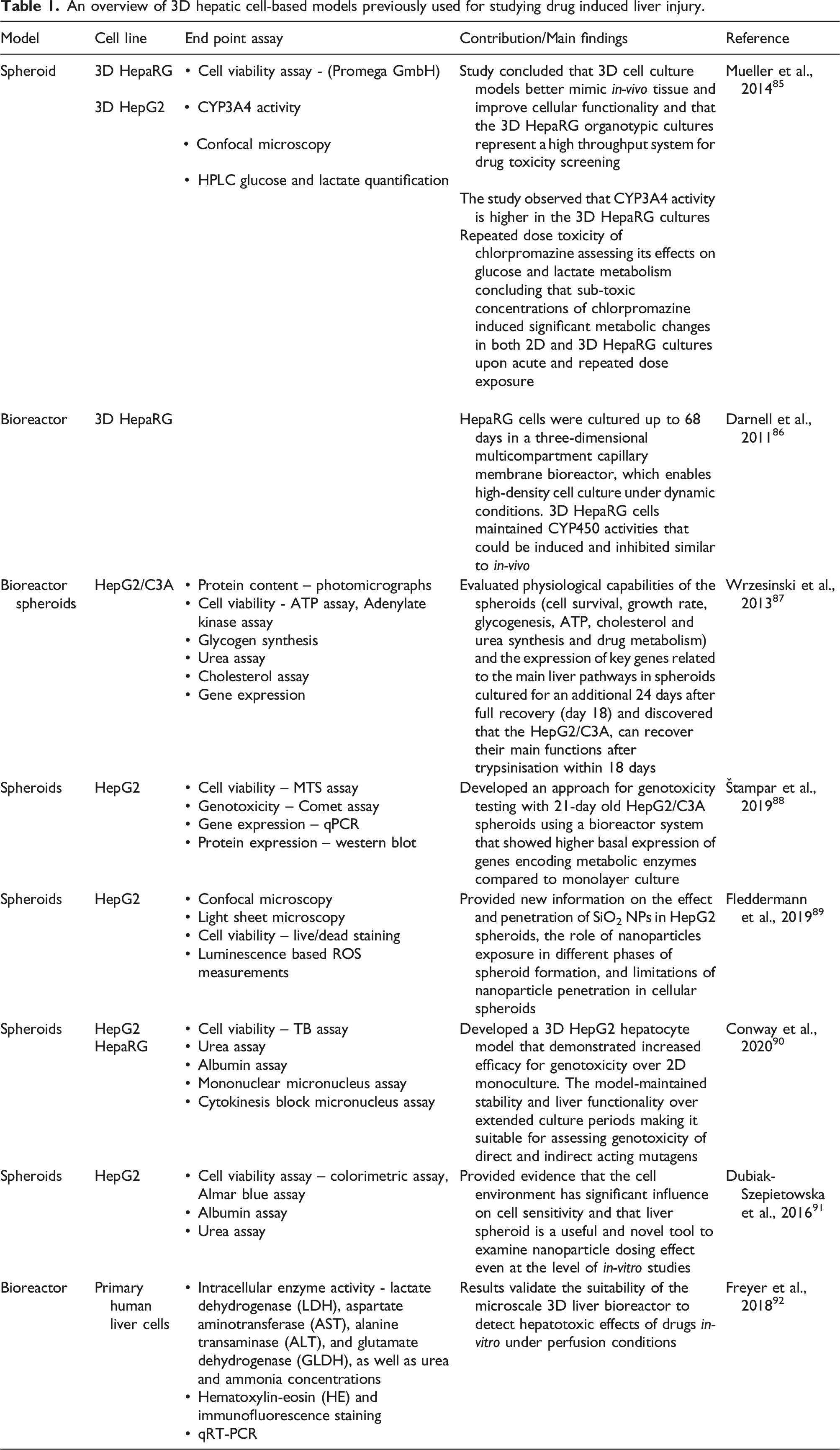
Mueller et al. tested the toxic effects of four drugs (aflatoxin B1, amiodarone, valproic acid and chlorpromazine) using a 3D HepaRG and 2D HepaRG and concluded that 3D cell culture models better mimic in-vivo tissue and improve cellular functionality and 3D HepaRG organotypic cultures represent a high throughput system for drug toxicity screening. 85 This makes the 3D HepaRG a promising tool in preclinical testing for early detection of DILI allowing the reduction of animals used in preclinical testing. The study has shown that 3D HepaRG cultures are more sensitive than the other tested cultures to aflatoxin B1 which is only toxic upon metabolic activation in the liver. The same study observed that CYP3A4 activity is higher in the 3D HepaRG cultures like the findings of Darnell et al., in a 3D bioreactor where HepaRG cells maintained CYP450 activities that could be induced and inhibited similar to in-vivo. 86 Mueller et al., investigated repeated dose toxicity of chlorpromazine assessing its effects on glucose and lactate metabolism concluding that low concentrations of chlorpromazine induced significant metabolic changes in both 2D and 3D HepaRG cultures upon acute and repeated dose exposure. 85 It was concluded acetaminophen-induced mechanism of toxicity in HepaRG cells is similar to animal models and humans, indicating this cell line is a good in-vitro model for studying hepatotoxicity. 18
Limitations of 3D cell culture technology in detecting DILI
Challenges remain with 3D cell culture technologies as a model for early detection of DILI due to 3D cell cultures having differences in terms of size, morphology, complexity, and protocol for assaying compared to 2D cell culture.100,101 Limited permeability impacts cell viability and functions making it difficult to have accurate automated system for high throughput screening. 100 For example, the addition of matrices or scaffolds creates a barrier that drug compounds may not be able to traverse, thereby preventing appropriate exposure of the test material to the target cells leading to dosimetry inaccuracies and uncertainty concerning the actual drug compound concentrations applied to the culture. 10 Spheroids form necrotic cores that impact drug toxicity testing; however, this challenge can be addressed by use of imaging techniques e.g. bright field, phase contrast, and fluorescence microscopy. Another limitation with in-vitro 3D liver models is that they are formed from static, non-dividing, fully differentiated cells, a factor which limits genotoxicity assessment where actively dividing cells are required. There is no 3D in-vitro liver model capable of detecting secondary genotoxicity mechanisms such as those induced by a chronic inflammatory response that is a major factor in the pathogenesis of DNA damage associated with drugs exposure in-vivo. 102 A major challenge with cell culture as models for detecting DILI has been the limited amount of time cells can survive in-vitro, which only makes cell culture models suitable for acute toxicity testing. 92 Although 3D models have been used for up to 68 days in a bioreactor, 86 the challenge of cell survival remains as the cells can’t survive beyond the 68-day period a factor that limits the use of 3D cell culture models for detecting long term exposure to hepatotoxins. Cell lines used for 3D models may have a challenge in enzyme expression for example the HepG2 cells have low levels of CYPs and normal levels of phase II enzymes except for UGTs, 103 making them suitable for detecting toxicity of parent compound but less likely to detect toxicity of the parent compound metabolites.
3D cell culture technology prospects in drug development
The 3D cell culture technology has great potential in finding solutions researchers have traditionally missed during drug discovery and toxicology as well as other areas leading to new product development thereby bridging the gap between 2D cell culture methods and animal models. More research on 3D cell technology is being driven by the need to develop alternatives to animal testing that can be attributed to the increasing initiatives to replace, reduce, and refine use of animals in experiments.
3D cell culture is currently used by stem cell researchers, and this trend is expected to continue in future as this technology can be used for testing efficacy of stem cell derived therapies in regenerative medicine. Pluripotent stem cells have been successfully used to develop organoids that have a potential to be used as a source of tissue for transplantation. 104 3D technology has a profound use in cancer research, for example in future 3D tumor panels for various cancer indications can be developed and used to understand tumor pathology, metastasis, and treatment. 105 In the future, organoids will help uncover the pathogenesis of many diseases when used as disease models for example organoids have a potential to be used as genetic disease models for neurodegenerative diseases such as Alzheimer. 106 In future, drugs can be tested on organ on a chip derived from spheroids for example the lung/liver-on-a-chip that was made by connecting liver spheroid cultures with a 3D organotypic bronchial model. 107 The gastrointestinal and liver on a chip model was found to have a potential to eventually lead to personalized medicine because patient-derived cells can be used. 108 3D culture models using human cells have an advantage in that they prevent the use of animal models which at times lead to incorrect conclusions about drug efficacy and side effects.11,108
Despite the potential and envisioned use of 3D cell technology in future, lack of infrastructure and high costs of setting up may hamper the pace at which some of the technologies described above are developed and validated.
Conclusion
Despite the limitations of 3D cell culture technology, it is evident that 3D cell culture systems hold great potential for early detection of DILI due to their improved cell-cell and cell-ECM interactions, cell populations and structures similar to in-vivo models. 3D cell culture models have detected traditional DILI biomarkers such as AST, ALT, GGT and ALP successfully. This makes it easy to extrapolate 3D cell culture results to humans without worrying about the discrepancy of differential expression and activity of drug metabolizing enzymes which makes 3D cell culture a good interphase between 2D cell culture models and in-vivo animal. Although traditional DILI biomarkers have been successfully detected, tests must be validated for in-vitro detection of new DILI biomarkers such as the HMGB1, GLDH, miRNA and Keratin 18.
Footnotes
Acknowledgements
The content hereof is the sole responsibility of the authors and does not necessarily represent the official views of the National Research Foundation (NRF) of South Africa.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Y Ntamo is a postdoctoral research fellow, funded by the National Research Foundation (NRF) of South Africa.