
Abstract
Drug induced liver toxicity is a serious health complication leading to high mortality rates and post marketing withdrawal of drugs. Although considered to be the gold standard biomarkers; aspartate aminotransferase, alanine aminotransferase, total bilirubin and alkaline phosphatase have been found to have specificities beyond liver, therefore more specific and predictive markers for the detection of antitubercular drug mediated liver damage are required. Unfortunately, the effectiveness of currently used first line antitubercular drugs namely isoniazid, rifampicin, pyrazinamide is often accompanied with liver injury, impeding the cure of patients. Keeping in view, the prognostic and diagnostic applications of microRNAs in various diseases, we tried to assess the importance of microRNAs 122 and 192 in antitubercular drug associated liver injuries. The study included subjects having tuberculosis of any type with antitubercular drug induced liver injury; naïve or newly diagnosed tuberculosis patients, tuberculosis patients on drugs not having toxicity and healthy controls. Observations from this study revealed that expression levels of miR-122 and miR-192 were significantly decreased in the serum of antitubercular drug induced liver injury patients only. Therefore, these microRNAs or the pathways associated with them can be used as a tool to predict or cure antitubercular drug associated liver injury in future.
Introduction
Drug induced liver injury (DILI) is the major concern which limits the clinical use of many important drugs. It is the major cause of acute liver damage and the post marketing withdrawal of many drugs.1,2 DILI may be caused by drugs or their metabolites affecting liver cells, biliary epithelial cells, and/or liver vasculature. Adverse effects experienced by the patients compel them to discontinue the drug treatment thus facilitating emergence of drug resistant tuberculosis. Antitubercular drugs (ATDs) mainly isoniazid (INH), pyrazinamide (PZA) and rifampicin (RIF) are responsible for causing hepatotoxicity. From the past 50 years, serum alanine aminotransferase (ALT) level, the gold standard biomarker has been used as an indicator of the liver damage. 3 Liver is enriched with ALT and during hepatocellular injury, their levels in serum are increased reflecting its release from injured cells. Raised ALT levels in serum samples of patients has been associated with hepatic inflammation, steatosis and necrosis as well. 4 However, around 40% of human drug induced liver injury cases were not detected in preclinical studies in general, whereas antitubercular DILI attributed to at least 13% of acute liver failure cases, 2% of jaundice and approx 30% of fulminant liver failure cases. 5 Despite its important role in clinical monitoring, ALT lacks the characteristics of an ideal biomarker for liver injury. It has specificity beyond liver, as high levels of ALT are also present in heart, skeletal muscle, kidney and pancreas as well. 6 Also, elevated serum ALT levels can increase due to muscular damage following exercise or myocardial infarction.7,8 Apart from this, it was also observed that ALT gene can be induced by enzymes under various metabolic stress conditions like diabetes mellitus, starvation and during treatment with drugs which alters metabolism. Moreover, ALT levels were found to be less comparable with preclinical histopathological data, thus making the interpretation of human clinical data more complicated, since liver tissue is not usually available. 9 Therefore, along with this classical biomarker, additional biomarkers which bring concordance among clinical and preclinical studies are needed. Biomarkers, which can assess drug induced liver damage at an earlier stage than ALT levels, as well as which serves as a potential candidate for the diagnosis and prognosis, would be helpful for clinical evaluation of DILI. Recently described putative translational candidate biomarkers of drug mediated liver damage are microRNA 122 (miR-122) and microRNA 192 (miR-192). Because of their abundance and stability in biofluids, circulating microRNAs have emerged as favorable biomarkers for clinical evaluation of a disease.10,11 It has been reported that expression of specific miRNAs at tissue levels correlates with pathological development of some cancers.12,13 Previous studies have shown that certain miRNA species like microRNA 122 and microRNA 192 are abundant in liver. These microRNAs exhibit drug dosage and treatment duration dependent changes in plasma levels that correlates with the levels of ALT and liver degeneration histopathology. 14 Both up as well as downregulated expression of liver specific miRNAs has been reported under various drug induced liver injury conditions,14–18 however limited literature is available on the association of these microRNAs with antitubercular drug induced liver injury. Among the first line antitubercular drugs, INH is the most effective chemoprophylactic and treatment drug but its metabolic intermediate hydrazine (HzN) causes liver toxicity and peripheral neuritis.19–22 Daily administration of INH leads to asymptomatic transaminase elevations which can be fatal if not detected early and requires immediate therapy interruption. 23 In this study, the potential of novel DILI biomarkers i.e. miR-122 and miR-192 was investigated in tuberculosis patients on treatment with first line antitubercular drugs.
Materials and methods
Selection of study subjects and design
Venous blood samples were collected from 50 subjects in each of the respective groups: group I-Healthy controls (individuals from medical outpatient department who attend it for health and were found to be healthy or from patient’s spouses and hospital staff), group II-naïve or newly diagnosed tuberculosis patients (subjects having tuberculosis of any form) not started antitubercular drugs, group III-tuberculosis patients having no hepatotoxicity and were on ATDs therapy for at least one week (≤ two-fold rise in ALT levels) and group IV-toxic TB subjects having ATD induced hepatotoxicity (serum ALT or AST ≥ two-fold rise than normal range in presence or absence of signs and symptoms). Study subjects provided written informed consent were recruited in the study and the use of human blood sample was reviewed and approved by the Institutional ethical committee (IEC) PGIMER, Chandigarh (IEC-10/2014-72). Patients recruited in the study were of either sex in the age group of 15–65 years. The tuberculosis patients were on antitubercular drug (ATD) therapy essentially with INH, PZA and RIF and were having ATD induced hepatotoxicity according to WHO definition of toxicity (serum ALT or AST more than two times the normal range in presence or absence of signs and symptoms). Diagnosis for tuberculosis was done by history, chest X-ray, sputum for acid fast bacilli, Mantoux test or microscopic examination performed by concerned physician attending medical and chest clinic of Outpatient Department, PGIMER, Chandigarh, India. Five milliliter of venous blood from each subject was collected in serum collection tubes, serum was separated by centrifugation which was aliquoted into microfuge tubes and stored at −80°C till further use. Anthropometric measurements like body mass index was also recorded. Patients with viral hepatitis, HIV infection, pregnancy, long-term alcoholism (i.e. 148 g alcohol consumption per day for at least 1 year), simultaneous consumption of other hepatotoxic drugs (e.g., valproate, phenytoin, methotrexate and fluconazole) and failed to give written informed consent were excluded from the study.
Biochemical analysis
Peripheral blood samples were taken from the patients and serum was separated by centrifugation. Serum samples were used for analysis of routine liver function parameters viz. alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase (ALP), gamma-glutamyltransferase (GGT) and total bilirubin (TBIL) on random access auto analyser (Beckman Coulter AU5811) using standard kits for quantifying and grading the severity of hepatotoxicity.
Analysis of drug levels by HPLC
For serum drug (INH, Acetylated Isoniazid (AcINH), PZA and RIF) estimation, the high-performance liquid chromatography (HPLC) system was used that was equipped with dual-piston reciprocating pump, UV/Visible detector, an online degasser and series 200 autosampler (Perkin Elmer Instruments, Shelton, CT, USA). Standard AcINH was synthesized by reacting isoniazid with acetic acid and its purity was confirmed by NMR and HPLC as described by Moussa et al. (2002). INH, PZA and AcINH were quantified in 100 µL protein free serum filtrate using C18 column (250 mm × 4.6 mm I.D., 5 µm particle size, Waters) and mobile phase containing 0.05 M ammonium acetate (pH 6.0) and acetonitrile (ACN) (99:1) with a flow rate of 1.0 mL/min and detected in the UV/Vis range at 275 nm. 24 Rifampicin was quantified simultaneously using C18 column and mobile phase consisting of 0.05 M Potassium dihydrogen phosphate (pH3.7) and Acetonitrile (52:48) with a flow rate of 1.0mL/min, and detection was done in the UV/Vis range at 335 nm. 25
MicroRNA isolation from serum
Total RNA, including microRNA was isolated from 200 µl serum taken from patients in all the four groups, following the manufacturer’s instructions using miRNeasy microRNA isolation Kit (Qiagen, Sollentuna, Sweden). Briefly, 5 volumes of Qiazol lysis reagent were added to the serum sample, mixed by pipetting gently and were incubated at room temperature (15–25°C) for 5 min. Then chloroform in equal volume to the starting sample was added and incubated at room temperature for 3 min. Samples were centrifuged for 15 min at 12,000 × g and 4°C, and upper aqueous phase was carefully separated. 1.5 volumes of 100% ethanol were added to the aqueous phase and loaded on the miRNeasy Min Elute spin column. Columns were then centrifuged at ≥8000 × g for 15 sec, further washing buffers were added with corresponding centrifugation steps. Flow-through was discarded and 80% ethanol was added to each column followed by 2 min centrifugation at ≥8000 × g. Total RNA including microRNA was eluted with RNAase free water. RNA concentration was quantified using spectrophotometer and equal quantity of RNA from each sample of a subject was converted to cDNA.
Expression analysis of miR192 and miR122
MicroRNA was reverse transcribed to cDNA using miRNA first strand cDNA synthesis Kit (Agilent Technologies, Inc., Santa Clara, CA), according to the manufacturer’s protocol. The protocol includes the polyadenylation of the miRNA followed by its conversion to cDNA. MicroRNA expression was quantified in serum by SYBR® Green chemistry based qPCR with SYBR green Universal PCR Master Mix (Roche) using specific set of forward primers for miR-122: 5’-TGGAGTGTGACAATGGTGTTTGT-3’ and miR-192: 5’-CTGACCTATGA ATTGACAGCC-3’ and universal reverse primer provided with the cDNA synthesis kit. The relative expression levels of miR-122 and miR-192 were normalized with U6 small nuclear RNA (U6 snRNA) and its primers for qPCR were 5’-CGCTTCGGCAGCACACATATACTAA-3’ (forward) and 5’-TATGGAACGCTTCACGAATTTGC-3’ (reverse). qPCR was performed on the Roche LightCycler® 96 RTPCR System: preincubation at 95°C for 10 min followed by amplification process of 43 cycles at 95°C for 10s and 60°C for 20s. The cycle threshold (CT value) was determined with instrument default threshold settings. Relative quantitation of target miRNA expression was estimated by using the comparative CT method (ΔΔCT) (Livak and Schmittgen, 2001) 26 which determines the relative target quantities in samples. Measurements were normalized using the endogenous control. Briefly, the ΔCT value was obtained by deducting the CT value of target from its respective U6snRNA (reference) CT value. Then ΔΔCT value was calculated by subtracting the mean ΔCT value of control sample from the mean ΔCT value of test sample. Fold change in the expression of the target microRNA is equivalent to 2−ΔΔCT.
Statistical analysis
One-way ANOVA was used to compare the biochemical parameters and miRNA expression in serum samples of various groups. Statistical Package for the Social Sciences (SPSS) software and Graphpad prism (V 8.0) were used for the statistical analysis. p value ≤0.05 was considered statistically significant.
Results
Drug analysis in serum samples of tuberculosis patients on antitubercular drugs
Demographic details of the subjects included in the study showed that mean age of untreated or naïve TB group was 27.22±8.6 years, 25.17±7.2 years for nontoxic group, 30.83±10.67 years for toxic group and 26.72±3.5 years for healthy control group. Other anthropometric measurements including BMI and gender ratio are mentioned in Table 1. Cohort of 200 subjects were divided into respective groups based on the exclusion and inclusion criteria of the study. Patients having antitubercular drug induced liver toxicity showed significant elevation of liver function markers i.e. ALT, AST, ALP and TBIL levels when compared to healthy controls, naïve TB patients and nontoxic TB patients (Figure 1). Further, serum levels of antitubercular drugs in tuberculosis patients on therapy with or without drug induced liver injury were evaluated by HPLC to find out the correlation of DILI with drug levels. Results showed the retention time for isoniazid, acetylated isoniazid, pyrazinamide and rifampicin was 8.5 min, 7.1 min, 11 min and 4.6 min respectively. The results showed that out of 50 nontoxic patients, the INH levels were detected in 46 patients with drug concentration of 4.6±2.6 µg/mL, AcINH in 42 patients with drug concentration of 4.1±2.6 µg/mL and rifampicin in 47 patients with drug concentration of 4.8±1.6 µg/mL. However, in case of toxic group, INH was detected in 46 patients with drug concentration of 2.4±1.7 µg/mL, AcINH in 42 patients with drug levels of 6.4±3.1 µg/mL and RIF in 46 patients with drug concentration of 3.3±2.0 µg/mL. Upon comparison of samples from each group, it was observed that group III and group IV patients did not have any significant difference in AcINH and RIF drug levels while INH levels were found to be decreased in DILI patients (group 4) as compared to the non-DILI patients (group 3) (Table 2).
Demographic details of subjects of different study groups.
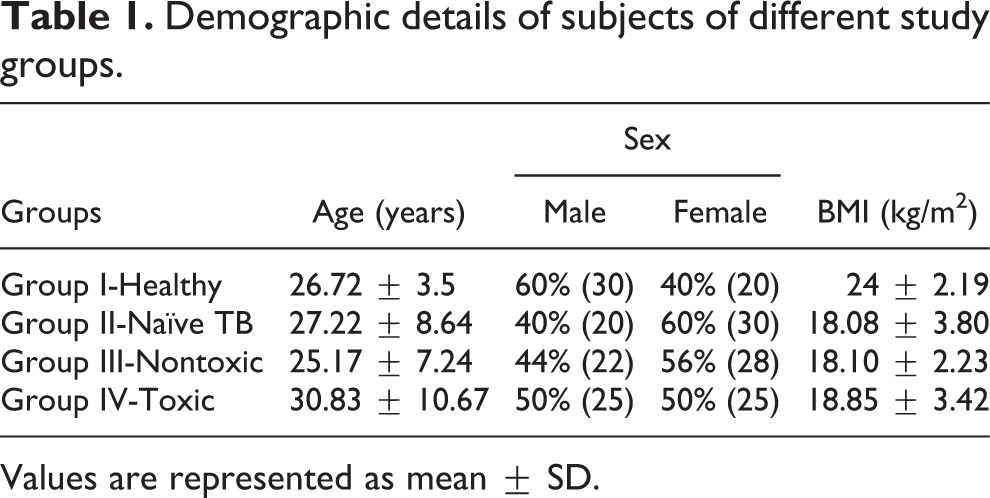
Values are represented as mean ± SD.

Comparison of AST, ALT, ALP and TBIL values of toxic patients (group IV) with different groups (Box plot distribution). Levels of ALT, AST, ALP and TBIL were found to be significantly increased in toxic patient group as compared to healthy, naïve TB patients and nontoxic TB patients. ***p < 0.001.
INH, AcINH and RIF levels in tuberculosis patients with or without drug induced liver injury.

Values are represented as mean ± SD.*p < 0.05 when compared with group 3 (nontoxic group).
Effect of antitubercular drug therapy on miR-122 expression
Further, expression of liver specific miR-122 was studied in serum collected from different study groups with U6snRNA as internal control. The results showed that miR-122 level was significantly decreased by 75% in DILI patients (group 4) when compared to healthy controls. Also, when antitubercular drug induced liver toxicity subjects were compared with naïve tuberculosis patients, the expression of miR-122 was found to be significantly decreased. Further, when comparison was done between nontoxic tuberculosis patients and tuberculosis patients having ATD induced hepatotoxicity, a significant reduction in miRNA expression by 73.7% was observed in the latter (Figure 2(a)). A comparison of miR-122 expression levels with the ALT levels individually in 50 patients of both the group 3 and group 4 showed decreased expression of miR-122 with the increase in the ALT levels in group 4 (DILI patients) but in group 3 patients, no decline in the expression was observed under normal ALT levels (Figure 2(b), 2(c)). Expression of miR-122 was also evaluated with respect to ALT levels raised up to 200 U/L and greater than 200 U/L in group 4 patients, just to observe the pattern of miRNA expression with the increased ALT levels (Figure 2(d)).

Fold change in the expression of miRNA 122 in AT-DILI patients. Comparison of the fold change in the expression of miRNA122 in group 4 versus group 1, 2 and 3 in an individual patient value plot (a). Values are represented as mean ± SD. ****p < 0.0001. miR-122 expression was also compared with the ALT levels of individual patients in the group 3 (b), group 4 (c) and with the group of toxic patients having ALT ≤ 200 U/L and >200 U/L (d). Graphpad prism V 8.0 software was used for statistical analysis.
There was an overall decrease in the expression of miR-122 in the toxic patients when compared to other three groups. Similar decrease in the expression of miR-122 was observed with further increase in the ALT levels above 200 U/L in toxic patients.
Effect of antitubercular drug therapy on miR-192 expression
The effects of antitubercular drug treatment on the levels of miR-192 in serum samples of patients was studied in patients grouped under various categories. The miR-192 levels were found to be significantly decreased by 75.6% in patients having antitubercular drug induced liver toxicity as compared to healthy subjects. Also, significant decline in miR-192 levels in case of ATD induced liver injury was observed when compared with naïve tuberculosis patient samples. Further, when nontoxic patient group was compared with liver injury patients, latter group showed significant decrease of 76.2% in miR-192 expression (Figure 3(a)). A comparison of miR-192 expression levels were made with the ALT levels individually in 50 patients of both the group 3 and group 4; decrease in the expression of miR-192 was observed with the increased ALT levels in group 4 but no such decrease was observed in group 3 patients (Figure 3(b), 3(c)). Further decrease in the expression of miR-192 was observed with the increase in the ALT levels above the 200 U/L in toxic patients (Figure 3(d)).

Fold change in the expression of miRNA 192 in AT-DILI patients. Comparison of the fold change in the expression of miRNA 192 in group 4 versus group 1, 2 and 3 in an individual patient value plot (a). Values are represented as mean ± SD. ****p < 0.0001. miR-192 expression was also compared with the ALT levels of individual patients in the group 3 (b), group 4 (c) and with the group of toxic patients having ALT ≤ 200 U/L and >200 U/L (d). Graphpad prism V 8.0 software was used for statistical analysis.
Discussion
The combined four-drug regimen, isoniazid (INH), rifampicin (RIF), pyrazinamide (PZA) and ethambutol (EMB) is used for the treatment of active tuberculosis, out of these four the first three drugs are reported to have hepatotoxic effect in TB patients.23,27,28 The most widely used indicator of ATD induced liver injury till now is more than two-fold rise in ALT levels and dosage discontinuation has been found to cause fall in ALT levels, 29 ultimately leading to therapeutic hindrance and increased susceptibility for developing resistant strains. The currently used standard biomarkers for the detection of ATD induced liver damage are serum ALT, AST, ALP and TBIL. Increased serum ALT levels were also found to be associated with other organ toxicities, which suggests the nonspecificity of the enzyme with respect to liver damage. Also, studies have documented that ALT levels were found to be ineffective for the detection of hepatic necrosis produced by acetaminophen. 30 To evaluate the risk of false positivity attributed by non-specific serum ALT levels, additional circulating biomarkers with enhanced liver specificity are needed. Apart from being known as major intracellular regulatory molecules for various gene expression networks, certain microRNAs are emerging as biomarkers for determining certain pathological conditions. MicroRNA are post-transcriptional modulators of >60% of human protein-coding genes.31,32 Reports have shown that microRNA has comparable stability in biofluids and tissues thus making them a suitable candidate in the biomarkers list. 10 Recent findings suggest that circulating microRNAs hold the potential for being specific and sensitive biomarkers for detection of various types of cancers like breast, 33 colorectal 34 and prostate, 35 therefore, the identification of miRNAs as specific and sensitive markers to the liver would be of immense help. Till date, only few studies have been carried out regarding the expression of microRNAs in antitubercular drug induced hepatotoxicity. In a study conducted by Wang et al. (2009) in mice model of hepatoxicity, expression of liver specific miRNAs (i.e. both miR-122 and miR-192) signifies their potential as favorable circulating biomarkers of acetaminophen (N-acetyl-p-aminophenol; APAP) mediated acute liver injury. 14 A study performed using mouse model of hepatotoxicity showed that during CCl4 and acetaminophen mediated acute liver toxicity, expression of miR-122 and miR-192 was found to be significantly increased and remained as such till 24 h of the treatment, and a decline to normal levels were observed after 72 h. 36 Also, miR-122 expression was found to be highly abundant in the liver but absent in other tissues. Among microRNAs, miR-122, shares approximately 70% of the total microRNA pool present in the adult liver 37 and is involved in various important liver functions i.e. maintenance of liver biology, homeostasis that includes cell cycle progression, and in certain diseases like hepatocellular carcinoma, 38 metabolism of lipids 39 and tissue fibrosis. 40 Furthermore, miR-122 has been proposed as a potent biomarker for the diagnosis of hepatotoxicity caused by APAP treatment 41 and alcohol consumption. 42 Also miR-122 and miR-192 possess high serum or plasma expression levels upon drug induced liver damage even much earlier than liver enzymes expression (ALT and AST), thus indicating their potential to be considered as suitable biomarkers of liver toxicity.14,43 Therefore, in order to fill the gap in the research area of ATD induced liver injury diagnosis, we screened the expression of microRNA 122 and microRNA 192 by qRT-PCR in all the 4 groups i.e. healthy (group I), naïve TB patients (group II), TB patients on antitubercular drug therapy with normal ALT levels (group III) and TB patients on ATD with > two-fold rise in ALT levels (group IV). The observations indicated increased hepatic injury in tuberculosis patients on antitubercular drug therapy. These findings were supported by a Korean study conducted by Jeong et al. (2015) in the cohort of 195 TB patients out of which 17 TB patients were found to have elevated liver function parameters. 44 Another study by Abera et al. (2016) which included 124 TB patients, showed that only 8% of the TB patients developed drug induced hepatotoxicity as reflected by five times elevation in the upper reference limits of AST and ALT. 45 Further for each drug the therapeutic levels in serum has been defined between 3–6 µg/ml for INH and 8–24 µg/ml for RIF46,47 but, our study showed lower INH and RIF serum levels which were below the therapeutic range and hence were not true reflection of liver injury. Tostmann et al. (2013) revealed that in 20 adult Tanzanian tuberculosis patients with varying HIV status, 53% had INH and 35% had RIF levels below the therapeutic range in the sera. 47 Heysell et al. (2010) have demonstrated that out of total patients recruited in the study, only 60% patient’s sera had INH and RIF within therapeutic range. 48 Interestingly, Park et al. (2016) observed that low antitubercular drug levels did not affect patient’s response to TB treatment. 49 Another reason for variable drug levels could be gene polymorphism in drug metabolizing genes. A study by Kumar et al. (2017) comprising 326 TB patients genotyped as slow (58%), intermediate (35%) and fast acetylators (7%) showed varying levels for INH well below the therapeutic range (i.e. 4.1µg/ml). 50 Therefore, NAT1/2 gene polymorphism can affect the drug metabolizing status. 51 Another study by Toure et al. (2016) demonstrated that in 96 Senegalese TB patients, NAT 2 genotyping played a vital role in phenotypically reflecting the INH or AcINH levels in serum. 52 This study for the first time unraveled that microRNA 122 and microRNA 192 can be considered as potent biomarkers for ATD induced hepatic injury diagnosis. Here we report that tuberculosis drugs mainly first line drugs (INH, RIF and PZA) leads to significant downregulation of miR-122 and miR-192 expression in case of ATD induced hepatotoxicity. Similarly decrease in the expression of both the miRNAs were also observed with the further increase in the ALT levels ≥200 U/L in toxic patients. Although considered to be the potent biomarkers, it still remains controversial whether the levels of these microRNAs are upregulated or downregulated in the circulation during liver injury. miR-122 levels were found to be decreased in the serum of patients suffering from hepatic decompensation and hepatorenal syndrome. 53 In a study carried out by Ding et al., 2012, levels of miR-122 was found to be lowered in 40% of the total hepatitis patients studied. Serum levels of microRNA 122 and microRNA 192 have been found to be downregulated in case of hepatitis B infections and cirrhosis 15 which is supported by a proposed link between microRNA 122 and IFN signaling indicating that suppression of miR-122 leads to inactivated IFN expression which enhances HBV replication. 54 MicroRNA 192 but more significantly microRNA 122 were found to be downregulated in the serum samples during various carcinomas including hepatocellular carcinoma,gliomas and lymphomas indicating their role in cell cycle regulation.55,56 Downregulated expression of miR-122 observed in tuberculosis patients with liver injury is further supported by the earlier observations of Jopling et al., 2012 suggesting that miR-122 may act as an indicator of damaged hepatocytes possibly because of its altered expression under normal physiological conditions vs liver injury. 16 Lardizabal et al. (2014) reported that reduced tissue expression of miR-122 is attributed to decreased transcription of its precursor, which is associated with the reduced expression of transcription factors C/EBP and HNF4 (transcription factors for miR-122) and is a sign of liver regeneration and repair.57–60 In addition, it has been reported that increased methylation of miR-122 leads to its decreased tissue expression and upregulation of miR-122 gene targets (cell cycle protein G1 and cationic amino acid transporter-1) upon isoniazid induced liver injury in rats, thus suggesting the role of decreased miR-122 levels in the regulation of cell proliferation and repair of damaged liver tissue. 17 Epigenetic modifications induced upon drug administration could be the possible reason for the decreased tissue expression of miR-122 as reflected by its decreased serum/plasma levels. Expression of another liver specific microRNA i.e. miR-192 was also found to be significantly downregulated during antitubercular drug induced liver toxicity in our study when comparisons were drawn between TB patients having liver injury due to ATDs (group IV) vs. healthy (group I), naïve TB patients (group II), TB patients who were on ATDs but did not have any toxicity (group III). The results were supported by a study where miR-192-5p expression has been shown restricted to hepatic cells and expression of miR-192-5p was found to be decreased in CCl4 induced liver toxicity. In a same study, the result of functional experiment revealed that decreased miR-192-5p expression was associated with protection of HepG2 cells upon H2O2 treatment, suggesting its role in preventing liver toxicity. 18 In a study carried out by Jarsiah et al. (2019), however the expression levels of microRNA 192 and 122 were found to be increased in the plasma after 1 h of acetaminophen injection but levels of microRNA 192 reverted back to the control levels after 3 h, indicating the link between microRNA levels and time duration after drug exposure. 61
Concluding remarks
This pilot study reveal that anti tubercular drug induced liver injury is associated with decreased expression of liver specific microRNAs i.e. miR-192 and miR-122 which can be considered as potential targets to fully understand the mechanism of hepatotoxicity. However these microRNAs needs to be validated in larger population to further establish their potential role in the diagnosis and better management of hepatic injury induced by antitubercular drugs.
Footnotes
Author contributions
Sadhna Sharma and Shikha Bakshi conceived, designed, and analyzed the experiments. S Bakshi performed the experiments and wrote the manuscript. Neha Saini and Maninder Kaur has equal contribution in preparation of the manuscript and Altaf Ahmed assisted in experimental work. S Sinha and Ajay Duseja helped in the patient recruitment and study design.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We want to acknowledge Indian Council of Medical Research (ICMR), New Delhi, India for providing financial assistance to carry out this research work.