
Abstract
Introduction
The present study was undertaken to investigate the prognostic value of the frontal QRS-T angle associated with adverse cardiac outcomes in patients with carbon monoxide (CO) poisoning in early stages in the emergency department.
Materials and methods
The data of 212 patients with CO poisoning who were admitted to the ED between January 2010 and May 2020 were retrospectively analyzed. The frontal QRS-T angle was obtained from the automatic reports of the EKG device.
Results
Compared to patients without myocardial damage, among patients with myocardial damage, statistically high creatinine, creatine kinase MB, cardiac troponin I, and frontal QRS-T angle values were found (p < 0.001 for all parameters), while the saturation of arterial blood pH and arterial oxygen values were found to be lower (p = 0.002 and p < 0.001, respectively). The frontal QRS-T angle values were correlated with creatine kinase, creatine kinase-MB, cardiac troponin I, and oxygen saturation (SpO2) in arterial blood (r = 0. 232, p = 0.001; r = 0. 253, p = < 0.001; r = 0. 389, p = < 0.001; r = −0. 198, p = 0.004, respectively). The optimum cut-off value of the frontal QRS-T angle was found to be 44.5 (area under the curve: 0.901, 95% confidence interval: 0.814–0.988, sensitivity: 87%, specificity: 84%).
Conclusions
The frontal QRS-T angle, a simple and inexpensive parameter that can be easily obtained from 12-lead surface electrocardiography, can be used as an early indicator in the detection of myocardial damage in patients with CO poisoning.
Introduction
Background
Carbon monoxide (CO) is an odorless, tasteless, colorless, non-irritating gas emitted due to the incomplete combustion of organic compounds. 1 The clinical severity of CO poisoning depends on the amount of gas ventilation absorbed, the exposure time, the environmental concentrations of O2 and CO, and the general health of the affected person.
Although CO poisoning is harmful to all the organs and systems, the primary target organ systems for CO poisoning are the central nervous system and heart, as they are the most dependent on oxygen. 2 Thus, effects of CO manifest through tissue hypoxia or/and direct cell damage. It has long been known that myocardial damage is related to CO poisoning, which subsequently leads to electrical, functional, and morphological changes in the heart. Therefore, left ventricular dysfunction and electrocardiography (ECG) changes are common in patients with CO poisoning.3–6 However, cardiac damage due to CO poisoning may be silent in some patients.7,8
The prognostic value of the frontal QRS-T angle, which is a useful ECG measure of the dispersion between depolarization (QRS axis) and repolarization (T axis), has recently become an area of research interest and has been studied extensively to assess the severity of cardiac damage in different populations. 9 The frontal QRS-T angle as a useful ECG measure of the dispersion between depolarization (QRS axis) and repolarization (T axis) is crucial in assessing the severity of cardiac damage.
Moreover, an association between increased spatial QRS-T angle and higher mortality in the general population has been demonstrated. Although spatial QRS-T angle can be calculated based on specialized software from ECG, no special software is required to calculate the frontal QRS-T angle from a routine 12-lead ECG. As previously reported, frontal and spatial QRS-T angles are comparable, and there is a strong correlation between them. 10 Recently, the frontal QRS-T angle has emerged as a powerful predictor of long-term mortality in patients with left ventricular systolic dysfunction after an acute myocardial infarction.11–14
Although the increased frontal QRS-T angle predicts mortality in different populations with a higher risk of cardiovascular diseases, no previous studies investigate the association between adverse cardiac outcomes and increased frontal QRS-T angle in patients with acute CO poisoning.
Therefore, the present study was undertaken to investigate the prognostic value of the frontal QRS-T angle in patients suffering from acute CO poisoning during the early stages.
Patients and methods
Study design and setting
The data of 212 patients with acute CO poisoning admitted to the emergency department between January 2010 and May 2020 were retrospectively analyzed.
The inclusion criteria were patients ≥ 18 years of age who had complete ECG and laboratory investigations including the COHb level by using a CO-oximeter device; these patients were also diagnosed with acute CO poisoning based on the history of one CO source exposure and clinical manifestations during their first admission to the emergency department. The exclusion criteria included left ventricular systolic dysfunction, ventricular or atrial premature depolarization, presence of a pacemaker, electrolyte imbalance, moderate and severe heart failure, atrial fibrillation, chronic renal and hepatic failure, bundle branch block, atrioventricular block, and use of antiarrhythmic and vasodilator drugs (Figure 1) Flow chart of the patients admitted with acute carbon monoxide poisoning according to inclusion.
The frontal QRS-T angle was obtained from the automatic reports produced by the ECG device. The frontal QRS-T angle is a new marker of myocardial repolarization, defined as the angle between the directions of ventricular depolarization (QRS axis) and repolarization (T axis). Data describing the typical ranges of frontal QRS-T angle from digital ECG transformation methods varied. The absolute value of the difference between the frontal plane QRS and T axes was calculated as the frontal QRS-T angle in the current study. If such a difference was over 180°, the QRS-T angle was adjusted to the minimal angle as 360° minus the absolute value of the difference between the frontal plane QRS and T axes.
Acute CO poisoning diagnosis was based on the clinical manifestations, laboratory records (carboxyhemoglobin (COHb)), and ECGs of the patients with CO source exposure history. Based on troponin measurement, patients with acute CO poisoning were divided into 2 groups according to the presence of myocardial damage. Patients with cardiac troponin I (cTnI) value above 0.40 ng/mL were considered as Group 1 (presence of myocardial damage) 15 and other patients with a cTnI value ≤ 0.40 ng/mL were considered as Group 2 (absence of myocardial damage). Also, based on the cut-off values in the receiver-operating characteristics (ROC) curve analysis for the frontal QRS-T angle, all patients were classified into two groups as Group 1 (1–44.5°) and Group 2 (> 44.5°). Clinical demographic and laboratory data were compared between the groups as appropriate.
All stages of this study have been carried out in compliance with the Helsinki Declaration on Research Projects. In addition, the study was reviewed and approved by the Ethical Committee of the Sivas Cumhuriyet University. Ethics approval for the study protocol (2020/06/13) was obtained from the Ethical Committee of the Sivas Cumhuriyet University (Sivas, Turkey)
Statistical Analyses
Statistical analyses were carried out on SPSS statistical software version 23.0 (SPSS Inc., Chicago, USA). Descriptive statistics, percentages, means, and standard deviations summarized patients’ demographic and laboratory characteristics. Differences in the characteristics between the two groups were assessed using the Mann–Whitney U test and chi-square test. Pearson correlation coefficients were used in comparing parameters. Next, logistic regression analysis was performed to assess independent variables associated with the QRS-T angle, using adjusted odds ratios and 95% confidence intervals (CI). The ROC curve and the area under the curve (AUC) were calculated with the frontal QRS-T angle on admission. All statistical tests were conducted at the 5% significance level.
Results
Of the 212 patients with acute CO poisoning included in the study, 122 (55.5%) were male, 90 (45.5%) were female, and the mean age was 68.9 ± 13.9 years.
Demographic features of patients with the carbon monoxide poisoning myocardial damage (−) patient group versus themyocardial damage (+) patient group.
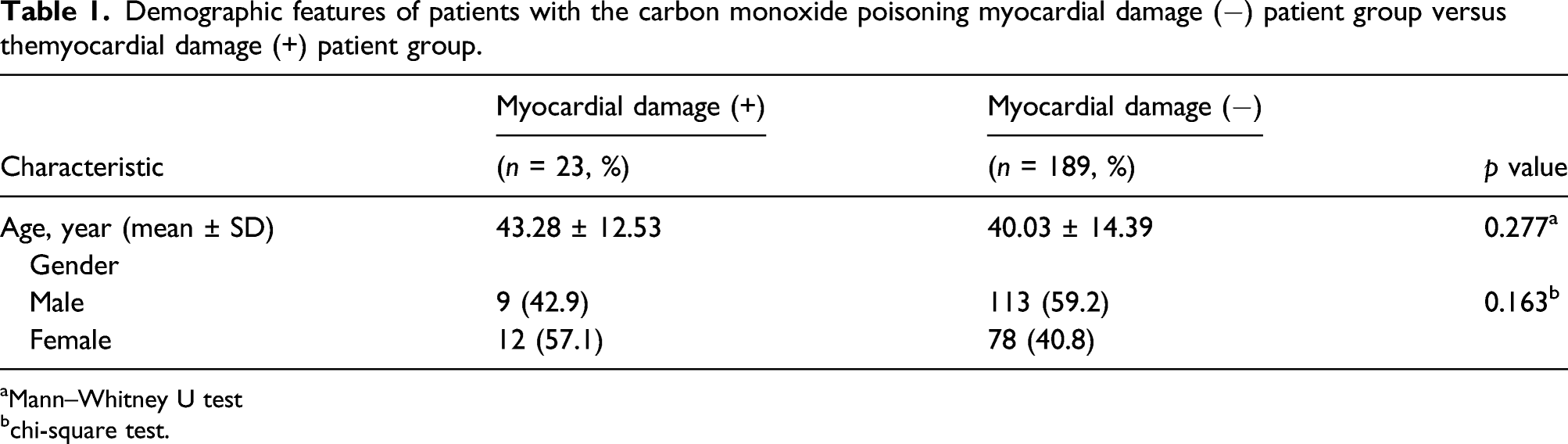
aMann–Whitney U test
bchi-square test.
The mean values of blood parameters of patients with and without myocardial damage due to carbon monoxide poisoning.

pH: power of hydrogen; SpO2: oxygen saturation in the arterial blood; PaO2: partial pressure of oxygen in the arterial blood; PaCO2: partial pressure of carbon dioxide in the arterial blood, Data p-value as median (25%–75% interquartile ranges).
aBUN: blood urea nitrogen.
Clinical and cardiovascular characteristics in carbon monoxide–poisoned patients in relation to QRS-T angle (n = 212).

aMann–Whitney U test.
Correlation between the frontal QRS-T angle and some variables in all patients with monoxide poisoning (n = 212).

Cut-off value, sensitivity, specificity of the frontal QRS-T angle, cardiac troponin I, creatine kinase, pH, and SpO2 for predicting myocardial damage in patients with carbon monoxide poisoning.

PPV: positive predictive value; NPV: negative predictive value; CI: confidence interval; pH: hydrogen in arterial blood; SpO2: oxygen saturation in the arterial blood.
aAUC: area under the curve.

Receiver-operating characteristic curve of the frontal QRS-T angle, cardiac troponin I, and creatine kinase for predicting myocardial injury in patients with acute carbon monoxide poisoning and exclusion criteria.
Logistic regression analysis was performed to explore associations with the frontal QRS-T and selected variables (creatine kinase, cTnI, arterial pH, and SpO2) (Table 6). As shown in Table 6, only the cTnI was associated with the frontal QRS-T. Receiver-operating characteristic curve of power of hydrogen in arterial blood, oxygen saturation in the arterial blood angle for predicting myocardial injury in patients with acute carbon monoxide. Logistic regression analysis of selected variables associated with the QRS-T angle (n = 212). OR: odds ratio; CI: confidence interval; pH: potential of hydrogen; SpO2: peripheral oxygen saturation.

Discussion
This study is the first in literature which determined the importance of a wide frontal QRS-T angle on the ECG in detecting myocardial damage among CO poisoning patients.
In CO intoxications, it competes with oxygen and forms carboxyhemoglobin (COHb) with 200 times greater affinity than oxygen. Displacement of oxygen reduces oxygen-carrying capacity. CO also stabilizes the Hb quaternary state and reduces oxygen release and delivery to tissues. However, the toxic effects of CO cannot be explained by this event alone. Due to the increase in the binding of CO to enzymes and proteins (cytochrome P-450 and myoglobin) at the cellular level, the resultant effect is a cellular damage caused by the reduction of energy production in the mitochondria of the cells mainly due to the binding of cytochrome aa3. With these effects occurring in the myocardium, anaerobic respiration begins, Adenosine triphosphate (ATP) production is interrupted, and lactate accumulates with free radicals at the cellular level. Relaxation of vascular smooth muscles with increased inflammation and thrombotic tendency, myocardial damage, and clinical complications are observed. As a result, the cardiotoxic effects of CO occur 16 in the early stages of CO poisoning; the oxygen requirement of the myocardium increases with compensatory tachyarrhythmias that develop due to systemic hypoxia, after which the diffusion of CO in the myocardium is accelerated; thus, the hypoxic damage is further increased. 17
Electrocardiography alterations are described in many studies. The alterations after acute CO intoxication can be reversed or prolonged according to the severity of the intoxication and can occur due to the repolarization disturbances (e.g., ischemic changes and QT interval prolongation). 18
In patients who were presented with CO poisoning, estimating the risk of myocardial damage can help determine both immediate and short-term treatment strategies. Patients suspected of exposure to CO should be screened for myocardial damage. One of the indications for hyperbaric O2 treatment of CO poisoning is myocardial ischemia. 19 It has been shown that cardiotoxicity-related morbidity and mortality rates can be reduced with appropriate treatment. 20
While myocardial damage due to severe CO poisoning can predict short-term undesirable bad results 21 in patients with moderate-to-severe CO poisoning, it was a significant predictor of mortality. 22 Therefore, emergency room physicians should always identify myocardial damage after CO poisoning with an ECG, cardiac markers (B-type natriuretic peptide), etc. and imaging (echocardiography or coronary angiography) tests. 16
Cardiac biomarkers are of great importance due to the fact that they indicate myocardial damage in systemic or cardiac diseases. Primary cardiac causes of myocardial damage and other systemic diseases play an essential role in the patient’s morbidity and mortality. Elevated troponin levels predict short-term (sepsis, pulmonary embolism, and ischemic stroke)23–25and long-term mortality (in critical patients, end-stage kidney disease, and major vascular surgery cases).26–29
Cardiac biomarkers have also been used to determine myocardial damage in CO poisonings.30,22
Cardiac dysfunction due to CO exposure can be indicated by chest pain, ECG changes, dyspnea, and low blood pressure measurement. 31 Most importantly, CO-induced myocardial damage can also occur in the absence of cardiac symptoms, 32 and ST-T changes in ECG can be a misleading indicator of severity in CO poisoning. 33
Electrocardiography is a noninvasive and prognostic diagnostic tool commonly used for cardiac damage in emergency departments. The frontal QRS-T angle is defined as the angle between the main electrical axes of ventricular depolarization and repolarization. 14 Evaluating QRS-T in the frontal plane is simple and can be easily calculated and included in the output results with automatic interpretation features to the ECG devices.
Pavri et al. demonstrate that a frontal QRS-T angle > 90° was a significant predictor of adverse outcomes in non-ischemic cardiomyopathic patients. They evaluated the groups with the endpoint for death, appropriate implantable cardioverter-defibrillator (ICD) shock, or resuscitated cardiac arrest. Relative risk was associated with a near doubling of the risk of death, appropriate ICD shock, or resuscitated cardiac arrest.34*
In addition, Zhang et al. found the frontal QRS-T angle to be significant for predicting the incidence of coronary heart disease and total mortality among women. Similarly, a study of atherosclerosis risk in communities involving 9498 patients found that the frontal and spatial QRS-T angle was a marker that predicted silent myocardial ischemia. 10
The frontal QRS-T angle is a strong predictor of cardiovascular events in different patient populations. Lown et al. investigated the survival of 1843 patients admitted with acute coronary syndromes, and they were stratified by the frontal QRS-T angle. A frontal QRS-T angle age-risk (FAAR) score was constructed according to their age and the frontal QRS-T angle. The FAAR score offered good discriminative performance for 30-day and 2-year mortality. 35 The frontal QRS-T angle at admission and after the percutaneous procedure was found to be a marker of in-hospital mortality, and 78 from 128 STEMI patients who had successful thrombolysis had a lower frontal QRS-T angle measured at 90 min compared to the failed thrombolysis group. 36 Blood pressure has a diurnal rhythm and decreases approximately 10% during sleep. A lack of blood pressure fall during the night is called a non-dipping blood pressure pattern and is associated with cardiovascular risk. A study conducted in hypertensive patients without left ventricular hypertrophy found that the frontal QRS-T angle predicted a non-dipper state. 37
Diabetes mellitus damages the autonomic nerve fibers in the heart, resulting in abnormalities in heart rate control and vascular dynamics. May et al. conducted a study in diabetic patients and observed 153 patients for 21.5 years. They concluded that the abnormal frontal QRS-T angle (QRS-T angle ≥ 73° in men and ≥ 67° in women), similar to cardiovascular autonomic neuropathy, independently predicted long-term mortality due to all causes. 38 Repolarization and depolarization abnormalities are commonly seen during heart failure with preserved ejection fraction clinical state. Increased frontal QRS-T angle was found to predict impaired left and right ventricular function, adverse cardiac remodeling, and undesirable cardiac events in patients with heart failure with a preserved ejection fraction. 39
In our study, the frontal QRS-T angle in the group of patients who developed myocardial damage after CO intoxication was greater, compared to the group who did not develop myocardial damage, and this is a strong predictor of cardiovascular events, as in previous studies (Table 2).9,40,41
It should be kept in mind that the COHb level does not correlate with clinical status, and the toxicity threshold can show individual differences. A correlation between COHb levels and ECG changes following acute or chronic CO exposure may not be observed. 18 In our study, COHb percentage levels were not significant between two groups with and without myocardial damage (Table 2). Since the COHb level does not provide information about myocardial damage, myocardial damage can be predicted by calculating the frontal QRS-T angle on the ECG, a cost-free and straightforward study.
In addition, our study also showed that the frontal QRS-T angle could be used to detect myocardial damage with high sensitivity and specificity with cut-off values above 44.5 (Table 3).
Strengths and limitations
Our work has some limitations. The first and most important limitation is that it is a retrospective study with a relatively small group of patients with myocardial damage and was not supported by echocardiographic and coronary angiography. Also, patients could not be monitored for possible complications and consequences after pain.
Conclusions
CO causes myocardial damage and tissue hypoxia with its direct and indirect effects. In order to prevent cardiovascular risks and other complications in CO poisoning we must select the right oxygen administration way and time. The frontal QRS-T angle is a simple and inexpensive parameter that can be easily obtained from ECG and can affect our management. Our study shows that this simple ECG parameter may have an essential role in determining the risk of myocardial damage, regardless of COHb levels, in patients with CO poisoning
Footnotes
Author contributions
The concept and design of the study; the acquisition, analysis, and interpretation of data for work; drafting of the work and the critical revision for important intellectual content; and final approval of the article was made by YKT. The drafting of the study and its critical revision for important intellectual content was performed by NN. GT, İK, and SY made the analysis and interpretation of data for the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest for the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The institutional ethics committee approved the Sivas Cumhuriyet University study protocol (2020–06/13).
Informed consent
The medical authorities of our hospital authorized this study, and patients were informed and signed their consent to their data collection.
Data availability
The data were retrieved from the Clinical Data Analysis and Reporting System, the Clinical Management System, and the Electronic Patient Record System of the Hospital Authority, Sivas.