
Abstract
Aim
Red blood cell distribution width (RDW) is a numerical measure of variability in the size of circulating erythrocytes and is routinely reported as a component of a complete blood count panel. It has been shown that higher RDW is associated with increased mortality and morbidity in several types of intoxication. This study was designed to evaluate the prognostic value of RDW for in-hospital mortality and need of invasive mechanical ventilation in patients with methanol poisoning.
Methods
A retrospective chart review of patients with methanol poisoning was performed using data from Adana City Training and Research Hospital obtained between January 2019 and January 2020. Patients’ demographics, clinical features, the time elapsed between ingestion and presentation, the treatment applied, blood gas analysis, laboratory measures including RDW on admission, and clinical outcome were obtained.
Results
A total of 42 patients with methanol poisoning were included in the study with a mean age of 45 ± 11 years. The overall mortality was 21.4%. Values of RDW on admission were significantly higher in non-survivors than in survivors. The area under the receiver operating curve of RDW was 0.778 (95% CI: 0.567–0.988) for predicting in-hospital mortality and 0.762 (95% CI: 0.592–0.932) for predicting mechanical ventilator requirement.
Conclusion
This study suggests that increased RDW on the first admission is associated with mortality and with mechanical ventilator requirement in patients with methanol poisoning.
Introduction
Methanol is a clear, colorless, toxic liquid with a mild alcoholic odor. It is used as a solvent in many commercial products, including antifreeze, pesticides, paint thinner, varnish, and gasoline.1-4 Methanol is first metabolized to formaldehyde by alcohol dehydrogenase. 3 Formaldehyde is then oxidized to formic acid by formaldehyde dehydrogenase. Formic acid is the primary toxin responsible for the most serious effects of methanol ingestion, including metabolic acidosis, ocular toxicity, and neurological disturbances such as coma and convulsions.1,5
Headache, dizziness, nausea, vomiting, and abdominal pain are the initial symptoms of methanol poisoning, which are also seen at later stages. Visual impairment may be the only symptom or may accompany other symptoms. In later stages, coma, seizure, pancreatitis, gastrointestinal bleeding, basal ganglia hemorrhage, and infarct may be present in patients with serious toxicity. 1 Treatment options for patients presenting with visual impairment and significant acidosis include the administration of intravenous sodium bicarbonate to correct acidosis, an antidote (fomepizole or ethanol) to block the metabolism of methanol, and hemodialysis to eliminate methanol and its toxic metabolite. 3 Theoretically, folate may have a role in improving the conversion of formic acid to CO2 and water.
Red cell distribution width (RDW) is a measurement of the range in the volume and size of circulating red blood cells and is reported as part of a standard complete blood count. The standard deviation of red blood cell (RBC) volumes is divided by the mean corpuscular volume (MCV) to determine the RDW. Higher RDW values reflect greater heterogeneity in RBC size (anisocytosis), which is usually caused by several disease processes involving the formation, in vivo transformation, and removal of RBCs from circulation. An elevation of RDW may occur in natural processes (aging), medical diseases, and poisonings.6–15 The pathophysiology of variation in RBC is still unclear. In erythropoietic stress, such as iron deficiency and nutritional deficiencies (folate or vitamin B12), RDW is elevated. Oxidative stress, inflammation, altered lifespan, or reduced deformability of RBCs have been suggested to influence RDW.8,13-16 In clinical conditions where inflammation is a factor, C-reactive protein increases more or less in parallel to the level of RDW.
Despite efficient treatment, methanol poisoning is associated with significant morbidity and mortality. To date, several studies have been conducted to identify the prognostic factors in methanol poisoning. To our knowledge, no study has investigated the impact of RDW on prognosis of patients with methanol poisoning. The primary aim of this study is to investigate the prognostic validity of RDW value for in-hospital mortality and need of invasive mechanical ventilation in patients with methanol poisoning.
Materials and methods
This retrospective cohort analysis enrolled a series of patients who were admitted with methanol poisoning to Adana City Training and Research Hospital between January 2019 and January 2020. The study was approved by the Institutional Review Board (Jan-2020, Ref 49–706) and conducted in accordance with the principles of the Helsinki Declaration. 17 The study was also registered at http://www.clinicaltrials.gov, with registration number NCT04064801. The inclusion criteria were as follows: patients 18 years of age or older and patients with a diagnosis of methanol toxicity. The diagnosis of methanol poisoning was based on a positive history of recent ingestion of alcohol (illegal spirits), clinical manifestations, and presentation of at least two of the following laboratory values on hospital admission: pH <7.3, serum bicarbonate <20 mmol/L, and anion gap ≥20 mmol/L. 18 We excluded patients with incomplete data, malignancy, and severe anemia and patients who had received anemia treatment or had a history of erythrocyte transfusion within the last 6 weeks.
The written and electronic medical charts of the patients were reviewed. Demographic characteristics, including age and gender, were collected. The estimated ingested volume of methanol, the time between ingestion and arrival at the hospital, initial vital signs and clinical findings, Glasgow Coma Score, length of hospital stay, mechanical ventilation requirement, and the outcomes of the patients were noted. The initial laboratory parameters consisted of white blood cell count, neutrophil to lymphocyte ratio, hemoglobin, arterial pH, PaCO2, HCO3, base deficit, glucose, blood urea nitrogen, creatinine, amylase, lipase, and arterial lactate. Mortality during hospital stay was used as the primary endpoint. The patients were divided into two subgroups: survivors and non-survivors.
Patient treatment was based on the standard protocols of the American Academy of Clinical Toxicology, including administration of sodium bicarbonate, ethanol, folic acid, and hemodialysis if necessary. 3
Statistical Analysis
The Shapiro–Wilk test was used to verify the normality of the distribution of continuous variables. Continuous variables are presented as mean ± SD or median (min–max) in the presence of abnormal distribution, and categorical variables are presented as frequencies (%). Comparisons between the groups of patients were made using Fisher’s exact test for categorical variables, the independent samples t-test for normally distributed continuous variables, and the Mann–Whitney U test for abnormal distributions. Correlations were evaluated using the Pearson correlation test.
Receiver-operating characteristic (ROC) curves were used to analyze the power of the prognostic performance of RDW in predicting mechanical ventilation requirements and in-hospital mortality. The optimal cutoff points for each parameter were determined using Youden’s index (sensitivity + specificity −1) and the maximized area under the curve (AUC). Sensitivity and specificity were calculated for these cutoff values. All statistical procedures were performed using SPSS statistical software package version 18.0 (SPSS, Inc., Chicago, IL). A P value of <0.05 was considered significant.
Results
Baseline characteristics of the patients with methanol poisoning.

Glu: glucose; BUN: blood urea nitrogen; NLR: neutrophil to lymphocyte ratio; MAP: mean arterial pressure; RDW: red cell distribution width. *
Patients’ clinical characteristics.

COPD: chronic obstructive pulmonary disease.
*P-values represent Fisher’s exact tests. Significant values are in bold.
ROC curve analysis of Glasgow Coma Score, glucose, red blood cell distribution width, pH, lactate, base deficit, and HCO3 values for hospital mortality.

AUC: area under the curve; SD: standard deviation; CI: confidence interval; GCS: Glasgow Coma Score; HCO3: bicarbonate. Significant values are in bold.
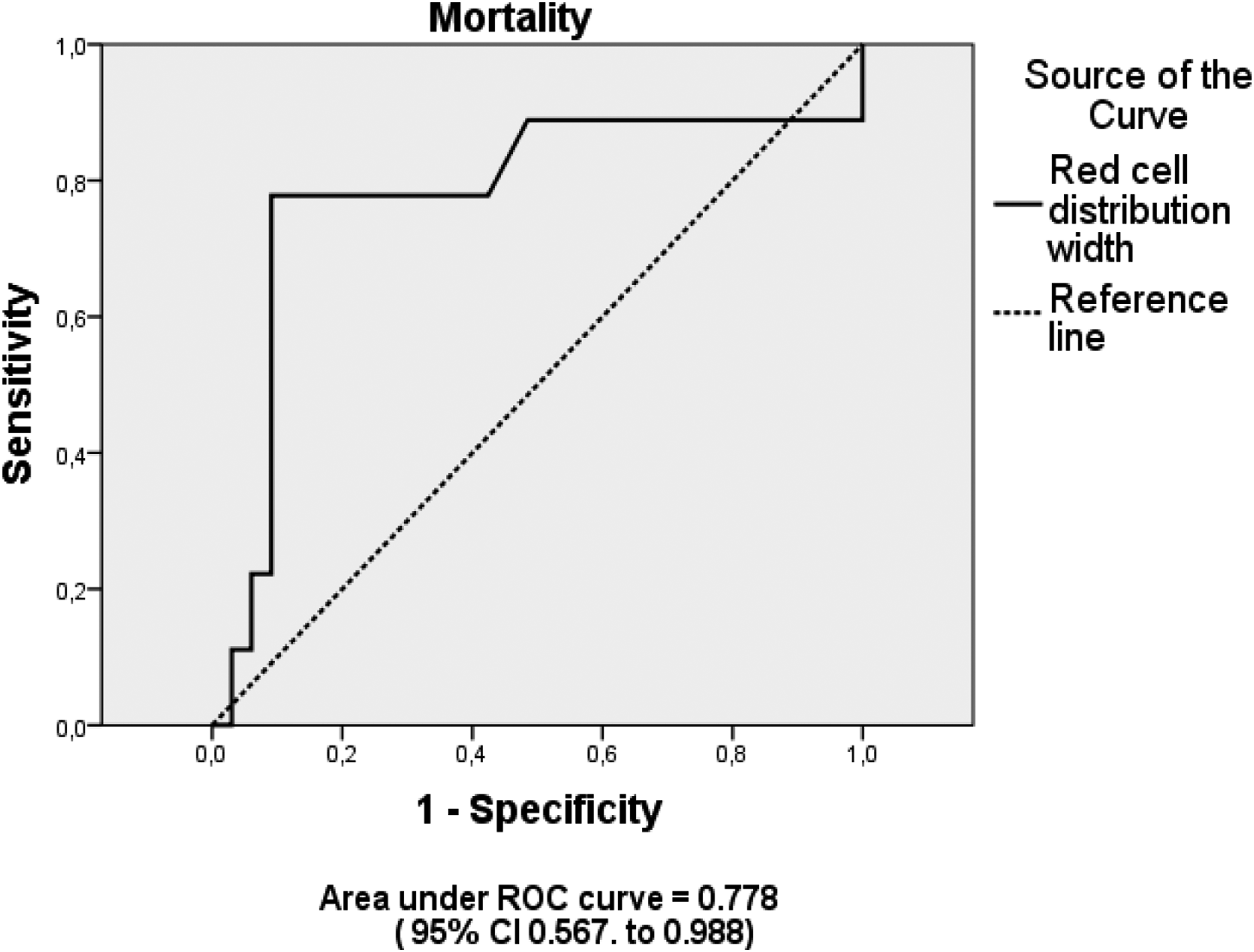
Receiver-operating characteristic curve for red blood cell distribution width for predicting hospital mortality in methanol poisoning patients.
Correlation between clinical parameters and RDW.

RDW: red cell distribution width; HCO3: bicarbonate; MAP: mean arterial pressure.
Significant values are in bold.
Of the 42 patients, 16 (38.1%) required mechanical ventilation support during the treatment period. Mechanically ventilated patients had significantly higher RDW values at admission than non-ventilated patients (p < 0.001). According to ROC curve analysis to predict mechanical ventilation requirement, the RDW had an area of 0.762 and a cutoff of 14.4 (sensitivity 77%, specificity 75%; the best Youden index was 0.52) (Figure 2). Receiver-operating characteristic curve for red blood cell distribution width for predicting mechanical ventilator requirement in methanol poisoning patients.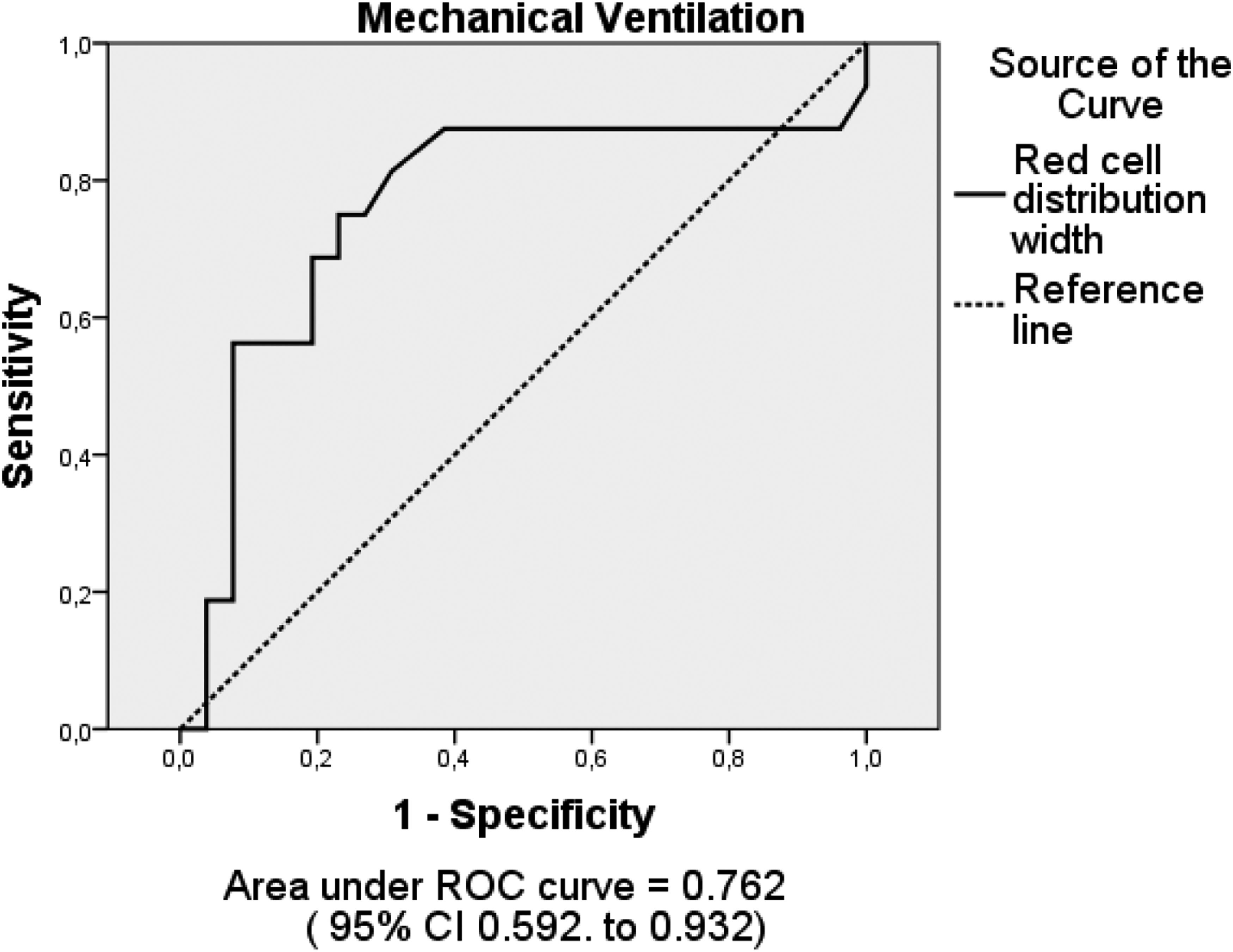
Discussion
To the best of our knowledge, our study is the first to evaluate RDW in methanol poisoning. We found that initial RDW values in methanol poisoning were significantly higher in non-surviving patients compared to surviving patients. Values of RDW on admission were also higher in patients requiring mechanical ventilation support than in patients who did not require mechanical ventilation support. The ROC curve indicated that the cutoff value of 14.4 of RDW can be valuable for predicting mechanical ventilation requirements.
Metabolic acidosis has been extensively studied in methanol poisoning, mainly because of its prognostic importance.4,19,20 Paasma et al. found that the severity of acidosis was an important prognostic factor in methanol poisoning. 19 Moghaddam et al. found that coma and metabolic acidosis on admission with pH below 7.00 were indicators of poor prognosis. In their study, the mortality rate was 90% for comatose patients compared with 10% for non-comatose patients. 4 Recently, Zadeh et al. reported that hyperglycemia in methanol poisoning was associated with poor clinical outcomes. 21
This study confirms previous findings that showed mortality correlated with a low Glasgow Coma Score on admission, severe metabolic acidosis, low serum bicarbonate levels, a high base deficit, and high glucose levels. According to our ROC curve analysis, Glasgow Coma Score (AUC:0.956), HCO3 (AUC:0.972), pH (AUC:0.960), and base deficit (0.907) had an excellent performance in the prediction of mortality. Our study also showed that RDW was a mild predictor of mortality in methanol toxicity with an AUC value of 0.778. The combination of RDW with other clinical prognostic parameters could provide an incremental predictive value for mortality. The RDW is a simple parameter that is automatically generated by all hemocytometers along with the complete blood count. For this reason, the measure of RDW does not entail any additional costs. The identification of new prognostic markers may identify at-risk patients early and provide extra information about disease severity.
Value of RDW has been regarded as an important biomarker of oxidative stress and inflammation. Oxidative stress represents an imbalance between the production of free radicals and the antioxidant capacity of the body. Oxidative stress, which plays a significant role in damaging the erythrocyte membrane and thus reducing the life span of the erythrocytes, has also been proposed to be associated with RDW. 14 It has also been shown that increased oxidative stress contributes to an increase in lipid peroxidation and a decrease in the phospholipid content of the erythrocyte membrane. In an experimental study, Mongi et al. reported that the treatment of rats with methanol increased lipid peroxidation and decreased the activities of the enzymatic antioxidants (superoxide dismutase, catalase, and glutathione peroxidase) in erythrocytes. 2 Several studies have been published regarding the relationship between RDW and oxidative stress. Value of RDW can be used as a novel potential parameter to evaluate prognosis in carbon monoxide intoxication and organophosphate poisoning.8,12 Also, it has been reported that methanol causes cell swelling. 3 Depending on the balance between these pathophysiological mechanisms and the duration and severity of the poisoning, different complete blood count results can be obtained.
Our study has several limitations. First, this was a retrospective study, and thus, the amount and quality of the data collected were limited. Second, we did not measure folate, vitamin B12, or iron levels on admission, all of which may affect RDW levels in patients. Finally, we cannot conclude that the observed higher RDW values with increased severity of methanol toxicity are a result of oxidative stress. However, further prospective studies, particularly in cases of methanol poisoning, are required to determine if this RDW elevation results from a high oxidative stress mechanism exposure.
Conclusion
Our study shows that RDW was high in methanol poisoning. Value of RDW was significantly higher in those dying compared with the survivors. Value of RDW might, therefore, be a new prognostic factor in methanol poisoning. In the case of hospitals that lack facilities, consideration of RDW level may be a simple and practical tool for assessing the severity of methanol poisoning.
Footnotes
Acknowledgments
Preliminary results of this study were presented at the fifth International Hippocrates Congress on Medical and Health Sciences, December 18, 2020.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.