
Abstract
MicroRNAs (miRNAs) are small noncoding RNAs stretching over 18–22 nucleotides and considered to be modifiers of many respiratory diseases. They are highly evolutionary conserved and have been implicated in several biological processes, including cell proliferation, apoptosis, differentiation, among others. Acute lung injury (ALI) is a fatal disease commonly caused by direct or indirect injury factors and has a high mortality rate in intensive care unit. Changes in expression of several types of miRNAs have been reported in patients with ALI. Some miRNAs suppress cellular injury and accelerate the recovery of ALI by targeting specific molecules and decreasing excessive immune response. For this reason, miRNAs are proposed as potential biomarkers for ALI and as therapeutic targets for this disease. This review summarizes current evidence supporting the role of miRNAs in ALI.
Introduction
Acute lung injury (ALI) is a serious pathological condition characterized by uncontrolled inflammation and damage to endothelial and epithelial barriers of the lung. ALI is characterized by the destruction of alveolar-capillary integrity, high infiltration of inflammatory cells, the excessive release of cytokines and chemokines, and the overflow of protein-rich fluid. 1,2 Acute respiratory distress syndrome (ARDS, defined in Table 1), a serious form of ALI, is caused by several risk factors classified as either direct or indirect (Table 2). These risk factors are associated with three main pathophysiological features including reduced ability to eliminate CO2, reduced lung volumes and compliance, and hypoxemia. 5 Despite high mortality rates linked with ALI/ARDS, lung-protective mechanical ventilation is regarded as the mainstay clinical treatment for improving patients’ breathing condition so as to upgrade their survival rates. 6,7 Due to immediate stability, proven safety, and powerful regenerative potential of mesenchymal stem cells (MSCs), 8 stem cell–based therapies are potential treatments for ALI, as revealed in preclinical and clinical studies. However, some aspects of their therapeutic effects remain undefined. 9 Further studies are required to solve this problem. 10
The Berlin definition of ARDS. 3
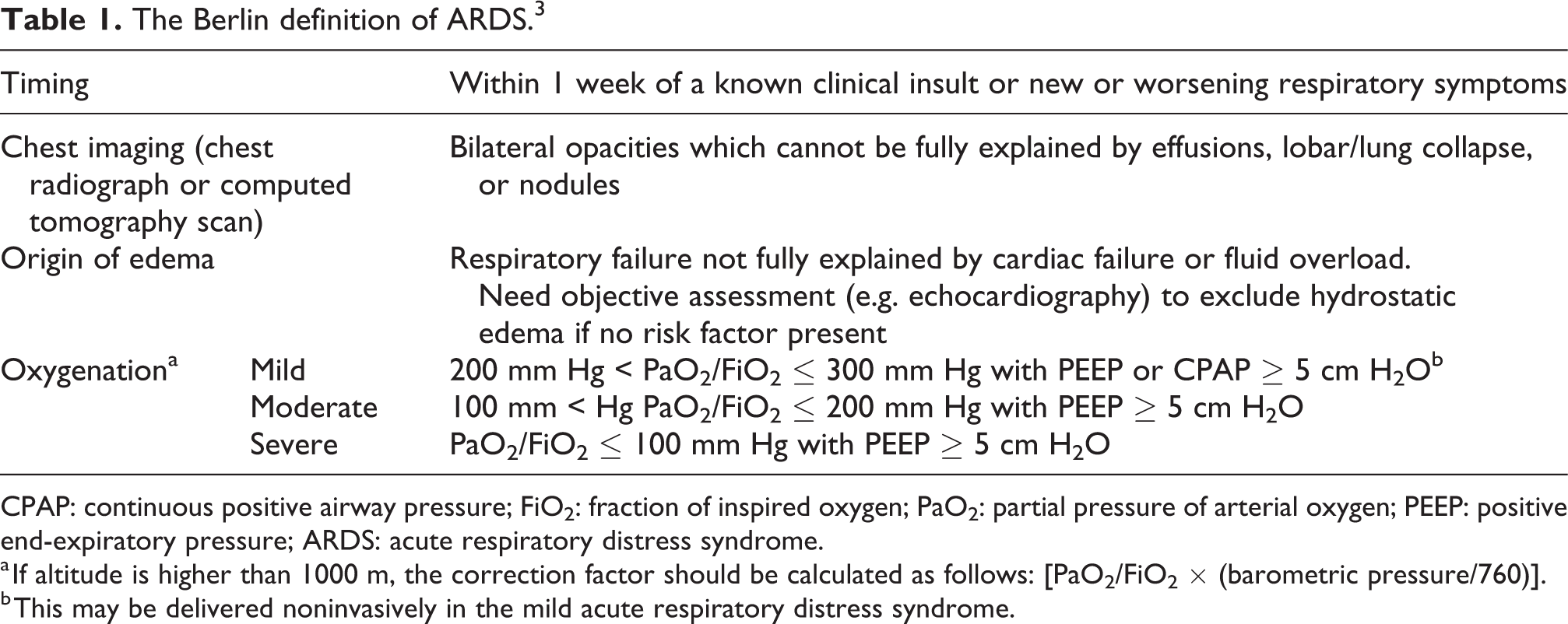
CPAP: continuous positive airway pressure; FiO2: fraction of inspired oxygen; PaO2: partial pressure of arterial oxygen; PEEP: positive end-expiratory pressure; ARDS: acute respiratory distress syndrome.
a If altitude is higher than 1000 m, the correction factor should be calculated as follows: [PaO2/FiO2 × (barometric pressure/760)].
b This may be delivered noninvasively in the mild acute respiratory distress syndrome.
Common risk factors related to ARDS. 4

ARDS: acute respiratory distress syndrome.
In recent years, investigations have revealed that microRNAs (miRNAs) may serve as biomarkers and treatments for diseases, such as cancer, 11 allergic diseases, 12 cardiovascular disease, 13 diabetes, 14 among others. It has also been found that miRNA plays an important role in ALI/ARDS. 15 Several therapeutic miRNAs have been found to be potential ingredients for biopharmaceuticals that are yet to be put on the market. 16 This review gives an overview of the current understanding on the role of miRNAs in ALI/ARDS and their diagnostic and therapeutic significance in this condition.
MiRNA: Biogenesis and function
miRNAs are a class of highly conserved, noncoding RNA molecules that are approximately 18–22 nucleotides long and single-stranded. 17 Biosynthesis of mature miRNA is a complicated process. The enzyme RNA polymerase II transcribes miRNA genes to create the primary transcripts (pri-miRNAs) within the nucleus. 18 Next, pri-miRNAs undergo two successive cleavage steps which are catalyzed by RNA endonucleases (RNase). The first cleavage occurs in the nucleus, where the RNase III type endonucleases Drosha (also known as RN3) releases a shorter oligonucleotide, precursor-miRNA (pre-miRNA) which is about 70–90 nucleotides long. 19 Drosha, together with a cofactor known as DiGeorge syndrome critical region gene 8 (DGCR8), presents an important center comprising of many regulatory proteins that control the miRNA maturation process. 20,21 The pre-miRNA is recognized by Exportin-5 (Exp-5) and its partner Ran-GTP, after which it is exported to the cytoplasm for further processing by RNase III enzyme Dicer. 22 Finally, the mature miRNA that is approximately 18–22 nucleotides long combines with Argonaute (Ago) protein thereby forming a miRNA-protein complex known as the RNA-induced silencing complex (Figure 1). 23 –25

A schematic illustration of miRNA biogenesis, function, and extracellular vesicle miRNA transfer. RNA polymerase II (RNA Pol II) and the Dorsha-DGCR8 microprocessor complex coordinate the synthesis of pre-miRNA. Exportin-5 recognizes pre-miRNA and exports it to the cytoplasm where pre-miRNA generates a mature miRNA which is then incorporated into complex RISC. This complex RISC aids in translational repression, translational activation, mRNA target degradation, and destabilization. Pri-miRNA: primitive miRNA; miRNA: microRNA; pre-miRNA: precursor-miRNA; RISC: RNA-induced silencing complex.
Expression of posttranscriptional target genes is regulated by miRNA. 26,27 When miRNA binds to the complementary sequences in the 3′ or 5′-untranslated region (UTR), it regulates gene expression by either degrading mRNA or inhibiting translation depending to the degree of completeness. 28 Individual miRNA can target several genes within one cell type or a single gene may be targeted by several miRNAs; however, one miRNA will have moderate effect on one target. 29,30 The relationship between gene expression and miRNAs is very complex. Studies have affirmed that miRNA takes part in several biological processes. The expression of miRNAs is characterized by tissue- and cell-specificity, with spatial and temporal patterns, making them potential therapeutic targets and biomarkers for various diseases. 31,32
MiRNA: Biomarker for ALI/ARDS
Biomarkers are used to identify the homogeneous phenotypes within a given situation, risk rank, and predict specific results (e.g. mortality). They are also used for assessing the degree of illness, prognosticating, and monitoring therapeutic response.
Thus, diagnostic biomarkers of ALI/ARDS can be used for identifying patients likely to benefit from therapeutic interventions. 33,34 Several biomarkers for ALI/ARDS have been identified (Table 3), but none has been fully proved to be reliable enough for clinical application. 62 –64 Therefore, it is imperative to identify more accuracy and specific biomarkers for ALI/ARDS.

miRNA: microRNA; ARDS: acute respiratory distress syndrome; ALI: acute lung injury; IL: interleukins; IL-1ra: IL-1 soluble antagonist sTNF: soluble tumor necrosis factor; sTNF-RI: soluble TNF receptor I; sTNF-RII: soluble TNF receptor II; RAGE: receptor for advanced glycation end products; SP: surfactant proteins; KL-6: Krebs von den Lungen-6; CC16: club cell protein 16; KGF: keratinocyte growth factor; Ang-1: angiopoietin-1; vWF: von Willebrand factor; VEGF: vascular endothelial growth factor; PAI-1: plasminogen activator inhibitor-1.
As prospective biomarkers for diseases, miRNAs have many advantages. First, miRNAs tend to be stable in varying physical conditions compared with other types of RNA, such stability is important in the early stages of gene expression. 65,66 Second, miRNAs can be isolated from various body fluids, and their changes can be detected by the available techniques. 67 Third, the expression of miRNAs changes in different kinds of diseases before presenting their subsequent effects. 68 Fourth, the expression profiles for most miRNAs are generally independent of sex; however, some may be influenced by specific factors, such as age and disease. 69 –71 Fifth, most of the miRNAs are expressed conservatively among different species but highly specific to tissue or biological state.
Since the discovery of stable expression of miRNAs in body fluids in 2008, 66 various studies have explored the extracellular miRNAs. Research has shown that extracellular miRNAs were very stable in serum or plasma despite the presence of ribonucleases because they were packaged in different extracellular vesicles (EVs). The EVs are classified into three types based on their size and biogenesis: exosomes, microvesicles, and apoptotic bodies (Table 4). 72 –74 A few of the circulating miRNAs exploit other transportation strategies to escape degradation. 78 Extracellular miRNAs are transferred from one cell to another via EVs. In this way, they recognize and degrade their target mRNAs within the recipient cells. Extracellular miRNAs regulate cell-to-cell communication (Figure 1). 79 –82 In addition to the above features, miRNAs seem to be selectively released from cells rather than passively released from necrotic or damaged cells because their levels in different biological fluids vary under different pathophysiological conditions. 83,84 In a recent clinical trial, miR-126 showed potential to predict the 28-day mortality. This shows that alteration of circulating exosomal miRNAs levels influences the prognosis of ARDS. 85

EVs: extracellular vesicles.
To sum up, both intracellular and extracellular miRNAs are ideal candidates to be used as biomarkers for predicting, diagnosing, or predicting the prognosis of ALI/ARDS. Some miRNAs are significantly upregulated or downregulated miRNAs in ALI/ARDS as evidenced in previous animal models (Table 5). Further screening for sensitive and specific miRNAs as clinical biomarkers is highly advocated.

miRNA: microRNA; ALI: acute lung injury; ARDS: acute respiratory distress syndrome.
MiRNA: Regulatory molecules in ALI/ARDS
Based on the pathological and clinical manifestations, ARDS can be classified into early and late stage of lung injury, this corresponds to exudative and fibroproliferative phase, respectively. 63 Damage mainly occurs in pulmonary vascular endothelial cells and alveolar epithelial cells. The early stage (first few hours or days) is characterized by increased capillary permeability and the recruitment of leukocytes to inflammatory sites occurs. 10,93,94 In the late stage (occurring as early as 7–10 days after initial injury), ARDS is characterized by a disordered healing whereby of fibrous and granulation tissue, alveolar type II cells, new blood vessels, and extracellular matrix. 95,96 Recent studies have shown that the regulatory functions of miRNAs in ARDS were mediated by various physiological and pathological processes such as inflammatory responses, cell apoptosis, among others. 97
Functions of lung epithelial cells and vascular endothelium in the pathogenesis of ARDS are well-known. Some miRNAs contribute to the apoptosis of epithelial cells and endothelial dysfunction. In cardiopulmonary bypass-induced ALI, miR-320 triggers the apoptosis and inhibits proliferation of A549 cells (human alveolar type II epithelial cell). 98 A study by Li et al. found that Bcl-2 was the target gene for miR-181a. Thus, decreasing miR-181a expression can reduce cell apoptosis of lipopolysaccharide (LPS)-treated A549 cells. 99 In a mouse model, it was found that LPS-induced apoptosis of pulmonary endothelial cells was meditated by miR-1246, and this was attributed to partial repression of angiotensin converting enzyme 2 (ACE2). 100 Shah et al. showed that miR-34a regulated endothelial cells apoptosis and endothelial dysfunction by modulating the expression of Sirtuin-1 and p53. 101 Delivery of miR-126 through endothelial progenitor cell exosomes increases expression levels of tight junction proteins and maintains the integrity of alveolar epithelial barrier. 102
Excessive pulmonary inflammation is the primary cause of ALI. The imbalance between inflammation and anti-inflammation precipitates the progression of ALI/ARDS. In human lung epithelial cells, miR-454 inhibited the translation of CXCL12 mRNA by targeting 3′-UTR of the mRNA. Overexpression of miR-454 inhibited the production of inflammatory cytokines and improved the integrity of alveolar epithelial barrier. 103 LPS-induced ALI is characterized by high level of the pro-inflammatory cytokine IL-6 and miR-181b. It has been reported that miRNA-181b controlled the amount of p65 protein via the signaling pathway to initiate its role in ALI. 104 Downregulation of miR-140-5p increases the protein expression of Toll-like receptor 4 (TLR4), MyD88, and NF-κB in human lung A549 cells. Up-expression of miR-140-5p inhibits the levels of inflammatory response in the ALI model by reducing the activation of the TLR4/MyD88/NF-κB signaling pathway. 105 In both viral and bacterial lung infection-induced ALI/ARDS, the expression of miRNA-200c-3p increases significantly while ACE2 protein expression decreases. Overexpression of miR-200c-3p which is dependent on nuclear factor-κB reduces the level of ACE2. This increases levels of angiotensin II leading to lung injury next step. 106
miRNA-466 family molecules are secreted in the airway via EV where they regulate inflammation response via the NLRP3 inflammasome pathway. 107 Recovery of intracellular miRNA-223/142 via vesicle-mediated delivery inhibits macrophage activation and pulmonary inflammation since Nlrp3 inflammasome is deactivated. 108 A study by Yan et al. found that miR-155 was expressed in bone marrow–derived lymphocytes and not in lung parenchymal lymphocytes where it promotes LPS-induced ALI via the Ang-2-Tie-2 pathway. 109 MiR-223 plays a vital role in the pathogenesis of damage-associated molecular pattern (DAMP)-induced ALI. Of note, miR-223 decreases the expression of NLRP3 and releases of IL-1β which reduces the number of Ly6G+ neutrophils. This ameliorates ALI induced by mitochondrial DAMPs. 110 Studies have also revealed that miRNAs regulated in inflammation through other pathways. For example, experiments performed by Yin and his colleagues showed that miR-34/449 suppressed inflammation by targeting IGFBP-3, thus inhibiting autophagy. 111
Macrophages are known to have irreplaceable functions in the initiation, development, and resolution of inflammation. Of interest is that macrophages are involved in initiating the lung repair process. 112 Based on current research, majority of the experiments involving both ALI and miRNAs have been related to macrophages. In a study where miR-128 was overexpressed in RAW264.7 cells treated with inactivated Staphylococcus aureus, it was noted that miR-128 bound to the UTR of MyD88, an important downstream adaptor molecule for most TLR and interleukin (IL)-1 receptors. This binding significantly downregulated miR-128 expression level, inhibiting NF-κB signaling pathway. 113 Expression level of miR-92a decreases when it binds to the 3′-UTR of phosphatase and tensin homolog (PTEN) in RAW264.7 murine macrophages. 43 Furthermore, it was reported that inhibition of miR-92a alleviated inflammation in LPS-induced ALI mice by blocking PTEN/AKT/NF-kappa B signaling pathway.
Macrophage exhibits two phenotypes under environmental stimulation, one is the classically activated (or M1) and the other is the alternatively activated (or M2) phenotype. 114 IFN-γ and LPS induce M1 phenotype which express high levels of iNOS and other genes associated with the clearance of pathogens and those that regulate the inflammatory responses to intracellular pathogens. On the other hand, IL-4 and IL-13 induce M2 macrophages that express high levels of arginase-1 (ARG-1). These macrophages upregulate the expression of genes related to wound repairing, the clearance of dead/dying cells or tissues, and those that reduce inflammation. 115 –117 Both M1 and M2 macrophages have a crucial role in pathophysiological processes of ALI/ARDS. 118 Pulmonary macrophages and U937 cell lines treated with LPS exhibit high expression of miRNA-34a as result of increased iNOS secretion from pulmonary macrophages via Stat3 pathway. 119 Cytokine IL-1β triggers M2 to M1 macrophages polarization. 120 Partial inhibition of Notch 1 by miR-146a inhibits M1 macrophage polarization and drives M2 macrophage polarization, respectively. In addition, PPARγ, another target of miR-146a-mediated macrophage polarization, is able to drive the transition of macrophage polarization to M2 phenotype. 121
Fibrosis is a major characteristic of late stage of ALI. It was earlier demonstrated that miR-204 alleviated the degree of fibrosis and alveolitis by silencing IRF2. 122 Nonphysiological stretch of alveolar type II (ATII) cells, inducing fibrosis and accelerating epithelial–mesenchymal transition process, exhibits a higher expression of relevant miRNAs, for example, miR-15b, miR-25, and let-7d. 123 Reduction of miR-425 upregulates lysine demethylase 6A (KDM6A) and then activates TGF-β signaling pathway, which promotes proliferation of lung fibroblast and induces fibrosis finally. 124
Other than traditional therapies, stem cell–based therapy has become popular in the treatment of ALI due to its noninvasive and significant effect in animal models. miRNAs regulate the biological processes of MSCs as demonstrated in previous experiments. Expression of ADAMTS-5 is regulated by miR-132-3p to promote chondrogenic differentiation of rat MSCs. 125 Notably, miR-302a and miR-34a regulate the proliferative capacity of human MSCs. Together with Parp1, these two miRNAs function as epigenetic switches that preserve pluripotency. Moreover, miRNA-302a and miRNA-34a exert opposing effects on PARP1 expression. 126 In rat bone marrow–derived MSCs, it has been identified that Wnt5a was a target gene of miR-374. The Wnt5a/β-catenin signaling pathway regulates the proliferation and migration of transformed MSCs. 127
The functions and roles of partial miRNAs in ALI/ARDS have been summarized to demonstrate why miRNAs play a regulatory role in both early and late stages of ALI more intuitively (Table 6).
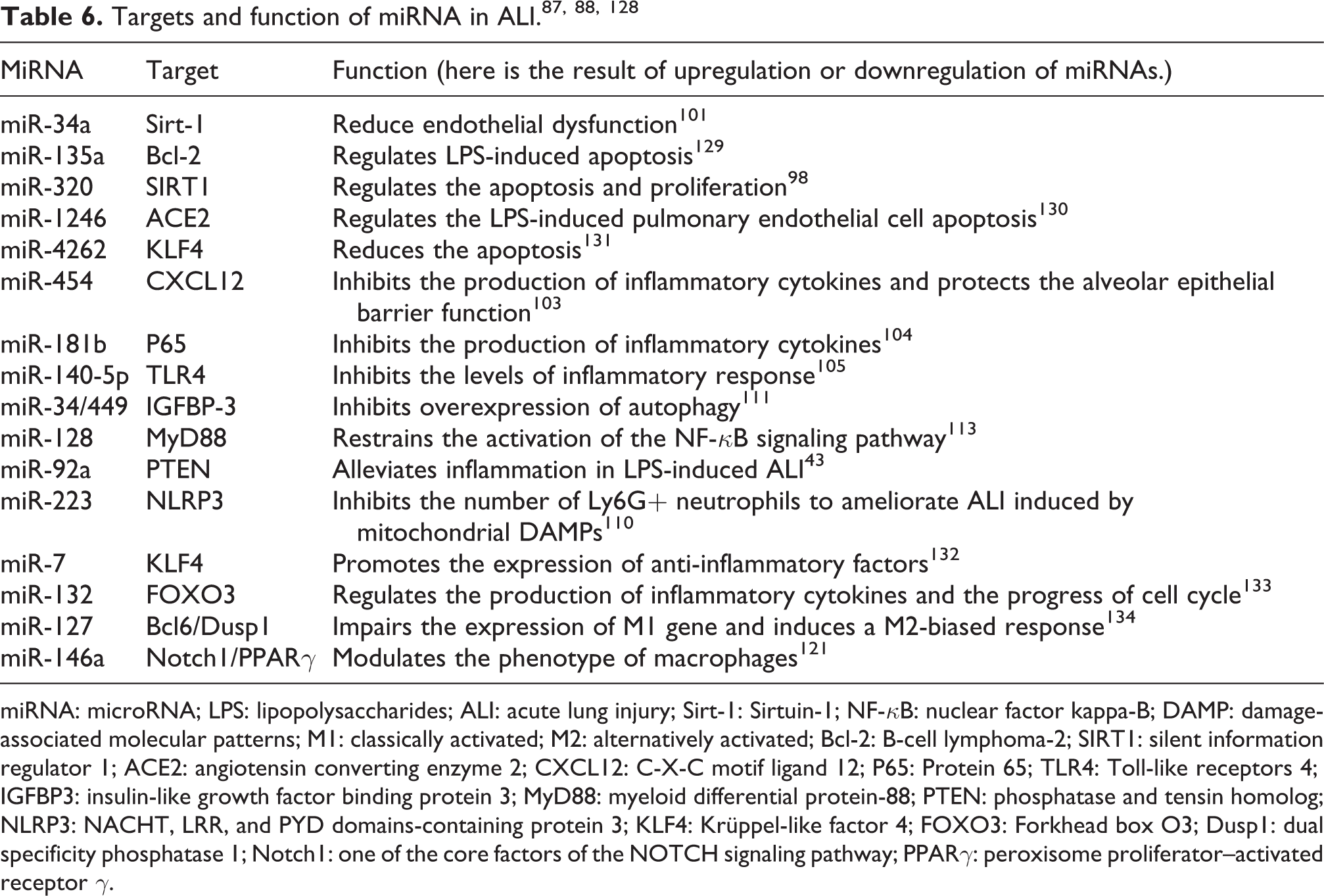
miRNA: microRNA; LPS: lipopolysaccharides; ALI: acute lung injury; Sirt-1: Sirtuin-1; NF-κB: nuclear factor kappa-B; DAMP: damage-associated molecular patterns; M1: classically activated; M2: alternatively activated; Bcl-2: B-cell lymphoma-2; SIRT1: silent information regulator 1; ACE2: angiotensin converting enzyme 2; CXCL12: C-X-C motif ligand 12; P65: Protein 65; TLR4: Toll-like receptors 4; IGFBP3: insulin-like growth factor binding protein 3; MyD88: myeloid differential protein-88; PTEN: phosphatase and tensin homolog; NLRP3: NACHT, LRR, and PYD domains-containing protein 3; KLF4: Krüppel-like factor 4; FOXO3: Forkhead box O3; Dusp1: dual specificity phosphatase 1; Notch1: one of the core factors of the NOTCH signaling pathway; PPARγ: peroxisome proliferator–activated receptor γ.
MiRNA: Potential therapeutic targets in ALI/ARDS
Currently, miRNAs have been identified as potential therapeutic targets for many diseases, such as heart disease, 135 liver disease, 136 and cancer. 137 Similarly, studies have documented the therapeutic significance of miRNAs in ALI/ARDS. The discovery of miRNAs as regulatory molecules has enhanced the development of synthetic RNA molecules, such as miRNA sponges, antagomiRs, and miRNA mimics that regulate expression of specific genes.
In 2005, the first new class of chemically engineered oligonucleotides “antagomiRs” were introduced, and they were specific silencers of endogenous miRNAs in mice. 138 However, the clinical application of antagomiRs has been limited by their low affinity and the need for high dosages to effectively inhibit miRNA. 135 Locked nucleic acid (LNA) which is an unconjugated, PBS-formulated locked-nucleic-acid-modified oligonucleotide improves binding affinity, nucleic resistance, and thus effectively inhibits miRNA in mice and nonhuman primates. 139,140 Short seed-targeting LNA oligonucleotides (also called tiny LNAs) are 7–8 nucleotides long, and these oligonucleotides simultaneously silence miRNAs within families sharing the same seed. 141
miRNA sponges are important tools for in vivo and in vitro studies on miRNA dysfunction. MiRNA sponges are described as transcripts with repeated miRNA antisense sequences, which act as competitive inhibitors to sequester endogenous miRNA from their target. 142
miRNAs mimics are chemically synthesized, double-stranded oligonucleotides that are processed into a single-stranded miRNA within a cell. 143 MiRNA mimics are capable of restoring downregulated miRNA levels to antagonize the effects of miRNA sponges and antagomiRs. Some of the miRNA mimics have shown good therapeutic effects in clinical trials. 144,145
In clinical applications, two methods for interference delivery are used in miRNA therapeutics: nonviral delivery and viral delivery. 146,147 These approaches regulate mRNA targets directly or indirectly, which finally achieved the effect of alleviating ALI/ARDS (Figure 2). However, some questions about this technology remain to be answered. These challenges are discussed in the conclusion section.

Schematic diagram showing the therapeutic targets of miRNAs in ALI. (a) In the pathological process of acute lung injury, miRNAs are upregulated or downregulated. Mature miRNA binds to a target mRNA and then regulates its level, leading to epithelial and endothelial cell injury, fibrosis, and activated inflammatory cascade. (b) There are four commonly used delivery methods to transfer miRNA modifications into cells. The levels of miRNAs can be recovered by miRNA modifications, which finally alleviates the lung injury. In summary, miRNAs have the potential to become therapeutic targets for ALI.
Conclusions and future perspectives
Although miRNAs regulate the initiation, development, and resolution of ALI in animal models, few studies have documented their potential to be biomarkers and therapeutic targets in clinical ALI or ARDS. Thus, further research is required to identify more specific miRNAs for clinical application. In addition, the following issues should be addressed:
Some miRNAs are either be upregulated or downregulated in ALI/ARDS, and some of these miRNAs are also associated with the existing biomarkers. Yet, it is not clear which miRNAs are specific and sensitive enough to be exploited as clinical biomarkers. Moreover, the cost of using standard laboratory techniques for testing and quantification of miRNAs is relatively high. Although miRNAs bind to target genes that are considered to be of therapeutic value, they also bind to nonspecific bystander mRNAs. When the expression of miRNAs is modified, this binding may lead to off-target effects, toxicity, and/or unfavorable immune response. ALI/ARDS is often accompanied with complications spreading to other organs or tissues. Whether miRNAs play a role in these complications is unclear. This is a gray area that deserves in-depth research. AntimiRs exhibit long-lasting effects after systemic delivery, and this may be associated with potential side effects. MiRNA mimics on the other hand have a short half-life and may induce immune responses.
148
Therefore, it is necessary to determine the optimal concentrations of miRNAs and appropriate cell/tissue-dependent delivery systems for effective treatment of ALI/ARDS.
Footnotes
Author contributions
ZJ and LZ collected and analyzed data, and cowrote the manuscript. JS reviewed this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by grant from the National Natural Science Foundation of China [No. 81801943], the Science and Technology Commission of Shanghai Municipality [No. 18411970200], and the Research project of Shanghai Health and Family Planning Commission [No. JSZK2019A01].