
Abstract
Introduction:
The affinity of hemoglobin for carbon monoxide (CO) is 250 times higher than that for oxygen. Therefore, exposure to CO leads to a reduction in oxygen delivery to tissues, resulting in cellular hypoxia and affects whole body. Hepatic dysfunction in critically ill patients is related to poor outcome, but few studies have been conducted on this subject that occurs after CO poisoning. This study aims to conduct a study of hepatic injury in CO-poisoned patients in emergency department (ED).
Methods:
This retrospective observational study collected data from patients who were diagnosed with acute CO poisoning at the ED between June 2011 and May 2018 in local tertiary-care hospital (Wonju, Republic of Korea). The primary end point of this study was to describe the prevalence of hepatic injury in acute CO-poisoned patients. The secondary goals were to investigate the recovery trends of hepatic injury caused by acute CO poisoning and the relation to neurologic outcome and mortality.
Results:
Eight hundred ninety-four patients were enrolled in the final analysis, 128 cases (14.3%) had subclinical hepatic injury and 15 (1.6%) cases had hepatic injury. The relationship with mortality was not statistically significant. However, the hepatic injury group was higher incidence of intensive care unit admission and other complications. Patients in the hepatic injury group recovered through conservative management within 1 week of being admitted to the ED.
Conclusions:
While CO-induced hepatic injury is relatively uncommon, it can be associated with complications and poor neurologic outcome. However, CO-induced hepatic injury was not found to have a statistically significant effect on mortality rate.
Introduction
Carbon monoxide (CO) competes with oxygen for hemoglobin binding. The affinity of hemoglobin for CO is 250 times higher than that for oxygen. Therefore, exposure to CO leads to a reduction in oxygen delivery to tissues, resulting in cellular hypoxia. 1 Acute CO poisoning is characterized by hypoxia and manifestations of the systemic ischemia–reperfusion injury. 2 CO poisoning is more likely to damage organs that require more oxygen. These include organs within the cardiovascular, respiratory, musculoskeletal, neurological, genitourinary, metabolic, and endocrinological systems. Hence, CO poisoning affects our whole body. 3
The pathophysiology of CO poisoning is as follows: first, due to the difference in oxygen affinity, CO leads to relative anemia, tissue asphyxia, and hypoxia; second, CO disrupts oxidative phosphorylation by binding to cytochrome c oxidase in mitochondria, which reduces cellular respiration and causes cellular hypoxia; third, CO increases the adhesion of white blood cells to endothelial surfaces and leads to leukocyte-dependent inflammatory changes and lipid peroxidation. This results in cellular edema, focal necrosis, and reperfusion injury. 4
The liver is also an organ that can be damaged by CO poisoning. Hepatic dysfunction is commonly found in critically ill patients and is associated with a poor outcome. 5 Hemodynamic instability or arterial hypoxemia can cause hypoxic hepatitis, which is frequently accompanied by multi-organ injury and high mortality. 6 This acute liver injury is mainly caused by insufficient oxygen uptake by hepatocytes, leading to centrilobular liver cell necrosis. 7 The mechanism of systemic injury caused by CO poisoning and hepatic dysfunction with critically ill patients is similar. Therefore, clinical reports on hepatic injury after CO poisoning caused by hypoxia are necessary. However, to our knowledge, no study has yet evaluated the prevalence of CO-induced hepatic injury. A knowledge of the clinical outcomes of early hepatic injury in CO-poisoned patients will allow clinicians to more closely observe patients in the emergency department (ED) who have an abnormal liver function test (LFT) value after CO poisoning.
The aims of this study were to describe the prevalence of early hepatic injury in acute CO-poisoned patients, to investigate the recovery trends of hepatic injury, and to describe the relationship between the associated complications and clinical outcome.
Material and methods
Patients
This retrospective observational study collected data from patients who were diagnosed with acute CO poisoning at the ED between June 2011 and May 2018. The ED was located in a single, suburban, tertiary-care hospital (Wonju, Republic of Korea) that has more than 46,000 annual visits and is staffed 24 h a day by board-certified emergency physicians. Since the study was retrospective and observational, informed consent was not required, and patient records and information were anonymized prior to analysis. This study protocol was approved by the International Review Board for Human Research (CR 318030) of Yonsei University Wonju Severance Christian Hospital.
A diagnosis of CO poisoning was made according to the patients’ medical history and a carboxyhemoglobin (CO-Hb) level of >5% (>10% in smokers). All patients presenting acute CO poisoning upon arrival at the ED were treated with 100% high-flow oxygen therapy through a face mask with a reservoir bag, and with hyperbaric oxygen therapy (HBOT), if indicated. 8 HBOT could not be performed in patients who were hemodynamically unstable, had uncontrolled irritability, or could not undergo equalization of the middle ear. Patients with normal consciousness at the time of hospital discharge were educated on delayed neuropsychiatric sequelae (DNS). Symptoms of DNS include mental deterioration, cognitive dysfunction, amnesia, gait disturbance, mutism, urinary or fecal incontinence, psychosis, depression, and Parkinsonism. 9
The patient exclusion criteria were as follows: (1) less than 18 years old; (2) profound shock that could affect liver enzyme level; (3) chronic liver disease including viral hepatitis or advanced liver disease; (4) alcoholic hepatitis—the serum aspartate aminotransferase (AST) and alanine aminotransferase (ALT) are typically less than 300 U/L and are rarely higher than 500 U/L, except in patients with alcoholic foamy degeneration (a histologic variant of alcoholic hepatitis). 10 The most common pattern observed when testing for abnormal liver biochemistry is a disproportionate elevation of serum AST compared with ALT. This ratio is usually two or greater in patients with alcoholic hepatitis, a value that is rarely seen in other forms of liver disease 11,12 ; (5) evidence of drug-induced liver injury (acetaminophen poisoning); (6) acute viral hepatitis (excluded by standard serology); (7) insufficient laboratory data.
Study variables and definitions
The following information was obtained from medical records: age, sex, source of CO, intentionality of poisoning, CO exposure time, history of smoking and alcohol, past medical history (diabetes mellitus and hypertension), initial mental status, vital signs, complications (rhabdomyolysis, acute kidney injury, and cardiomyopathy), and final neurologic outcome (normal, DNS).
The LFT recorded measurements of ALT, AST, bilirubin, gamma-glutamyl transferase (GGT), and alkaline phosphatase (ALP). The LFT, complete blood counts, arterial blood gas and lactate, creatinine kinase (CK), lactate dehydrogenase, international normalized ratio (INR), and albumin data were extracted at the time of patient arrival in the ED. However, CO-Hb has a different half-life depending on the situation (250 to 320 min when breathing room air, about 90 min when breathing high-flow oxygen, and 30 min when breathing 100% hyperbaric oxygen). Therefore, the first extracted result was used (the initial level of CO-Hb was checked from prehospital sources or obtained at our hospital).
CO-induced hepatic injury was defined as a serum ALT level of more than three times the upper limit of normal (ULN). Subclinical hepatic injury was defined as when ALT was above the ULN, but less than three times the ULN. As a general rule, similar to in the case of drug-induced liver injury, 13 histological proof is not required when the clinical definition is fully met. AST is less specific to liver injury than ALT and may increase for other reasons such as myocardial infarction or rhabdomyolysis. 14,15
Complications were listed in three categories: acute kidney injury, which was diagnosed using kidney disease improving global outcome (KDIGO) guidelines, 16 rhabdomyolysis with elevated CK and related symptoms (such as myalgia, muscle pain, myoglobulinuria), and secondary cardiomyopathy in patients who did not have a history of myocardial infarction, or cardiomyopathy and diagnosed according to the International Takotsubo Registry. 17
Data were collected via a retrospective review of patients’ electronic medical records. This review was conducted by one emergency physician who was blinded to the study objectives and hypothesis. The physician was also blinded to the patient group categorization and was trained prior to data collection to reduce possible bias in the data collection procedure. Explicit case reports were used for this study. The physician and study coordinator met periodically to resolve any disputes and review the coding rules. The study coordinator monitored the evaluator’s performance.
Study end points
The primary end point of this study was to describe the prevalence of hepatic injury in acute CO-poisoned patients. The secondary goals were to investigate the recovery trends of hepatic injury caused by acute CO poisoning and the relation to neurologic outcome and mortality.
Statistical analysis
Categorical variables are presented as frequencies and percentages, while continuous variables are presented as means and standard deviations or as medians and interquartile ranges. The differences between normal, subclinical hepatic injury, and hepatic injury groups were tested using an analysis of variance test, Crosstabs, a nonparametric test, and a Kruskal–Wallis test with multiple comparisons compensated for using the Bonferroni correction method. p Values <0.05 were considered statistically significant, and the analysis was performed using SPSS version 23 (IBM, Armonk, New York, USA) and MedCalc Statistical Software version 17.5.3 (MedCalc Software, Ostend, Belgium).
Results
Between June 2011 and May 2018, a total of 1090 acute CO-poisoned patients visited the ED. We excluded the patients who were less than 18 years old (n = 91); experienced profound shock that could affect liver enzyme level (n = 27); had chronic liver disease including viral hepatitis or advanced liver disease (n = 34); had alcoholic hepatitis (n = 6); or showed evidence of drug-induced liver injury (n = 19). Patients without sufficient laboratory data (n = 19) were also excluded. This left 894 patients finally enrolled (Figure 1).

Flow chart of the selection of patients for inclusion in the study on CO-induced hepatic injury. CO: carbon monoxide.
General patient characteristics
Among the 894 patients, there were 583 women (60%), and the mean age of the patients was 52 (±17) years. The number of patients with hypertension and diabetes mellitus was highest in the normal group and smallest in the hepatic injury group, but this difference was not statistically significant (hypertension; p = 0.308, diabetes mellitus; p = 0.251). Maximal exposure time was the longest in the hepatic injury group but was not significantly different between groups. HBOT was treated in 819 patients (91.6%) and not significantly different between groups. AST, ALT, total bilirubin, GGT, and lactate levels were also highest in the hepatic injury group (p < 0.001), but there was no significant difference in ALP (p = 0.925), albumin (p = 0.925), or INR (p = 0.091) between groups (Table 1).
General patient characteristics in each group of patients suffering from CO poisoning.a
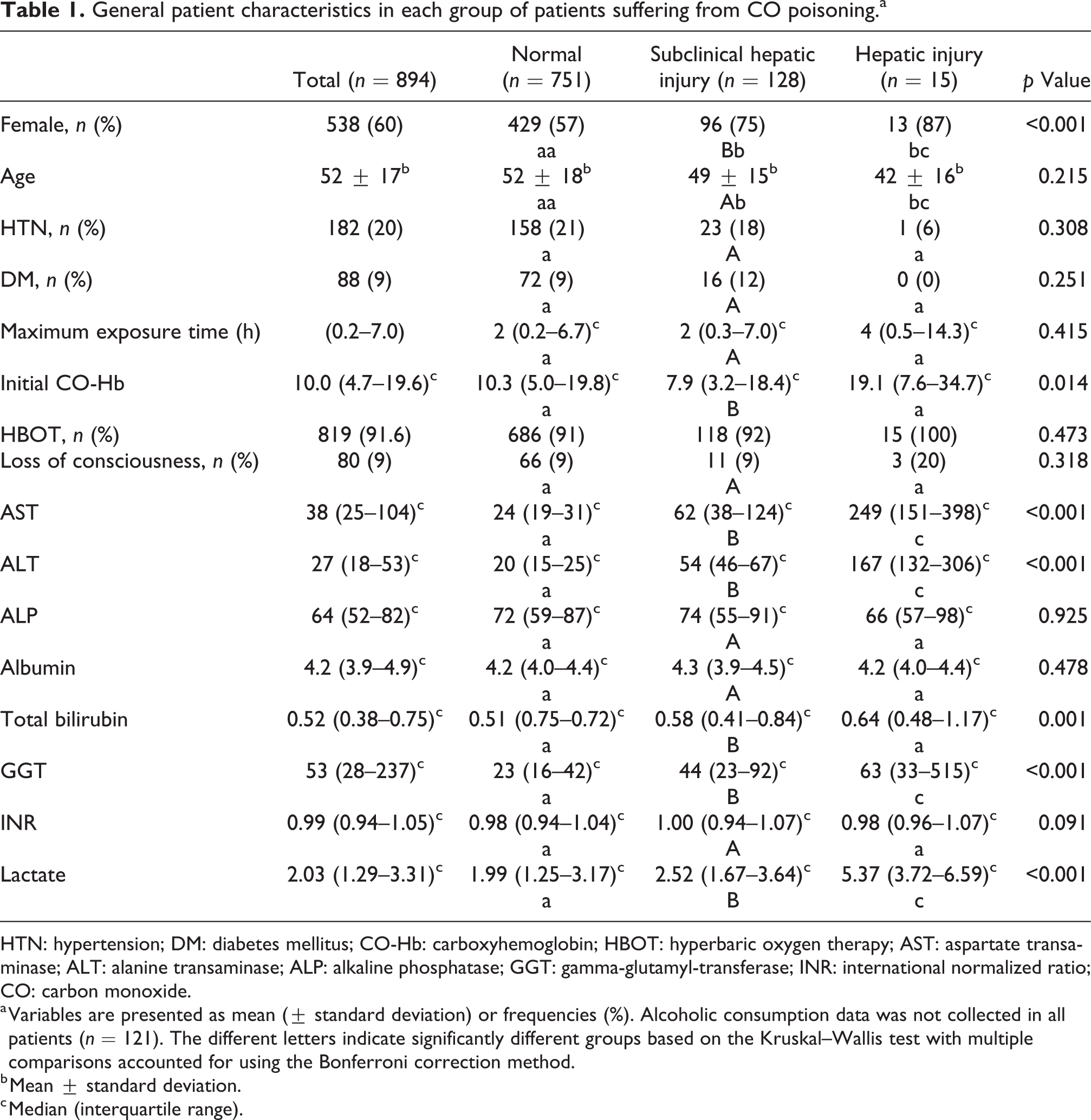
HTN: hypertension; DM: diabetes mellitus; CO-Hb: carboxyhemoglobin; HBOT: hyperbaric oxygen therapy; AST: aspartate transaminase; ALT: alanine transaminase; ALP: alkaline phosphatase; GGT: gamma-glutamyl-transferase; INR: international normalized ratio; CO: carbon monoxide.
a Variables are presented as mean (± standard deviation) or frequencies (%). Alcoholic consumption data was not collected in all patients (n = 121). The different letters indicate significantly different groups based on the Kruskal–Wallis test with multiple comparisons accounted for using the Bonferroni correction method.
b Mean ± standard deviation.
c Median (interquartile range).
Clinical outcomes and complications
There were 779 patients admitted to the general ward and discharged alive, 110 patients admitted to the intensive care unit and discharged alive, and 5 patients expired. Among the complications, delayed neurologic sequelae, acute kidney injury, secondary cardiomyopathy, and rhabdomyolysis showed statistically significant differences between the three groups (p <0.001; Table 2).
Clinical outcomes and complications in each group of patients suffering CO poisoning.

GW: general ward; ICU: intensive care unit; DNS: delayed neurologic sequelae; HBOT: hyperbaric oxygen therapy; CO: carbon monoxide.
Recovery trends of hepatic injury
The follow-up data from the hepatic injury and subclinical hepatic groups were observed, and a generally decreasing trend was found in ALT level. Within 1 week of admission with conservative management, a pattern of normalization was observed (Figure 2).

Daily serum ALT levels recorded in subclinical hepatic injury (blue line) and hepatic injury (orange line) groups. ED: emergency department; HD: hospital day; ALT: alanine aminotransferase.
Discussion
In our study, the prevalence of hepatic injury after CO poisoning was relatively small (1.6%) and the relationship with mortality was not statistically significant. However, in comparison to patients in the normal group, the admission rate to the intensive care unit and the occurrence of delayed neurologic sequelae, acute kidney injury, rhabdomyolysis, and secondary cardiomyopathy was significantly higher in the hepatic injury patient group. Patients in the hepatic injury group recovered through conservative management within 1 week of being admitted.
Hepatic dysfunction has been demonstrated in several studies to correlate with poor outcome and mortality. 18 However, in our study, the relationship between hepatic injury and mortality rate was not statistically significant. A reason for this result could be that the liver is tolerant to ischemic insult because the blood flow to the liver is supplied through both an artery and a portal system; 70% of blood flow is through the portal system. 19 The pathophysiology of hepatic injury may be similar to hypoxic hepatitis due to the reduced delivery of oxygen to the liver. When hepatocytes are exposed to ischemic assault, the cell energy supply is disrupted, causing cell edema and fatty change. The first affected area is the centrilobular area but the effects are known to be fully reversible when the blood supply recovers within 2 h. 20
According to a study by Hwang, abnormal liver function after cardiac arrest resuscitation is a benign phenomenon and liver function is restored within 2 weeks of the resuscitation. 21 Considering that the results of cardiac arrest on the liver are benign despite entry into a complete ischemic state, it is concluded that the results of CO-induced hepatic injury are also benign; only temporary ischemia is induced due to the competition for hemoglobin and hence less ischemic damage is done. This is further supported by the fact that patients recovered with conservative treatment within a week of admission. In addition, the results were influenced by the use of high-oxygen therapy to reduce the half-life of CO, and use of HBOT to reduce ischemic damage. 22 These results support that hepatic injury after CO poisoning is benign, not permanent. However, the hepatic injury itself is a temporary result of benign, generally delayed neurologic sequelae generally causes problems rather than mortality in CO poisoning. The incidence of delayed neurologic sequelae was significantly higher in the group of patients with hepatic injury than in the other groups. Therefore, clinicians should always consider that patients with early hepatic injury in the ED may have delayed neurologic sequelae. More research is expected using a prospective design.
Patients within the subclinical hepatic injury group should be considered to have received some liver damage, despite this being less than in the hepatic injury group. As with patients in the hepatic injury group, subclinical hepatic injury patients displayed no difference in mortality with normal patients, but significant differences were found in the complications of CO poisoning and delayed neurologic sequelae. There was a pattern of recovery within a week of admission with conservative management.
This study has several limitations. Firstly, the data were retrospectively collected. Secondly, there can be selection bias when studying a single medical center, even if a relatively large population has been studied. Thirdly, this study focused on the initial data processed in the ED. Further research may be needed as there is no information on the prevalence and pattern of secondary hepatic injury that may occur after CO poisoning in patients from the normal group, due to the lack of follow-up data.
Conclusion
While CO-induced hepatic injury is relatively uncommon, it can be associated with complications and poor neurologic outcome. However, CO-induced hepatic injury was not found to have a statistically significant effect on mortality rate; further study will be needed to investigate this.
Footnotes
Authors’ note
YSC and SJK contributed equally to this study as first authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health and Welfare, Republic of Korea under grant number HI18C2196.