
Abstract
Introduction:
Accidental carbon monoxide (CO) intoxication is a major cause of unintentional poisoning. This study aimed to determine the value of initial lactate levels in patients with CO poisoning and to evaluate its utilization in the emergency department (ED).
Methods:
A retrospective cross-sectional study was carried out among patients with CO intoxication, who were admitted to the ED between April 1, 2011 and April 1, 2012. The study data were extracted from a hospital database system using International Classification of Diseases-10 diagnosis codes. The patients were analyzed according to lactate levels, carboxyhemoglobin (COHb) levels, electrocardiographic manifestations, and clinical features at admission to the ED.
Results:
A total of 74 patients with CO poisoning were enrolled in this study. The average COHb value of the patients was 21.5 ± 13.9%. A total of 50 patients (67.6%) received normobaric oxygen treatment and 24 patients (32.4%) received hyperbaric oxygen (HBO) treatment. The patients who received HBO treatment had increased lactate levels compared with patients receiving normobaric oxygen treatment (2.3 mmol/L vs. 1.0 mmol/L, p < 0.001). The lactate levels were positively correlated with COHb values (r = 0.738, p < 0.001). We determined that a lactate level of 1.85 mmol/L has a sensitivity of 70.8% and a specificity of 78.0% to predict the HBO treatment needed in CO poisoning.
Conclusion:
In evaluating patients with CO poisoning, an initial lactate level could be taken into consideration as an adjunctive parameter of severity, together with the clinical criteria and levels of COHb.
Introduction
Carbon monoxide (CO) is a colorless, odorless, tasteless, and nonirritating gas generated during the incomplete combustion of carbon-based compounds. It is a common cause of poisoning, resulting in more than 40,000 cases per year in the United States with 15,200 annual visits to emergency departments (EDs). 1,2 It is also regarded as a public health problem in Turkey and other developing countries due to the widespread use of coal stoves and insecured heating systems, which have resulted in unintentional CO poisoning. 3
Normobaric and hyperbaric oxygen (HBO) treatments play an important role in the management of CO poisoning. However, there is still debate about the accuracy of HBO treatment and its application to different patient groups. 4 –7 The treatment rationale for HBO relates to reducing the risk of delayed neurologic sequelae and other complications. 6,7
Lactate is the product of anerobic glycolysis, is considered as an important marker of tissue hypoxia, and responds to several inflammatory mediators. Elevated lactate levels and lactate clearance are accepted as reliable prognostic indicators in septic and cardiogenic shock; these indicators have been increasingly used in the management of several critical patients. 8 –10 There are very few studies concerning the alteration of lactate levels in CO poisoning, even though lactate levels might be used as an indicator for tissue hypoxia and hypoperfusion. 9,11,12 The present study aimed to analyze the lactate levels in patients with CO poisoning, who were presented to an adult ED after unintentional CO exposure.
Methods
Study design
This retrospective cross-sectional study was carried out in a training and research hospital, which has approximately 120,000 ED admissions per year. Owing to the regional and local characteristics of the hospital, CO intoxication, by way of insecured heaters and coal stoves, is a common cause of admission to the ED. The study data were retrospectively extracted from the electronic database system of the hospital. Electronic analysis covered data input between April 1, 2011 and April 1, 2012. This research was conducted in accordance with the tenets of the Declaration of Helsinki.
Study protocol
Two study investigators extracted data from the hospital database system using the International Classification of Diseases-10 diagnosis codes for CO poisoning. The diagnosis of CO intoxication was established based on carboxyhemoglobin levels (COHb), related symptoms, and an identified source of CO poisoning. The exclusion criteria were patients with no accessible laboratory values and uncertain CO intoxication diagnosis.
The blood gas analysis was performed by collecting venous blood samples during the initial evaluation, and values for pH, bicarbonate, COHb, and lactate were gathered via evaluating these results. Myocardial injury was diagnosed with electrocardiographic (ECG) manifestations and increased cardiac troponin I levels (normal < 0.1 ng/mL). Indications for referral to HBO treatment were as follows: syncope, confusion/altered mental status, seizure, coma, focal neurologic deficit, pregnancy with COHb level > 15%, COHb level > 25% in any patient, and evidence of acute myocardial ischemia.
According to our laboratory test limits, lactate levels below 2.1 mmol/L were considered normal. The subjects were divided into two groups and compared based on their HBO treatment status. The referral for HBO treatment was considered an important sign of severe poisoning, and along with the above-mentioned criteria, alterations in lactate levels were also evaluated in both groups. Data were collected from all patients on age, sex, vital signs, ECG features, and laboratory values including renal function tests, cardiac biomarkers, and venous blood gas analysis.
Statistical analysis
Statistical analyses were performed with Statistical Package for the Social Sciences for Windows (version 11.0; SPSS Inc., Chicago, Illinois, USA). Student’s t test was used in the analysis of groups of continuous variables with normal distributions, and data were expressed as mean ± standard deviation. The Mann–Whitney U test was performed in the analysis of groups of continuous variables with nonnormal distribution, and data were expressed with medians (interquartile range). Categorical variables were shown with the number of cases and percentages and evaluated using Pearson’s χ 2 test. The Spearman correlation was used for the relationship between COHb values and lactate levels. A receiver operating characteristic (ROC) curve analysis was carried out to determine the sensitivity and specificity of elevated lactate levels in patients with severe CO poisoning. An α value of 0.05 was accepted as the nominal level of significance.
Results
A total of 74 patients with CO poisoning were enrolled in this study. Subjects consisted of 30 male (40.5%) and 44 female (59.5%) patients. All the patients were accidentally exposed to CO gas due to insecured heating systems or coal stoves. All patients were discharged from hospital within 12–24 h. Neurological worsening or death was not observed among the study group. The average COHb value was 21.5 ± 13.9%. Baseline characteristics of the study population are shown in Table 1.
Baseline characteristics of the study population.

IQR: interquartile range; COHb: carboxyhemoglobin; BUN: blood urea nitrogen; HCO3: bicarbonate.
The most common patient complaints were headache (27%), lightheadedness (22%), and nausea and vomiting (32%). Altered mental status was observed in 20 patients (27.0%), whereas only 9 patients (12.2%) presented with chest pain. According to ECG readings, 8 patients (10.8%) had ischemic ST segment and T wave abnormalities. Twenty-four patients (32.4%) received HBO treatment after the initial assessment was accomplished.
The comparison of patients with CO poisoning according to HBO treatment status is shown in Table 2. The patients who received HBO treatment had increased lactate levels compared to patients with normobaric oxygen treatment (2.3 mmol/L vs. 1.0 mmol/L, p < 0.001).
Comparison of patients with CO poisoning regarding to HBO treatment.
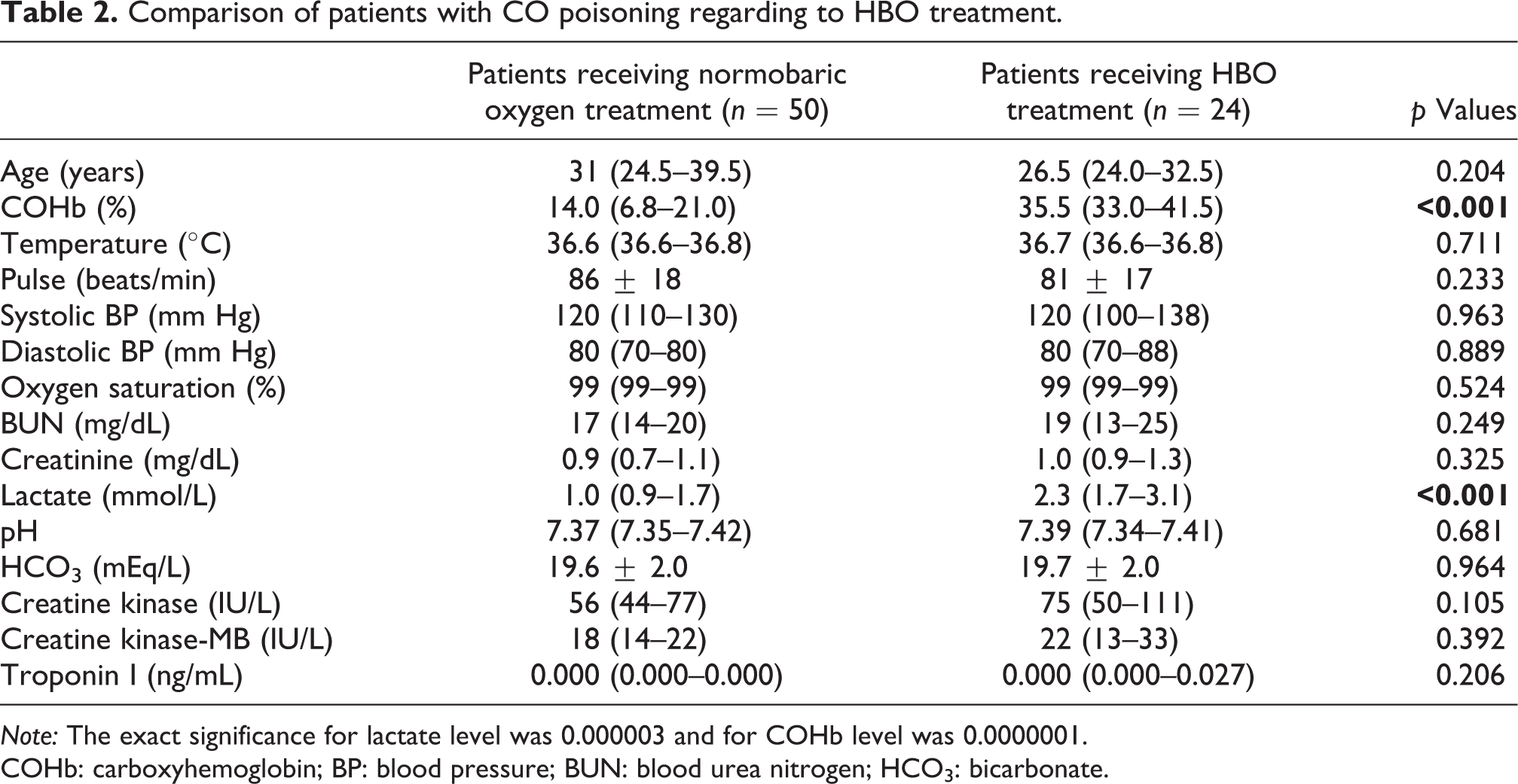
Note: The exact significance for lactate level was 0.000003 and for COHb level was 0.0000001. COHb: carboxyhemoglobin; BP: blood pressure; BUN: blood urea nitrogen; HCO3: bicarbonate.
Elevated lactate levels (≥2.1 mmol/L) were observed in 19 patients (25.7%) and 55 patients (74.3%) had normal lactate levels. Altered mental status was more common in patients with elevated lactate levels (73.7% vs. 10.9%, p < 0.001). Elevated lactate levels were not associated with either chest pain (p = 0.223) or ischemic ECG findings (p = 0.192) during ED admission. However, lactate levels were positively correlated with COHb values (r = 0.738, p < 0.001).
We constructed an ROC curve to determine the accuracy of predicting HBO treatment status, and the area under the curve for plasma lactate concentration was 0.838 (95% confidence interval, 0.743–0.933; p < 0.001; Figure 1). When the lactate level was 1.85 mmol/L, sensitivity of 70.8% and specificity of 78.0% were found. Also we found that a lactate level of 1 mmol/L had a negative predictive value (NPV) of 96.3%. Different criterion values and coordinates of the ROC curve are shown in Table 3.

Receiver operating characteristics (ROC) curve analysis.
Criterion values and coordinates of the ROC curve.
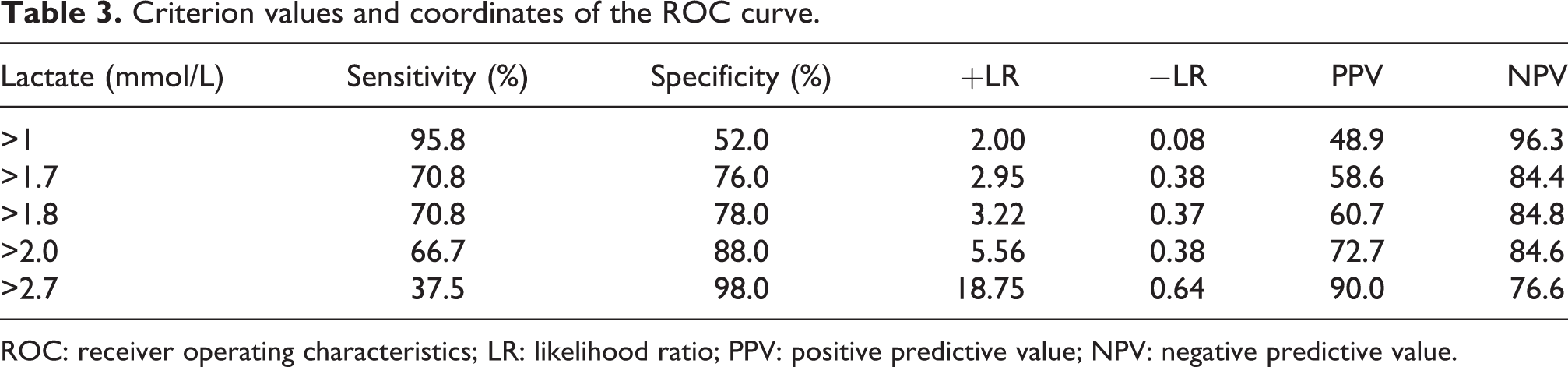
ROC: receiver operating characteristics; LR: likelihood ratio; PPV: positive predictive value; NPV: negative predictive value.
Discussion
The present study suggests that COHb levels are positively correlated with initial lactate levels in CO poisoning. Patients who received HBO treatment had elevated plasma lactate concentrations and also had more frequent altered mental status. Although HBO treatment indications widely vary in different settings, generally accepted indications for HBO treatment are the presence of significantly increased COHb values, and neurologic or cardiac deterioration. Regarding our results, a lactate value >1.85 mmol/L can predict the need for HBO treatment, which could be taken as a measure of severe poisoning.
Although lactate levels have been increasingly used in the decision-making process of several critical patients, 8 –10 few studies have utilized this value in CO intoxication. The literature on lactate levels and intoxication mainly deal with alcohol intoxication, salicylate poisoning, and paraquat poisoning. 13 –15 In these studies, the role of the initial lactate level to predict the prognosis of the patients was not clearly established. Also, the number of studies dealing with alterations of lactate levels in CO poisoning is extremely low. Some studies concluded that severe poisonings were associated with a prominently higher blood lactate level, compared to mild and moderate cases. 9,12,16 Benaissa et al. conducted an observational study in patients with CO poisoning by dividing patients into different neurological impairment groups. They stated that unintentional CO exposure resulted in a mild elevation in plasma lactate concentration. However, this elevation was not useful in distinguishing the severity of neurological impairment due to the extensive overlap between the lactate levels of the groups. 12 Regarding our results, elevated lactate levels were observed in patients with an altered mental status. This finding was also consistent with the results of Moon et al. who found that the patients with high plasma lactate levels had a higher incidence of altered mental status on admission. 9 However, the development of delayed neuropsychological sequelae after CO poisoning is probably not associated with plasma lactate concentrations, 2 although initial lactate levels were related to altered mental status.
In the current study, we found a strong correlation between COHb values and lactate levels (r = 0.738, p < 0.001). The correlation coefficient was weaker in studies by Sokal and Kralkowska (r = 0.340, p < 0.05) and Moon et al. (r = 0.493, p < 0.001). 9,13 This finding may be attributed to the relatively high COHb values (mean: 21.6 ± 13.1%) in our study.
Plasma lactate concentrations are influenced by several factors, and elevated lactate levels may result from the effects of several toxic mechanisms associated with CO poisoning. 9 Tissue hypoxia, as a consequence of the mitochondrial oxidative capacity impairment, may play a role in the increased lactate production. 17 In our study, patients with HBO treatment had no cardiovascular collapse or significant hemodynamic abnormalities compared with patients who received normobaric oxygen treatment. This finding might be related to early cellular changes in the oxidative capacity without causing any alteration in hemodynamic variables.
HBO treatment is still a conflicting issue in CO poisoning. When indications for HBO treatment were taken into account, plasma lactate concentrations were also elevated in those conditions (COHb > 25%, neurologic impairment, altered mental status). An elevated lactate level can predict the need for HBO treatment, and this finding may help clinicians to better identify patients with severe CO poisoning. We also found that a lactate level of 1 mmol/L had an NPV of 96.3%, which could be used as a cutoff value for significant CO poisoning.
Lippi et al. stated that the clinical spectrum of heart involvement in patients with CO intoxication is rather broad and may present with different clinical features. 18 This may explain higher troponin I levels in different study groups. Our study group consisted of relatively young patients, and they had probably lesser underlying coronary artery disease, which may result in negative troponin levels in case of severe poisoning.
Our study had several limitations. First, even though the study was carried out during a 1-year period, the sample size was relatively small, and in particular, the number of patients with elevated lactate levels was low. Second, this was a retrospective single-center study, which limits its generalizability. Third, the lactate clearance values might have been more useful in assessing patients with severe poisoning. However, we could not calculate the lactate clearance by obtaining a second lactate level due to the retrospective design of the study.
In conclusion, in evaluating patients with CO poisoning, an initial lactate level could be taken as a measure of severe poisoning at admission to the ED. Lactate levels could also determine the need for HBO treatment; however, this finding should be validated in studies concerning short- and long-term neuropsychiatric sequelae and delayed encephalopathy due to CO poisoning.
Footnotes
Conflict of interest
The authors declared no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.