
Abstract
Purpose:
The aim of this study was to investigate the demographic and clinical characteristics and treatment modalities of elderly patients with carbon monoxide (CO) intoxication. The secondary aim was to evaluate the importance of plasma lactate values in the diagnosis of acute CO intoxication in geriatric patients.
Methods:
Data on geriatric patients who were admitted to the emergency department of Atatürk University Medical Faculty between January 2013 and April 2016 were analyzed retrospectively.
Results:
Of the 197 cases included in the study, 97 were in the intoxication group and 100 were in the control group; 82.5% of the intoxication cases had mild neurological symptoms and 17.5% had severe neurological symptoms. Carboxyhemoglobin levels were significantly higher in patients with severe neurological symptoms (p = 0.031). All patients with severe neurological symptoms received hyperbaric-oxygen therapy (p < 0.001). In the intoxication group, lactate levels were significantly higher than in the control group (p = 0.001). The specificity for lactate 4 mmol/L and above was found as 98.0% with a positive predictive value and negative predictive value of 84.5% and 53.3%, respectively.
Conclusion:
High initial lactate levels may be a guide for cases with nonspecific symptoms in geriatric patients with suspected CO intoxication.
Introduction
Carbon monoxide (CO) is a toxin in the gas form that binds to hemoglobin with an approximately 200 times greater affinity than oxygen. Carboxyhemoglobin (COHb), caused by binding of CO to hemoglobin, causes severe hypoxia in the tissues. 1 For this reason, the tissues most affected by intoxication are the brain and heart, in which the demand for oxygen is the highest. Symptoms of CO intoxication may vary depending on the level of exposure. In mild exposure, nonspecific symptoms such as headache, myalgia, and nausea were observed; severe exposure may result in myocardial ischemia, impaired consciousness, and death. 2
COHb measurement alone in CO intoxication is not sufficient for diagnosis and treatment determination. A diagnosis is made according to the patient’s clinical status. 3 The patient’s history, symptoms, and COHb levels should be evaluated together for CO exposure. However, COHb levels in acute intoxication may not always correlate with symptoms, clinical findings, and patient prognosis. Even in the presence of severe CO intoxication, COHb levels may be normal. Therefore, more reliable laboratory parameters than COHb levels in CO intoxication are urgently needed.
Lactate is the final product of anaerobic glycolysis when the oxygen supply to the tissues is insufficient. Hypoxia, which is the deadly mechanism of CO intoxication, leads to anaerobic glycolysis and lactate formation. Therefore, plasma lactate levels have been used in the care of patients with CO intoxication as well as in critically ill patients. In addition, it is known that laboratory values of CO intoxication cases are affected in different ways. Metabolic stress in acute poisoning and hypoxia causes an increase in white blood cell (WBC) values in the complete blood count and especially in the circulating neutrophil count. 4 The reflection of this increase in the neutrophil–lymphocyte ratio (NLR) can be used as a marker for detecting and assessing the severity of CO intoxication cases. NLR values are used to assess the clinical status and prognosis of patients with cardiac and cerebral ischemia, inflammation-related conditions, and malignancy. 5
The first and only choice of treatment in all CO intoxication cases is normobaric oxygen therapy. Hyperbaric-oxygen therapy (HBOT) is recommended for patients with serious CO poisoning manifested by transient or prolonged unconsciousness, abnormal neurologic signs, cardiovascular dysfunction, or severe acidosis; patients who are 36 years of age or older; those were exposed for 24 h or more (including intermittent exposures); or those who display a COHb level of 25% or more. 6 The main purpose of the application of HBOT is to reduce the rates of delayed cognitive sequelae.
Being over 65 years of age is a risk factor for increased mortality alone in CO intoxication cases. 7 The geriatric population is more severely affected by CO intoxication; many patients are diagnosed late and unfortunately cannot be saved. There are not many studies on this particular vulnerable patient population. The primary aim of this study was to evaluate the demographic characteristics, clinical features, and treatment modalities of geriatric CO intoxication cases admitted to our emergency department. The secondary aim was to investigate whether high plasma lactate levels at the time of admission were diagnostic for CO intoxication.
Methods
Research design
In this study, from January 2013 until April 2016, patients of a university hospital with available system data and laboratory results were analyzed retrospectively. Approval was given by the institutional ethics committee.
Patient selection
Patients older than 65 years (geriatric) who were admitted to the emergency department and diagnosed with CO intoxication were included in this study. Demographic data, presenting complaints, physical examination findings, electrocardiography (ECG) findings, laboratory findings, and treatment information were scanned from patient files and the electronic information system. Patients with acute or chronic infection, chronic organ failure (liver, kidney, heart, etc.), hematological disease, a history of malignancy, and alcohol or cigarette addiction were excluded from CO intoxication group (Figure 1). Also, patients with >2% methemoglobinemia and a closed-space fires experience were excluded as well. In this study, only isolated CO intoxication patients were reviewed.
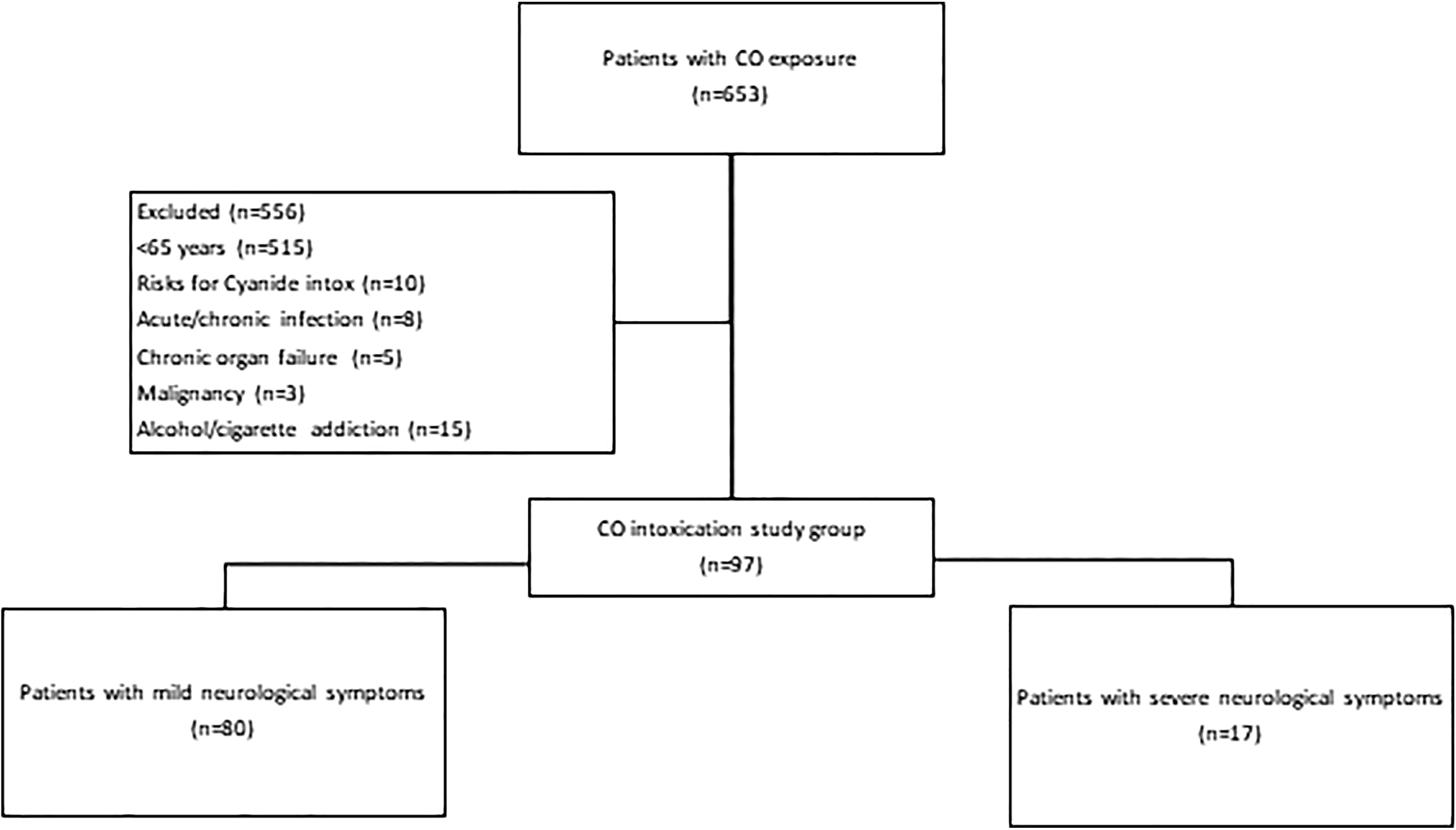
Study flow chart: patient selection. CO: carbon monoxide.
In addition, a normal control group was created to compare plasma lactate levels and other laboratory findings. The control group consisted of patients over the age of 65 who presented to the emergency department with the single complaint of “headache” within the same date range. The “headache” complaint is the most common and often the first finding in 80–90% of patients with acute CO intoxication. 8 Patients who were included in the control group had no CO exposure, but blood COHb levels were measured for the differential diagnosis of headache. Patients with acute or chronic infection, chronic organ failure (liver, kidney, heart, etc.), hematological disease, a history of malignancy, and alcohol or cigarette addiction were excluded from this group as well. Patients with vital instability which may cause headaches, patients with a diagnosis of neurological disease in the emergency room or prior, patients with abnormalities on a neurological examination, and patients with a COHb level of 3% or higher were not included in the control group. 3 The two patient groups were similar in terms of age and gender distribution.
Study protocol
Cases with CO exposure were examined in two groups as “mild” and “severe” according to the presenting symptoms. Patients presenting with common neurological symptoms such as headache, nausea, and dizziness were named as the mild case group. Patients presenting with more serious neurological symptoms like a change in consciousness, syncope, convulsion/confusion, coma, and focal neurological deficit were the severe case group.
In accordance with the routine approach to treatment of CO intoxication in our clinic, blood was collected from the peripheral artery in order to examine arterial blood gas within the first 10 min after admission. In this study, blood gas data obtained by using an ABL 800-flex Radiometer (Radiometer Medical ApS, Bronshoj, Denmark), biochemical markers, and blood count data were examined. COHb; lactate; creatine kinase (CK); troponin I values; and WBC, neutrophil, and lymphocyte counts were evaluated. The neutrophil count was divided by the lymphocyte count, and the NLR was calculated. For lactate, values of 2 mmol/L and above were considered as “high lactate.” For troponin I, values of 0.1 ng/mL and above were considered to be above normal (positive).
Intoxication cases were divided into two groups in terms of COHb levels. COHb levels of 25% and above were evaluated as COHb group 1, and COHb levels under 25% were evaluated as COHb group 2. 9
HBOT is planned for cases with signs and symptoms of “high risk” CO intoxication in our clinic. In our routine practice, HBOT is indicated for patients with symptoms and signs of neurological and cardiac involvement, COHb levels of 25% and above, the presence of metabolic acidosis, and an exposure history of 24 h or more. Patients who received HBOT in our study were classified as “high risk intoxication cases.”
The 12-lead ECG findings of the patients were examined in the system, and ST elevation ≥1 mm in the following two leads and those with the presence of ST depression ≥ 0.5 mm or T-wave inversion ≥2 mm were classified as having “ischemic ST-T changes.” 10
Statistical analysis
All statistical analyses were performed using Statistical Package for the Social Sciences for Windows 20.0 (Chicago, Illinois, USA). Categorical variables belonging to both patient groups were expressed as percentages and numerical values. Values of continuous variables were expressed as means (with standard deviations) and medians (with interquartile ranges). The normal distribution of continuous variables was assessed by the Shapiro–Wilk test. Student’s t-test or the Mann–Whitney U test was used to compare the normal distribution of continuous variables in binary comparisons. For categorical variables, the χ 2 test was used. Logistic regression analysis was used to evaluate the variables (age, symptoms, laboratory findings) that may affect the outcome of HBOT. Spearman’s and Pearson’s correlation analyses were used to evaluate the relationship between COHb levels and laboratory parameters of intoxication cases. Receiver operating characteristic curve analysis was used to evaluate the sensitivity and specificity of increased lactate levels in detecting CO intoxication. The confidence interval (CI) was determined as 95%, and a value of p < 0.05 was accepted as statistically significant.
Results
A total of 197 patients were included in the study, 97 in the CO intoxication group and 100 in the control group. The mean age of intoxication cases was 75.9 ± 7.8, 49.5% were female, and 50.5% were male. The mean age in the control group was 74.3 ± 6.2, 43% were female, and 57% were male. There was no significant difference in the age (95% CI: −3.73 to 0.22; p = 0.080) or gender (p = 0.361) distribution between the two groups (Table 1).
Demographics, vitals, and laboratory findings of the patient groups.

CK: creatine kinase; CO: carbon monoxide; DBP: diastolic blood pressure; HR: heart rate; IQR: interquartile range; NLR: neutrophil–lymphocyte ratio; RR: respiratory rate; SD: standard deviation; SBP: systolic blood pressure; WBC: white blood cell. The difference in lactate levels was statistically significant (p = 0.001).
The most common patient complaint was headache (56%) in CO intoxication cases, and in 22.7% of cases, headache was the only complaint. The most common symptoms associated with headache were nausea-vomiting (24.7%) and dizziness (11.3%). Of the intoxication cases, 82.5% had mild neurological symptoms and 17.5% had severe neurological symptoms. Cardiac symptoms (palpitation, chest pain, shortness of breath) were present in 2.1%. The median value of the Glasgow Coma Scale score was 15. Ischemic ST-T changes were observed on the ECG in 18.6% of cases. ECG was arrhythmic in 22.7% of cases. The incidence of ischemic ST-T changes (35%, 6 of 17 cases) on the ECGs of patients with severe neurological symptoms was found to be higher than in those with mild neurological symptoms (15%; p = 0.05).
The mean COHb value of the intoxication cases was 15 ± 1.3. In terms of these levels, 21.6% of the cases were group 1 and 78.4% were group 2. The rate of COHb in group 1 was significantly higher among patients with severe neurological symptoms (p = 0.031). There was no correlation between COHb levels and other laboratory findings.
HBOT was applied to 49.5% of CO intoxication cases. All cases with severe neurological symptoms were found to have received HBOT (p < 0.001). However, 67% of cases with ischemic ST-T changes had HBOT (p > 0.05). Of the 82 patients (52.4%) who were positive for troponin I, 43 had received HBOT. There was no significant increase in CK, troponin I, lactate levels, and NLR in cases with CO intoxication (p > 0.05). No parameters other than COHb levels were found to be associated with the treatment decision, which could affect the decision to administer HBOT in intoxication cases. Only COHb was significantly associated with HBO treatment (p < 0.001; odds ratio: 1.177; 95% CI: 1.095–1.266).
Among intoxication cases, 44.3% had high lactate. Blood lactate levels were examined for an association with two critical conditions: having HBOT treatment and the presence of severe neurological symptoms. There was no significant relationship between them (p > 0.05). There was no significant increase in lactate levels in the COHb group 1 (p > 0.05). There was a weak correlation between lactate and NLR (r = 0.205, p = 0.04).
Lactate, CK, and troponin I levels were higher in CO intoxication cases than in controls (Table 1). The difference in lactate levels was statistically significant (p = 0.001). The area under the curve for predicting CO intoxication was 0.65 (95% CI: 0.57–0.73; p < 0.001; Figure 2) for blood lactate. The diagnostic sensitivity and specificity for CO intoxication with a lactate value of 2 mmol/L were 51% and 80%, respectively. When the lactate level was 4 mmol/L and above, the specificity was found as 98.0%. And at this lactate level, positive predictive value and negative predictive value were found as 84.5% and 53.3%, respectively. NLR was high in both groups (Table 1), but there was no significant difference between the two patient groups (p > 0.05).

ROCs curve analysis of plasma lactate levels for predicting the HBOT. ROC: receiver operating characteristic; HBOT: hyperbaric-oxygen therapy.
Discussion
We examined the geriatric patient group treated in the emergency department for acute CO intoxication and compared these patients with the geriatric control group with similar characteristics. The main results of our study can be summarized as follows: (1) In the geriatric patient population, the presence of severe neurological symptoms (change in consciousness, syncope, convulsion/confusion, coma, focal neurological deficits) may be more important than other findings in the HBOT decision. (2) Among the laboratory examinations in geriatric CO intoxication cases, which we requested routinely in the emergency room, only COHb levels were found to be associated with HBOT. (3) It was observed that plasma lactate levels were increased at the time of admission in patients with geriatric acute CO intoxication, and this increase was statistically significant when compared with normal geriatric cases.
HBOT is recommended for high risk CO intoxication cases. However, there is still a debate about whether HBOT is better than normobaric oxygen alone or how the HBOT treatment process will work. 11 There are studies in the literature showing the efficacy of HBOT on survival and neurological sequelae formation in CO intoxication. 7,12 In our study, all patients with severe neurological symptoms, that is, neurologically “high risk” patients, received HBOT. However, only slightly more than half of the subjects who had ischemic ST-T changes in the ECG or who were positive for troponin I had received HBOT, which was expressed as “high risk.” Looking at these results, we found that the main guide in the HBOT decision was neurological symptoms. Increased predisposition to CO-induced neuronal hypoxia may be the main reason for this condition in elderly patients due to atherosclerosis in cerebral vessels. 13 We believe that ECG and troponin are inadequate as auxiliary tests in elderly patients because in the geriatric population, ST-T changes can be seen on ECG without acute cardiac ischemia, and the frequency of factors that may affect troponin I levels is increasing. 14 In addition, the rate of HBOT-treated cases was found to be significantly higher in our study compared with similar studies, and we believe that the most important reason for this is the high average age in our study group. 15
COHb levels in acute intoxications may not always be indicative of symptoms, clinical findings, and prognosis. 16 Even in cases of severe CO intoxication, normal COHb levels may be observed. The main reason for this is that the half-life of COHb is quite short, and the variability in the time taken for patients to reach the emergency department can prolong the process of laboratory examination. However, high COHb levels on admission to the emergency department are associated with long-term neurological sequelae development. 17 In their study, Cevik et al. showed that the mean COHb levels were higher in “severe” CO intoxication cases than in other groups. 18 In our study, COHb levels were frequently 25% or higher in cases with severe neurological symptoms.
Ideas differ on how plasma lactate levels can be used in the diagnosis and treatment of patients presenting with CO intoxication. Considering that the intoxication mechanism is tissue hypoxia, it is still controversial that high lactate levels may be an important predictor of the patient’s clinical condition. Benaissa et al. found no evidence to support lactate measurement in CO intoxication. 19 Cervellin et al., on the other hand, stated that high lactate levels are important in patient triage and may be used as prognostic markers. 2 In our study, initial plasma lactate values of geriatric patients with CO intoxication were significantly higher than those in a control group with similar features. However, we did not find any evidence that these lactate levels could be effective in the differentiation of critical patients and the decision to administer HBOT in cases of intoxication. Therefore, we believe that lactate levels at the time of diagnosis may be helpful in the diagnosis of geriatric patients with suspicion of CO intoxication, but they cannot be useful in patient management.
High NLR has been associated with a serious clinical course and mortality in many diseases in the literature. 20,21 However, a study comparing the effectiveness of NLR in the treatment decision in CO intoxication cases and comparing it with the NLRs of the normal patient group has not been found in the literature. There are publications showing that neurological and cardiac effects of CO intoxication are associated with higher NLR values. 22,23 The mean NLR of both groups in our study was quite high. In our study, we found that NLR was not a reliable parameter in the differentiation of CO intoxication cases. This may be because NLR is a value that varies with age and is particularly high in the geriatric population. 24
Limitations
One of the most important limitations of our study was the unavailability of data on how long after exposure CO intoxication cases were delivered to the emergency department. Changes in COHb values could be evaluated more accurately by including these periods. In addition, receiving HBOT was accepted as a critical outcome. The evaluation of short- and long-term mortality rates as a critical outcome may also be a guide for the geriatric patient population.
As a result, lactate levels at the time of presentation may be supportive and may guide the diagnosis of CO intoxication in geriatric patients with nonspecific symptoms. According to the results of our study, the measurement of COHb levels in our routine practice continues to be important in the differentiation of critical patients. The findings associated with cardiac ischemia in CO intoxication do not always reflect the acute picture in elderly patients. Therefore, the most important and indispensable element to be considered in the treatment decision is the patient’s symptoms.
Footnotes
Acknowledgment
We thank Prof Zeynep Gökcan Çakır for providing access to the archive of the Emergency Medicine Department.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.