
Abstract
This article presents updated information on the worldwide burden of carbon monoxide (CO) poisoning. The worldwide epidemiologic data were obtained from the Global Health Data Exchange registry, a large database of health-related data maintained by the Institute for Health Metrics and Evaluation. The worldwide cumulative incidence and mortality of CO poisoning are currently estimated at 137 cases and 4.6 deaths per million, respectively. The worldwide incidence has remained stable during the last 25 years, while both mortality and percentage of patients who died have declined by 36% and 40%, respectively. The incidence of CO poisoning does not differ between sexes, whilst mortality is double in men. The incidence shows two apparent peaks, between 0–14 years and 20–39 years. The percentage of patients who died constantly increases in parallel with aging, peaking in patients aged 80 years or older. The number of CO poisoning grows in parallel with the socio-demographic index (SDI), though more detailed analyses would be needed to confirm our findings. Mortality displays a similar trend, being approximately 2.1- and 3.6-fold higher in middle and middle-to-high than in low-to-middle SDI countries. In conclusion, while these data suggest that the worldwide burden of CO poisoning remains stable, and the number of fatal outcomes and percentage of patients who die have both consistently declined during the last 25 years, the unreliability of the primary data sources in many countries with respect to accurate diagnosis of CO poisoning means that caution is required, and that field studies, particularly in poorer countries, are required.
Introduction
Carbon monoxide (CO) is an odorless, colorless, and tasteless molecule, which is normally present in the atmosphere at a concentration of approximately 0.03–0.20 parts per million. This gas can be generated by natural or anthropogenic sources, especially by incomplete combustion of fossil fuels and biomasses 1 . The toxicity of CO is mostly attributable to its capability to diffuse into the erythrocytes and bind to hemoglobin, for which CO has a nearly 200-fold higher affinity than oxygen. In poisoned patients, both oxygen and CO compete for binding to hemoglobin, but even small volumes of CO dissolved in the blood may be effective to largely displace oxygen binding (i.e. the so-called Haldane effect). 2 The severity of symptoms is conventionally determined by the exposure values of CO and the consequent carboxyhemoglobin (COHb) level, whose normal concentration in blood is typically comprised between 0.5% and 1.5% in non-smokers. 1 A CO concentration between 10% and 20% is usually accompanied by nausea, fatigue, tachypnea, emotionality, confusion, and clumsiness, CO levels between 21% and 30% is accompanied with headache, exertional dyspnea, angina, visual impairment, and decreased sensory perception, and that between 31% and 50% is accompanied with dizziness, fainting, confusion, nausea, vomiting, visual impairment, and problematic decision-making, while CO values >51% typically trigger seizures, coma, severe acidosis, and death. 3 Toxic exposures more frequently occur from faulty heaters, fires, industrial accidents, and car exhausts. 4
Several lines of evidence clearly attest that most cases of CO poisoning are preventable. 5 Moreover, both uneasy diagnosis and underestimation of severity of the CO poisoning may contribute to foster adverse outcomes and even tragic consequences, with some patients discharged to the environment that has previously poisoned them. 6 Among the various measures that can be established for lowering the clinical, societal, and economic burden of CO poisoning, public health surveillance, accurate diagnosis, and accurate prehospital strategies are pivotal for supporting prevention and intervention activities. 5 Nevertheless, these initiatives need major alertness and responsibility from clinicians, public health practitioners, and policy makers, which can only be obtained by providing accurate and updated epidemiologic information. Therefore, the aim of this article is to present updated data on the worldwide burden of CO poisoning.
Materials and methods
Worldwide epidemiologic information on CO poisoning was garnered from the Global Health Data Exchange (GHDx) registry, a large database of health-related data maintained by the Institute for Health Metrics and Evaluation. 7 This large catalogue encompasses data on over 350 human pathologies obtained from 195 different countries and territories. The information derives mostly from survey or surveillance data, admission and outpatient records, health insurance claims, and literature studies from approximately 69,000 sources. 8
A specific search was carried out in the GHDx database for the condition “poisoning by carbon monoxide” (i.e. respiratory conditions due to CO inhalation from burning materials, accidental poisoning by, and exposure to CO during unspecified activity, while engaged in leisure activity, working for income, engaged in other types of work, resting, sleeping, eating, or during unspecified activity). The CO poisoning data in the GHDx repository have been collected from 308 site-years, accounting for 5 of 7 Global Burden of Disease super-regions (i.e. 71.4% world coverage). The electronic search was performed with a selection of various epidemiologic variables, such as “measure” (“incidence” AND “deaths”), sex (“male” AND “female”), “metric” (“number”), “year” (“1992” AND “1997” AND “2002” AND “2007” AND “2012”AND “2017”), “Age” (“Under 5” AND “5 to 9” AND “10 to 14” AND “15 to 19” AND “20 to 24” AND “25 to 29” AND “30 to 34” AND “35 to 39” AND “40 to 44” AND “45 to 49” AND “50 to 54” AND “55 to 59” AND “60 to 64” AND “65 to 69” AND “70 to 74” AND “75 to 79” AND “80 plus”), and “location” (“Low SDI” AND “Low-middle SDI” AND “Middle SDI” AND “High-middle SDI” AND “High SDI”, where SDI stands for socio-demographic index). The rate of CO-poisoned patients who died for this reason is expressed as the percentage of patients who died. The year 2017, the last searchable in the GDHx database, was selected for providing the most recent statistics on the worldwide burden of CO poisoning. The final output of the electronic search was downloaded in comma-separated values, imported into an Excel file (Microsoft, Redmond, Washington, USA). Pearson’s correlation (r) was used for assessing potential associations among epidemiologic variables, while the overall risk was finally reported as odds ratio (OR) and 95% confidence interval (95% CI). The statistical analysis was then carried out with Analyse-it (Analyse-it Software Ltd, Leeds, UK) and MedCalc statistical software (MedCalc Software, Ostend, Belgium). The study was performed in accordance with the Declaration of Helsinki, under the terms of relevant local legislation. Ethics board approval is unnecessary at the local institution (University of Verona) for articles based on free scientific database searches.
Results
According to GDHx data, the worldwide cumulative incidence and mortality of CO poisoning in 2017 were estimated at 137 cases per million and 4.6 deaths per million, respectively. The trend of both incidence and mortality recorded during the last 25 years is shown in Figure 1. Although no significant correlation (r) can be observed between time (i.e. years) and incidence of CO poisoning (r = 0.40; 95% CI, −0.61 to 0.92; p = 0.427), the mortality for this pathology has exhibited a highly significant and time-dependent decrease (r = −0.96; 95% CI, −1.00 to −0.64; p = 0.003). The risk of dying for CO poisoning has hence declined by 36% (OR, 0.64; 95% CI, 0.44–0.92; p = 0.018) between the years 1992 and 2017, from 7.2 cases to 4.6 cases per million population. The combination of a virtually stable incidence with declining mortality is then reflected by a 40% decrease of the percentage of patients who died (i.e. CO poisoned patients who died) recorded during the last 25 years, from 5.5% in 1992 to 3.4% in 2017 (OR, 0.60; 95% CI, 0.59–0.61; p < 0.001).

Worldwide epidemiology and last 25-year trend of CO poisoning. CO: carbon monoxide.
The incidence and mortality of CO poisoning in the two sexes are given in Table 1. Although the number of cases is virtually identical, the mortality for CO poisoning is nearly double in men than in women. The age-related distribution of CO poisoning is shown in Figure 2. The incidence shows two apparent peaks, the former between 0 year and 14 years (∼31% of all cases) and the latter between 20 years and 39 years (∼34 of all cases). The mortality seems instead more heterogeneous, without displaying a specific pattern. Most CO-related deaths seem clustered in the age range between 25 years and 69 years (∼63% of all deaths), while the highest overall value is then observed after the age of 80 years (∼9% of all deaths). The pattern of the percentage of patients who died is instead straightforward, constantly increasing in parallel with aging (r = 0.94; 95% CI, 0.83–0.98; p < 0.001). Notably, the risk of dying after CO exposure was found to be nearly double in infants (<5 years; OR, 1.83 and 95% CI, 1.69–1.99; p < 0.001) and approximately 26-fold higher in very elderly patients (≥80 years; OR, 25.8 and 95% CI, 23.9–27.9; p < 0.001) than in children aged 5–9 years.
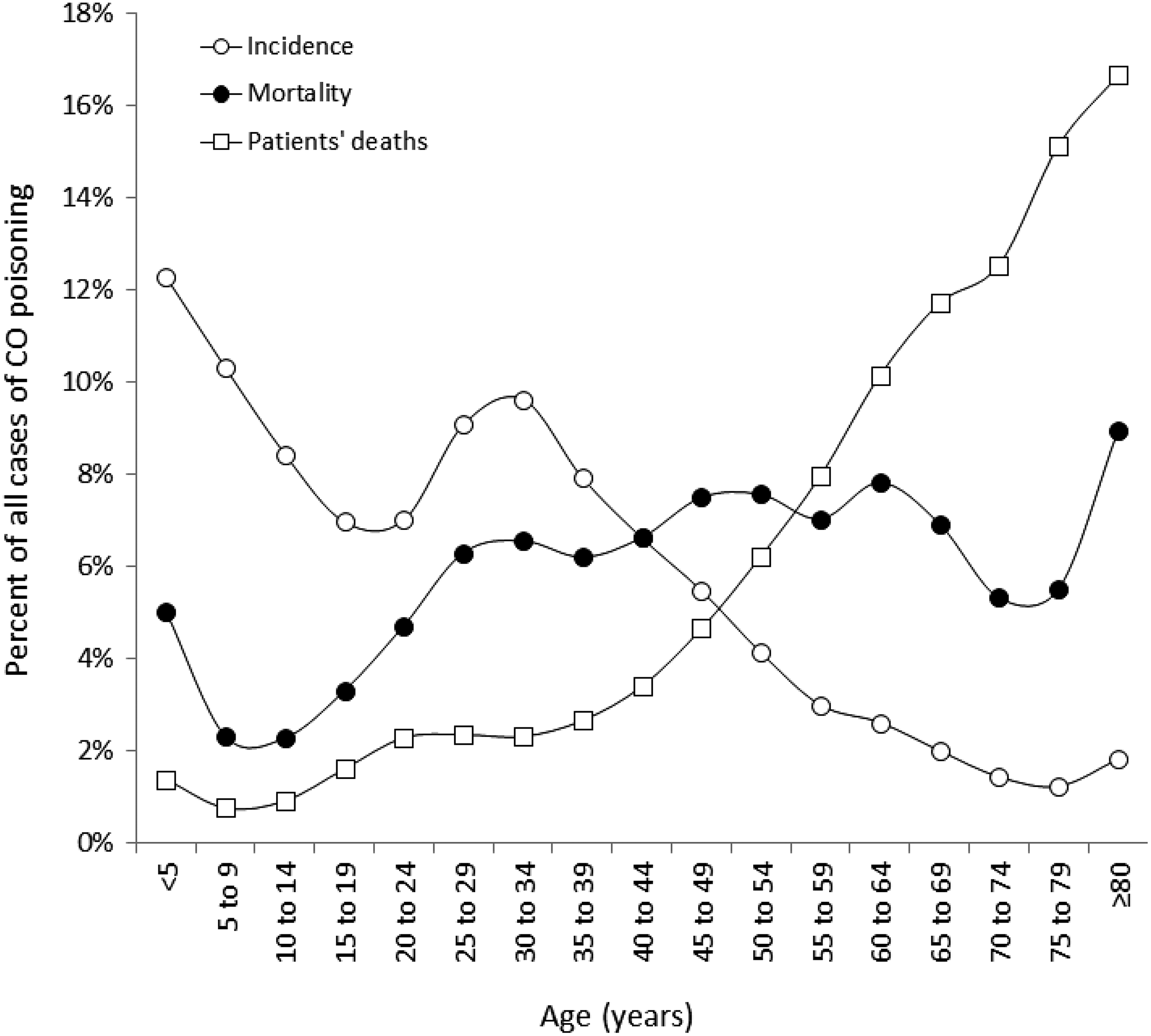
Worldwide epidemiology of CO poisoning in different age groups. CO: carbon monoxide.
Worldwide epidemiology of CO poisoning by sex.

CO: carbon monoxide; OR: odds ratio; CI: confidence interval.
a Per million.
The incidence and mortality of CO poisoning stratified according to the SDI is given in Table 2. The number of cases gradually increases from low-to-middle to middle-to-high SDI countries, with an approximately 2.5-fold higher risk in the latter countries. The mortality shows an analogous trend, with mortality in both middle (∼2.1-fold) and middle-to-high (∼3.6-fold) SDI countries significantly higher than in low-to-middle SDI nations.
Worldwide epidemiology of CO poisoning in countries with different SDI.
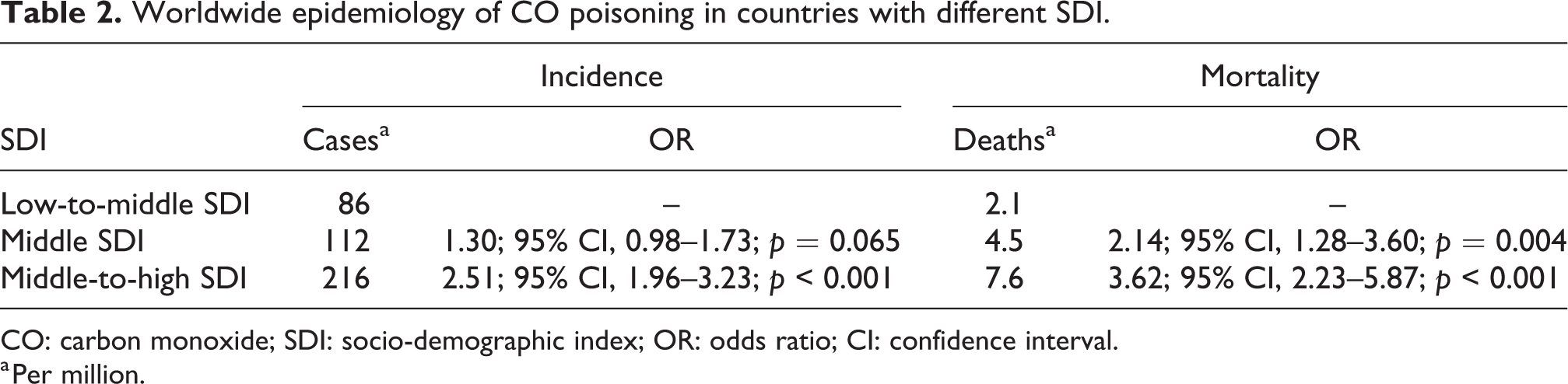
CO: carbon monoxide; SDI: socio-demographic index; OR: odds ratio; CI: confidence interval.
a Per million.
Discussion
Prehospital and hospital diagnosis and emergency care of CO poisoning are pivotal for preventing the dramatic consequences of this poisoning, which can be as severe as causing massive deaths of many poisoned patients. Epidemiologic data are essential prerequisites for developing organized efforts that can be really effective to mitigate the cumulative impact of CO poisoning. 1,2
Our analysis of the worldwide burden of CO poisoning prompts us to make some important health-care remarks. First, as clearly shown in Figure 1, the worldwide incidence of CO poisoning has remained virtually stable during the last 25 years, while mortality and percentage of patients who died have, instead, both declined by 36% and 40%, respectively. Therefore, although CO poisoning shall still be considered as an insidious cause of morbidity, its life-threatening burden seems globally declining. This is likely due to continued public education, enhanced efficacy of residential CO alarms, and more efficient therapeutic management of patients with CO poisoning. 9 This epidemiologic evidence confirms the trends observed years ago in some countries around the world, with decreasing mortality for CO poisoning reported in the United States, 9 England, 10 and China. 11
As predictable according to its most frequent causes which affect both sexes almost equally (i.e. heating system failures and fires), the incidence of CO poisoning is almost identical between sexes, though mortality was found to be double in the male sex. This is not really surprising according to CO biology. In a recent study, published by Zavorsky et al., 12 nine men and eight women were exposed to CO for increasing their COHb up to approximately 10%. Minute ventilation, hemoglobin concentration, and COHb, which were then measured at 5 min intervals, revealed that women had a shorter CO elimination halftime compared to men, even after adjusting for ventilation rate. This implies that CO toxicity is predictably lower in women and, accordingly, the risk of death is higher in the male sex. Indeed, women are also less likely to go to a health-care facility and hence be diagnosed with CO poisoning in poorer countries. 4
As regards the age distribution, we found two major peaks of poisoning cases, between 0–14 years (∼31% of all cases) and 20–39 years (∼34 of all cases). The mortality trend does not apparently follow a specific path, though the percentage of patients who died constantly increases in parallel with aging, with the highest mortality for CO poisoning observed after the age of 80 years (Figure 2). This worldwide evidence is in keeping with data recently published by Sircar et al. on CO poisoning in the United States 13 whereby the highest crude rate of deaths was also observed in people aged ≥85 years. This seems reasonable, wherein CO toxicity is predictably higher in older adults, due to slower elimination and enhanced presence of comorbidities (especially coronary heart disease), which will both contribute to increase the fatality rate. 14,15 Unlike the previous report of Sircar et al., 13 however, we found a larger number of deaths in children aged <5 years compared to those aged ≥5 years (i.e. 5% vs. 1%), probably reflecting the different risk of poisoning at this age around the world. Similar evidence has been earlier published by Gozubuyuk et al. 3 who concluded that CO poisoning in infants may be associated with a more severe course than later in childhood. This would actually mirror our findings that the percentage of patients who died is nearly double in children aged <5 years than in those aged 5–9 years.
As concerns, the relationship between CO poisoning and sociodemographic development, incidence and especially mortality were found to gradually increase in parallel with the SDI, a demographic measure reflecting average income, educational attainment, and total fertility rate. Notably, the relationship between climate and SDI has been known for a long time. 16 Basically, warmer countries tend to have lower SDI, and this would then be mirrored by a lower risk of CO poisoning from heating system failures, which is indeed the leading cause of CO-related death in many other colder nations. 17 Moreover, the apparent difference in incidence by SDI can also be explained by the fact that cooking can be done on open fires, charcoal, or gas/paraffin sources, all of which are potential sources of CO.
Epidemiological research is regarded as an irreplaceable instrument for developing and implementing health-care interventions that can be applied to large populations, thus contributing to promote clinical, societal, and economic benefits beyond the individual. 18 CO poisoning makes no exception, since accurate epidemiologic information is necessary for establishing appropriate and timely public health surveillance measures, as well as for improving health-care preparedness to face emerging challenges. Taken together, our data suggest that the worldwide burden of CO poisoning remains stable, but the number of fatal outcomes and the percentage of patients who died have both consistently declined during the last 25 years. Men and elderly individuals are more vulnerable, thus requiring more accurate diagnosis and aggressive care. Finally, reinforced efforts shall be made for developing public health infrastructures specifically aimed at preventing CO poisoning in middle-to-high SDI regions. We finally acknowledge that our data would only apply to the world as a whole, and this is perhaps a limitation, along with the fact that incidence and mortality of CO poisoning varies by SDI, so that the pattern in specific countries or smaller regions might be inherently different.
This article has a number of weaknesses. In the original data source used for the analysis, the number of countries from which the information is obtained (i.e. the GHDx repository), data increases year by year. Detailed reading of previous publications using the database provides some insight into that. 8 We are basically unable from our access to the database to establish how this is changed for the economic less well-developed groups of countries as opposed to the richer ones. It is somewhat surprising that our analysis revealed that poor countries may suffer less morbidity and mortality from CO than more wealthy ones (Table 2), since CO-based fuels are almost universally used for cooking in such areas. The major weakness we face is that the tools for accurate diagnosis of both fatal and nonfatal CO poisoning are much less likely to be available in remote areas in poorer countries. To confirm the results of the analysis on income status and CO poisoning proper field studies are required. In contrast, we feel the findings on age and mortality are more likely to be robust.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.