
Abstract
Carbon monoxide (CO) is an important cause of deaths via poisoning. CO poisoning causes inhibition of O2 transport and development of tissue hypoxia, which then causes cell apoptosis. A significant indicator of cell apoptosis, soluble tumor necrosis factor-like weak inducer of apoptosis (sTWEAK) protein, is important for the stimulation of apoptosis. The primary purpose of this study is to determine whether apoptosis occurs during acute CO poisoning and to show that sTWEAK protein is an indicator of apoptosis that can be analyzed as a marker in the peripheral blood sample. The secondary aim is to determine the diagnostic and prognostic values of sTWEAK protein. The study was performed prospectively on 43 patients with CO poisoning and 30 healthy volunteer control individuals. The anamneses were taken from all patients, who also underwent physical examination. Complete blood count, biochemical markers, cardiac enzymes, and arterial blood gas measurements were analyzed. All the patients’ sTWEAK protein levels were also analyzed. The sTWEAK protein level of patients with CO poisoning was 2278 pg/mL (1197–7234), while the level of the control group was 1609 pg/mL (310–3721). The patients’ sTWEAK levels were significantly higher than the controls (area under the curve: 0.77 (0.66–0.89); p < 0.001), and the cutoff value was determined as 1895.50 pg/mL. The cutoff level had a sensitivity of 74.4%, a specificity of 76.7%, a positive predictive value of 82.0%, and a negative predictive value of 67.6%. sTWEAK is a significant indicator of apoptosis in CO poisoning that can be analyzed in the peripheral blood. However, further clinical trials are needed in terms of prognostic criteria.
Introduction
Carbon monoxide (CO) is an important cause of deaths via poisoning. 1 –4 Transport of oxygen is inhibited, and delivery of oxygen to tissues is restricted in CO poisoning, which leads to tissue hypoxia. The most affected systems are central nervous system and cardiovascular system. 3 Mortality is substantially associated with problems in these two systems. Death might be caused by cardiac toxicity, neurotoxicity, systemic acidosis, or respiratory arrest. 1
When CO is inhaled, it binds with 220 times more affinity to hemoglobin and forms carboxyhemoglobin (COHb). 5 CO poisoning is known to cause both tissue hypoxia and direct cellular changes involving immunological or inflammatory damage through several mechanisms. 4
While patients with less than 10% COHb concentration are usually asymptomatic, the concentration of over 16% COHb is enough for clinical symptoms to appear. When the COHb level is over 30%, some clinical signs are observed, which may include severe headaches, loss of strength, nausea, vomiting, blurring of vision, dizziness, collapse, and dark red coloring of lips and skin. Once the COHb level reaches around 60%, coma, convulsion, and cardiopulmonary arrest may occur. 5,6 However, it is accepted that there is not a strong correlation between the COHb levels and severity of poisoning, and especially between the symptoms and prognosis of the patient in the acute phases and measured COHb levels at admission to the hospital. 5 –7
Soluble tumor necrosis factor (TNF)-like weak inducer of apoptosis (sTWEAK), first defined in 1997, is a growth regulator protein from the TNF-α family with a weak apoptotic activity. 8,9 sTWEAK protein is mainly responsible for stimulation of apoptosis and the regulation of many biological functions such as release of inflammatory cytokines, cell growth, and induction of angiogenesis. 10,11 sTWEAK is found in the intestines, pancreas, lungs, ovaries, brain tissues, skeletal muscle, blood vessels, and in lesser amounts in the kidneys and liver. 12 The receptor that binds sTWEAK via physiological affinity, fibroblast growth factor inducible 14 (Fn14), is the smallest member of the TNF receptor family. 9 In healthy tissues including blood vessels and heart, Fn14 is generally in low or undetectable levels. After tissue damage, its level increases rapidly. Studies showed that there were dramatic increases in sTWEAK levels during chronic liver damage, encephalitis, renal insufficiency, and myocardial infarction (MI). 12 Fn14 is induced by the interleukins, cytokines, and several growth factors found in monocytes, macrophages, vascular smooth muscle cells, and damaged vascular walls of endothelial cells. 13 –16
To the best of our knowledge, no studies have so far investigated apoptosis in the peripheral blood samples of CO-poisoned patients. The primary purpose of this study is to determine whether apoptosis occurs in patients during acute CO poisoning and to show that sTWEAK protein is an indicator of apoptosis that can be analyzed as a marker in the peripheral blood sample. Secondarily, the study aims to determine the diagnostic and prognostic values of the sTWEAK protein.
Subjects and methods
This prospective study was performed at the Departments of Emergency Medicine and Medical Biochemistry, Kırıkkale University, Turkey, between November 2015 and April 2017. It was approved by the Kırıkkale University Faculty of Medicine ethical committee (Decision Number: 2015-20/06). Patients who were over 18 and who applied to the emergency service with CO poisoning were included in the study. Patients who had conditions that would cause higher-than-normal levels of sTWEAK such as chronic heart failure, MI, chronic liver failure, chronic renal failure, and diabetes mellitus were excluded.
Demographical data (age and gender) of the patients were recorded, and their routine evaluations included anamnesis and routine physical examination. Complete blood count, biochemistry, cardiac enzymes, and arterial blood gas and COHb levels were analyzed in addition to sTWEAK levels. Treatments of all the 43 patients were started promptly. Data about the patients were recorded in standardized study forms. The control group was composed of 30 individuals of similar ages with no history of illness, smoking, or CO contact. Only the sTWEAK levels were measured for the control group, because the COHb levels, which can be determined via an invasive arterial blood sampling, were strongly expected to be minimal.
sTWEAK measurement protocol
Blood samples of 8–10 mL volumes were taken from the patients and the control group, their serums were separated in sterile conditions, and within 30 min of sampling they were frozen and kept at −80°C. The samples were returned to room temperature 3 h before analysis. The sTWEAK concentrations were measured in serum samples using an ELISA kit (Human TNSF12/TWEAK PicoKine™ ELISA Kit (Catalog Number: EK0920) Boster Biological Technology, Pleasanton, California, USA) in accordance with the manufacturer instructions. The kit could measure concentrations between 62.5 pg/mL and 10,000.0 pg/mL with a sensitivity of <10 pg/mL. Intra-assay and inter-assay CV values were 5.4% and 6.4%, respectively.
Methods
Standards and samples that were placed in the wells lined with antihuman sTWEAK antibody were incubated at 37°C for 90 min. Then biotinylated antihuman TNFSF12 antibody was added, and they were once again incubated at 37°C for 60 min. Once the incubation period was over, the wells were washed with 0.01 M Tris-buffered saline (TBS) three times. Afterward, avidin–biotin-peroxidase complex was added to the wells and they were set to incubate at 37°C for 30 min. After this incubation, the wells were washed again five times with 0.01 M TBS. Following the washing, 3,3′,5,5′-Tetramethylbenzidine (TMB) color-developing reagent was added, and the plate was incubated in the darkness at 37°C for 25–30 min. Then, TMB stop solution was added to the wells, and their absorbance at 450-nm wavelength was read using an automatic ELISA reader. The sTWEAK concentrations of the samples were calculated via the curve prepared using the results of the standards.
Statistical analyses
All data were analyzed with SPSS (Statistical Package for Social Sciences) for Windows 22.0 (SPSS Inc, Chicago, Illinois, USA). Descriptive statistics were presented as mean ± standard deviation, median (min–max), frequency distribution, and percentage. Categorical variables were assessed using Pearson’s χ2 test and Fisher’s exact test. Normally distributed data were analyzed using visual (histograms and probability graphs) and analytical (Kolmogorov–Smirnov test) methods. Descriptive statistics were presented as mean and standard deviation for normally distributed variables and as median and quartiles for non-normally distributed ones. Student’s t-test was used to assess the differences of the normally distributed variables in both groups, while the Mann–Whitney U test was employed for the non-normally distributed ones. p-Values of <0.05 were considered statistically significant. To determine the correlation between the variables, at least one of which distributed non-normally, the coefficient of correlation was calculated using the Spearman test. For statistical significance, type-I error level was 5%. The diagnostic importance of sTWEAK protein in CO poisoning was assessed with the receiver operating characteristic (ROC) curve analysis. The specificities, sensitivities, and positive and negative predictive values were calculated for significant boundary values. Statistical significance was set at p < 0.05.
Results
Several demographical and clinical properties of the patients with CO poisoning are presented in Table 1. Of all the patients, 38 (88.4%) had no substance history, while 5 (11.6%) were smokers. The Glasgow Coma Scale (GCS) score was 15 for 37 patients (86%), 14 for 4 patients (9.3%), 11 for 1 patient (2.3%), and 7 for 1 patient (2.3%).
Demographical and clinical information about the CO-poisoned patients.

SD: standard deviation; n: number of patients; CO: carbon monoxide.
Blood laboratory values and the sTWEAK levels of the patients with CO poisoning are presented in Table 2. According to these results, leukocyte (white blood cells (WBC)), hemoglobin, creatinine, alanine aminotransferase (ALT), aspartate aminotransferase (AST), lactate, and partial pressure of CO2 (pCO2) variables were distributed normally, while urea, high-sensitivity cardiac troponin T (hs-TnT), COHb, and sTWEAK variables were not distributed normally. Distribution of age and sTWEAK levels of the patients and the controls is given in Table 3. The graph depicting the sTWEAK levels of the patients and controls is given in Figure 1.
Blood laboratory results and sTWEAK concentrations of CO-poisoned patients.

sTWEAK: soluble tumor necrosis factor-like weak inducer of apoptosis; CO: carbon monoxide; COHb: carboxyhemoglobin; WBC: white blood cells; SD: standard deviation; ALT: alanine aminotransferase; AST: aspartate aminotransferase; hs-TnT: high-sensitivity cardiac troponin T.
Age and sTWEAK concentration distribution of CO-poisoned patients and healthy controls.

sTWEAK: soluble tumor necrosis factor-like weak inducer of apoptosis; CO: carbon monoxide; n: number of patients.
aMann–Whitney U test.

Distribution of sTWEAK levels in CO-poisoned patients and healthy controls. sTWEAK: soluble tumor necrosis factor-like weak inducer of apoptosis; CO: carbon monoxide.
Levels of sTWEAK protein were found to be statistically significantly higher (p < 0.001) in patients with CO poisoning compared to the control group (Table 3).
As part of the study, the predictive ability of sTWEAK protein in the diagnosis of CO poisoning was assessed using ROC curve analysis. Results showed that sTWEAK was an important indicator of CO poisoning (area under the curve: 0.77 (0.66–0.89); p < 0.001), with a cutoff value of 1895.50 pg/mL (Figure 2). For the cutoff value, calculations showed that the sensitivity was 74.4%, specificity was 76.7%, positive predictive value was 82%, and negative predictive value was 67.6% (Table 4).
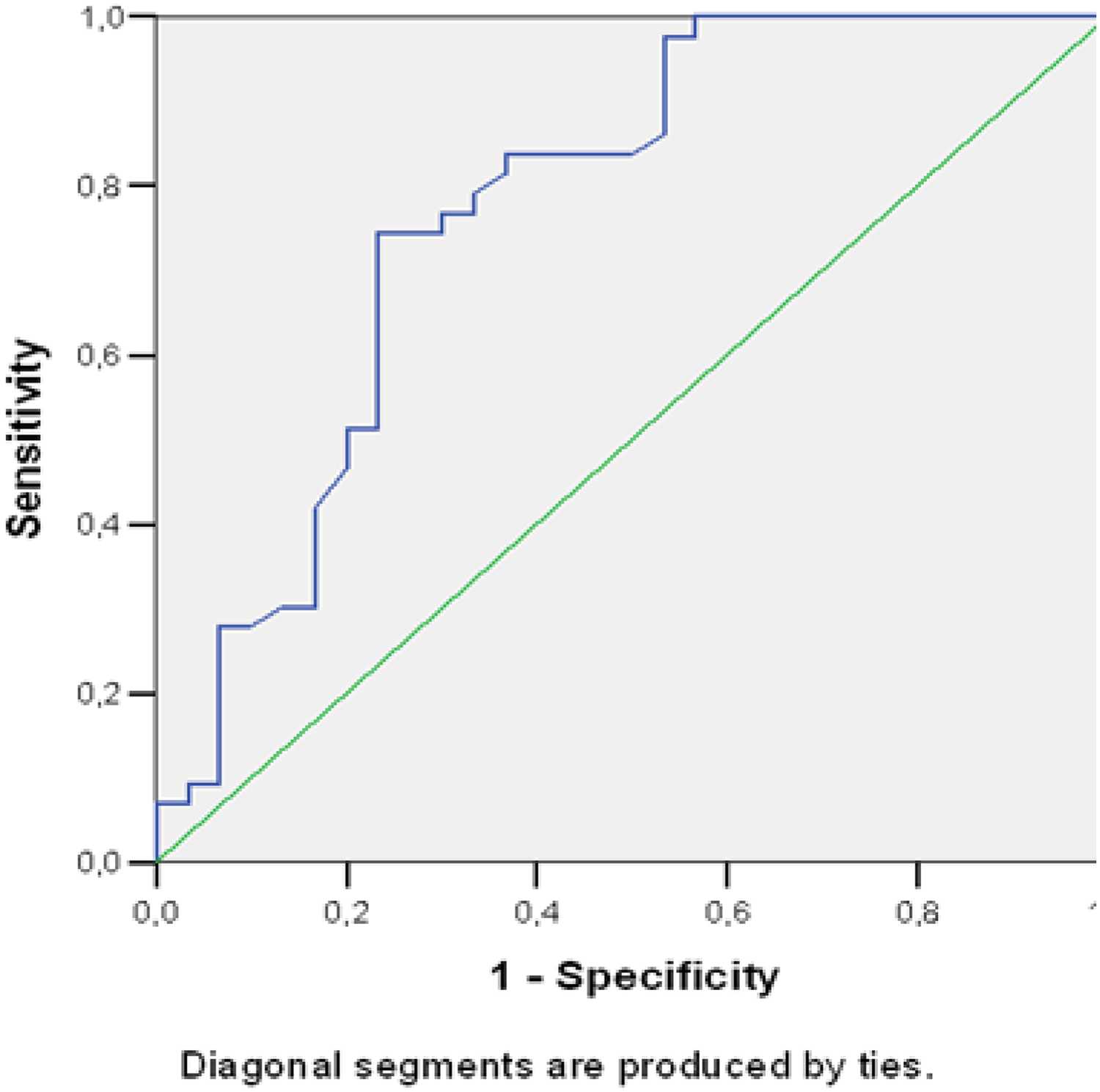
Assessment of the diagnostic value of sTWEAK protein in CO-poisoned patients using the ROC curve. sTWEAK: soluble tumor necrosis factor-like weak inducer of apoptosis; CO: carbon monoxide; ROC: receiver operating characteristic.
Sensitivity, specificity, and positive and negative predictive values of the determined sTWEAK cutoff level in CO poisoning diagnosis.

sTWEAK: soluble tumor necrosis factor-like weak inducer of apoptosis; PPD: positive predictive value; NPD: negative predictive value; %: percentage.
The relationships between sTWEAK protein levels, age, and laboratory results were assessed for all the patients with CO poisoning. The results are as given in Table 5. The statistical analyses showed no relationships between the sTWEAK levels and age of the patients (p = 0.6). There was no correlation between sTWEAK levels and GCS scores (p = 0.224). However, GCS score was statistically related to lactate levels (p = 0.002), WBC count (p = 0.023), and COHb levels (p = 0.004). In addition, ALT and AST were found to be statistically related (p = 0.0001). No correlations were found between the patients’ sTWEAK levels and COHb (p = 0.751), urea (p = 0.225), creatinine (p = 0.688), AST (p = 0.612), ALT (p = 0.422), troponin T (p = 0.197), and lactate levels (p = 0.114). A statistical relationship was found between the sTWEAK protein and WBC (p = 0.033). Laboratory values of the patients indicated that lactate levels were statistically related to COHb (p = 0.038) and WBC (p = 0.010); hemoglobin was related to creatinine (p = 0.029) and AST (p = 0.005); urea was related to creatinine (p = 0.003), troponin (p = 0.038), WBC (p = 0.041), and ALT (p = 0.045).
Correlations between the laboratory results.a

sTWEAK: soluble tumor necrosis factor-like weak inducer of apoptosis; CO: carbon monoxide; COHb: carboxyhemoglobin; WBC: white blood cells; SD: standard deviation; ALT: Alanine aminotransferase; AST: Aspartate aminotransferase; hs-TnT: high-sensitivity cardiac troponin T; GCS: Glasgow Coma Scale; Cor. Coeff.: correlation coefficient.
aListwise N = 43.
bCorrelation is significant at the 0.05 level (two-tailed).
cCorrelation is significant at the 0.01 level (two-tailed).
While 38 patients had no prior substance history, 5 patients were smokers. As seen in Table 6, when the COHb and sTWEAK levels of these two groups of patients were investigated, nonsmokers’ average COHb level was at 22.80%, and smokers’ average COHb level was at 23.64%; the average value of sTWEAK level of nonsmokers was 2351 pg/mL, and the average value of smokers was 3013 pg/mL. When the smokers and nonsmokers were compared, although the smokers had higher COHb and sTWEAK levels on the average than nonsmokers, no statistically significant difference was detected (p = 0.352 and p = 0.716, respectively).
Comparison of the sTWEAK and COHb levels of smokers and non-smokers.

sTWEAK: soluble tumor necrosis factor-like weak inducer of apoptosis; n: number of patients; COHb: carboxyhemoglobin; SD: standard deviation.
Of the 43 patients, 27 (62.8%) were discharged after the treatment in the emergency room (ER) unit within the same day, 1 (2.3%) was admitted to service, and 15 (34.9%) were placed in the intensive care unit. All the patients were successfully treated. Seven (16.3%) of the in-patients were discharged after 1 day, three (7.0%) were discharged after 2 days, four (9.3%) were discharged after 3 days, one (2.3%) was discharged after 10 days, and one (2.3%) was discharged after 90 days. The mean hospitalization duration was 2.9070 ±13.70751 (min: 0 and max: 90 days). No statistically significant relationship was found between the hospitalization duration and sTWEAK levels (p = 0.475), nor between the sTWEAK levels of the patients who were discharged on the same day and the patients who were hospitalized (p = 0.618). Similarly, the relationship between COHb levels and hospitalization duration was not statistically significant (p = 0.058).
When the sTWEAK levels of the patients with COHb levels of over and under 30% were compared, no statistically significant difference was found (p = 0.122; Table 7).
Relationship between COHb and sTWEAK levels in CO-poisoned patients.

sTWEAK: soluble tumor necrosis factor-like weak inducer of apoptosis; COHb: carboxyhemoglobin.
Discussion
In this study, the sTWEAK protein levels of patients with CO poisoning were statistically significantly higher than the control group. It was also found that apoptosis occurred in patients with CO poisoning, and sTWEAK could be used as a valuable indicator of CO poisoning diagnosis.
sTWEAK is one of the proinflammatory cytokines. 17 In recent years, its popularity has grown as studies have focused on the use of this protein in the stimulation of apoptosis and regulation of other biological functions such as release of inflammatory cytokines, cell growth, and induction of angiogenesis. 17
Chorianopoulos et al. reported that sTWEAK levels in patients with ST elevation acute MI were noticeably higher than both the control group and other patients with stable coronary artery diseases. 18 Hengdao et al. investigated the role of sTWEAK in atherosclerosis and showed that sTWEAK participated in the formation and progress of atherosclerosis; when it binds to the first receptor, Fn14 is rapidly released, resulting in negative biological consequences during atherosclerosis such as phenotypical changes in smooth muscle cells and inflammatory responses of monocytes and macrophages. 19 Muñoz-García et al. stated in their study that, in apolipoprotein E knockout mice that were fed with a hyperlipidemic diet, sTWEAK was shown to enhance the inflammatory response associated with a lipid-rich diet, as well as increasing the proinflammatory cytokines along with macrophage cell uptake, resulting in vascular lesions and renal damage caused by the hyperlipidemic situation. 20 In another study, Martín-Ventura et al. compared the sTWEAK levels of patients with abdominal aortic aneurism (AAA) with healthy control individuals and reported that there was a negative correlation between the aorta radius and low sTWEAK levels, which could be used to diagnose and prognose AAA. 21
According to the established literature, in cases of cardiovascular diseases, sTWEAK is known to be in higher levels compared to the control groups. The present study also indicates similar results as CO poisoning is cardiotoxic, and it causes apoptosis in the cardiovascular system.
Bertin et al. stated that the sTWEAK/Fn14 pathway can be used as a biological indicator in the diagnosis and tracking the progress of several human autoimmune/chronic inflammatory diseases such as lupus, rheumatoid arthritis, and multiple sclerosis. 22 However, they also expressed difficulties in sTWEAK quantification and standardization in data acquisition in routine practice. 22 In their study that investigated the relationships between ischemic stroke and sTWEAK, Inta et al. reported that the sTWEAK and Fn14 levels of patients who were admitted within 24 h of an ischemic stroke were significantly higher than the control group, and these levels were related to post-stoke survival. However, they were unrelated to the infarction size. 23 Studies showing the relationships between sTWEAK protein and recovery are not limited to these. sTWEAK protein was reported to be the indicators of mortality and prognosis for chronic renal failure by Yılmaz et al., nonischemic heart failure by Richter et al., and chronic stable heart insufficiency by Chorianopoulos et al. 24 –26 Therefore, in our study, we specifically aimed to measure the sTWEAK levels in acute CO poisoning cases by excluding patients with chronical diseases.
Several immunohistochemical studies showed cell-level apoptosis in the central nervous and cardiovascular systems caused by CO poisoning. 27,28 However, no studies in the literature on CO poisoning investigated or showed the detection of apoptosis using peripheral circulation. Xue et al. investigated the immunohistochemical effects of neural apoptosis and hyperbaric oxygen on different areas of the hippocampus of acutely CO-poisoned rats and found that apoptosis occurred, and it could be prevented by 7 days of hyperbaric oxygen treatment. 27 Rezaee et al. experimentally determined that in acutely CO-poisoned rats, immunohistochemically, apoptosis occurs in the myocardial tissues and application of erythropoietin noticeably suppresses the apoptosis in myocardial cells. 28 In our study, we found that the serum sTWEAK levels of patients were significantly higher than the control group, which also indicated that serum or plasma sTWEAK levels could be a marker for apoptosis in CO poisoning.
With the results, the sTWEAK cutoff value was determined as 1895.50 pg/mL in our study and higher sTWEAK levels were found to be significant in CO poisoning diagnosis. Previous studies reported a wide range of sTWEAK cutoff levels. 18,29 These differences could be caused by the heterogeneity in the study groups and/or methods. In addition, it could be argued that the differences result from the variability of sTWEAK levels in acute and chronic illnesses and stable and unstable patients.
The literature indicates a very limited number of studies on sTWEAK protein concentrations in blood circulation that are used to indicate disease prognosis. 21,30 We initially thought that the sTWEAK concentrations would be higher in CO-poisoned patients who had cardiac and central nervous system effects, and it could be an important indicator in prognosis. However, we could not detect a relationship between the sTWEAK levels and prognosis. We believe that this relationship could not be established because of the fewer number of patients, particularly with severe cases of poisoning.
Limitations
The first limitation we encountered in our study was the limited number of patients. The second limitation was that the COHb concentrations were lower than expected, caused by the oxygen treatment en route to the ER. The third limitation was the inability of prognostic assessment due to lack of posttreatment sTWEAK concentrations.
Conclusion
In our study, sTWEAK concentrations were significantly higher in CO-poisoned patients compared to healthy controls. This indicates that apoptosis occurs in the CO-poisoned patients, and sTWEAK protein is a useful indicator in CO poisoning diagnosis. The results of the ROC curve analysis, conducted to determine the diagnostic value of sTWEAK in CO poisoning, yielded a cutoff value of 1895.50 pg/mL.
When the sTWEAK protein concentrations of patients with COHb levels of over 30% and below 30% were compared, no statistically significant difference was detected. Apoptosis occurs during CO poisoning; however, the level of apoptosis does not increase with the severity of poisoning.
The present study is the first study demonstrating the importance of the sTWEAK concentrations in CO poisoning cases; however, we believe that further reference value studies need to be established for utilizing sTWEAK levels as an apoptosis indicator in routine clinical practice. Additional clinical studies involving more patients are also recommended to determine whether sTWEAK protein level is an important marker in prognosis. Finally, further research could show new correlations between other common biomarkers and sTWEAK and COHb levels.
Supplemental material
Supplemental Material, ndindar_stweak_Supplementary_Info - How much apoptosis does carbon monoxide poisoning cause? Primary clinical soluble TWEAK protein level study
Supplemental Material, ndindar_stweak_Supplementary_Info for How much apoptosis does carbon monoxide poisoning cause? Primary clinical soluble TWEAK protein level study by N Dindar Badem, E Cömertpay and F Coşkun in Human & Experimental Toxicology
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by Kırıkkale University Scientific Research Projects Unit, project number 2015/019.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.