
Abstract
Objective:
The aim of the study was to assess netrin-1 levels in carbon monoxide (CO) poisoning to determine its relationship with poisoning severity and neurotoxicity.
Methods:
This is a cross-sectional prospective study. The patients older than 18 years with CO poisoning were included. The patients were categorized into two groups on the basis of neurological involvement. Both the patient and the control groups were sampled for netrin-1 at 0th hour, and the patient group only was sampled for netrin-1 at 4th hour.
Results:
A total of 84 patients and 50 healthy controls were enrolled. The median 0th hour netrin-1 level of the patient group (765.1 pg/mL (619.8-983.1) was significantly higher than the control group (484 pg/mL (376-1031.6)) (p < 0.001). There was also a significant difference between the 0th hour and 4th hour netrin-1 (888.9 pg/mL (700.3–1175.5)) levels in the patient group (p < 0.001).There was no significant statistical difference between patients with and without neurological involvement (p = 0.62) and between those who underwent hyperbaric oxygen therapy (HBOT) and those who did not (p = 0.76) with respect to 4th hour netrin-1 levels.
Conclusion:
The significantly higher netrin-1 levels in patients with CO poisoning, suggests that netrin-1 is elevated as a stress marker. Although there is no significant difference in netrin-1 levels in patients with neurological impairment in CO poisonings, netrin-1 may show subclinically neurological effects. Hence, we believe that netrin-1 cannot be used as a marker of poisoning severity.
Introduction
Carbon monoxide (CO) is a colorless, odorless, nonirritant gas lighter than air, which is released by incomplete combustion of carbon compounds. 1 CO poisoning is still one of the important causes of mortality and morbidity worldwide. CO poisoning produces different signs and symptoms, depending on the involved tissue. The earliest signs are produced by involvement of brain and heart, which are highly oxygen dependent. 2
CO poisoning is diagnosed on the basis of blood carboxyhemoglobin (COHb) level. There is a weak correlation between the latter and organ injury. In general, poisonings exceeding a COHb level of 60% result in death, while lower percentages produce mild-to-severe clinical signs and symptoms. Poisoning severity cannot be necessarily determined by COHb level. Non-COHb biochemical markers have been investigated to predict CO poisoning, which is particularly neurotoxic and cardiotoxic. 3 –6 Doğan et al. reported that COHb levels are positively correlated with lactate levels in CO intoxication. 7
Netrins are important precursor proteins for neural and vascular development. Unlike its role during neural development, netrin-1 is known as myelin-associated inhibitor on spinal cord, and it causes axonal growth retardation after spinal cord injury. When we look beyond neural development, netrin-1 guides the emigration of adult neural root cells in injured central nervous system regions. 8 Previous studies have indicated that netrin-1 plays an important role for peripheral nerve renewal. 9 Recent studies have suggested that netrin-1 is an important neuromarker. 10,11 Various studies have used many markers like S100B, glial fibrillary acidic protein (GFAP), and neuron-specific enolase (NSE) to assess neurological involvement in CO poisoning. 3 –6 However, we did not come across any study in the literature that specifically evaluated the use of netrin-1 level in CO poisoning.
The aim of this study was to investigate netrin-1 level in CO poisoning. By this way, we aimed to assess the feasibility of the use of netrin-1 for both diagnosing CO poisoning and detecting CO-induced brain injury. We additionally aimed to examine any potential correlation between the clinical severity of CO poisoning and netrin-1 level.
Methods
This is a prospective case control study approved by the local ethics committee (dated October 25, 2017; No: 1534). Our study was conducted between November 01, 2017 and April 30, 2018 in a tertiary care emergency department (ED) with approximately 250,000 patient admissions per year. Patients with COHb level >10% were enrolled to the study consecutively.
Patient selection
This study involved 104 adult patients older than 18 years who presented to ED with CO poisoning and who gave informed consent. A total of 50 consecutive healthy subjects of similar age and gender who were not smokers were enrolled as the control group. We excluded patients who did not gave informed consent, those who were unconscious and whose relatives refused giving informed consent, those with oncological disorders, those with hematological malignancy and/or disorder, those with chronic inflammatory disorder, and pregnant patients. Fourteen patients were excluded due to missing data and not meeting the study entry criteria, and six patients due to missing 4th hour blood samples, making a total of 20 patients excluded from the study. A total of 84 consecutive patients were enrolled in the study.
Neurological involvement was acccepted positive when there was syncope (loss of consciousness), history of convulsion, a Glascow Coma Score (GCS) below 15, and focal neurological deficit. Depending on the need of the patients, they were administered normobaric oxygen therapy (NBOT) or hyperbaric oxygen therapy (HBOT). Patients with syncope, loss of consciousness, convulsions, coma, blood COHb level >25%, focal neurological deficit, and acute myocardial ischemia were referred to HBOT. Others were administered 100% NBOT with reservoir mask at the ED.
Considering α = 0.05, power of 80% and 335 pg/mL 10 acceptable standard deviation (SD) in the reported sensitivity, we selected 45 control people which was later increased to 50 people to compensate for expected dropouts or missing data.
Analysis of blood samples
The blood sample was taken twice; within 5 min of patient admission and at the 4th hour of follow-up. Sunredbio® (Shangai/China) Human Netrin-1 ELISA kit was used. Blood samples were studied with manual enzyme-linked immunosorbent assay (ELISA) immunoassay method. The measurements were read in BioRad PR4100® (France) ELISA plate reader device. Delta netrin-1 values were calculated from the 0th hour and 4th hour netrin-1 levels.
Statistical analysis
The study data were analysed with IBM® SPSS 20.0 (Chicago, IL, USA) software package. Discrete and continuous variables were subject to a test for normality of distribution using Kolmogorov–Smirnov test. The descriptive statistics included mean ± SD or median (minimum–maximum) for discrete and continuous variables and number and percentage (%) for categorical variables.
The difference between the mean values of the patient and control group’s measurements was analyzed with the Mann–Whitney U test. Wilcoxon test was used to compare 0th hour and 4th hour netrin-1 levels within the patient group. The value of p < 0.05 was considered statistically significant.
Results
There was a total of 47 (56%) women in the patient group and 28 (56%) women in the control group. The median age was 36 (interquartile range (IQR) 28–48) in the patient group and 33 (IQR 26–36) in the control group. Sixty-three (75%) patients received NBOT and 21 (25%) patients HBOT. Table 1 summarizes the demographic data of the study population.
Demographics and general properties of the study subjects.

COHb: carboxyhemoglobin.
The median 0th hour netrin-1 level of the patient and control groups were 765.1 (IQR 619.8-983.1) pg/mL and 484 (IQR 376–1031.6) pg/mL, respectively (p < 0.001). We detected a significant increase in the netrin-1 levels from 0th hour to 4th hour in the patient group, that is from 765.1 (IQR 619.8–983.1) pg/mL to 888.9 (IQR 700.3–1175.5) pg/mL) (p < 0.001; Table 2).
Netrin-1 levels of the patient and control groups.
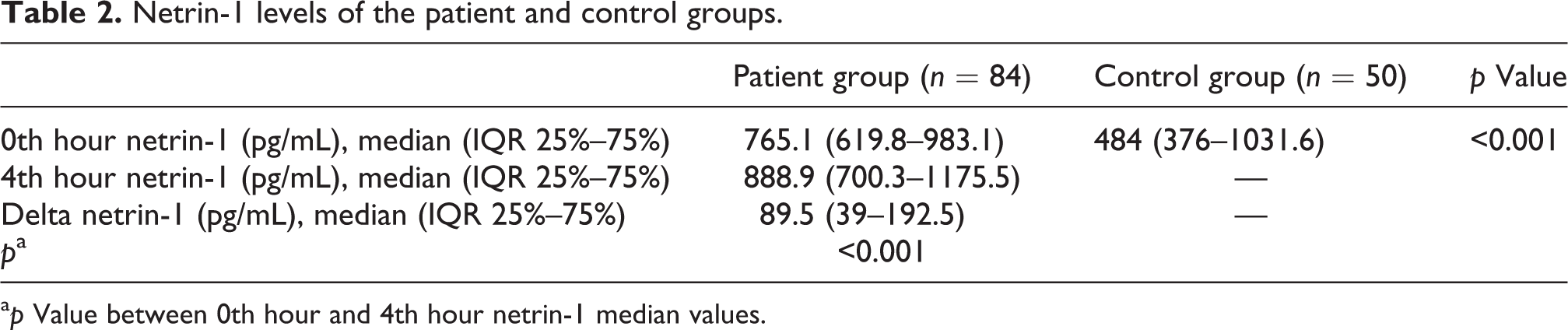
a p Value between 0th hour and 4th hour netrin-1 median values.
There was a total of 16 (19%) patients with neurological involvement. The comparison of patients with versus without neurological involvement revealed no significant difference between the two subgroups with respect to 0th and 4th hour netrin-1 levels (p = 0.19, p = 0.62, respectively; Table 3). There were no statistically significant differences between the groups receiving hyperbaric oxygen treatment and normobaric oxygen treatment at the 4th hour netrin-1 and delta netrin-1 levels (p = 0.76, p = 0.41, respectively; Table 4).
Comparison of netrin-1 levels at 0th hour and 4th hour in patients with and without neurological involvement.

Assessment of the effect of therapy on netrin-1 levels.

A receiver-operating characteristic (ROC) analysis was performed, and the area under the curve (AUC) was calculated to find out the cutoff level for netrin-1 level for distinction between the patient group and the control group. Accordingly, the AUC value was found to be 0.663 (0.559–0.767; Figure 1). To determine the cutoff values of netrin-1 between CO poisoning and control groups, an ROC curve was generated, and the AUC was calculated. Accordingly, when the cutoff value was taken 640.6 pg/mL, the sensitivity and specificity values were 73% and 66%, respectively. Table 5 lists the netrin-1 levels with relatively higher sensitivity and specificity values of AUC values.

ROC analysis for netrin-1 levels between the carbonmonoxide poisoning group and the control group. ROC: receiver-operating characteristic.
Sensitivity and specificity values of different netrin-1 levels for differentiation of the healthy control group and the CO poisoning group.

CO: carbon monoxide.
Discussion
We believed that this study, where we investigated netrin-1 level and the relationship between netrin-1 level and neurological involvement in CO poisoning, revealed two important major results. Firstly, we found a higher netrin-1 level in patients presenting with CO poisoning than healthy controls. However, the rise in netrin-1 level was not significant as a stress marker in CO poisoning. The second major finding is that we did not show any significant difference between the 0th hour and 4th hour netrin-1 levels and delta netrin-1 value between the patients with neurological involvement and without neurological involvement. Although we did not find a significant difference in netrin-1 levels in patients with neurological impairment in CO poisoning, netrin-1 may show subclinically neurological effects. Furthermore, netrin-1 was not a useful marker for determining poisoning severity in CO poisoning.
The most important diagnostic tool for CO poisoning is the patient history. In equivocal cases, the diagnosis is supported by measuring blood COHb level and determining clinical signs. However, COHb level may sometimes be misleading. COHb level is insufficient to determine the severity of CO intoxication similar to neurological impairment. Thus, there is a need for novel markers in this field. Many studies on markers detected in blood and body fluids have been conducted to determine the severity of and to identify patients with neurological involvement in CO poisoning. 3,11 –14 The most notable markers are neuromarkers such as S100B, NSE, and GFAP. However, studies with these markers have reported conflicting results. In a study by Akdemir, where the roles of S100B, NSE, and GFAP in the assessment of hypoxic cerebral injury among patients with acute CO poisoning, S100B, NSE and GFAP’s serum levels were significantly higher in the patient group than in the control group. 4 Akelma et al. could not find any correlation between S100B protein level and Glasgow Coma Score (GCS) in children with CO poisoning. They detected that S100B protein level did not increase but NSE level increased. 12 In another study where copeptin levels were assessed to determine CO poisoning severity, patients presenting with CO poisoning were grouped into those with versus without altered consicousness; blood copeptin levels were significantly higher in the group with altered consciousness. The group that developed GNS had a higher copeptin level. In conclusion, plasma copeptin level was found to be correlated to poisoning severity and neurological involvement. 13 İrem et al. revealed higher copeptin levels among patients who had CO poisoning, concluding that this hormone may be used to diagnose CO poisoning and especially neurological injury. 14
Netrin-1 level has been previously studied in certain disorders. 10,11,15,16 However, to the best of our knowledge, no study has yet been conducted on the use of netrin-1 in CO poisoning. Our study is the first one conducted in this manner. A similar study on the role of netrin-1 to show neurological involvement was conducted by Ivelik et al. 10 who investigated the effect of blood netrin-1 level on 6-month survival among patients presenting to ED with acute stroke. They found a lower netrin-1 level among patients who sustained an acute stroke but could not relate netrin-1 level to mortality. Recent studies, on the other hand, have shown that netrin-1 suppresses inflammatory cytokines and chemokines in addition to its activity at cellular level. Some studies have suggested that netrin-1 suppresses infiltration and inflammation in certain conditions such as sepsis, acute renal failure, and acute lung injury. 15,16 We detected a higher netrin-1 level in our patients compared with the controls. This suggests the presence of netrin-1 in antioxidant and anti-inflammatory processes in CO poisoning involving oxidative stress and endogenous free oxygen radicals. Furthermore, we found higher netrin-1 level at 4th hour compared to netrin-1 level at 0th hour. We believe that this reflects the possibility that, in CO poisoning, despite a decrease in blood COHb level, toxicity and inflammatory status persist at cellular level. Although we could not detect any significant statistically difference between netrin-1 levels of patients with versus without neurological involvement, netrin-1 may show subclinically neurological effects. We consider that this stemmed from the fact that our poisoning group mostly consisted of mild poisoning cases. Also, netrin-1 is insufficient to determine treatment.
An ROC analysis carried out to find a cutoff level for netrin-1 levels between the group with CO poisoning and the control group revealed an AUC value of 0.663. We found that 640.6 pg/mL was the best cutoff point for netrin-1. According to these findings, when a cutoff point of 640.6 pg/mL was taken, a sensitivity of 73% and a specificity of 66% were found. These results suggest that netrin-1 would not be useful for use in the differential diagnosis of poisoning.
Limitations
Our study is a single-center study and consisted of relatively small sample size. We believe that as a result of this limitation, netrin-1 levels and its range of control subjects were found very large. This limitation may be due to the potential unintentional selection bias for control subjects. Our study group mostly consisted of mild poisoning cases. Neurological imaging was performed in only patients with neurological effects. The criteria for neurological effect were based on the clinical status of the patients. In our study, the patients for whom cranial computed tomography (CT) was performed (n = 16) had no pathological signs on their imaging. Cranial magnetic resonance imaging (MRI) was not performed in the ED or during admission in the hospital, because there was no ongoing neurological finding. In our study, the netrin-1 levels of the patients were examined at the time of admission to the ED and at the 4th hour after the admission. The period between the exposure to CO and the time of admission to the ED was not taken into consideration. This is one of the limitations of our study. We were unable to perform long-term follow-up for neurological sequela in patients with neurological involvement, and thus we could not assess the relationship between netrin-1 and delayed neurological sequela.
Conclusion
We found a significantly higher netrin-1 level in patients with CO poisoning. This suggests that netrin-1 is elevated as a stress marker in CO poisoning. However, we were unable to find any significant difference in the patients with neurological involvement with respect to netrin-1 level, netrin-1 may present subclinically neurological effects. Therefore, we believe that netrin-1 cannot be used as a marker of poisoning severity in CO poisoning. There is a need for new studies on netrin-1 and CO poisoning patients who have serious neurological effects.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.