
Abstract
The rate of mortality from dapsone poisoning is high because of the long absorption half-life of dapsone. This study aimed to evaluate the usefulness of the sequential organ failure assessment (SOFA) and acute physiology and chronic health evaluation II (APACHE II) scoring systems for the early prediction of mortality in patients with dapsone poisoning. This is a retrospective and observational study of consecutive patients diagnosed with dapsone poisoning. The SOFA and APACHE II scores were obtained within the first 24 h of admission. Patients were divided into survivor and non-survivor groups. In total, 106 patients were included. The SOFA scores of the survivor and non-survivor groups were 1 (0–8) and 4 (1–10), respectively (p < 0.001). The APACHE II scores of the survivor and non-survivor groups were 9 (1–25) and 14 (3–23), respectively (p < 0.001). Based on these scores and in-hospital mortality cases, the standardized mortality ratios for the APACHE II and SOFA were 1.00 (95% confidence interval (CI): 0.64–1.48) and 1.00 (95% CI: 0.64–1.49), respectively. In the model adjusted for clinically important variables and variables with significant differences between the survivor and non-survivor groups, the area under the curve of the SOFA (0.907; 95% CI: 0.834–0.955) was significantly higher than that of the APACHE II (0.793; 95% CI: 0.703–0.867) (p = 0.008). The SOFA and APACHE II score systems had good discrimination and satisfactory calibration performance in patients with dapsone poisoning. However, the SOFA score was a more useful method in predicting mortality than the APACHE II score.
Introduction
Dapsone, a synthetic sulfone that inhibits folate synthesis, is one of the common agents that can cause methemoglobinemia. 1 –4 It was first used in humans in the 1940s to treat leprosy. 5 The adverse effects of dapsone are classified as follows: acute adverse effects (nausea, vomiting, abdominal pain, methemoglobinemia, seizure, and unconsciousness) and chronic adverse effects (neutropenia, thrombocytopenia, eosinophilic pneumonia, aplastic anemia, hemolysis, neuropathy, hepatitis, and agranulocytosis). 6,7 Of these side effects, dapsone-induced methemoglobinemia can cause hypoxia due to the decreased oxygen-carrying capacity and left-shifted oxygen hemoglobin dissociation curve. 4,8 Although the principal metabolite of dapsone is mono-N-acetyl dapsone, it is not associated with toxicity. 9 Another metabolic pathway is the N-hydroxylation of dapsone (DDS-NHOH), and it is mainly responsible for hematological toxicity. 10 Dapsone-induced methemoglobinemia affects various organs, including the brain, heart, lungs, kidneys, and liver. Despite the use of methylene blue as an antidote in dapsone poisoning, the associated mortality rate is higher than 20%. 11,12 Thus, early and quick prediction of a high probability of death can guide a physician to apply intensive treatment from the emergency department (ED).
The sequential organ failure assessment (SOFA) and acute physiology and chronic health evaluation II (APACHE II) scoring systems are tools widely used for predicting the clinical outcomes of patients admitted in the intensive care unit (ICU). These scoring systems have been evaluated and validated in numerous centers, and the use of scoring systems specifically developed to assess patients at the time of ICU admission has reduced numerous problems and facilitated treatment planning. 13 –18 Several studies have assessed the early prediction of case fatality in acute organophosphate or paraquat poisoning using these scoring systems. 18 –21
However, despite the high mortality rate, no information is available on the clinical usefulness of the SOFA and APACHE II score systems for the early prediction of mortality in individuals with dapsone poisoning.
Therefore, this study aimed to evaluate the usefulness of the SOFA and APACHE II scoring systems for the early prediction of mortality in patients with dapsone poisoning.
Methods
Study design and population
This is a retrospective and observational study of consecutive patients diagnosed with dapsone poisoning between October 1996 and June 2017. Due to the retrospective and observational nature of the study, the need for informed consent was waived. The institutional review board of the Wonju Severance Christian Hospital approved this study (approved number: CR317357). The ED was located in a single suburban, tertiary care hospital (Wonju, Republic of Korea), with more than 46,000 annual visits. Moreover, this hospital has board-certified emergency physicians who are available 24 h a day.
Dapsone poisoning was confirmed based on the statements of the patient or guardian and elevated methemoglobin (met-Hb) level, and drug verification was performed by an emergency physician who transcribed the drug into the patient’s records. Overdose was defined as the ingestion of more than the minimum of two 100-mg tablets. 11 In dapsone poisoning, when patients have a met-Hb concentration higher than 30% or signs and/or symptoms, such as hypoxia, cyanosis, altered mental status, seizures, ischemic chest pain, electrocardiogram changes, newly developed arrhythmia, and/or hypotension, even if the met-Hb concentration was lower than 30%, methylene blue is then administered. In our hospital, the protocols for methylene blue administration include the infusion of 1–2 mg/kg over 10 min intravenously. If symptoms or methemoglobinemia persists, methylene blue is again administered. 11
Some of the participants were excluded based on the following criteria: (1) age below 19 years, (2) co-ingestion with other drugs, (3) prehospital cardiac arrest, (4) transfer to another hospital after ED admission, and (5) insufficient data.
Study variables and data collection
The following parameters were assessed: age, sex, ingested dose (mg), intentionality, periods from ingestion to ED arrival (hours), gastric irrigation or charcoal administration (single or multiple dose), dose of methylene blue used within 24 h after visiting the ED (mg), mean arterial blood pressure (mmHg), pulse rate, Glasgow Coma Scale (GCS) score, and medical history (diabetes mellitus, hypertension, chronic lung disease, congestive heart failure, liver cirrhosis, and chronic renal disease) at the ED. White blood cell and platelet count; hematocrit, aspartate transaminase, alanine transaminase, bilirubin, met-Hb, glucose, blood urea nitrogen, creatinine, and serum lactate levels; and pH and bicarbonate (HCO3 −) level were assessed. All laboratory parameters were measured within the first hour after arrival at the ED. Pneumonia, shock, acute kidney injury, and use of continuous renal replacement therapy (CRRT) as well as mechanical ventilation (MV) or continuous positive airway pressure (CPAP) were evaluated and considered as complications during hospitalization. Shock was defined as systolic blood pressure less than 90 mmHg requiring the administration of a vasoactive drug. Acute kidney injury was defined as the increase in serum creatinine ≥0.3 mg/dL within 48 h or ≥50% within 7 days or urine output <0.5 mL/kg/h for >6 h. 22 The indications of MV or CPAP were hypoxia (PaO2 < 70 mmHg) or hypercapnia (PaCO2 > 60 mmHg).
The SOFA and APACHE II scores were obtained within the first 24 h after admission. 14,16 The expected hospital case mortality was calculated according to the SOFA and APACHE II scores, as in the previous studies. 14,16 The patients were divided into the survivor group and non-survivor group.
Data were collected via retrospective reviews of the electronic medical records of patients by an emergency physician who was blinded to the study objectives and hypothesis. The evaluator was blinded to the groupings of the patients and was trained prior to reduce possible bias during data collection. We used specific case report forms in this study. The chart evaluator and study coordinator met periodically to resolve any disputes and reviewed the coding rules. The study coordinator monitored the evaluator’s performance. The patient records and information were anonymized prior to the analysis.
Data analysis
General characteristics of the participants, laboratory findings, and clinical scoring system were presented as means ± standard deviations, median (mini-max) for continuous variables, and frequencies (percentages) for categorical variables in dapsone poisoning. Differences between the survivors and non-survivors were assessed using the independent t test or Mann–Whitney U test for continuous variables and χ2 test for categorical variables. The differences between the sensitivities, specificities, and accuracy rates of the SOFA and APACHE II scoring systems in predicting mortality were examined using the McNemar test. p Value was corrected using Bonferroni’s method. Calibration of the predicted model was examined with the Hosmer–Lemeshow goodness-of-fit test (with a p value greater than 0.05 indicating good calibration) and standardized mortality ratio (SMR; defined as the actual population mortality divided by individual patient predicted mortality). 23 Receiver operating characteristic (ROC) curves were generated, and the area under the curve (AUC) was calculated to assess the relationship between clinical scoring systems and mortality rates using the multiple logistic regression model adjusted for sex, age, GCS, and ingested dose. In addition, we compared the ROC curves of the SOFA and APACHE II scores. All statistical analyses were performed using SPSS version 23 (IBM Inc., Chicago, Illinois, USA) and MedCalc version 18.2 (MedCalc Inc., Mariakerke, Belgium), and the significance level was set at 0.05.
Results
During the study period, 12,357 patients came to the ED due to drug intoxication. Of 12,357 drug intoxicated patients, 123 consecutive patients (0.99%) were identified with dapsone poisoning, and 17 patients were excluded from the study based on the following exclusion criteria (Figure 1).

Flow diagram of patient selection. ED: emergency department.
Twenty-eight patients (26.4%) were men, with a median age of 69.5 (range: 18–95) years. The poisoning was intentional in 76.4%, and the median ingested dose was 600 mg. Patients arrived at the ED within a median of 12 h after ingestion. Gastric irrigation was performed in 42.5% of the participants, and 77.4% and 21.7% of the participants received single and multiple doses of synthetic charcoal, respectively. In total, 110 mg of methylene blue was used within 24 h after visiting the ED. The complications during hospitalization were as follows: pneumonia (39.6%), shock (26.4%), acute kidney injury (24.5%), and use of CRRT (3.8%) as well as MV or CPAP (40.6%).
A comparison of patient characteristics and laboratory results is shown in Table 1. The mortality rate was 22.6% (24 of 106 patients). Of 24 patients, 23 (91.7%) died in the hospital, and 1 (8.3%) was discharged with impending death (non-survivor group). Patients in each group significantly differed in terms of age, ingested dose, GCS, and creatinine level. All complications, including pneumonia, shock, acute kidney injury, and use of CRRT and MV or CPAP, were observed in the non-survivor group. There was no significant difference in terms of medical history in each group.
General characteristics of the participants, laboratory findings, and clinical scoring systems used in dapsone poisoning.a
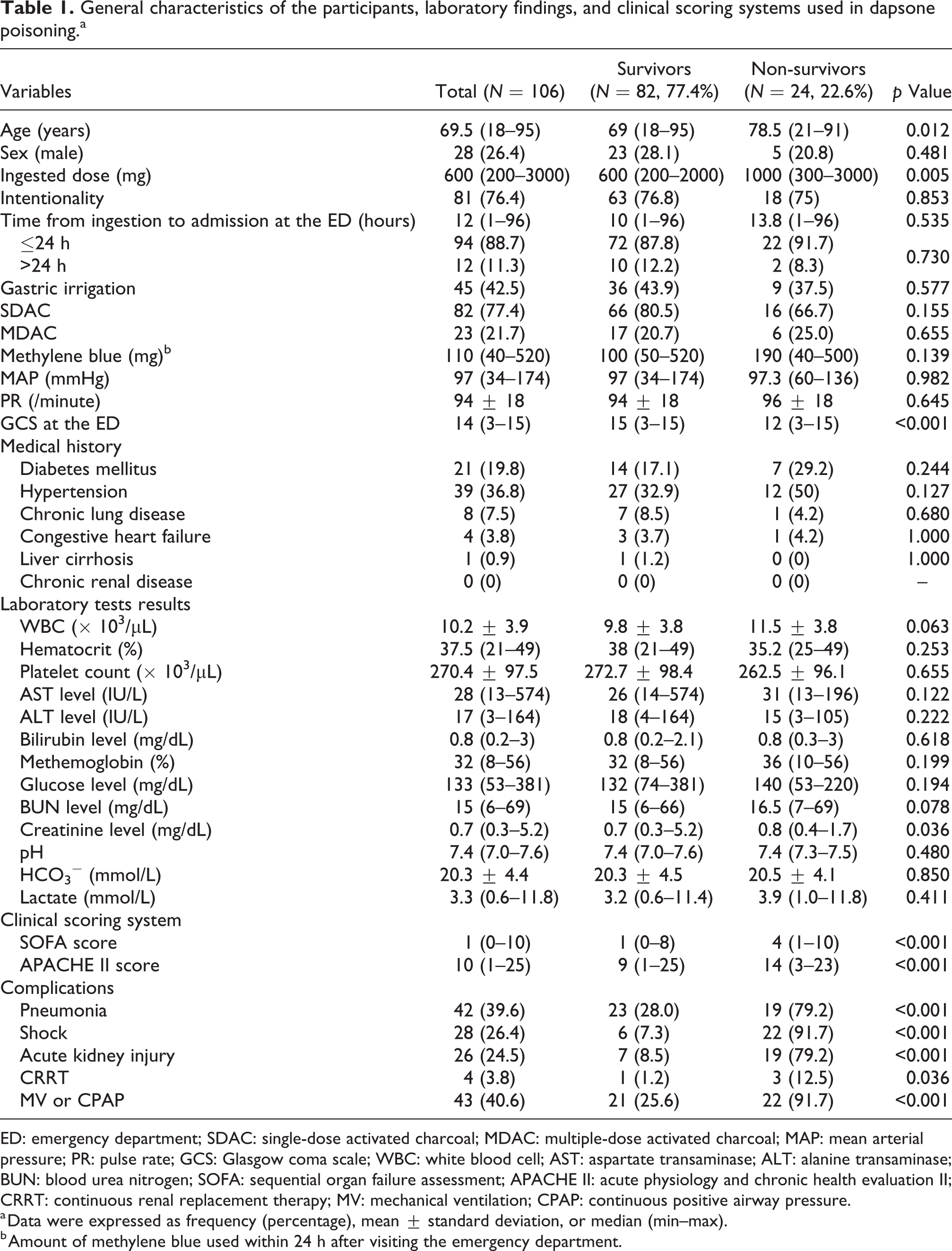
ED: emergency department; SDAC: single-dose activated charcoal; MDAC: multiple-dose activated charcoal; MAP: mean arterial pressure; PR: pulse rate; GCS: Glasgow coma scale; WBC: white blood cell; AST: aspartate transaminase; ALT: alanine transaminase; BUN: blood urea nitrogen; SOFA: sequential organ failure assessment; APACHE II: acute physiology and chronic health evaluation II; CRRT: continuous renal replacement therapy; MV: mechanical ventilation; CPAP: continuous positive airway pressure.
a Data were expressed as frequency (percentage), mean ± standard deviation, or median (min–max).
b Amount of methylene blue used within 24 h after visiting the emergency department.
The SOFA and APACHE II scores were significantly higher in the non-survivor group than in the survivor group. The SOFA scores of the survivor and non-survivor groups were 1 (0–8) and 4 (1–10), respectively (p < 0.001). Meanwhile, the APACHE II scores of the survivor and non-survivor groups were 9 (1–25) and 14 (3–23), respectively (p < 0.001).
Table 2 shows the predictive power of the mortality estimates for the overall study population according to the SOFA and APACHE II scoring systems. Sensitivity of the SOFA score was significantly higher than that of the APACHE II score (p = 0.013). Specificity of the SOFA score was not different from that of the APACHE II score (p = 1.000). The accuracy rate of SOFA score was higher than that of the APACHE II score. However, the difference was not statistically significant (p = 0.057).
Sensitivities, specificities, and accuracy rates of the APACHE II and SOFA scoring systems in predicting mortality.

APACHE II: acute physiology and chronic health evaluation II; SOFA: sequential organ failure assessment.
ap < 0.05 versus APACHE II (McNemar’s test with Bonferroni correction).
The SOFA and APACHE II scoring systems had good calibration based on the Hosmer–Lemeshow goodness-of-fit C-test results: χ2 = 6.208 and p = 0.184 as well as χ2 = 8.142 and p = 0.420, respectively. Based on these scores and in-hospital mortality cases, the SMRs of the SOFA and APACHE II scoring systems were 1.00 (95% confidence interval (CI): 0.64–1.49) and 1.00 (95% CI: 0.64–1.48), respectively (Table 3).
Predicted mortality, Hosmer–Lemeshow goodness-of-fit test, and SMRs for the APACHE II and SOFA prognostic models in dapsone poisoning.
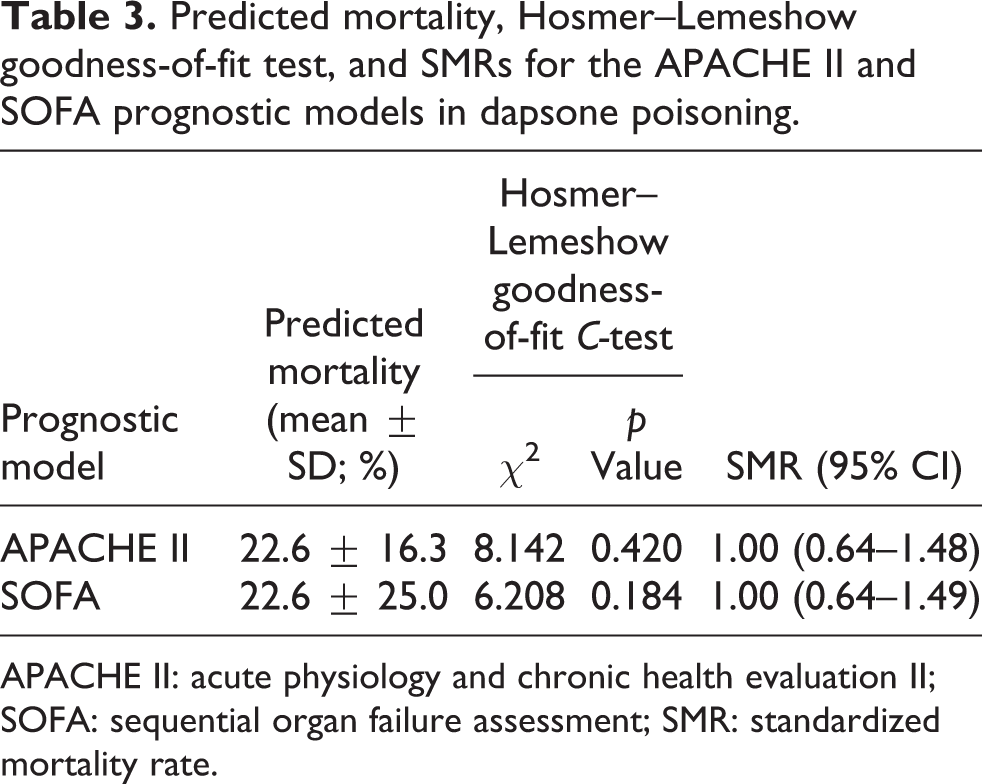
APACHE II: acute physiology and chronic health evaluation II; SOFA: sequential organ failure assessment; SMR: standardized mortality rate.
To evaluate the predictive value of the scoring systems, we evaluated the AUC of the ROC curve calculated using the model adjusted for clinically important variables and variables with significant differences in the survival and non-survival groups (sex, age, ingested dose, and GCS). The AUC of the SOFA score (0.907; 95% CI: 0.834–0.955) was significantly higher than that of the APACHE II score (0.793; 95% CI: 0.703–0.867; p = 0.008; Figure 2).

Receiver operating curves for predicting death according the APACHE II and SOFA scores. Adjusted areas under the curve and 95% confidence intervals for these indicators were 0.793 (0.703–0.867) for the APACHE II and 0.907 (0.834–0.955) for SOFA. The model adjusted sex, age, ingested dose, and GCS. APACHE II: acute physiology and chronic health evaluation II; SOFA: sequential organ failure assessment; GCS: Glasgow Coma Scale.
Discussion
The elimination half-life of dapsone ranges from 20 to 30 h in adults. 24 In addition, a longer elimination half-life was observed because dapsone is fat soluble and distributed mostly in tissues. Therefore, a relapse of methemoglobinemia may be observed. 25,26 In this study, mortality rate can reach as high as 22.6%, which is similar to a previous study. 11,12
In this study, we compared the usefulness of the SOFA and APACHE II scores in predicting the mortality of patients with dapsone poisoning. Despite the fact that we investigated the SOFA and APACHE II scores within the first 24 h after admission, regardless whether the patient was admitted in the ICU, the SOFA and APACHE II score systems were considered as a good and practical method in predicting the mortality of patients with dapsone poisoning (Table 3).
The SOFA score was developed during a consensus conference organized by the European Society of Intensive Care and Emergency Medicine. 14 SOFA score is usually used to monitor a person’s status during ICU admission to determine the extent of a person’s organ dysfunction or rate of failure. Organ dysfunction is associated with high rates of ICU morbidity and mortality. 27,28 The score system is based on six different scores, that is, one for each system (respiratory, cardiovascular, hepatic, coagulation, renal, and central nervous systems). 14,29 –32
APACHE II is a severity-of-disease classification system, and it is applied within 24 h after ICU admission. 16,33 APACHE II uses a point score based on the initial values of the 12 routine physiological measurements, patient age, and medical history to assess the disease severity of a patient. Higher scores correspond to more severe diseases and a higher risk of death because of the significant and consistent association between acute physiological dysfunction and the risk of death due to acute illness. 34 –36 However, the use of the APACHE II scoring system involves extremely complicated calculations.
In a study by Kim et al., the SOFA score is more useful than the APACHE II in predicting the outcomes of patients with organophosphate poisoning who are admitted in the ICU, and a significant association was observed between the SOFA scores and actual death rate. 20 Previous studies have shown that the APACHE II system is a useful index for evaluating mortality due to multiple organ system involvement in individuals with organophosphate or paraquat poisoning. 18,21
In this study, although these two scores can be used as an objective parameter to predict mortality of dapsone-poisoned patients, the SOFA scoring system had more significant superior discriminative power than the APACHE II scoring system (Figure 2). The use of the SOFA is more advantageous than the APACHE II score because its calculations are easier. Therefore, the SOFA score system may be a more practical method in predicting the mortality of patients with dapsone poisoning.
In the present study, the non-survivor and survivor groups differed in terms of age. Moreover, mortality may be observed more frequently in older patients due to the lack of physiological functional reserve to overcome toxicity. In this study, the ingested dose was significantly higher in the non-survivor group than in the survivor group. Therefore, when a patient has ingested large amounts of dapsone, clinicians should keep in mind that patients are more likely to die. Numerous complications, including low GCS, pneumonia, shock, acute kidney injury, and use of CRRT as well as MV or CPAP, were observed in the non-survivor group. Severe complications may have caused patient death.
This study had several limitations. First, the study was limited due to its retrospective design. Moreover, some data were missing, and not all relevant assessment parameters could be included. The ingested amount of toxin and the arrival time at the ED after ingestion may have been overestimated or underestimated. Second, the sample size of the patients was small because the study was limited to a single center. However, we evaluated all patients with dapsone poisoning to reduce possible bias. Third, variations in time interval from ingestion to admission at the ED (1–96 h) may be a limitation in the interpretation of results. However, the same results were obtained in analyses involving acute poisoning patients who arrived to ED within 24 h. The SOFA score was a more useful method to predict mortality than the APACHE II score (Online Supplemental Material). Fourth, due to the long period of case inclusion, it may be thought that there can be difference in treatment modalities. However, in this hospital, the only major change of treatment modality is using multiple-dose activated charcoal. We have applied multiple-dose activated charcoal for patients with dapsone poisoning since 2013, but there was no difference in the use of multiple-dose activated charcoal between the survivor group and non-survivor group. To overcome these limitations, a well-designed prospective study must be conducted.
Conclusion
The SOFA and APACHE II score systems had good discrimination and satisfactory calibration performance in individuals with dapsone poisoning. However, the SOFA score was a more useful method in predicting mortality than the APACHE II score.
Supplemental material
Supplement_figure - The usefulness of the SOFA and APACHE II scoring systems for the early prediction of mortality in patients with dapsone poisoning
Supplement_figure for The usefulness of the SOFA and APACHE II scoring systems for the early prediction of mortality in patients with dapsone poisoning by Y Lee, SJ Kim, YS Kim, H Kim, DK Lee, J Lee, TH Go, and YS Cha in Human & Experimental Toxicology
Supplemental material
Supplement_file - The usefulness of the SOFA and APACHE II scoring systems for the early prediction of mortality in patients with dapsone poisoning
Supplement_file for The usefulness of the SOFA and APACHE II scoring systems for the early prediction of mortality in patients with dapsone poisoning by Y Lee, SJ Kim, YS Kim, H Kim, DK Lee, J Lee, TH Go, and YS Cha in Human & Experimental Toxicology
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIP). (No. NRF-2017R1C1B5017695).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.