
Abstract
Background:
Glufosinate-containing herbicide is increasingly used in agriculture. Its poisoning is a worldwide concern. More and more patients are poisoned by glufosinate. The aim of this study was to determine the factors associated with mortality of patients with acute poisoning of glufosinate.
Methods:
This was a retrospective cohort study conducted from January 1998 to October 2015. Using a multivariate logistic analysis, data for the total population were retrospectively analyzed to determine the factors associated with mortality. Various variables were compared in survivors and non-survivors. Significant predictive variables, Acute Physiology and Chronic Health Evaluation (APACHE) II scoring system, the Simplified Acute Physiology Score (SAPS) II, and Sequential Organ Failure Assessment (SOFA) score were compared by analyzing receiver operating characteristic (ROC) curves.
Results:
A total of 253 patients (mean age: 58 years) were enrolled. Of the 253 patients, 219 (86.6%) survived and 34 (13.4%) died. Decreased Glasgow Coma Scale (GCS) and bicarbonate (HCO3 −), use of mechanical ventilator, and use of vasopressors (dopamine, dobutamine, norepinephrine) were associated with mortality. The areas under the curve in the ROC curve analysis for the predictive variables, SOFA score, APACHE II scoring system, and SAPS II were 0.952, 0.829, 0.927, and 0.944, respectively.
Conclusion:
Four predictive variables (GCS < 9, HCO3 − < 16.0 mmol/L, mechanical ventilator apply, and use of vasopressors) were associated with mortality in the total population of patients with acute poisoning of glufosinate. These predictive variables had good discriminative power for predicting mortality of patients with acute poisoning of glufosinate-containing herbicide compared to APACHE II, SOFA, and SAPS II.
Keywords
Introduction
Glufosinate-containing herbicide is now available in many countries, including the United States, Canada, Germany, the United Kingdom, and Korea. Its use has gradually increased. 1 Increased use of glufosinate herbicide has been accompanied by increased incidence of human poisoning cases in Asian countries, such as Korea, Japan, and Taiwan. 2,3
Glufosinate selectively inhibits the activity of glutamine synthetase, glutamate decarboxylase, and ammonia, resulting in decreased glutamic acid levels and intracellular accumulation of ammonia, which in turn causes tissue necrosis and death of plants. 4 The characteristic features of acute glufosinate herbicide poisoning in humans are primarily classified into two categories: neurotoxicity and hemodynamic toxicity. 5 Hemodynamic toxicity is likely to be attributed to formulated surfactant, 6 whereas neurotoxicity including seizure, altered mental state, amnesia, and central apnea requiring mechanical ventilation support is thought to be caused by glufosinate. 1
Severe effects from acute glufosinate poisoning include convulsions, respiratory arrest, coma, and disturbance of consciousness. They may appear after a latent period of 4–60 h. 7
There are several previous reports on severe adverse effects in patients with acute glufosinate poisoning. 2,8 –11 Although there have been studies on the severe effects and neurologic complications in patients with acute glufosinate poisoning, no subsequent studies were conducted to characterize the predictor of mortality of patients with acute glufosinate poisoning in emergency department (ED) and the intensive care unit (ICU).
Therefore, the purpose of this study is to identify possible predictive parameters for the mortality of patients with acute glufosinate poisoning. The primary outcome parameter is 90-day mortality.
Materials and methods
Study design and setting
This study is conducted at a regional emergency center affiliated with an academic university hospital in Changwon, Republic of Korea. The annual ED census of the hospital during the study period was ranged from 38,000 to 42,000 patients.
This is a retrospective cross-sectional study conducted from January 1998 to October 2015. 12
Data collection
Medical records of glufosinate-poisoned patients admitted to the emergency center were examined carefully. Acute glufosinate poisoning was defined based on the history of exposure and characteristic clinical features. Patients with any of the following conditions were excluded: (1) uncertain exposure history, (2) combined drug exposure, (3) exposure for greater than 24 h prior to presentation, (4) discharge against medical advice and transfer to another hospital, (5) prehospital cardiac arrest, (6) less than 15 years of age, (7) history with renal failure or renal disorder, or (8) missing data.
Standardized medical emergency procedures were followed to assess glufosinate intoxication. Gastric lavage was performed for all subjects observed within 2 h after ingestion. Hemodialysis or hemoperfusion was started if indicated.
From the medical records, two investigators collected the following parameters: age, sex, amount of glufosinate ingested, systolic blood pressure (SBP), diastolic blood pressure (DBP), mean arterial blood pressure (MAP; mmHg), heart rate, respiratory rate, body temperature, initial Glasgow Coma Scale (GCS), arterial blood gas analysis (pH, partial pressure of oxygen (PaO2), and partial pressure of carbon dioxide), fraction of inspired oxygen (FiO2), PaO2/FiO2 ratio (mmHg), 13 laboratory data (white blood cell count; hematocrit; platelet count; and sodium (Na), potassium (K), BUN, creatinine, albumin, glucose, aspartate aminotransferase, ALT, bilirubin, amylase, lipase, and C-reactive protein (CRP) levels), poisoning mechanism (incidental, intentional, unknown), mentality (alert, verbal response, painful response, and non-response), use of mechanical ventilation, past medical history (acquired immune deficiency syndrome, hepatic failure, lymphoma, metastatic cancer, leukemia/multiple myeloma, immunosuppression, cirrhosis, etc.), seizure, pneumonia, presence or absence of systemic inflammatory response syndrome (SIRS), 14 Shock Index, use of vasopressors (dopamine, dobutamine, norepinephrine), mortality, Sequential Organ Failure Assessment (SOFA) score, Acute Physiology and Chronic Health Evaluation (APACHE) II score, and Simplified Acute Physiology Score (SAPS) II. We defined the volume of ingestion as “a little” or “a spoonful” (5 mL), “a mouthful” (25 mL), “a small cup” (100 mL), and “a bottle” (300 mL).
The investigators who collected the data were blinded to the study objectives. They collected the same data and compared them for accuracy.
The SOFA score, APACHE II score, and SAPS II were calculated as described previously. 15 –17 Based on logistic regression predictive model for the scoring systems, the probability of death was calculated and compared between survivors and non-survivors.
Statistical analysis
Data were analyzed using IBM SPSS statistics 24.0 version (IBM Corp, Armonk, New York, USA) and MedCalc 15.6 version (MedCalc Inc., Mariakerke, Belgium). Data were presented as mean ± standard deviation, median with interquartile range, or frequency. Differences between the two groups were tested using the independent two-sample t-test or the Mann–Whitney U-test for continuous variables and the χ2 test or Fisher’s exact test for categorical variables. All variables significant in a univariate analysis underwent multivariate logistic regression analysis. Logistic regression analysis was performed with a backward elimination procedure to analyze predictors with a p value of less than 0.05 in univariate analysis. The area under the receiver operating characteristic (ROC) was calculated to determine the ability of the scores to discriminate using mortality as an independent variable. Cut-off values were determined by analyzing the best Youden index (sensitivity + specificity − 1) and the maximal area under the ROC curve. 18
Differences in sensitivities, specificities, and accuracies of the scores were determined using McNemar’s test. Type I error was corrected by Boneferroni’s method for comparisons of three or more variables. Calibration or agreement between predicted mortality of the study population was examined with Hosmer–Lemeshow goodness-of-fit test. Statistical significance was considered when p value was less than 0.05 (p < 0.05).
Ethics statement
This study was conducted in compliance with the principles of the Helsinki Declaration and approved by Institutional Review Board (IRB) of Samsung Changwon Hospital, Sungkyunkwan University School of Medicine (IRB No. 2016-SCMC-009-00). Informed consent was waived by the board.
Results
Among a total of 269 patients enrolled from January 1998 to October 2015, 253 were included in the study. Exclusion criteria were poisoning by any additional material except alcohol (n = 3; two by pyrethroid and one by glyphosate), prehospital cardiac arrest (n = 1), and insufficient data (n = 3; Figure 1). Of the 253 patients, 34 (13.4%) died, including 25 (73.5%) died in the hospital and 9 (26.5%) died after being discharged with impending death.

Study profile of glufosinate-poisoned patients between January 1998 and October 2015.
The baseline and clinical characteristics of the enrolled patients are summarized in Table 1. Their mean age was 58 years (range: 21–98 years). Of the 253 patients, 178 (70.3%) were males.
Baseline and clinical characteristics of patients with acute glufosinate poisoning.a
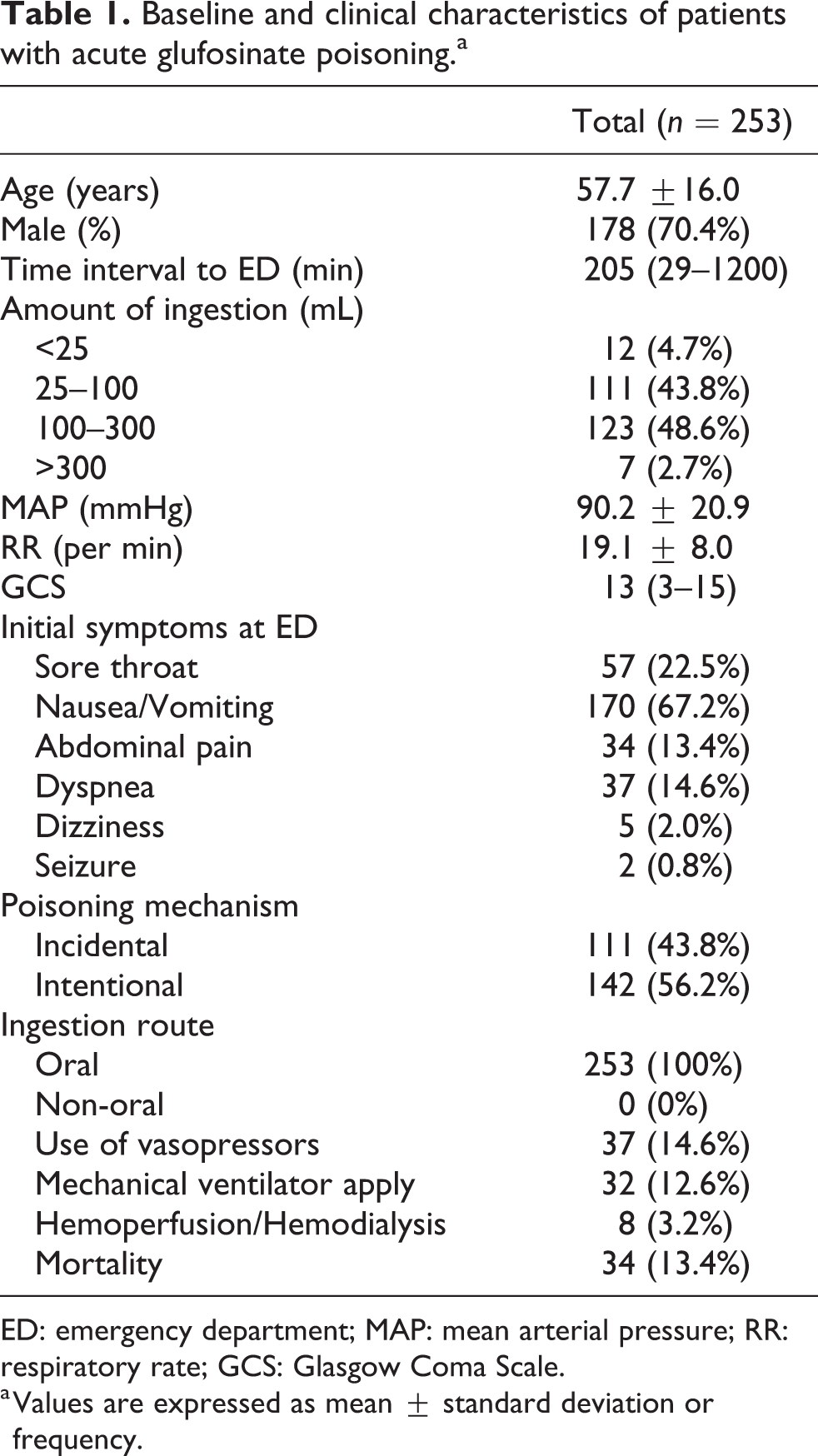
ED: emergency department; MAP: mean arterial pressure; RR: respiratory rate; GCS: Glasgow Coma Scale.
a Values are expressed as mean ± standard deviation or frequency.
Poisoning mechanism (incidental vs intentional) and ingestion route (oral vs non-oral) were significantly different between survivors and non-survivors (p = 0.004 and 0.001, respectively). Patient’s initial symptoms of dyspnea with or without chronic illness (metastatic cancer, hematologic malignancy), pneumonia, use of vasopressors, and mechanical ventilator apply were significantly different between survivors and non-survivors (all p < 0.001). However, patient’s initial symptoms of sore throat, nausea/vomiting, abdominal pain, dizziness, seizure at ED, and presence or absence of SIRS (p = 0.156) were not significantly different between survivors and non-survivors. SBP, DBP, Shock Index, PaO2, FiO2, mechanical ventilator apply, and ICU days were significantly different between survivors and non-survivors (p < 0.05 for all comparisons). The general characteristics and laboratory data related to the demographic and laboratory findings in both survivors and non-survivors are summarized in Table 3. Age, amount of ingestion, creatinine, amylase, lipase, Na, K, lactate, ammonia, CRP, SOFA score, APACHE II score, and SAPS II score in non-survivors were higher than those in survivors, whereas MAP, GCS, PaO2/FiO2, bicarbonate (HCO3 −), and pH in non-survivors were lower than those in survivors (p < 0.05 for all comparisons; Table 2). APACHE II, SAPS II, and SOFA scoring systems were significantly different between survivors and non-survivors (Table 2).
Characteristics and laboratory findings between survivors and non-survivors.a

MAP: mean arterial pressure; RR: respiratory rate; GCS: Glasgow Coma Scale; WBC: white blood cell count; CRP: C-reactive protein; APACHE II: Acute Physiology and Chronic Health Evaluation II; SAPS II: Simplified Acute Physiology Score II; SOFA: Sequential Organ Failure Assessment; PaO2: partial pressure of oxygen; FiO2; fraction of inspired oxygen; Na: sodium; K: potassium; HCO3 –: bicarbonate.
a Values are expressed as mean ± standard deviation or frequency.
Multiple logistic regression analysis of clinical parameters predicting mortality after glufosinate ingestion.a,b,c

GCS: Glasgow Coma Scale; MV apply: mechanical ventilator apply; vasopressor: use of vasopressors (dopamine, dobutamine, norepinephrine); SBP: systolic blood pressure; WBC: white blood cell count; AST: aspartate aminotransferase; CRP: C-reactive protein; GCS: Glasgow Coma Scale; ROC: receiver operating characteristic; PaO2: partial pressure of oxygen; FiO2; fraction of inspired oxygen; Na: sodium; HCO3 −: bicarbonate; CI: confidence interval.
a Mental status, amount of ingestion, past history, age, vasopressors, dyspnea, hemodialysis, MV apply, PaO2/FiO2, SBP, WBC, HCO3 −, lactate, creatinine, potassium, Na, AST, ammonia, CRP, pH, GCS, amylase, and lipase were included in the backward-elimination logistic regression analysis after the variables were dichotomized according to cut-off values from the ROC curve analysis.
b Nagelkerke R2: 0.670.
c Hosmer–Lemeshow test: p = 0.901.
Multivariate analysis (outcome: mortality) was performed with a p value of <0.05, which was included in all variables. The probability of death estimate as predictors (GCS, HCO3 −, mechanical ventilator apply, and use of vasopressors) is shown in Table 3 for both survivors and non-survivors.
The predictive power of mortality estimates for each variable for the overall study population according to predictors (GCS, HCO3 −, mechanical ventilator apply, and use of vasopressors) is shown in Table 4.
Sensitivities, specificities, positive predictive value, and negative predictive value of the GCS, HCO3 −, mechanical ventilator apply, and use of vasopressors for predicting mortality.a

PPV: positive predictive value; NPV: negative predictive value; GCS: Glasgow Coma Scale; MV apply: mechanical ventilator apply; vasopressor: use of vasopressors (dopamine, dobutamine, norepinephrine); HCO3 −: bicarbonate.
a Values are 95% confidence interval.
The area under the ROC curve was calculated to evaluate the predictive value of the predictors (GCS, HCO3 −, mechanical ventilator apply, and use of vasopressors) and the scoring systems (Figure 2).

Receiver operating curves for predicting death according to the predictors (GCS < 9, HCO3 − < 16.0 mmol/L, mechanical ventilator apply, and use of vasopressors), the SOFA, APACHE II, and SAPS II scoring systems. The areas under the curve and 95% confidence intervals for these indicators were 0.952 (0.910–0.994) for the predictors, 0.829 (0.749–0.908) for the SOFA, 0.927 (0.885–0.969) for the APACHE II, and 0.944 (0.904–0.985) for the SAPS II. GCS: Glasgow Coma Scale; HCO3 −: bicarbonate; SOFA: Sequential Organ Failure Assessment; APACHE: Acute Physiology and Chronic Health Evaluation; SAPS: Simplified Acute Physiology Score.
Discussion
In this study, the predictors of mortality following acute glufosinate poisoning were found to be decreased: GCS and HCO3 −, mechanical ventilator apply, and use of vasopressors. Many studies have reported that GCS and HCO3 −, mechanical ventilator apply, and use of vasopressors are useful for evaluating the mortality of all patients. These findings are consistent with our results.
The GCS was introduced in 1974. 19 It was the first grading scale to offer an objective assessment of the consciousness of patients. There is a linear relationship between decreasing GCS sum score and increasing mortality in patients with traumatic brain injury. 20 In our study, the overall mortality rate was 13.4%. Patients with GCS < 9 died significantly much more than patients with GCS > 9.
HCO3 −, an alkaline, is a vital component of the pH buffering system of the human body to maintain acid–base homeostasis. 21 A low serum HCO3 − concentration can be manifested as an important clinical disturbance to metabolic acidosis, which may depress cardiac contractility and predispose patients to pulmonary edema by decreasing pulmonary vascular compliance. Disturbance to metabolic acidosis is believed to be an important cause of many deleterious metabolic consequences including protein-energy wasting, inflammation, bone disease, and disturbance in endocrine function. 22 –24 This study showed that a low serum HCO3 − level (HCO3 − < 16.0 mmol/L) was an independent risk factor for mortality in patients with acute glufosinate poisoning. The relationship between low HCO3 − levels and adverse outcome may be related to depressed cardiac contractility and enhanced inflammation.
Mechanical ventilation can be noninvasive involving various types of face masks or invasive involving endotracheal intubation. There are numerous indications for endotracheal intubation and mechanical ventilation. However, in general, mechanical ventilation should be considered when there are clinical or laboratory signs that the patient cannot maintain an airway, adequate oxygenation, or ventilation. In this study, mechanical ventilator was initially applied to 173 people, of which 33 died. For 80 patients who initially did not use mechanical ventilator, one person died.
Vasopressors are powerful drugs that can induce vasoconstriction, thereby elevating MAP. 25 Vasopressors are indicated for a decrease of greater than 30 mmHg from baseline SBP or an MAP < 60 mmHg that results in end-organ dysfunction due to hypoperfusion. In this study, we use the vasopressors (dopamine, dobutamine, norepinephrine) and found that such use was associated with mortality of patients.
In this study, we compared the performance of SOFA, APACHE II, and SAPS II scores of patients with acute glufosinate poisoning to predict mortality. APACHE II uses a point score based on initial values of 12 routine physiological measurements, patient age, and medical history to provide a general measure for disease severity. This system stratifies a wide variety of patients according to prognosis because of the strong and consistent relationship between acute physiological dysfunction and the risk of death due to acute illness. 26 –28 SAPS II score is calculated based on 12 routine physiological measurements during the first 24 h, health status information, and information obtain at admission. This calculation method results in a predicted mortality. 17 The SOFA score was developed during a consensus conference organized by the European Society of Intensive Care and Emergency Medicine. The SOFA score calculates a summary value for the degree of dysfunction of six sets of organs (respiratory, coagulation, liver, cardiovascular, central nervous system, and renal). We confirmed that mortality of patients with acute glufosinate poisoning could be predicted precisely using any of the three scoring systems upon ICU admission. Any of the three scores could be used as an objective parameter to identify glufosinate-poisoned patients being monitored in the ICU. And, the four predictors found in this study (GCS < 9, HCO3 − < 16.0 mmol/L, mechanical ventilator use, and use of vasopressors) had better overall performance compared to the three scoring systems.
Our study has several limitations. First, due to the single-center retrospective nature of the study, our results may lack wider applicability due to missing data and small sample size. In addition, we could not determine the effect of time difference between patient arrival at ED and the time they ingested the poison because this was a retrospective study. Furthermore, we did not measure plasma glufosinate level although it might be able to reflect the severity of glufosinate exposure more accurately. Therefore, a multi-center or randomized trial should be conducted in the future, and plasma glufosinate levels should be determined to avoid these limitations and confirm our results.
Conclusions
We evaluated the factors associated with mortality of patients with acute poisoning by glufosinate-containing herbicide. Four predictors (GCS < 9, HCO3 − < 16.0 mmol/L, mechanical ventilator apply, and use of vasopressors) provided potentially valuable prognostic information to evaluate the severity and mortality of patients with acute glufosinate poisoning. Combination of these four predictive variables showed better discriminative power for predicting mortality compared to APACHE II, SOFA, and SAPS II for patients with acute glufosinate poisoning.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.