
Abstract
Background:
Acute pesticide poisoning has long been a serious problem as a method of suicide worldwide. This poisoning is a highly fatal condition that requires a rapid and precise diagnosis for adequate treatment. However, various studies on mortality predictor factors have been insufficient for whole pesticide treatments. We hypothesized that the initial plasma anion gap (AG) and base deficit (BD) are reliable prognostic factors.
Methods:
A retrospective study analyzed 561 patients with a diagnosis of acute pesticide poisoning between January 1, 2014 and June 30, 2017. The initial AG and BD values were divided into quartiles according to the number of patients. Survival at 30 days from admission was estimated using the Kaplan–Meier survival analysis. Receiver-operator characteristic (ROC) curves were drawn, and the areas under the curve for AG and BD for mortality were calculated.
Results:
Fifty-eight (10.3%) of 561 patients died within 30 days. The highest AG quartile (>22 mEq/L) was associated with an increased risk of 30-day hospital mortality. Compared to patients with an AG less than 14.7 mEq/L, these patients had a 4.18-fold higher risk of 30-day hospital mortality and the highest BD quartile (>7.9 mEq/L) was associated with an increased risk of 30-day hospital mortality. Compared to patients with a BD less than 1.4 mEq/L, these patients had 2.23-fold higher risk of 30-day hospital mortality. The areas under the ROC for AG and BD curve were 0.699 and 0.744, respectively.
Conclusions:
Initial high AG and BD values could predict mortality and require precise intensive care.
Introduction
Pesticide poisoning has long been a serious problem as a method of suicide worldwide. 1 Pesticides are classified as herbicides, insecticides, and rodenticides. 2 Globally, more than 800,000 people died by suicide in 2012, according to World Health Organization (WHO) Global Estimates. 3 WHO has reported that pesticide poisoning is now the most common method of suicide, and it has been estimated that they accounted for approximately 30% of all suicides worldwide in 1990–2007. 4–5 A conservative estimate based on these data indicates that there were approximately 110,000 pesticide self-poisoning deaths each year from 2010 to 2014, comprising 13.7% of all global suicides. Pesticide self-poisoning remains a major public health concern although there appears to have been a substantial decline in recent years. 6
Acute pesticide poisoning is a highly fatal condition that requires a rapid and precise diagnosis for adequate treatment. Predicting prognostic factors is important to have a proper and rapid treatment. There are various studies on predicting the outcome factors of poisoning patients. 7 Several clinical studies have evaluated the severity of paraquat (PQ) poisoning, including plasma PQ concentration, arterial lactate, lactate metabolic clearance, the Acute Physiology and Chronic Health Evaluation II (APACHE II) score, the Sequential Organ Failure Assessment score, and the severity index of PQ poisoning. 8 –10 Studies for predicting the outcomes of organophosphate insecticide poisoning use the red cell distribution width (RDW), base deficit (BD), the Glasgow Coma Scale, the APACHE II score, C-reactive protein levels, and electrocardiogram recordings (e.g. prolongation of heart rate-corrected QT interval). 11 –16 The anion gap (AG) is a predictive factor in patients with acute pesticide poisoning. 17 Age >50 years, X-ray abnormalities, and alanine aminotransferase (ALT) >40 U/L were significant predictive factors for complications in patients with glyphosate surfactant herbicide poisoning. 18 There have been several studies investigating mortality predictor factors by type of pesticide, but the studies are insufficient for treating whole pesticides. Additionally, the kind of pesticide may not be known at the initial stage and in many cases the kind of pesticide is wrong or mixed with other types of pesticide poisoning in the actual field.
Acute pesticide intoxication often affects the acid–base balance due to a variety of factors. Respiratory acidosis and metabolic acidosis are also a common clinical presentation of acute pesticide poisoning. 19 Therefore, it is important to assess the acid–base equilibrium status in patients with acute pesticide poisoning. The BD represents tissue hypoperfusion and hypoxia, and it is defined as the amount of strong acid or base required to normalize the pH of 1 liter of whole blood to 7.4, assuming a temperature of 37°C and a partial pressure of carbon dioxide (PCO2) of 40 mmHg. 20 Increased serum AG was associated with results from variable drug intoxication, methanol and ethanol poisoning, cyanide poisoning, ethylene glycol poisoning, and pesticide poisoning. 17,21 –24 If acute pesticide poisoning progresses, the patient begins to feel weak and drowsy, eventually, leading to shock, coma, and death. 2 In light of these findings, we hypothesized that AG and BD are reliable prognostic factors in patients with pesticide poisoning.
Methods
Ethics statement
This study followed the guidelines of the Declaration of Helsinki and was approved by the Gyeongsang National University Hospital institutional review board.
Study setting
A retrospective study was performed on 854 patients who attempted suicide by pesticide ingestion between January 1, 2014 and June 30, 2017, at a single emergency department (ED) in an 800-bed academic hospital with an annual ED census of 35,000 patients. We reviewed a database of patient poisoning data from electronic charts.
We analyzed 621 patients with a diagnosis of acute pesticide poisoning. Patients were excluded if they were transferred from another hospital after treatment of the acid–base equilibrium imbalance with intravenous sodium bicarbonate (NaHCO3) administration or after receiving hemodialysis, and mixed pesticide poisoning patients with other drug or chemical material were also excluded. The type of pesticide was confirmed by the pesticide bottle that was presented by patients or family. Unconfirmed types of pesticides were declared to be unknown. A total of 561 patients were included in this study and 60 patients were excluded, including 36 patients who were transferred to other hospitals, 17 patients who were discharged against medical advice, 3 patients who experienced prehospital cardiac arrest, and 4 patients who inhaled the poison or were poisoned through skin contact.
In the ED, patients received standard medical emergency treatment. Treatment for acute pesticide poisoning begins with airway management and adequate oxygen. Endotracheal intubation and mechanical ventilation were performed when patients had respiratory or hemodynamic compromise. Decontamination with gastric lavage was performed within 2 h after ingestion, and activated charcoal administration was conducted when indicated.
Data collection
All patient-related data were obtained from a consecutive retrospective chart review. Demographic variables (e.g. age and gender) and initial vital signs were collected. Pesticides were categorized as herbicides, insecticides, fungicides, and unknown. The initial laboratory findings, including tests for arterial pH, HCO3, BD, electrolytes (Na+, K+, Cl−), white blood cell count, hemoglobin, platelet count, blood urea nitrogen, creatinine, albumin, and creatinine kinase, were obtained simultaneously in the emergency room prior to beginning extracorporeal treatment. The serum AG corrected for albumin was calculated as follows: serum AG = Na – [Cl + HCO3 + 0.25 (normal albumin − observed albumin)]. The normal range of the serum AG was defined as 6–14 mEq/L, and serum AG >14.1 mEq/L was considered to be a high level. 25 BD is defined as the amount of base required to return the blood pH to homeostatic levels. The normal range of BD is -2 to +2 mEq/L. 26 The arterial blood gas test including arterial pH, HCO3, and BD levels were determined using the Rapid lab 1265 blood gas analyzer (Simens, Germany).
A comparison of BD and AG was performed on patients with acute pesticide poisoning. The parameter for assessing clinical outcomes of this study was hospital mortality within 30 days after ED admission for acute pesticide poisoning.
Statistical analysis
Continuous variables were expressed as the mean with SD and were compared using Student’s t-test. Categorical data were described according to the frequency of occurrence (percentage) and compared with a χ 2 test. The AG values were divided into quartiles according to the number of patients: less than14.7 mEq/L (n = 139), 14.7–7.7 mEq/L (n = 144), 17.8–22.0 mEq/L (n = 136), and greater than 22 mEq/L (n = 142). The BD values were divided into quartiles according to the number of patients: less than 1.4 mEq/L (n = 145), 1.4–3.7 mEq/L (n = 138), 3.8–7.8 mEq/L (n = 139), and greater than 7.8 mEq/L (n = 139). Thirty-day survival (from ED admission) was estimated using the Kaplan–Meier survival analysis, and the 30-day survival relationship of the AG level and the BD level represents the linear regression analysis. Univariate and multivariate Cox proportional hazards regression analyses were applied to investigate the predictors of 30-day hospital mortality. Receiver-operator characteristic (ROC) curves were drawn, and the area under the curves (AUCs) of the AG and the BD for mortality were calculated. Furthermore, a comparison of the AG and the BD for 30-day hospital mortality was determined using Youden’s J statistic and ROC curves. All of the p values were two-sided, and p < 0.05 was considered to be statistically significant. All statistical analyses were performed using the SPSS 21.0 software (SPSS Inc., Chicago, IL, USA) and MedCalc software (version 9.3.7.0; MedCalc Software, Ostend, Belgium).
Results
The distribution of the types of the 561 pesticide poisoning patients is shown in Table 1. Two hundred ninety-nine (53.3%) patients had herbicide poisoning, 194 (34.6%) patients had insecticide poisoning, 39 (7.0%) patients had fungicide poisoning, and 29 (5.2%) patients had unknown pesticide poisoning. Fifty-eight (10.3%) of these patients died within 30 days. Table 2 summarizes the baseline demographics and clinical characteristics of acute pesticide poisoning patients.
Distribution of pesticide poisoning patients.a
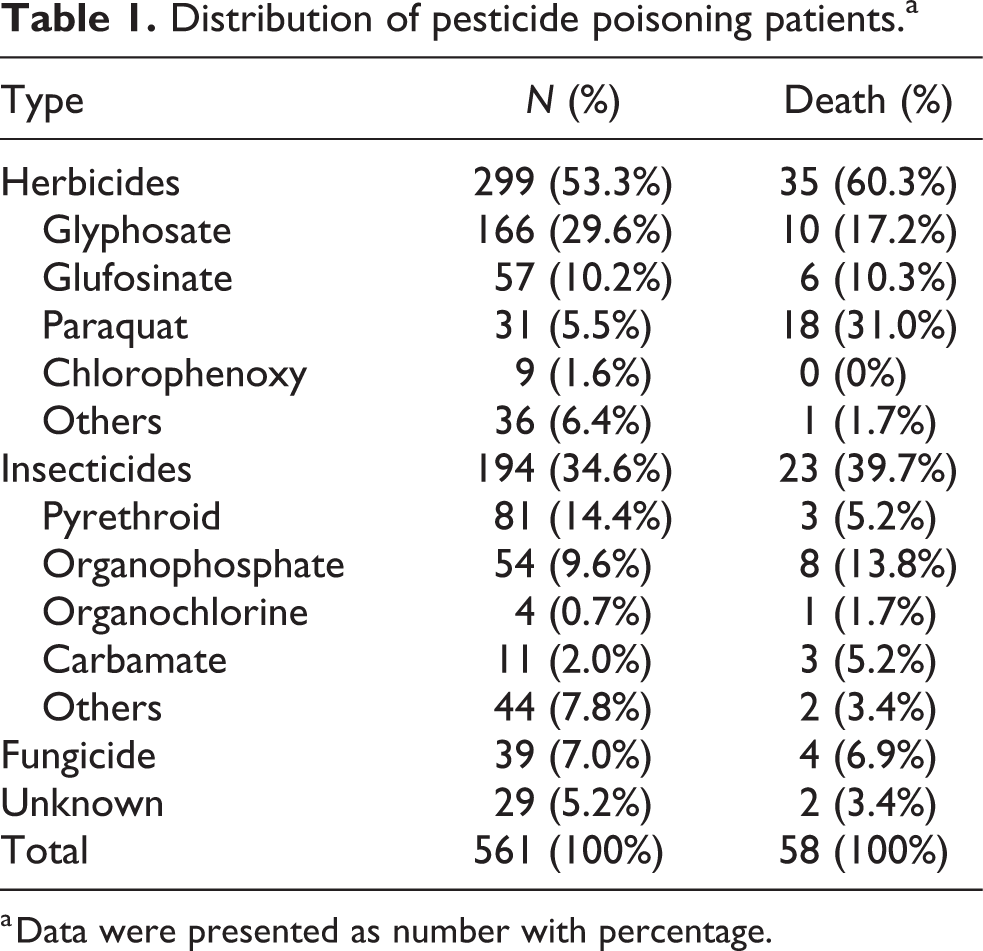
a Data were presented as number with percentage.
Baseline demographics and clinical characteristics of pesticide poisoning patients.a

a Data were presented as means with SDs.
SBP: systolic blood pressure; WBC: white blood cell; BUN: blood urea nitrogen; SD: standard deviation.
b Difference calculated by comparing survivor and nonsurvivor (chi-square test)
Increased AG was associated with a significantly higher risk of 30-day hospital mortality in the Kaplan–Meier survival analysis with a log-rank test. The highest AG quartile (Q4: >22 mEq/L) had the lowest survival rate, and the quartiles lowered in order the second AG quartile (Q3: 17.8–22.0), the third AG quartile (Q2: 14.7–17.7), and the lowest AG quartile (Q1: <14.7) were significantly different (p < 0.001) (Figure 1). Increased BD was associated with a significantly higher risk of 30-day hospital mortality in the Kaplan–Meier survival analysis with a log-rank test. The highest BD quartile (Q4: >7.8 mEq/L) had the lowest survival rate, and those lowered in order the second BD quartile (Q3: 3.8–7.8), the third BD quartile (Q2: 1.4–3.7), and the lowest BD quartile (Q1: <1.4) were significantly different (p < 0.001) (Figure 2).
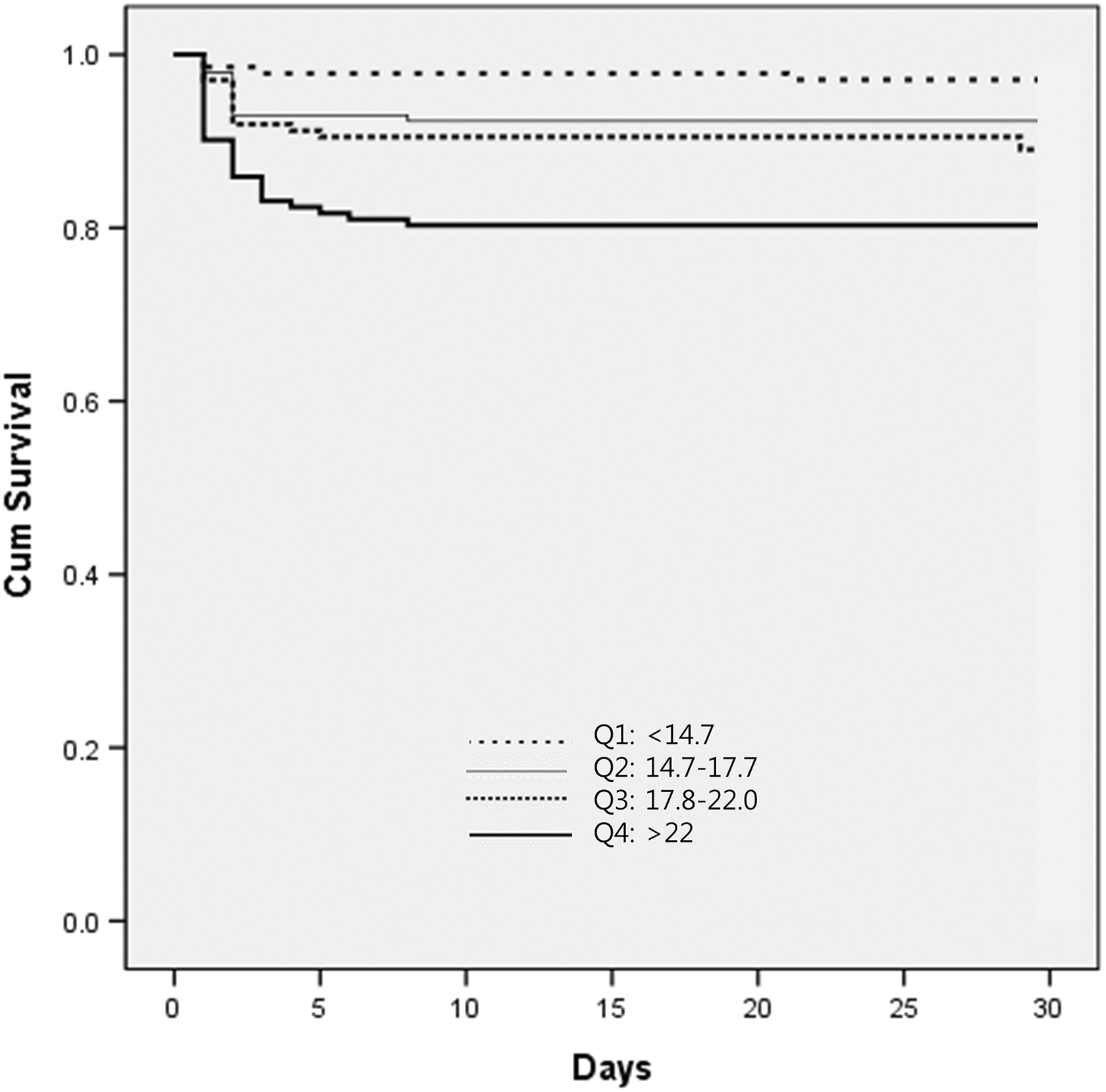
Kaplan–Meier survival curve of plasma anion gap by patients with acute pesticide poisoning. p < 0.001 for the log-rank test.

Kaplan–Meier survival curve of base deficit by patients with acute pesticide poisoning. p < 0.001 by the log-rank test.
The univariate and multivariate Cox regression analyses are shown in Tables 3 and 4. In the multivariate analysis, the highest AG quartile (>22 mEq/L) was associated with an increased risk of 30-day hospital mortality. Compared to patients with AG less than 14.7 mEq/L, these patients had a 4.18-fold higher risk of 30-day hospital mortality, and the highest BD quartile (>7.8 mEq/L) was associated with an increased risk of 30-day hospital mortality. Compared to patients with a BD less than 1.4 mEq/L, they had a 2.23-fold higher risk of 30-day hospital mortality.
Cox regression analysis of risk factors for mortality within 30 days in AG quartile.

HR: hazard ratio; CI: confidence interval; SBP: systolic blood pressure; AG; anion gap
Cox regression analysis of risk factors for mortality within 30 days in BD quartile.

HR: hazard ratio; CI: confidence interval; SBP: systolic blood pressure; BD: base deficit.
A comparison of the AG and BD for predicting 30-day hospital mortality was conducted by ROC curve analysis. The cut-off point for AG was more than 19.1, and the area under the ROC curve was 0.699 (95% CI, 0.676–0.813). When the AG was more than 19.1, the sensitivity was 84.2%, and the specificity was 65.1%. The cut-off point for BD was more than 7.1, and the area under the ROC curve was 0.744 (95% CI, 0.627–0.770). When the BD was more than 7.1, the sensitivity was 86.4%, and the specificity was 68.1%. The p value of each AUC was 0.37 (Figure 3).

Comparison of areas under the ROC curve for predicting 30-day mortality during acute pesticide poisoning with AG and BD.
Discussion
The traditional risk factors for death by acute pesticide poisoning are the toxicity of the major component, ingestion amount, time taken to arrive at the hospital, and the clinical characteristics of the patient after arriving at the hospital: age, illness or medical condition, vital signs, and consciousness. 17 In addition, previous studies have shown that acute organophosphate poisoning is a predictive factor of severity and mortality, and it may be expressed using APACHE II, BD, and RDW. 11, 12, 27 Patients with ethylene glycol, methanol, and cyanide poisoning have high AG levels in plasma. 21 –23 The acid–base status predicts the survival of the poisoned patients. 28 However, various studies on mortality predictor factors have been insufficient for whole pesticides, and these parameters may have been limited to their rapid and adequate use in ED for patients with acute pesticide poisoning. Additionally, in initial emergency room sites, it is not often that we learn about the types of pesticides from initial management start, and there are many cases that different kinds of pesticides are judged or mixed with other types of pesticide poisoning. So, it was judged that access to the overall pesticide would be needful. In the present study on patients with acute pesticide poisoning, we observed that AG levels of non-survivors were higher than those of survivors, and there was a graded association between AG and 30-day mortality (Figure 1). We also observed that BD levels of non-survivors were higher than those of survivors, and there was a graded association between BD and 30-day mortality (Figure 2).
BD is defined as the amount of base required to return the blood pH to homeostatic levels. The normal range of BD is -2 to +2 mEq/L, and a high BD, along with lactate, correlates with metabolic acidosis, hypoperfusion, and oxygen debt. BD has also been observed to be a prognostic risk factor in patients with multiple traumas and burns. 26, 29
Calculating the serum AG is the first step in analyzing acid–base equilibrium disorder. The level of AG is mostly increasing because there is an increase in unmeasured anions, but less commonly, there is a decrease in cations. The definition of the AG as the unmeasured anion is incorrect in the current study. The serum AG may decrease with a decrease in anionic albumin. The normal range of the serum AG was defined as 6–14 mEq/L, and serum AG >14.1 mEq/L was considered to be a high level. 24, 30
Acute pesticide poisoning patients with acid–base equilibrium disorder are highly common in everyday clinical practice. Acid–base equilibrium disorder results from various causes. Clinical manifestation of respiratory failure, unconsciousness, and seizure can result in respiratory acidosis, and metabolic acidosis is also common, whether directly or as compensation action. 17 Drug-induced acid–base disorder can be classified into five different categories— (1) metabolic acidosis caused by acid overload, which may occur through the accumulation of acids by endogenous mechanisms, (2) base loss: proximal renal tubular acidosis caused by drugs, (3) alkalosis resulting from acid loss, (4) exogenous HCO3 loads, and (5) respiratory acidosis or alkalosis resulting from drug-induced depression of the respiratory center or neuromuscular impairment. 19 BD may be used as a substitute to detect metabolic acidosis because it has a strong linear correlation with serum HCO3. 31
Acute pesticide poisoning patients died within 30 days of their ED admission due to various causes. The mechanism of death in acute pesticide poisoning has a complex background. There are various kinds of pesticides and complex ingredients. Pesticide formulations are generally composed of active ingredients and inert ingredients. The additives include surfactant, spreader, diluent, solvent, emulsifier, synergist, and safener. 32, 33 It is unclear which factors play a dominant role in pathophysiology during the process of an important clinical outcome. However, we can assume pathophysiologically that the mechanism of metabolic acidosis is due to organ damage by the chief ingredient, direct cell injury due to exogenous factors, metabolites, hypoxia, and increased lactate levels. 34, 35 Metabolic acidosis occurs when either an increase in the production of nonvolatile acids or a loss of bicarbonate from the body overwhelms the mechanism of acid–base homeostasis or when renal acidification mechanisms are compromised. 36 Abnormalities in intermediary mechanisms such as lactic acid synthesis can increase acid production severalfold. 37 Plasma AG is a valuable diagnostic tool as the various disorders that produced metabolic acidosis can affect the plasma AG differently. No change in the AG is observed in some disorders, whereas in other disorders, the plasma AG is increased (high AG metabolic acidosis). 38, 39 Mixed normal and high AG patterns are also common. In our study, we were able to estimate the relevance of AG and patients with pesticide poisoning. Irrespective of the definition of high AG, higher level of AG and mortality is associated. There was a statistical significance in both the 30-day mortality of AG level and the 30-day mortality of BD level (Figure 3).
Limitations
Several limitations of this study must be acknowledged. First, our study was a retrospective review potentially limited by selection bias. Therefore, to eliminate potential selection bias, the study excluded patients who were administered intravenous NaHCO3 before blood collection, were transferred to other hospitals, were discharged against medical advice, or experienced either prehospital cardiac arrest or unintentional poisoning. Second, the amount of time before arrival at the emergency room was not considered, which may have influenced our initial findings. Third, without considering various ingredients and additives, it is difficult to accurately identify each mechanism. Our study investigated predictor mortality factors of whole pesticide poisoning, because it is difficult to determine the type of pesticides, especially in the early stages. Fourth, we used only the initial reports of AG and BD, which were measured upon admission to the ED, and subsequent AG and BD measurements after the intervention were not collected in the study. At the present time, these subsequent measurements would be difficult to study because stable patients rarely are subsequently subjected to these measurements and patients who die within a short time after acute pesticide poisoning are also not subjected to these measurements. Additionally, subsequent values of AG and BD are affected by NaHCO3 treatment. Furthermore, patients in the study were not treated by the same physician. However, the treatments were performed according to appropriate protocols by trained physicians. Despite these limitations, we are confident that AG and BD could be reliable prognostic factors in patients with acute pesticide poisoning, and the initial AG and BD values are important with regard to the patient’s clinical condition.
Conclusions
Acute pesticide poisoning may be a highly fatal condition that requires a fast and proper treatment. Initial high AG and BD values could be used to predict mortality and require precise intensive care
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.