
Abstract
Objective:
This study aimed to assess the demographic characteristics, emergency department (ED) complaints, laboratory findings, and latent phase periods of patients who presented to the ED due to mushroom poisoning (MP) as well as the efficacy of conventional and hemofiltration therapies.
Method:
The study was conducted on patients who presented to the ED with MP between 2010 and 2012. The patient’s demographic characteristics, complaints at the ED, latent phases, laboratory findings, and treatments of MP cases were evaluated.
Results:
The mean age of patients was 38.03 ± 15.96, where 63.8% of them were female and 36.2% were male. Visits occurred most frequently in the autumn (32.6%). When presenting to the ED, the most frequent complaint was nausea–vomiting. The aspartate aminotransferase (AST), alanine aminotransferase (ALT), international normalised ratio (INR), and blood urea nitrogen values of patients with a latent phase between 0 h and 5 h were significantly lower than the values of patients with a latent phase between 6 h and 24 h. In this study, 62% of the patients (n = 36) had stomach lavage and received activated charcoal. Altogether, 55.2% of the patients had received conventional therapy, 37.9% of them received hemofiltration, and all of them received supportive treatment. The AST, ALT, and INR values of those who had received hemofiltration and conventional therapies were significantly higher than of those who received only supportive treatment (p < 0.01).
Conclusion:
Hemofiltration, in combination with conventional therapy, seems to be an effective treatment for reducing mortality in suspected MP cases involving late acting toxins.
Introduction
Mushroom poisoning (MP) is a rare medical emergency with a serious outcome. 1,2 The incidence of MP in Turkey is unclear. 3 Annually, there are more than 1000 wild MP cases reported to the National Poison Control Centre of Turkey. 4 Previous studies have reported an increase in the incidence of MP in the spring and autumn. 5,6,7
Since the identifiers of poisonous and non-poisonous mushrooms are not obvious, consuming wild mushrooms increases the rate of MP. Mushroom appearance, taste, and odour cannot be used to differentiate between poisonous and non-poisonous varieties. The most important method of identifying poisonous mushrooms is to recognize the specific features of a species. However, only experienced people trained in this subject know these features. The toxin content of poisonous mushrooms varies according to climatic and environmental conditions. 8,9 Although poisonings associated with cultured mushrooms (widely consumed by people) may also occur, poisoning from cultured mushrooms is the result of denatured proteins rather than toxins. 10,11
There are more than 5000 mushroom species all over the world and approximately 100 of these species are toxic. According to their clinical symptoms, mushroom toxins are divided into five groups such as (1) toxins that cause cellular damage (cyclopeptides); (2) toxins that affect the renal system; (3) toxins that affect the central nervous system and cause neurological symptoms (ibotenic acid, psilocybin, and psilocin); (4) toxins that affect the autonomic nervous system (muscarine and coprine); and (5) toxins that affect the gastrointestinal system. 6,7,10
MP can cause various clinical conditions ranging from gastroenteritis to mortal liver necrosis. 12 Serious intoxications are rare overall and most deadly MPs are caused by Amanita phalloides species. 3 The amount of toxins in this mushroom species reportedly varies according to the climate and region. 8,9 The most important factors affecting mortality and morbidity in MP are early diagnosis and treatment. Identifying the mushroom type during treatment is vital in distinguishing those with a deadly progress. 13 –15 However, this is not possible in most MP cases. There are various treatment options in mushroom intoxications; these include silibinin, 3,6,10 hemodialysis, 12 hemoperfusion, 16,17 hemofiltration, 18,19 fluid electrolyte treatment, symptomatic treatment, and high-dose penicillin G. 10 Early hemoperfusion reportedly produces successful results, especially in A. phalloides poisonings. 16,17 Some studies indicate that hemofiltration is also an effective treatment in MP. 18 The superiority of hemofiltration over hemoperfusion is seemingly because it is more successful in eliminating toxins that rebound after the procedure. 19
In this study, the purpose was to evaluate the demographic characteristics, emergency department (ED) admission symptoms, laboratory findings, latent phase periods, and the efficacy of conventional and hemofiltration therapies in MP patients.
Method
This study was designed retrospectively by examining the files of patients with MP admitted to the Haydarpasa Numune Training and Research Hospital Emergency Department between January 2010 and December 2012. This study was conducted in accordance with the Declaration of Helsinki II and the Guidelines of Good Clinical Practice.
Demographic characteristics, symptoms on ED admission, latent phases, laboratory findings, and treatments were assessed. Excluded from the study were patients under the age of 18 whose files could not be reached and poisoning cases that occurred for other reasons. Patients over 18, admitted to the ED for MP were included in the study.
Data were presented as mean ± SD or n (%). Parametric data were compared using a Student’s t test. Nonparametric data were compared using a Mann–Whitney U test. A Kruskal–Wallis test was used for a comparison of three or more groups without a normal distribution. Categorical data were compared using Pearson’s χ 2 test and a Yates continuity correction test. The values of p < 0.05 and p < 0.01 were considered statistically significant. Data were analyzed using Number Cruncher Statistical System (NCSS) and Power Analysis & Sample Size (PASS) software (NCSS LLC, Kaysville, Utah, USA).
Results
A total of 58 patients were included in this study. The patients’ ages ranged from 18 years to 71 years. The mean age was 38.03 ± 15.96. Of those patients, 63.8% were females (n = 37) and 36.2% were males (n = 21).
MP was commonly seen in the autumn (32.6%, n = 19). However, many presentations occurred in the spring and winter (25.9%, n = 15), with the least number of presentations occurring in the summer months (15.5%, n = 9).
Upon presentation to the ED, the most common symptom was nausea and vomiting at 69% (n = 42). Twenty (34.5%) patients had abdominal pain and diarrhea, and 16 patients (27.6%) complained of headache. None of the patients experienced dizziness, hypersalivation, dry mouth, blurred vision, tachycardia, or bradycardia.
The duration of time from ingesting the mushroom to the onset of symptoms is defined as the latent phase. The patients in this study were divided into two groups namely those who had a latent phase of 0–5 h and those who had a latent phase of 6–24 h. The 36 patients who had a latent phase of 0–5 h (62.1%) were poisoned from mushrooms that had early acting toxins; the 22 patients who had a latent phase of 6–24 h (37.9%) were poisoned from mushrooms with late acting toxins.
After evaluating the age, gender, time of poisoning, and symptoms of patients according to their latent phases, no statistically significant difference was found (p > 0.05). Table 1 presents an evaluation of descriptive characteristics using the latent phases. The aspartate aminotransferase (AST), alanine aminotransferase (ALT), international normalised ratio (INR), and blood urea nitrogen (BUN) values of patients with a latent phase of 0–5 h were significantly lower than those of patients with a latent phase of 6–24 h. Creatinine (CR) values did not present statistically significant differences according to the latent phases. Table 2 presents an evaluation of laboratory parameters according to the latent phases.
Evaluation of descriptive characteristics by latent phases.

aStudent t test.
bYates’ continuity correction test.
cPearson’s chi-squared test.
Evaluation of laboratory parameters by latent phases.

AST: aspartate aminotransferase; ALT: alanine aminotransferase; INR: international normalised ratio; BUN: blood urea nitrogen; CR: creatinine.
a p < 0.01: Mann–Whitney U test.
b p < 0.05: Mann–Whitney U test.
c p > 0.05: Mann–Whitney U test.
In this study, 62% of the patients (n = 36) were administered lavage and received activated charcoal. Altogether, 55.2% of the patients (n = 30) received conventional treatment (penicillin G + silibinin), 37.9% (n = 22) received hemofiltration (with a carbon filter), and all of them received supportive treatment (fluid + symptomatic treatment). Treatments administered to the patients according to their latent phases were compared and a statistically significant difference was found. The proportion of hemofiltration administration to patients who had a latent phase of 0–5 h was significantly lower than patients who had a latent phase of 6–24 h.
A statistically significant difference exists between the AST, ALT, and INR values in patients according to the manner of treatment. The result of the dual comparisons, conducted to identify which group caused the difference, illustrated that the AST, ALT, and INR values of patients who received hemofiltration and conventional treatment were significantly higher than in patients who only received supportive treatment.
The BUN and CR values of patients did not indicate statistically significant differences according to the manner of treatment. Table 3 presents an evaluation of laboratory parameters according to the manner of treatment.
Evaluation of laboratory parameters by manner of treatment.a
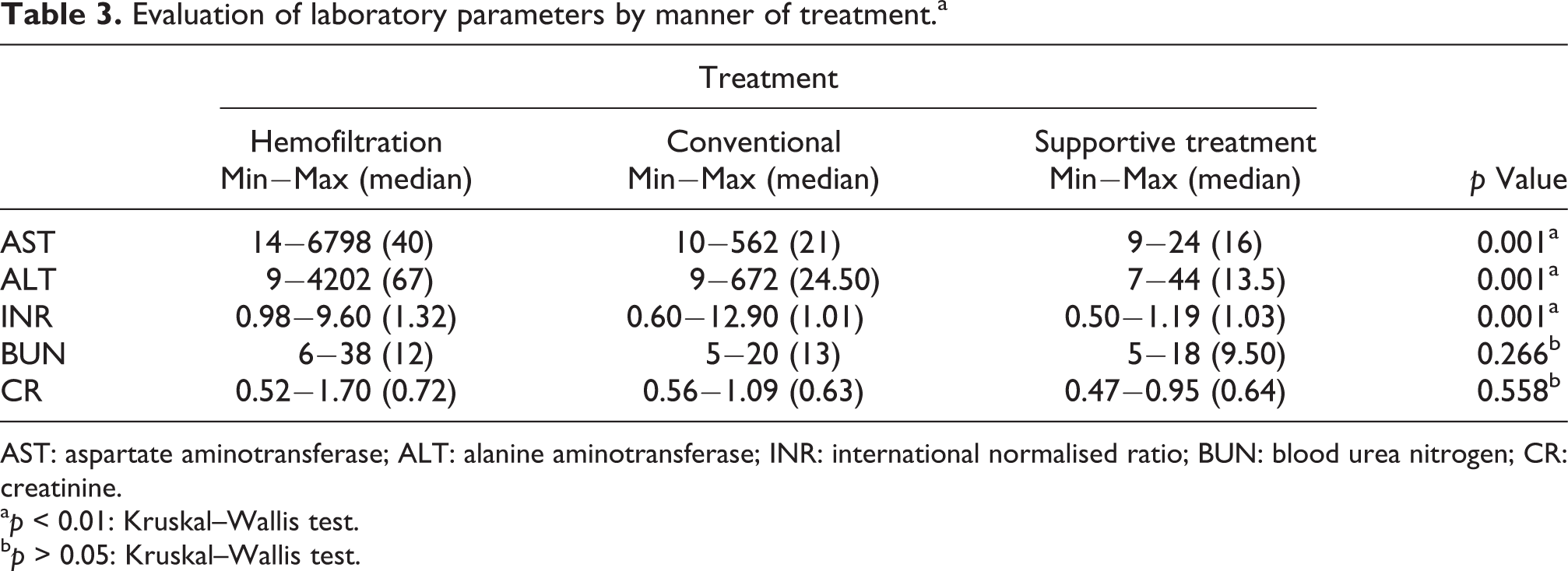
AST: aspartate aminotransferase; ALT: alanine aminotransferase; INR: international normalised ratio; BUN: blood urea nitrogen; CR: creatinine.
a p < 0.01: Kruskal–Wallis test.
b p > 0.05: Kruskal–Wallis test.
While 6.9% of the patients (n = 4) developed liver failure and 5.2% (n = 3) were referred to other centers for transplantation, 1 patient (1.7%) had mortal progression. One of these patients had a latent phase of 0–5 h and three patients had a latent phase of 6–24 h. Two of the three patients (5.2%) who were referred to another center for liver transplantation did not need a transplant; one patient died while waiting for transplantation.
There were four (6.9%) intensive care unit (ICU) admissions. In all, 83.1% of the patients (n = 54) were discharged in a satisfactory clinical condition with the recommendation of outpatient controls, one patient in ICU and one patient with indication of transplantation (3.5%) died.
Discussion
MPs are typically rare. Although incidence is not fully known in Turkey, it is estimated that MP occurs frequently. 1 –3,6 The seasonal breakdown of MP varies by region and mushroom variety. 20 Studies from various regions of Turkey reveal the seasonal breakdown and variations of MP. Some studies have reported that the prevalence of MP increases in the spring. 15,21,22 However, other studies report that MP incidence increases in the autumn. 3,7,20 In this study, hospital visits for MP were observed to be most frequent (32.6%) in the spring. There were a similar number of visits in the autumn and winter (25.9%) with in the summer (15.5%). Mushrooms primarily grow in the spring and autumn; that is when they are commonly collected and consumed—explaining the frequent hospital visits during these times. The prevalence of MPs in other seasons is related with consumption of dried or frozen mushrooms that had been collected in the spring or fall.
MP is reportedly the most frequent between the ages of 35 and 45 with women being the most affected. 6,12,21,23 –25 In this study, the mean age was 36, and women were most frequently affected.
Mushrooms containing early acting toxins produce symptoms shortly after being consumed (approximately 1–2 h). Generally, these are severe gastrointestinal symptoms, the most frequent of which include nausea–vomiting, abdominal pain, and diarrhea. 2,7,11,14,21,22,26 In this case, the most frequently observed symptom was nausea–vomiting. Other major symptoms were abdominal pain, diarrhea, and headache. MP may also result in muscarinic and anticholinergic symptoms. Severe abdominal pain, hypersecretion, hypotension, bradycardia, euphoria, and paraesthesia are among the possible muscarinic effects. Atropine-like effects include hyperpyrexia, mydriasis, delirium, convulsion, and coma. 26 No hypotension, bradycardia, euphoria, paresthesia, delirium, hyperpyrexia, mydriasis, convulsion, or comas were observed in any of the study cases. Mushroom species such as Psilocybe and Panaeolus may also produce hallucinations such as flying bright spots in the eyes. 6 No similar symptoms were observed in any of the study’s cases; the reason may be that these mushrooms do not commonly grow in this region.
Mushrooms that contain late acting toxins usually produce acute poisoning symptoms 6–24 h after having been consumed. 6 Mushrooms containing toxins that cause cellular damage and affect the renal system produce these symptoms. The best known of these are A. phalloides and Gyromitra esculenta. A. phalloides poisoning, which involves the phalloides syndrome, leads to vomiting, abdominal pain, and diarrhea approximately 12 h later with the symptoms gradually intensifying. A rise occurs in liver function tests and the patient will suffer hepatic damage. Clinical prognosis varies depending on the amount of toxin consumed. If abundant, the patient may die from liver failure; otherwise, the patient can recover without any sequels. Analyses of mushroom toxins are generally performed using the high-performance liquid chromatography (HPLC) method. 27,28 Toxin identification of MPs cannot be performed in the hospital in this study; therefore, identification of the consumed toxins was not possible. The patients whose symptoms began later were deemed to have been poisoned by the mushrooms whose most frequent symptom is nausea–vomiting (36.4%) experienced in the early period. In this study, the AST, ALT, and INR values of those with a latent phase between 6 h and 24 h were significantly higher than the values of those with a latent phase between 0 h and 5 h (Table 2). This result is similar to those in the literature. Although the toxin type cannot be identified in patients presenting to emergency rooms with MP, mushrooms containing late acting toxins are reported to cause poisoning in patients with a latent phase of 6–24 h. Amatoxin is the toxin type that most frequently results in such poisonings, while hepatoxin is reported to cause elevated liver enzymes due to its early impact. 6,10
Early and effective treatment increases survival in cases of MP. 7 Since amatoxins are eliminated from the kidneys, an aggressive fluid therapy should be used to protect patients’ renal function. This therapy also increases toxin discharge from the kidneys. A gastric lavage should be performed to reduce toxin absorption from the gastrointestinal system and activated charcoal should be administered. 29 A gastric lavage was administered to all of the patients within the first 0–5 h (62%); they were given activated charcoal in recurring doses and were hydrated with physiologic saline. Penicillin G is a frequently used medicine. Although its mechanism of action is not obvious, it is reported to prevent α-amanitin from penetrating hepatocytes. Silibinin reportedly enables membrane stabilization by blocking lysosome proteases and prevents the entry of α-amanitin into hepatocytes. 10,29 These two drugs may be used separately or in combination. In this study, 55.2% of the patients (n = 30) were given a conventional treatment and 37.9% of the patients (n = 22) were administered continuous venovenous hemofiltration. The AST, ALT, and INR measurements for patients who received hemofiltration and conventional treatment were significantly higher during the consultation than those of patients who only received supportive treatment. After hemofiltration and conventional treatment, it was observed that the AST, ALT, and INR values of 16 patients (80%) returned to normal and the AST, ALT, and INR values of 4 patients (20%) increased. For this reason, hemofiltration, in combination with an early administered conventional treatment, is believed to be an effective treatment in MP. In this study, liver toxicity developed in four patients; three of these patients (5.2%) were referred to another center for transplantation and one patient died in the ICU. One of the patients who developed liver toxicity had a latent period of 0–5 h and the other three had a latent period between 6 h and 24 h. Early onset of symptoms does not rule out seriousMP. It is possible to consume poisonous mushrooms that cause early and late poisoning together. 7 Therefore, patients with short latent phases should be closely monitored for possible serious liver toxicity.
Although some studies report that MP mortality rate is between 2.3% and 3.8%, 6,30 other studies report higher mortality rates. 31 –33 In this study, mortality was 3.5%. This low mortality rate resulted from most of the MP involving low toxicity and the administration of conventional and hemofiltration therapies at an early stage.
One of the limitations of this study is that the species and toxin levels of the mushrooms were not identified. Other limitations include its retrospective pattern and the small number of patients with serious intoxication being studied.
In conclusion, MPs are common in the Marmara region of Turkey. The fact that all patients presented to the ED within 24 h illustrates that people are aware of poisoning risks. Despite this, they continue to consume mushrooms. People should be informed that mushroom appearance cannot distinguish poisonous from non-poisonous varieties and that eating wild mushrooms can result in death. Conventional treatment, in combination with hemofiltration, seems to be effective in lowering mortality in cases of MP involving late acting toxins; however, there remains a need for further studies.
Footnotes
Conflict of interest
The authors declared no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.