
Abstract
There is a growing concern over the timing of pubertal breast development and its possible association with exposure to endocrine disrupting chemicals (EDCs), such as bisphenol A (BPA). BPA is abundantly used to harden plastics. The aim of this study was to investigate the relation between premature thelarche (PT) and BPA by comparing the urinary BPA levels of PT girls with those of healthy subjects. Twenty-five newly diagnosed nonobese PT subjects (aged 4–8 years) who were admitted to the Pediatric Endocrinology Department at Akdeniz University were recruited. The control group composed of 25 age-matched girls without PT and other endocrine disorders. Urinary BPA levels were measured by high pressure liquid chromatography. The median urinary concentrations of BPA were found to be significantly higher in the PT group compared to the healthy control group (3.2 vs. 1.62 μg/g creatinine, p < 0.05). We observed a weak positive correlation between uterus volume and urinary BPA levels. There was a weak correlation between estradiol and urinary BPA levels (r = 0.166; p = 0.37); and luteinizing hormone and urinary BPA levels (r = 0.291; p = 0.08) of PT girls. Our results suggest that exposure to BPA might be one of the underlying factors of early breast development in prepubertal girls and EDCs may be considered as one of the etiological factors in the development of PT.
Introduction
Puberty is a critical period of life and it causes dramatic physiologic and psychological changes. A recent decline in the onset of puberty has been observed particularly among girls, first in the United States in the mid-1990s and now also in Europe. Early breast development is especially prevalent during the first year of life, when the gonadal axis is usually active. 1 Premature thelarche (PT) is defined as “early breast development in girls” and is frequently regarded a benign condition that disappears without influencing stature growth and the timing of puberty. In the last decade, the development of breast tissue in girls occurs at a much younger age and the incidence of PT is rising.
There are not clear numbers for the prevalence of PT and precocious puberty (PP) in Europe and also in Turkey. In Istanbul, the biggest city of Turkey, the prevalence of PT and PP were found to be 8.9% (73 of 820 girls) and 4.3% (35 of 810 girls), respectively. 2 In a US study, the incidence rate of PT in the period 1940–1984 was 2.1 per 10,000 person years. 3 A population-based study performed in Minnesota found an incidence of 20.8 in 100,000 for PT, with 60% of cases presenting in the first 2 years after birth and a less pronounced incidence peak at ages 5–7 years. 4 Another study performed in the United States found a prevalence of 2.1% among 3-year-old African-American and 0.7% among Caucasian girls. De Vries et al. (2010) and Pasquino et al. (1995) reported that 13% and 14%, respectively, of girls with PT progressed into PP. 5,6 Curfman et al. (2011) recruited 318 girls (aged 12–48 months) to a study performed in Ohio, United States. They found that the overall prevalence of PT was 4.7%. The prevalence was the highest among White Hispanics (6.5%). The peak prevalence was observed between 12 months and 17 months of age. All PT cases were found to be Tanner stage 2. Upon follow-up, 44% of the cases of PT had persistent breast development. 7 PT is a self-limiting condition in the majority of girls, but it may progress into PP in a subset of girls. 6 –8
PT is generally considered a phenomenon of endogenous origin; but several factors, like genetic predisposition, psychosocial and socioeconomic conditions, nutrition, ethnicity, and increasing prevalence of adiposity, may contribute to this phenomenon. Moreover, different environmental factors are also likely to be involved. The widespread presence of endocrine disrupting chemicals (EDCs), in particular, estrogen-like EDCs (EEDCs), is suspected to contribute to the trend of earlier pubertal onset and early breast development. 9
The similar molecular structure of most of the EEDCs and estrogen is suggested to be the underlying factor of their effects on endogenous hormone balance. In addition, EEDCs can cause various health defects related to disorders of male reproductive tract, 10 –15 reproductive disorders of female like disorders of the ovary and uterus, and breast cancer. 16,17 The effects of EEDCs are prominent, particularly during puberty. 18
Today’s life is inconceivable without plastics. Bisphenol A (BPA) is used to harden plastics. BPA is considered as an EEDC with high abundance in the environment and is used in the production of polycarbonate plastics and epoxy resins used in many consumer products. There is evidence that BPA functions as a xenoestrogen by binding to estrogen receptor α (ERα), ERβ, and strongly to ERRγ. 19 –23 Though there are controversial results on the effects of BPA on sexually dimorphic character, puberty, fertility, and abnormal genital development of female rats, there is also evidence that BPA causes weight gain which is frequently associated with reproductive dysfunction and early onset of puberty and early breast development both in animals and humans. 24 –26
Based on this background and taking into account the frequency of high BPA exposure in humans, particularly in young children, this study aimed to investigate the relation between PT and BPA by comparing the urinary BPA levels of PT girls with those of healthy subjects.
Materials and methods
Subjects
The current study was designed as a case-control study and approved by Akdeniz University’s ethical committee. It was conducted between September 2010 and February 2012 in the outpatient clinic of Pediatric Endocrinology, Akdeniz University. All of the subjects in both the control and study groups voluntarily participated in the study. A written consent was obtained from their parents.
Subjects recruited in the study were grouped as follows: Newly diagnosed girls with PT (n = 25) were recruited in the study. These girls were admitted to the outpatient clinic of Pediatric Endocrinology for their complaint of enlargement of breasts before the age of puberty. The inclusion criteria were: (a) PT is defined as isolated breast development in girls before the age of 8; (b) age: 4–8 years (patients younger than 4 years were not recruited in the study because of difficulty to obtain the urine samples and risk of contamination of the special bottles); (c) no advancement of bone age >1 year above the chronological age. The PT group was followed up regularly in the pediatric clinic for at least 12 months and showed breast development alone without other progression of puberty. Gonadotropin-releasing hormone stimulation test (Gonadorelin acetate, Ferring®) was performed on girls with the diagnosis of PT to exclude the central PP. The control group comprised of 25 completely healthy girls of comparable age with no history of PT and any other endocrine disorder and no secondary sexual characteristics in their physical exam. All girls in the control group had no history of any other chronic or acute pathological condition (i.e. diabetes, metabolic syndrome and/or obesity, hypertension, cancer, etc.). The control group was recalled 1 year later for evaluating pubertal development.
All controls and subjects with PT were born, still living in Antalya Province and were examined by the same pediatrician, who is a child endocrinologist with a background of both pediatrics and endocrinology. Clinical evaluations included measurement of height and body weight. The body mass index (BMI) of the study subjects were calculated and obesity was defined as BMI >95th percentile according to national standards. 27
The exclusion criteria for PT group were: Girls who were diagnosed with PP or who had a family history of PP, who were using estrogen containing pills or creams and who had benign non-progressive PT were not recruited. Obese patients and controls were excluded from the study. Pelvic ultrasonography (USG) findings were evaluated in all PT group girls to exclude organic lesions, such as ovarian cysts.
The exclusion criteria for control group were: Girls having pubertal signs (PT, PP, premature pubarche, etc.) at their second consultation were excluded from the study.
Spot urine samples from control group and subjects with diagnosis of PT were collected into deplasticized glass beakers. Samples were aliquoted in deplasticized glass bottles and kept at −20°C for 2 months. Extreme caution was taken in order not to contaminate the samples with plastic material. All the urine samples were transferred to Hacettepe University, Faculty of Pharmacy, and Department of Toxicology on dry ice for the determination of BPA levels. Analysis was performed in 1–2 months after receiving the samples.
Deplasticization of the glassware
In order to prevent the contact with plastic material, special attention was given throughout the present study. All the glasswares were deplasticized with a mixture of tetrahydrofuran and n-hexan (50:50, v/v) for 2 h and later dried. All the test tubes were deplasticized on a heater at 400°C for 4 h.
Chemicals and reagents
Chemicals were purchased from Sigma-Aldrich (St. Louis, Missouri, USA). Glucuronidase/aryl sulfatase enzyme (from Helix pomatia) was obtained from Roche (Mannheim, Germany). All high pressure liquid chromatography (HPLC) equipment were from Agilent (Santa Clara, California, USA).
Measurement of hormones
Serum estradiol levels were measured by electrochemiluminescence immunoassay using a commercial kit (Roche, Mannheim, Germany). The limit of detection (LOD) for estradiol was ≤5 pg/mL. Measuring range of the kit was 5–3000 pg/mL. Calibration was performed on two points. Quality control was used for each batch measurement. Recovery value was 99.1% ± 4.2%.
Serum free T4 (fT4) and thyroid-stimulating hormone (TSH) levels were measured by chemiluminescence microparticle immunoassay using DiaSorin Liaison chemiluminescence immunoassay (CLIA) kits (Stillwater, Minnesota, USA) on a DiaSorin Liaison CLIA Analyzer (Stillwater, Minnesota, USA). The LOD values were 0.29 ng/dL for fT4 and 0.02 mIU/L for TSH. Measuring range of fT4 and TSH kits were 0.29–7.7 ng/dL and 0.02–90 mIU/mL, respectively. Calibrations were performed on two points for both of the kits. Quality controls were used for each batch measurement for fT4 and TSH. Recovery values were 98.4% ± 3% for fT4 and 100% ± %1.1 for TSH.
Serum luteinizing hormone (LH) and follicle-stimulating hormone (FSH) in plasma were measured by enzyme-linked immunosorbent assay using commercial kits (Abcam, Cambridge, Massachusetts, USA). The LOD values were 1.4 mU/mL for FSH and 0.09 mU/mL for LH. Measuring range of FSH and LH kits were 2.5–300 mU/mL and 0.22–300 mIU/mL, respectively. A blank and seven standards (1.5, 2.5, 5, 15, 50, 100, and 200 mU/mL) were used to obtain a typical standard curve for FSH. A blank and seven standards (0.1, 1, 2, 2.5, 5, 25, 50, 100, and 200 mIU/mL) were used to obtain a typical standard curve for LH. Quality controls were used for each batch measurement for fT4 and TSH. Recovery values were 98.1 ± 3.00% for FSH and 97.00% ± 3.58% for LH.
Analysis of urinary BPA levels
Extraction of BPA from urine
The method of Yang et al. (2003) was used with some modifications for the analysis of urinary BPA. After spiking urine (500 μL) with BPA (5 ng/mL), sodium acetate buffer (200 M, pH 5) and glucuronidase/aryl sulfatase was added. The mixture was incubated for 3 h at 37°C to obtain free BPA. Later, HCl (2 N, 100 μL) and ethyl acetate (5 mL) were added and the mixture was centrifuged at 3000 r/min. The supernatant (2.5 mL) was then evaporated under nitrogen stream. Residues were kept at −20°C until analysis. 28
Chromatographic analysis
At the day of analysis, residues were dissolved in 60% acetonitrile (400 μL), and 100 μL of the dissolved residue was injected to HPLC (Hewlett-Packard Agilent 1100 series, Santa Clara, California, USA).
HPLC parameters were as follows: C18 column (25 cm × 5 μm × 4.6 mm i.d.); column temperature (25°C); fluorescence detector (λ exitation = 230 nm, λ emission = 315 nm).
Mobile phase was acetonitrile: tetrahydrofuran (2.5%). Gradient elution was used as 60:40–5:95. The flow rate of the mobile phase was 0.4 mL/min. The retention time was recorded to be between 18.3 and 19.2 min with an analysis duration of 40 min.
The LOD value was calculated according to the method of the United States Environmental Protection Agency (EPA) 29 and it was 0.5 ng/mL. The limit of quantitation was 1.25 ng/mL.
BPA standards used were 1.25, 2.5, 5, 10, 25, 50, and 100 ng/mL. The urinary BPA levels were calculated using the standards and the peak heights obtained from the chromatogram. After spiking urine samples with 5 ng/mL of BPA, recovery studies were performed. The average recoveries were found to be (mean ± standard deviation (SD)) 97.37 ± 1.23% on ten occasions. Between-run precision was 2.76 ± 0.24% and within-day precision was 2.63 ± 1.23%.
Urinary creatinine concentrations were analyzed simultaneously according to Jen et al. (2000) with slight modifications. The urinary BPA concentrations were adjusted by urinary creatinine concentrations. 30
Primary and secondary endpoints
The primary endpoint of this study was to compare the urinary BPA levels of PT patients and healthy controls. The secondary endpoints of the study were to compare the urinary BPA levels in girls with PT with regard to breast development, to determine the correlations between urinary BPA levels and pelvic USG findings and to correlate the urinary BPA levels and sex hormones in girls with PT.
Statistical analysis
Predictive Analytics SoftWare (PASW, Quarry Bay, HK) statistics release was used for statistical analysis. The distribution of BPA values was analyzed using the Shapiro–Wilk test. For the comparison of BPA levels in girls with PT with regard to breast development, Kruskal–Wallis test was used. The comparison between two parametric values was performed using Student’s t test and for nonparametric values Mann–Whitney U test was used. The correlations between urinary BPA levels and sex and thyroid hormones were determined using the Spearman’s ρ correlation test. p < 0.05 was accepted as significant. The results were given as mean ± SD. Besides, median (min–max) values were also shown.
Results
Subjects
The clinical characteristics of the patients with PT and the control group are shown in Table 1. There were no statistically significant differences between the ages and BMIs of the groups.
The age and BMI of control and PT groups.a

BMI: body mass index; PT: premature thelarche.
aResults are given as mean ± SD. p < 0.05 is considered as statistically significant. There were no significant differences between ages of control and PT groups. There were no marked differences between BMIs of control and PT groups.
Hormone levels
The reference range of estradiol levels from birth to 11 years is <20–53 pg/mL. In girls with PT, basal estradiol levels were 10.25 ± 6.58 pg/mL. 31
In healthy girls, the LH reference range from birth to 13 years is <1–3.3 IU/L. For girls with PT, we anticipated that basal LH levels should be close to zero and we found that basal LH levels were 0.11 ± 0.03 IU/L, as expected. The reference FSH levels for girls from birth to 8 years is <1–7.1 IU/L. Basal FSH levels in PT patients were 1.72 ± 0.79 IU/L. 31
Pediatric TSH levels from 1 month to 18 years of age are expected to be 0.46–5.8 mIU/L. TSH levels in PT patients were 2.34 ± 0.93 mIU/L. Pediatric fT4 levels from 1 year to 10 years of age are expected to be 0.46–5.8 mIU/L. 32 TSH levels in PT patients were 2.34 ± 0.93 mIU/L, while fT4 levels were 1.35 ± 0.15 ng/dL.
All hormone levels were in normal ranges in the healthy controls.
Urinary BPA levels
Urinary BPA levels were markedly higher in the PT group versus control (p = 0.02) [median: 3.21 (0.3–45.14) and 1.62 (0.3–25.79) μg/g creatinine (OR = 1.77, 95% confidence interval (CI): 1.03–3.04, p = 0.03)] (Figure 1).

Urinary BPA levels in PT and control groups. BPA: bisphenol A; PT: premature thelarche.
Median BPA levels in girls with PT with regard to breast development is given in Table 2. There were no differences in the urinary BPA levels of PT girls with pain and no pain in the breasts (3.21 vs. 3.64; p = 0.92). Besides, breast development timing did not affect BPA levels (p = 0.27). Moreover, there were no statistically significant differences between the urinary BPA levels of girls who had one-sided or two-sided breast development although girls with two-sided breast development had almost 30% more urinary BPA levels compared to girls who had one-sided breast development (3.15 vs. 4.45, p = 0.70).
Median BPA levels in girls with PT with regard to breast development.
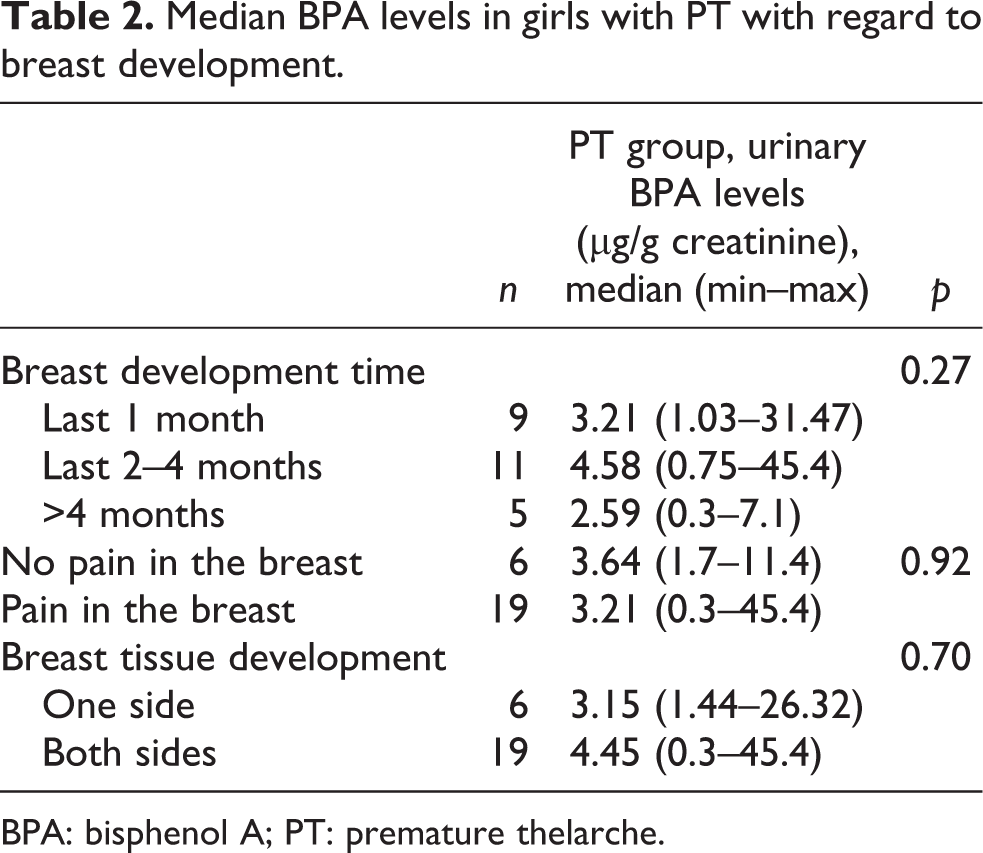
BPA: bisphenol A; PT: premature thelarche.
The correlations between urinary BPA levels and pelvic USG findings are given in Table 3. We observed a weak, insignificant positive correlation between the uterus volume and urinary BPA levels. The correlations between urinary BPA levels and hormones are shown in Table 4. We did not find any significant correlation between the urinary BPA levels of PT girls and the measured hormones. However, there was a weak correlation between estradiol and urinary BPA levels (r = 0.166; p = 0.37); and LH and urinary BPA levels (r = 0.291; p = 0.08) of PT girls.
The correlations between urinary BPA levels and pelvic USG findings in PT group.

BPA: bisphenol A; USG: ultrasonography; PT: premature thelarche; ρ: Pearson’s correlation coefficient.
The correlations between urinary BPA levels and hormones in PT group.
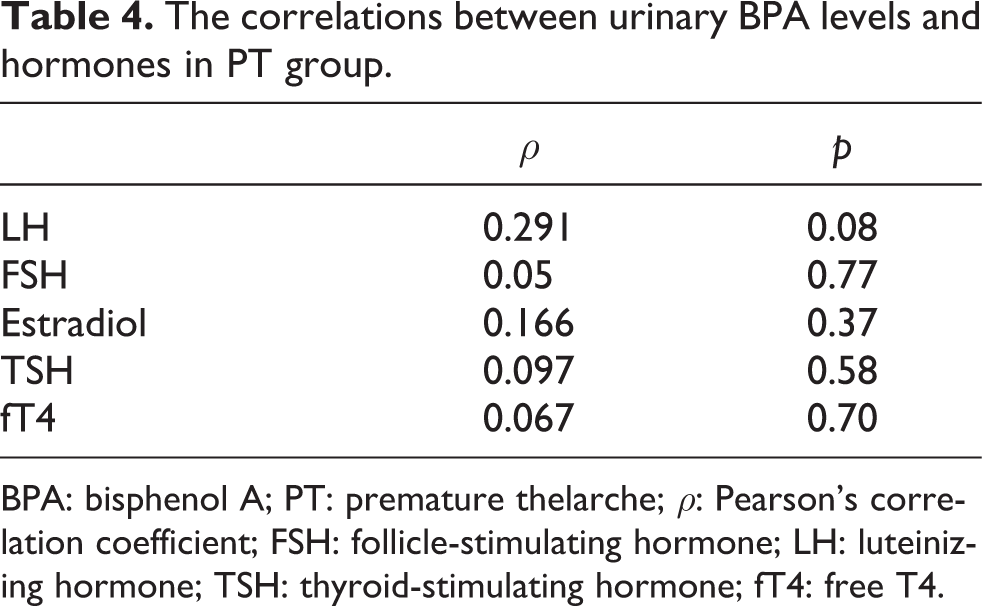
BPA: bisphenol A; PT: premature thelarche; ρ: Pearson’s correlation coefficient; FSH: follicle-stimulating hormone; LH: luteinizing hormone; TSH: thyroid-stimulating hormone; fT4: free T4.
Discussion
Throughout the globe, a secular trend toward an increasing prevalence of PT and PP is observed in girls aged between 4 years and 8 years. 33,34 There is limited available information for the reasons of high PT occurrence. Childhood exposures to EEDCs (present in plastics, food, pesticides, and baby products) were suggested to be one of the underlying factors for PT. 35 –38
BPA is an EEDC, used as the building block of polycarbonate plastics, which are present in reusable baby bottles and water bottles, and in the inner lining of food cans. 39 Particularly at high temperatures, this compound leaches into food and therefore, food consumption is suggested to be the primary exposure route. Lakind and Naiman (2011) showed that consumption of meals prepared outside home was associated with higher urinary BPA levels in school children. 40 Tzatzarakis et al. (2017) reported that approximately 41.7% of the canned solid food (33.4 ± 4.4 ng/g BPA), 25.0% of the canned liquid food (70 ± 0.08 ng/mL), and 43.8% of the soft drinks (2.30 ± 0.18 ng/mL) were positive for BPA. The results of this study showed that canned solid food contained higher levels of BPA compared to canned liquid food. 41
The current study is unique as it investigates the relationship between PT and urinary BPA levels in nonobese girls aged 4–8 years. We found that in PT group, urinary BPA levels were approximately two times higher compared to control group. In addition, we observed insignificant correlations between estradiol and urinary BPA levels along with an unmarked correlation between LH and urinary BPA levels in PT group. This correlation may perhaps be significant if we had more number of subjects with PT in this study. Chen et al. (2015) conducted a study on female infants (aged 4 months to 2 years, n = 251) with PT. The researchers observed that serum BPA concentrations of PT group were markedly higher than the healthy controls (3.48 ng/mL, 95% CI: 0.09–140.26 vs. 1.70 ng/mL, 95% CI: 0.06–51.78; p = 0.039). However, there was no correlation between age and serum BPA levels. 42 Leonardi et al. (2017) reviewed the results of different studies on BPA exposure and puberty and concluded that currently available data do not allow establishment of a clear role of BPA in pubertal development as there are conflicting results from all clinical and epidemiological studies. 43 Human exposure to different EDCs were suggested to exert different effects on both male and female reproductive systems. Besides, these chemicals may be related to different pathological conditions like endometriosis, breast cancer, testicular cancer, and polycystic ovary syndrome. 44 On the other hand, other EDCs like organophosphate and organochlorine pesticides were also found to be associated with different male reproductive system disorders, including hypospadias. 45
In humans, although urinary BPA levels have not been linked to PT before, we have observed that the urinary BPA levels were markedly higher in the idiopathic central PP (n = 26) group versus control (n = 21) [median 8.34 (0.84–67.35) μg/g creatinine and 1.62 (0.3–25.79) μg/g creatinine (OR = 8.68, 95% CI: 2.03–32.72, p = 0.001), respectively]. 46 Besides, serum BPA levels of Chinese PP patients showed positive correlation with the volume of the uterus, in accordance with our results, and volume of the ovary, and girls with PP were found to be more severely contaminated than controls. 47 However, in a recent study of our working group, we observed that urinary BPA levels were not statistically different between control, peripheral PP, and idiopathic central PP groups (medians: 10.91, 10.63, and 10.15 µg/g creatinine, respectively; p > 0.05). Buluş et al. (2016) suggested that their study group lived in Ankara and as Ankara is an industrialized city, the girls might be exposed to environmental chemicals more than girls living in Antalya (the city in which the study of Durmaz et al. was conducted), which is a sea-side city with more agricultural facilities. 48
In the present study, BPA concentrations of Turkish girls were comparable with other studies performed in the United States, Europe, and Asia. Besides, LOD levels (0.5 ng/mL = 0.5 μg/L in the current study) were also in the same range with other research. 49 –54 In US population, urinary BPA concentrations of children and adolescents were found to be higher when compared to adults. Two recent US government-sponsored reviews on BPA literature, conducted in 2007 and 2008, stated specific cautions should be given to exposure of fetuses, infants, and children. 55,56 Moreover, the Food and Drug Administration (FDA) indicated that it had “some concern” about the potential effects of BPA on fetuses, infants, and young children in January 2010. Since then, the organization supports reduced exposure of BPA in infants. The FDA states that this can be provided by the elimination of BPA from baby bottles/cups and by the development of new BPA-free alternatives for linings of infant food cans. 57
The mechanisms underlying the relationship between BPA and early breast development are not fully understood. In MCF-10F cells (human breast epithelial cells), BPA exposure for 2 weeks caused higher expression of genes involved in DNA repair (i.e. BRCA1, CtIP) and lower expression of genes involved in apoptosis (i.e. PDCD5, BCL2L11). The epigenetic changes caused by BPA in MCF-10F cells involve the hypermethylation and therefore the inhibition of BCL2L11 and the hypomethylation of CtIP gene which plays a role in the double strand brake repair. 58 On the other hand, perinatal exposure to BPA increased the adult mammary gland progesterone response and cell number in mice and it is indicated that BPA is the major proliferative stimulus in the adult mouse mammary gland. 59 Moreover, BPA, similar to certain estrogen metabolites, can react with DNA and can generate adducts that can produce a variety of DNA modifications that, if not countered by DNA repair, can lead to mammary cell growth and cell transformation. 60 –63
In animals, BPA does not follow a monotonic dose–response curve (“U” or inverted “U” shaped dose–response curve) and low doses can cause potentially harmful effects, varying at different stages of development. 64,65 Regulatory bodies in the United States and EU have concerns on safety of low-dose BPA exposure and the reference dose was defined as ≤5 mg/kg body weight (bw)/day, which is also the lowest dose used in standard toxicological tests. EPA calculated reference dose as 50 μg/kg bw/day. 66 In rodents, several studies were concerned that exposure to low doses of BPA may have developmental effects in various hormone-responsive organs, including the mammary gland and the same kind of effect might be valid for humans, with potential consequences for public health. 67 –69 In vivo studies showed that both early-life and adult-life exposure in rodents to BPA results in persistent alterations in mammary gland morphogenesis and increased susceptibility to tumorigenesis. 70,71 Maternal exposure to BPA during lactation decreased the time to first tumor latency in rats, and increased the number of 7,12-dimethylbenz[α]anthracene (DMBA) induced mammary tumors in their female offspring. 72
In Turkey, BPA is banned from baby bottles, nipples, and other polycarbonate baby products in July 2012 by a notification which was included in the Turkish Food Codex—baby formulas and baby follow-up formulas. 73 However, there are still cheap baby bottles, toys, or baby care products in the market containing BPA. On the other hand, throughout the globe, including Turkey, there is a trend toward consuming readily prepared, canned, or packaged food than homemade food, especially among children and adolescents. As the number of working mothers increase, it is inevitable that children are fed with fast food or microwave heated food. In a recent study performed on US infant formulas, the highest BPA concentrations were present in small cans of ready-to-feed formula and the lowest BPA levels were found in powder formula and small glass and polymeric containers of ready-to-feed formula. 74 This situation might be one of the underlying factors of increment of PT among girls. Parents should limit their children’s exposure to BPA by avoiding the use of polycarbonate plastics (specifically by avoiding putting hot beverages in plastics and bottles with polycarbonate origin). In addition, canned foods should be avoided for young children. Besides, mothers should be encouraged to breastfeed or use powdered formula.
In conclusion, further study is required to establish the role of childhood BPA exposure in early breast development. Given the short half-life of BPA and temporal variability of urinary BPA concentrations, a single spot urine sample may not correctly classify exposures; however, it may reflect the accustomed lifestyle and the customary exposure to such chemicals. Although our study has some limitations (i.e. few subject numbers), this might lead other researchers to design similar studies investigating a relationship between BPA and PT with high subject numbers.
Footnotes
Acknowledgements
The authors thank the patients and their families for their patience and consent.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Akdeniz University Scientific Research Unit (grant no. 2010.04.0103.26).