
Abstract
The incidence and clinical aspects of seizures remain to be elucidated in patients with acute pesticide intoxication. The present study included subjects who ingested pesticide with the intention of committing suicide and were treated at Soonchunhyang University Hospital (Cheonan, Korea) between January 2011 and December 2014. We analyzed the incidence and characterized the type and frequency of seizure, from the medical records of 464 patients with acute pesticide intoxication, according to the pesticide class. The effect of seizure on the clinical outcome was assessed. The incidence of seizure was 31.5% in patients who ingested glufosinate ammonium {2-amino-4-[hydroxyl (methyl) phosphinoyl] butyrate; ammonium DL-homoalanin-4-yl (methyl) phosphinate}, followed by those who ingested pyrethroid (5.9%) or glycine derivatives (5.4%). All of the seizures developed between 12 and 24 h of pesticide ingestion and had ceased by 72 h after seizure initiation, following treatment with antiseizure medication. Generalized tonic–clonic seizures were the most commonly observed (85.7% of the cases). Multivariable logistic regression analysis showed that the effect of seizure on mortality was not statistically significant. In conclusion, glufosinate ammonium herbicide is the most common seizurogenic pesticide class. Seizure itself was not a risk factor for mortality in patients with acute glufosinate ammonium intoxication.
Introduction
Glufosinate is a phosphorus-containing amino acid that occurs naturally as a component of bacteria-derived bactericidal and fungicidal tripeptides. 1 The ammonium salt of glufosinate is a broad-spectrum herbicide that is used worldwide. 2 This compound acts by inhibiting plant glutamine synthetase, causing accumulation of ammonium ions and inhibition of photosynthesis. 3 Although glufosinate ammonium herbicides are considered safe when used properly, 4 many clinical toxicologists have reported that the ingestion of a large amount of glufosinate ammonium can cause convulsions. 5 –8
From a neurophysiological viewpoint, glutamate is an important seizurogenic chemical in
mammals, because the intracellular Ca2+ concentration increases sharply and
neurons become depolarized when glutamate binds to its receptors.
9
Glufosinate and glutamate have similar chemical structures: glufosinate has a
chemical formula of C5H12NO4P and a molar mass of 181.13 g,
while glutamate (2-aminopentanedioic acid) has a chemical formula of
C5H9NO4 and a molar mass of 147.13 g. Based on this
information, researchers have investigated whether glufosinate can activate neuronal
glutamate receptors. One of the most outstanding studies in this field was reported by Lantz
et al..
10
Based on the results of an elegantly designed experiment, they concluded that
glufosinate bound the N-methyl-
Meanwhile, clinical toxicologists have indicated that seizures are not infrequent in patients intoxicated with other classes of pesticide. 12,13 This suggests that other pesticides may also be seizurogenic chemicals. In reality, many insecticides are neurotoxic and various target sites have been described; these include voltage-gated sodium channels for pyrethroids; 14 γ-aminobutyric acid type A receptors for cyclodienes; 15 neuronal nicotinic acetylcholine receptors for nicotine 16 and imidacloprid [(E)-1-(6-chloro-3-pyridylmethyl)-N-nitroimidazolidin-2-ylideneamine] 17 ; and acetylcholinesterase for organophosphate and carbamate insecticides. 18 Seizures can cause subsequent seizure activity. 19 Therefore, seizures occurring after pesticide intoxication should be treated properly. However, the incidence and clinical characteristics of seizures remain to be elucidated in patients with acute pesticide intoxication. In the present study, we investigated seizure incidence and effect on the clinical outcome of pesticide-intoxicated patients.
Materials and methods
Patients
This study was approved by the institutional review board (IRB) of Soonchunhyang University Hospital Cheonan (IRB No. 2013-12-010). The requirement for informed consent was waived by the IRB.
Four hundred and sixty-four patients (male: 289, age 59.1 ± 15.2 years; female: 175, age 59.6 ± 16.1 years) were included in this study. Each patient ingested more than one mouthful of pesticide with the intention of committing suicide and was treated at the Institute of Pesticide Poisoning at Soonchunhyang University Hospital Cheonan between January 2011 and December 2014. Patients were excluded from the study if they had ingested less than one mouthful of pesticide, if they had ingested an unidentified pesticide, if they had preexisting brain damage, or were taking anticonvulsive medication.
Information about symptoms, routine laboratory findings, clinical outcomes, underlying disease, and the ingested pesticide (class of pesticide, ingested volume, time between ingestion, and hospital admission) were derived retrospectively from the medical records. The pesticide type was confirmed by inspecting the pesticide bottle that was presented by the individual accompanying the patient.
Upon admission, patients received standardized medical emergency treatment, including hydration and oxygen supply as indicated. Gastric lavage was performed if the patients arrived within 2 h after pesticide ingestion. Blood samples for arterial blood gas analysis, electrolytes, and blood chemistry were drawn in the emergency room.
Pesticides were subdivided into the classes published by the respective Resistance Action Committee; these Specialist Technical Groups of CropLife International were indicated by HRAC for herbicides, IRAC for insecticides, FRAC for fungicides, and RRAC for rodenticides. The common name of the pesticide was used, as determined by Technical Committee 81 of the International Organization for Standardization (ISO/TC81). The amount of pesticide ingested was calculated using the number of mouthfuls (1 mouthful = 20 mL), as stated by the patient, or calculated from the remaining amount in the pesticide bottle.
Clinical outcomes
The parameters used to assess clinical outcome included the death rate, length of hospital stay (days), length of intensive care unit (ICU) stay (days), and the seriousness of the toxic symptoms. The seriousness of the toxic symptoms was evaluated using the Workload Management System for Critical Care Nurses (WMSCN) 20 and Acute Physiology and Chronic Health Evaluation II (APACHE II) scores. 21 According to the workload of the ICU nurse, the seriousness of the toxic symptoms was either WMSCN Class 1 (patient able to care for themselves, minimal degree of nursing care required), Class 2 (moderate degree of nursing care required), Class 3 (acute degree of nursing required), Class 4 (intensive degree of nursing required), Class 5 (continual nursing required), or Class 6 (intensive nursing from two or more nurses required). The APACHE II score was calculated using the patient’s age and the following 12 routine physiological measurements: PaO2, body temperature, blood pressure, arterial pH, heart rate, respiratory rate, serum Na+ and K+, creatinine, hematocrit, white blood cell count, and Glasgow Coma Scale score. These measurements were taken during the first 24 h after admission.
Seizure characteristics
Since January 2011, every patient with a convulsive disorder at our institute of pesticide poisoning has been referred to a neurologist. This neurologist classified the seizures with respect to their frequency and type. Seizure frequency was classified as a single seizure, seizure cluster, status epilepticus, or nonconvulsive status epilepticus, while seizure type was classified as focal, generalized tonic–clonic, mental change, myoclonic, or tonic. Electroencephalography (EEG) was obtained from all of the seizure patients, with a time lag between the final seizure and the EEG of between 2 and 12 h. Taken together, the above findings were used to categorize the seizure as an acute symptomatic seizure, an epileptic seizure, or epilepsy.
Comparison of parameters between the seizure and nonseizure groups
The following parameters were compared between the seizure group and nonseizure group: age, volume of pesticide ingested, time lag between ingestion and arrival at the hospital, clinical outcome parameters, grade of toxic symptoms, and laboratory values, including the complete blood count, blood chemistry, electrolytes, and arterial blood gas analysis.
Death rate (%) was calculated according to the following equation:

For the parameters that were significantly different between the two groups, univariate and multivariate logistic regression analyses of the risk factors for a poor clinical outcome (death) were performed.
Analysis of the significance of seizure as a risk factor for mortality
The number of patients who had ingested paraquat dichloride (1,1′-dimethyl-4, 4′-bipyridinediium dichloride; 1,1′-dimethyl-4-4′-bipyridinium dichloride; 1,1′-dimethyl-4,4′-bipyridylium dichloride) was greater in the nonseizure group than in the seizure group. Although the number of deaths was too small to attempt statistical analysis within each pesticide class category, this was possible for the glufosinate ammonium category. To adjust for these confounding effects, we only assessed the significance of seizure as a risk factor for mortality in the patients who ingested glufosinate ammonium.
Statistical analysis
All demographic data are presented as the mean ± standard deviation, unless otherwise noted. A comparison of the parameters between the seizure and nonseizure groups was performed using parametric or nonparametric methods, according to the data distribution. Student’s t-test was used in univariate analyses to analyze differences between the two groups, and the χ 2 test was used to compare the categorical variables. Multivariable logistic regression analysis was used to assess the relationship between pesticide class and seizure development and to assess the relationship between seizure episode and mortality, while adjusting for age, time delay between ingestion and hospitalization, ingested volume, and other risk factors. All variables with a p value <0.05 in univariate analyses were considered statistically significant, and they were used for multiple logistic regression analysis. All data were analyzed using R (The R Foundation for Statistical Computing, Vienna, Austria) version 3.1.2 or SPSS (SPSS, Inc., Chicago, IL, USA) version 17.0 for Windows.
Results
Recruitment/patient number
Pesticides were classified into six classes as follows: glyphosate (glycine derivatives, n = 130), paraquat (n = 94), glufosinate ammonium (n = 73), organophosphate (n = 54), pyrethroid (n = 34), and others (n = 79). This latter class included various other pesticides, each of which was ingested by a small number of patients.
Comparison of the seizure and nonseizure group demographics
There was no difference in gender distribution between the seizure and nonseizure groups (male/female = 269/160 for the nonseizure group and 20/15 for the seizure group, p = 0.514). Age (p = 0.007) and admission period in both ICU and general ward (p < 0.001) were greater in the seizure group than in the nonseizure group, whereas ingested volume was greater in the nonseizure group than in the seizure group (p = 0.002; Table 1).
Comparison of seizure group and nonseizure group parameters.
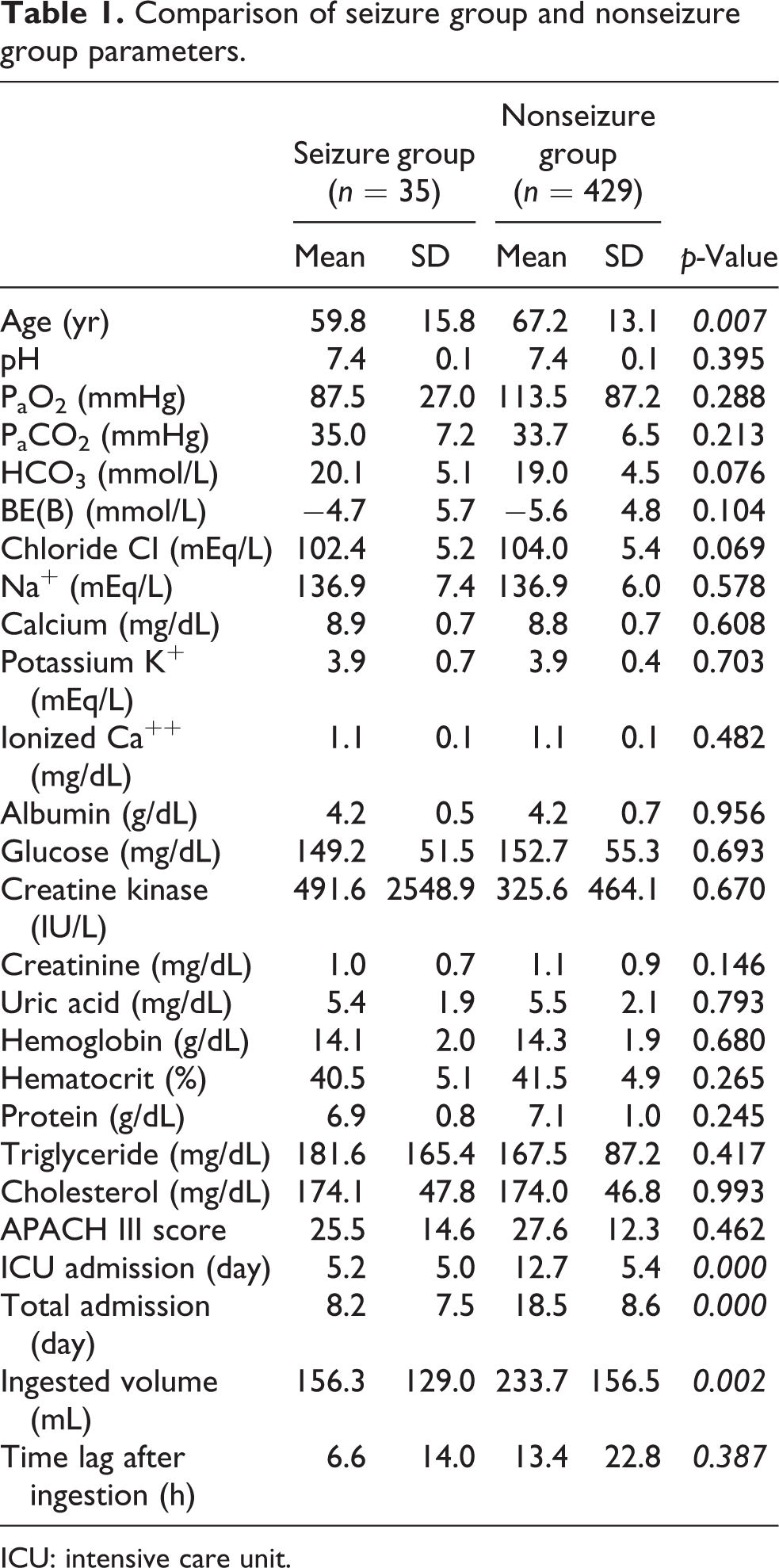
ICU: intensive care unit.
Incidence of seizure within each pesticide class
As shown in Figure 1, the incidence of seizure was significantly higher in the glufosinate ammonium class (31.5%; 23/73 patients), as compared to the other classes of pesticide: 5.9% (2/34 patients) for pyrethroid, 5.4% (7/130 patients) for glyphosate, 1.1% (1/94 patients) for paraquat, and 2.5% (2/79 patients) for the other pesticide class. No seizures were observed in the organophosphate class (0/54 patients). Multivariable logistic regression analysis showed that ingestion of glufosinate ammonium was a significant risk factor for seizure (p < 0.001). Age (p = 0.032), ICU admission period (p < 0.001), and the time interval between ingestion and arrival at hospital (p = 0.024) were also significant risk factors for seizure development.

Incidence of seizure, according to the pesticide class. The incidence of seizure is shown for patients who had ingested the indicated type of pesticide. Note that the incidence of seizure was significantly higher in the patients who ingested glufosinate ammonium (p < 0.001, χ 2 test).
Seizure characteristics
The present analysis of seizure frequency indicated that the majority of patients with seizure (26 cases, 74.3%) showed a seizure cluster, followed by those showing a single seizure (5 cases, 14.3%), nonconvulsive status epilepticus (3 cases, 8.6%), and convulsive status epilepticus (1 case, 2.9%). All of the seizures developed between 12 and 24 h after undiluted pesticide ingestion. Seizure type classification showed a generalized tonic–clonic type in 30 cases (85.7%), followed by 2 cases (5.7%) of focal seizure type, and 1 case each of mental change, myoclonic, and tonic type (2.9% for each category). Following the administration of an antiseizure medication, such as diazepam and diphenylhydantoin, all of the seizures had ceased by 72 h after seizure initiation. EEG findings, obtained 2- to 12-h post-seizure, showed diffuse slowing waves in 16 cases (45.7%), epileptiform discharge in 14 cases (40.0%), normal findings in 4 cases (11.4%), and focal slowing in 1 case (2.9%). These findings indicated that 32 cases (91.4%) showed acute symptomatic seizure and 3 cases (8.6%) showed epileptic seizure or epilepsy.
Comparison of death rates in the seizure and nonseizure groups
The overall death rate was 21.6% (100/464 patients). The death rate was lower in the seizure group (2.9%; 1/35 patients) than in the nonseizure group (23.1%; 99/429 patients) (p = 0.005). However, after adjusting for other risk factors, univariate and multiple logistic regression analyses showed that the effect of seizure on mortality was not statistically significant (Table 2).
Analysis of the risk factors for seizure.

OR: odds ratio; ICU: intensive care unit.
aInclude all of the classes except glufosinate ammonium class.
The significance of seizure as a risk factor for mortality in glufosinate ammonium ingested patients
Only one patient died in the seizure group, and the interval between pesticide ingestion and death was 15 days. On the other hand, 99 patients died in the nonseizure group, and the average interval between pesticide ingestion and death (mean ± SD) was 4.7 ± 0.6 days, (interquartile range: min, 25%; median, 75%; and max = 1, 2, 3, 5, and 48 days). Multivariable logistic regression analysis adjusted for ingested volume found that the effect of seizure on mortality was not statistically significant (p = 0.316).
Discussion
The present study made the notable finding that there was a higher incidence of seizure in the patients who had ingested glufosinate ammonium, as compared with patients who ingested other classes of pesticide (Figure 1 and Table 2). The majority of the seizures (85.7%) were of the generalized tonic–clonic type and occurred as a seizure cluster (74.3%). It was also notable that none of the patients who ingested organophosphates suffered seizures. However, the presence of seizure does not provide an indication of the severity of neuronal damage. In our clinical experience, organophosphate intoxication is more likely to result in unconsciousness or coma, as compared with intoxication by other pesticide classes (data not presented in this article). Further study will be required to compile all of the neurologic manifestations of acute pesticide intoxication.
The mechanism underlying the seizure observed following pesticide intoxication is beyond the scope of the current study. The results of a previous report 10 indicate that the seizurogenic activity of glufosinate is likely to be the cause of the high incidence of seizure in patients who ingested glufosinate ammonium. However, our current observation of seizures following the ingestion of other classes of pesticide, including pyrethroid and glycine, implies that other ingredients in the pesticide formulation may be seizurogenic.
In general, the additives in pesticide formulations include an emulsifier (surfactant), a stabilizer, a coloring agent, a pH regulator, an antifoaming agent, and supplements. During the past decade, we 22,23 and other investigators 24,25 have reported that surfactants in herbicides are more cytotoxic toward a neuronal cell line than the chief ingredient. The formulation of glufosinate ammonium herbicides may differ between manufacturers. In Korea, the level of glufosinate ammonium accounts for less than 20% of the commercial product, which contains about 30% surfactant (note that the exact details of the formulation are not disclosed by the manufacturers). Thus, we propose that surfactants in glufosinate ammonium herbicide formulations such as “alcohol, ethoxylated mono ether with sulfuric acid, sodium salts” may be partly responsible for the neurologic manifestations of this herbicide. Further study is necessary to test this hypothesis.
The current study had some limitations. Firstly, consciousness levels were assessed using the Glasgow Coma Scale score, but these may not be completely correct because a tracheal tube was inserted (with or without mechanical ventilation) in many patients. This makes verbal communication impossible. Furthermore, because each patient had ingested undiluted pesticide to commit suicide, many patients showed irritability and were thus treated with a sedative or tranquilizer to suppress their mental status. The long time-delay between the seizure and EEG measurement in some cases represented a further limitation of this study.
In conclusion, the incidence of seizure was highest in patients who ingested glufosinate ammonium, followed by patients who ingested pyrethroid or glycine derivatives. In most cases, seizures developed between 12 and 24 h of pesticide ingestion and had ceased by 72 h after the initiation of seizure. The average ingested volume of pesticide was 156.3 ± 129.0 mL in the seizure group, and generalized tonic–clonic seizures were the most common. The presence of seizure was not a risk factor for mortality in patients with glufosinate ammonium intoxication.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Cooperative Research Program for Agriculture Science & Technology Development (project no. PJ01083201), Rural Development Administration, Republic of Korea.