
Abstract
The aim of this study was to assess changes in bone mineral density (BMD) and cadmium (Cd) levels in blood and urine in individuals living in a Cd-contaminated area according to the type of osteoporosis medication over a three-year period. This follow-up study included 204 residents living in the vicinity of a closed copper refinery, who had been found to have elevated urinary or blood Cd levels. Cd levels in the blood and urine, as well as BMD, were measured every 6 months. After the first BMD measurement, individuals were prescribed antiresorptives such as alendronate or vitamin D and calcium, according to their BMD. Subjects were classified according to the type of medicine provided over the previous 6 months. General linear models controlling for other factors were used to evaluate the effects of each type of medication on the participants’ Cd levels and BMD. Spinal BMD showed a significant increase in the antiresorptive group compared to the nontreatment group. Significant decreases in blood Cd levels were found in the vitamin D and calcium group, in comparison to the nontreatment group, as well as a marginally significant decrease in the antiresorptive group. The vitamin D and calcium group showed a significantly greater decrease in urinary Cd levels than the nontreatment group. In contrast, antiresorptive medication was found to have a negative effect on urinary Cd excretion. These results suggest that vitamin D and calcium treatment for osteoporosis lowers blood Cd levels more effectively and improves urinary Cd excretion.
Introduction
Cadmium (Cd) is a widely distributed metal that is an airborne contaminant in the ambient environment and workplaces as well as in various food, water, and tobacco. 1 Intake of contaminated food is an important route of excessive Cd exposure in Koreans. 2 Cd has a long biological half-life and can induce nephrotoxicity and bone damage. 3
The mechanisms of the toxic effects of Cd on bone are not completely understood, but two possible explanations have been suggested. One hypothesis is that Cd acts directly on bone through the stimulation of osteoclasts and interference with collagen production in bone. 4 The other is that Cd primarily induces renal dysfunction, which is followed by secondary bone damage. 5,6 Cd can increase the urinary excretion of calcium and phosphorus, reduce the generation of active vitamin D [1,25(OH)2 D] in the kidneys, and reduce calcium uptake and reabsorption in the gastrointestinal tract. 3,4 Consequently, exposure to Cd causes bone demineralization and an increased risk of osteoporosis and bone fractures. 3,5,7
Various treatment options are available for osteoporosis, and usually the choice of medication depends on the bone mineral density (BMD). 8 Generally, pharmacologic agents such as bisphosphonates, calcitonin, estrogen, and parathyroid hormone are recommended to individuals, whose T-scores at the hip or lumbar spine are −2.5 or less. 8 For the prevention of bone loss and the treatment of osteopenia, with a T-score between −2.5 and −1.0, calcium and vitamin D supplementation has been recommended, especially in elderly individuals. 9
Our previous studies reported that residents living near an abandoned copper refinery were exposed to various heavy metals, especially Cd, and that temporal changes of Cd levels in the urine were significantly associated with renal tubular damage and osteoporosis. 10,11 Many studies have reported an association between exposure to Cd and adverse effects on bone in subjects living in Cd-contaminated area. 6,7,12,13 It has also been reported that antiresorptive medications for osteoporosis may inhibit the release of some toxic metals, such as lead. 14 Madeddu et al. reported that dietary calcium intake was inversely associated with blood Cd levels in women. 15 However, few studies have evaluated the effects of medications for Cd-induced bone loss on Cd levels within the body.
The aim of this study was to assess temporal changes in BMD and blood and urinary Cd levels, according to the type of medication prescribed for reduced BMD over a 3-year period in individuals living in a Cd-contaminated area.
Materials and methods
Study subjects
The study design and the method used to select the study population were described in detail in previous studies. 10,11,13 The baseline study was conducted among 572 subjects from May to August 2008, and a total of 307 subjects were enrolled in this follow-up survey until March 2011. All subjects agreed to participate in this 6-month-interval follow-up survey. Among the 307 subjects, 166 individuals showed a high Cd level (blood Cd > 4 µg/L and/or urinary Cd > 4 µg/g creatinine) and 141 subjects had a marginally high Cd level (2–4 µg/L or µg/g creatinine) and an abnormal renal tubular damage index (urinary β2-microglobulin > 300 µg/g creatinine or urinary N-acetyl-β-D-glucosaminidase activity > 11.5 U/L) or a marginally high Cd level and a low BMD (T-score < −2.5). Until November 2013, the blood and/or urinary Cd levels and BMD of 204 subjects were measured during follow-up, at least once after the baseline survey. After written informed consent was obtained from all subjects at baseline and at each follow-up, a trained interviewer collected information on each subject’s demographic characteristics, smoking habits, alcohol consumption, occupation, duration of residence, and past medical history. In addition, we also investigated dietary habits and the consumption of crops produced locally. Local crop products include rice, which is the staple food of Koreans, and a variety of cereals, such as barley, millet, and corn. Whole blood and spot urine were collected from all subjects and stored at −80°C until the Cd analysis was carried out. The study protocol was approved by the Institutional Review Board of Chungbuk National University (CBNU-IRB-2011-BQ02).
Determination of Cd in blood and urine
Concentrations of Cd in blood and urine were determined using a flameless atomic absorption spectrophotometer equipped with a Zeeman graphite furnace (Model Z-8270, Hitachi, Tokyo, Japan). Briefly, blood or urine was added to nitric acid and diluted with di-ammonium hydrogen phosphate and 1% Triton X-100, followed by vigorous mixing. The detection limits were 0.02 µg/L for blood Cd and 0.01 µg/L for urinary Cd, and all measured values for 204 subjects were higher than the detection limits.
Measurement of BMD and osteoporosis diagnosis
BMD was measured at the hip and lumbar spine using dual-energy X-ray absorptiometry. The T-score was estimated from the lowest measured BMD value. Osteoporosis was diagnosed when the T-score was 2.5 or less, and osteopenia when the value was between −1.0 and −2.5. 16 Subjects diagnosed with osteoporosis were prescribed an antiresorptive and those with osteopenia were provided calcium and vitamin D supplements (Dicamax 1000, Dalim Biotech, Seoul, Korea) for 6 months. 17 After 6 months of treatment, BMD was measured again and the corresponding medications were prescribed.
Statistical analysis
The concentration of Cd in blood and urine was log-transformed for statistical analyses as this parameter fits a log-normal distribution. Changes in the lumbar spine, BMD and Cd concentration in blood and urine was calculated as the difference throughout the last follow-up interval. On graphical inspection, changes of Cd in blood and urine and that of BMD approximately fit a normal distribution. Subjects were classified into three groups (no treatment, vitamin D and calcium, and antiresorptive).
According to the type of medicine provided during the last 6 months of the follow-up period. Comparison of the mean changes in the lumbar spine BMD and Cd concentrations in blood and urine according to the medication type was tested using analysis of variance, and if significant, Duncan’s multiple comparison test was performed. Multiple regression analyses were carried out to determine the effect of osteoporosis medication on changes of BMD and Cd levels in the blood and urine. The level of statistical significance was set at p < 0.05. All statistical analyses were performed using IBM SPSS version 21 (IBM Corp., Armonk, New York, USA).
Results
A total of 204 subjects participated in the follow-up survey from 2011 to 2013, with 133 (65.2%) participating in 2010, 196 (96.1%) in 2012, and 170 (83.3%) in 2013.
Table 1 shows the general characteristics of the participants at baseline: 55 of the participants were men and 149 were women. The mean age at baseline was 66.22 years old. The geometric mean (GM) of blood Cd levels was 4.09 μg/L and the GM of urine Cd concentrations was 5.00 μg/g creatinine. A significant difference was found in urine Cd and spinal BMD at baseline according to sex (Table 1).
Baseline characteristics of the study subjects.

SD: standard deviation; GM: geometric mean; GSD: geometric standard deviation.
aThe p-values were obtained using the t-test or the χ2 test to evaluate differences between men and women.
Spinal BMD showed a significant increase in the antiresorptive group in comparison to the nontreatment group. Although this trend was observed in both sexes, it was only statistically significant in women. Decreases in blood Cd levels were statistically significant in the vitamin D and calcium group in comparison to the nontreatment group and marginally significant in the antiresorptive group. The vitamin D and calcium group showed significant reductions in urinary Cd levels in comparison to the nontreatment group. In contrast, antiresorptive medications exerted a negative effect on urinary Cd excretion (Figure 1).

Change in lumbar spine bone mineral density (a) and blood (b) and urinary (c) Cd concentrations according to the type of osteoporosis medication. † p < 0.1, *p < 0.05, and **p < 0.01, compared with the nontreatment group. Error bars indicate standard deviation. Cd: cadmium.
We conducted a multivariate regression analysis to assess the factors influencing changes in BMD. We found that the intake of antiresorptives was closely related to increases in BMD (p = 0.015). This effect was only found in women. The intake of vitamin D and calcium supplements did not result in any significant difference in BMD compared to the nontreatment group (Table 2).
General linear models for changes in bone mineral density.

SE: standard error.
In all subjects, consumption of vitamin D and calcium supplements was significantly associated with a decrease in blood Cd (β = −0.240, p = 0.002). However, in men, diabetes was significantly related with elevated blood Cd (β = 0.347, p = 0.006; Table 3). In all subjects, consumption of vitamin D and calcium supplements was significantly linked to decreased levels of Cd in urine (β = −0.385, p = 0.045). When stratified by sex, this trend was only found in women (β =− 0.500, p = 0.025; Table 4).
General linear models for changes in blood cadmium levels.

SE: standard error.
General linear models for changes in urinary cadmium levels.
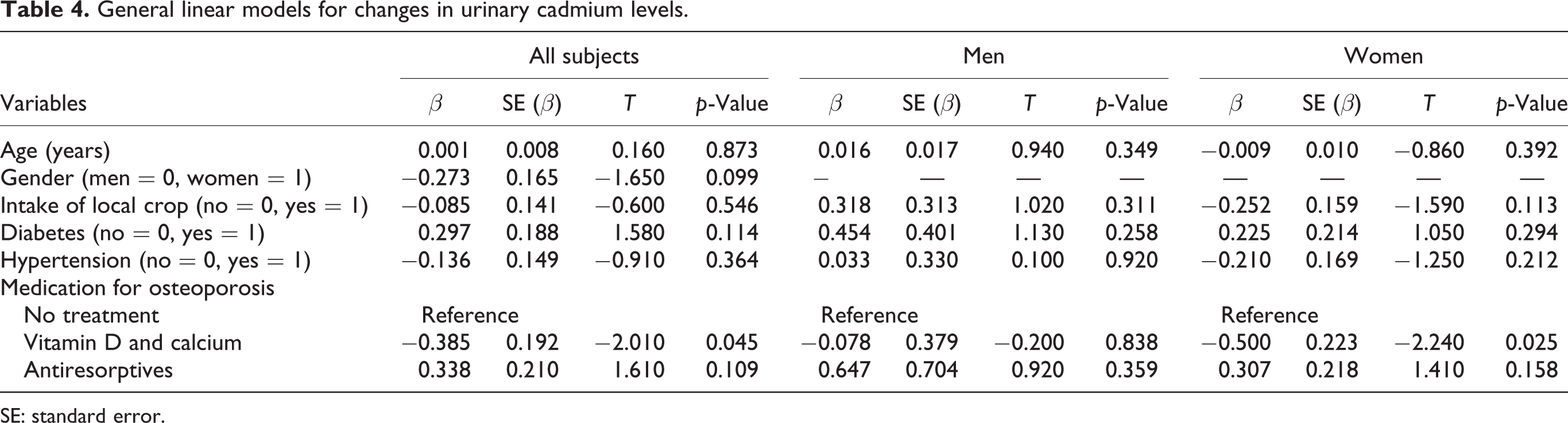
SE: standard error.
Discussion
In this observational follow-up study, we examined the effect of the consumption of calcium and vitamin D or antiresorptives on BMD and Cd levels in residents living in a Cd-polluted area. We found that consumption of calcium and vitamin D supplements to improve BMD was significantly effective in decreasing the Cd body burden in women, living in this Cd-contaminated area. Similarly, Madeddu et al. reported an inverse association between calcium intake and blood Cd in women. 15 Moreover, Kang et al. likewise observed a significant inverse association between the consumption of milk, a major source of calcium and blood Cd, in their study of a Korean population. 18
Food is the main environmental source of Cd. Approximately 5% of the Cd ingested through the digestive tract is absorbed in the body. It has been reported that the levels of minerals such as calcium, zinc, and iron in the body play an important role in the absorption rate of Cd. 1,19 –22 Calcium, in particular, can competitively interact with Cd, due to its similar chemical characteristics and ionic radius. Additionally, several studies have reported that Cd enters cells via the calcium transport system. 19,23,24 Therefore, consumption of calcium and vitamin D supplements, which improve the absorption of calcium, may reduce the uptake of Cd in the body. Moreover, such an effect would be more pronounced in those who have a calcium deficiency.
In this study, a statistically significant tendency for calcium and vitamin D supplements to reduce the Cd body burden was only observed in women. Analyses of the Korea National Health and Nutrition Examination Survey have shown that calcium consumption and serum 25-hydroxy vitamin D levels were significantly higher in men and that women were twice as likely to have a vitamin D deficiency as men. 25,26 Notably, in post-menopausal women, female hormones decline drastically, which leads to a lower uptake of calcium in the intestine, elevated urinary excretion of calcium, and decreased secretion of parathyroid hormone. 27 Most of the female subjects of this study were post-menopausal, which suggests that most of them may have experienced calcium and vitamin D deficiencies. In this study, the Cd-lowering effect of calcium and vitamin D was not significant in men. This is speculated to be due to the fact that female subjects—many of whom had decreased calcium and vitamin D levels—were more likely to have taken supplements to increase their calcium and vitamin D levels, thereby reducing their absorption of Cd. In contrast, male subjects may not have suffered equally significant deficiencies of calcium and vitamin D.
Smoking is one of the sources of Cd exposure in the general population, 1 but in this study, we did not observe a significant association between changes in Cd levels and smoking status. The reason for this phenomenon is that the study population has been living in Cd-contaminated areas and exposed to high concentrations of Cd in the environment for a long time. Similarly, Uetani et al. also reported that smoking does not influence the blood and urine Cd concentrations of people living in Cd-contaminated areas. 28 In the present study, a total of 55 subjects (27%) were smokers, and most of them were males (46 subjects, 84%). Since smoking status and sex were closely related to each other, if these variables were included in the linear model at the same time, a multicollinearity problem would have occurred. For this reason, the parameter of smoking was not included in the final multivariate model.
Osteoporosis refers to a condition in which an imbalance exists between bone resorption and bone formation; in particular, more bone resorption occurs than bone formation, leading to drastic bone loss. 27 The participants of the present study who were diagnosed with osteoporosis were mostly prescribed bisphosphonates, the most common antiresorptive agents. Bisphosphonates inhibit bone resorption by weakening the functions of osteoclasts and reinforcing the affinity between bone and calcium. 8 In this study, the therapeutic effect of antiresorptives for osteoporosis was demonstrated to be statistically significant in women only, consistent with prior studies. 29
In this study, urinary Cd concentrations were negatively correlated with BMD values (r = −0.149, p < 0.001), but the degree of the changes in urinary and blood Cd levels was not associated with the changes in BMD. When the change in Cd levels was included into the linear model, the significance of this model disappeared (data not shown). These results suggest that short-term changes in the body burden of Cd do not directly affect the changes in BMD and a decrease in the body burden of Cd is not directly involved in the improvement of BMD by anti-osteoporosis drugs such as antiresorptives.
This is the first study to verify that the intake of calcium and vitamin D supplements can help maintain BMD and reduce the Cd body burden in a population that is chronically exposed to environmental Cd. Those who live in a Cd-contaminated area are at a high risk of a wide range of adverse effects, such as kidney damage and decreased BMD due to chronic exposure to Cd. However, to date, few studies have addressed the treatment of chronic environmental Cd toxicity.
Chelators such as ethylenediaminetetraacetic acid are used to treat acute Cd toxicity. 30 Nonetheless, for chronic exposure to Cd (as in the case of residents of Cd-polluted areas), chelation therapy is not desirable. 31 That is because the chelators used in such treatments bind not only to heavy metals but also to essential minerals such as calcium, iron, copper, zinc, and magnesium, such that these substances are also excreted. 31,32 Therefore, calcium and vitamin D supplements—which do not have adverse effects when taken in moderate amounts—are recommended for the treatment and prevention of the adverse health effects of Cd toxicity on residents in Cd-polluted areas.
In conclusion, vitamin D and calcium treatment for osteoporosis reduces blood Cd levels more effectively than antiresorptives and improves urinary Cd excretion. Antiresorptive medicines effectively increase BMD but do not improve urinary Cd excretion.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the research grant of Chungbuk National University in 2014.