
Abstract
In the past 10 years, “designer drugs” such as synthetic cannabinoids and cathinones have emerged and come into widespread use, resulting in more overdose cases involving these new drugs in the United States. Emergency departments regularly treat a diverse array of drug intoxications, and providers must be cognizant of novel drugs of abuse and the associated clinical presentations in order to provide the most appropriate care. This review aims to describe the epidemiology, mechanism of action, clinical presentation, and treatment of intoxication for both the common and newest drugs of abuse.
Background
Emergency physicians are exposed to designer drugs and their complications on a daily basis in both the acute and critical care settings. In a study by Lank et al., 80% of physicians completed a survey stating they were not prepared to care for a patient with synthetic cannabinoids exposure in 2010. 1 There were 2500 calls made to US poison control centers pertaining to synthetic cannabinoid exposures from January 1, 2016, to November 30, 2016. 2 Fattore and Fratta reported identification of more than 140 synthetic cannabinoids and the European Monitoring Center for Drugs and Drug Addiction reported over 160 synthetic cannabinoids in 2016. 3,4
The emergence of new designer drugs has been of particular interest to both the United States and the international community. 5 These drugs are synthesized as chemical analogs to preexisting psychoactive or analgesic molecules, but are often disguised in household items and labeled “not for human consumption” to subvert and bypass regulatory agencies. The most popular products of this new group include synthetic cannabinoids (K2, Spice), synthetic cathinones (bath salts), and nontraditional opioid analogs. 5 Emergency department (ED) providers are often the first line in stabilizing and treating acute drug intoxication. Therefore, provider familiarity with emerging drugs of abuse, their clinical manifestations, and treatment is critical for optimal patient care.
The increase in ED visits for overdose of any type has the potential to increase resource utilization, ED crowding, and healthcare costs. In addition, there has been controversy regarding the ED’s lack of substance abuse intervention and treatment programs; however, this is often due to limited resources in the setting of large numbers of ED patients with substance abuse complaints. 6 –8
This review focuses on common designer drugs of abuse that are encountered in the ED setting, including epidemiology, clinical features, and management. While typical presentations will be described in this article, it is important to remember each clinical encounter will present differently given different dosages, co-ingestions, and preexisting medical conditions.
Emerging substances of abuse
Synthetic cannabinoids
Synthetic cannabinoids, colloquially referred to as “K2,” “Spice,” or “fake marijuana,” are a class of recently developed designer drugs that contain chemical analogs of the psychoactive component of marijuana: tetrahydrocannabinol (THC). THC interacts with cannabinoid receptors CB1 and CB2 as partial agonists. This interaction effectively delays synaptic transmission and produces a variety of psychoactive effects such as relaxation, increased appetite and sleepiness, and marked changes in perception. 9 Signaling pathways related to CB1 receptor interaction include decreased cellular cyclic adenosine monophosphate and interference with ion channels. The analogs of THC found in synthetic cannabinoid products act as full-agonists at the same CB1 receptor, increasing the inhibition of gamma-aminobutyric acid (GABA) neurotransmission and therefore the severity of the psychoactive symptoms. 9,10 Many synthetic cannabinoids have since become schedule I controlled substances. However, new synthetic derivatives are constantly created to avoid regulation and are rebranded and redistributed across the United States. 10 Since the production of synthetic cannabinoids is not regulated, each batch created may vary in their composition and in recent years, there have been more presentations with potentially life-threatening conditions. 11,12 It is important to know that synthetic cannabinoids and their metabolites are not detected with routine drug screens. Although secondary assays are now available to detect synthetic cannabinoids, they are often not available in a timely fashion and results generally do not impact patient care.
Clinical presentation
Patients may present with a variety of symptoms, based on the type, dose, and route of synthetic cannabinoid exposure. The most common symptoms with which patients present include tachycardia, agitation, diaphoresis, confusion, emesis, anxiety, headache, and dizziness. 10 –13 In more severe cases, patients may be in an almost semicatatonic state, unresponsive to verbal or painful stimuli with other physical signs and symptoms such as bradycardia, hypotension, renal failure, or severe secondary trauma. The long-term consequences of prolonged synthetic cannabinoid use remains unclear. 10,13 –15
Treatment
In most cases, the treatment for synthetic cannabinoid intoxication is supportive, and relies on the principle of ABCs: airway, breathing, and circulation. Patients who are present with altered mental status should initially be closely observed and trialed with less invasive interventions such as oxygen, nasal trumpet, and repositioning for optimal airway patency. Patients unable to protect their airway or not oxygenating normally may require intubation. Hypotension should be treated and will often respond to intravenous (IV) fluids. If hypotension is persistent, vasopressors can be used. Severe bradycardia may require atropine or external cardiac pacing. Tachycardia should be treated with benzodiazepines and IV fluids, and an electrocardiogram should be performed to rule out myocardial ischemia and dysrhythmia. Benzodiazepines, such as lorazepam, starting with 2–4 mg and titrated to effect, can be used to treat agitation, catatonia, and anxiety. 10,11,15 Patients presenting with psychosis and more severe psychological symptoms should be closely monitored and may be treated with antipsychotics if deemed necessary. Patients with severe and persistent symptoms generally require admission. Patients whose symptoms improve in the ED should be monitored until they are at minimum awake, have normal vital signs, and deemed safe from harming themselves or others prior to discharge.
Bath salts
“Bath Salts,” “Zoom,” “Ivory Wave,” and “Vanilla Sky” are common names for products that contain synthetic cathinones, a chemical analog of the naturally occurring molecule found in the leaves of the Catha edulis plant. 16 Although the abuse of cathinones is not a new phenomenon, there has been a recent surge in its popularity. Since 2008, European countries and the United Kingdom experienced a dramatic increase in synthetic cathinone intoxications and even fatalities. A variety of demographic reports and surveys have been conducted to determine the prevalence and use of this designer drug. The most common users are “club-goers” and young adults, many of whom have also experimented with other “party drugs,” such as cocaine, amphetamines, and 3,4-methylenedioxy-methamphetamine (MDMA). 16 Structurally, cathinone and its synthetic derivatives are similar to amphetamines and MDMA. Therefore, cathinones have similar functionality—mainly stimulating the release of monoamine neurotransmitters, such as norepinephrine, dopamine, and serotonin, and preventing their reuptake. 17 The most common synthetic cathinones found in these products include mephedrone, methylone, and 3,4-methylenedioxypyrovalerone. Many synthetic cathinone products are continuously developed in clandestine laboratories to avoid regulation. 18
Clinical presentation
The variety and combination of synthetic cathinones in products that are abused creates a diverse spectrum of clinical presentations. Overall, the common manifestations are cardiovascular, gastrointestinal, and psychological/neurological. The most common neurological symptoms are agitation, anxiety, paranoia, psychosis, and headaches. Some psychological symptoms, including psychosis and hallucinations, may persist for several days after drug use. 17,18 In addition to neurological symptoms, hypertension, tachycardia, chest pain, hyperthermia, nausea, and emesis are other common symptoms which may require medical intervention. 18,19 More severe and long-term effects of synthetic cathinone use include liver and kidney failure, and potentially death.
Treatment
There is currently no antidote for synthetic cathinone intoxication; therefore, supportive care starting with the stabilization of the ABCs is the mainstay of treatment. Benzodiazepines are used for the treatment of agitation, aggression, tachycardia, and hypertension. Due to the similarity of synthetic cathinones to cocaine and amphetamines, there is a great deal of overlap in management. 17 –19 Tachycardia should be treated with benzodiazepines and IV fluids, and an electrocardiogram should be performed to rule out potential myocardial ischemia or dysrhythmia. Severe hyperthermia should be treated with active cooling measures to reestablish normal core temperature, and basal temperatures should be continually monitored. 19 In more severe cases, long-term hospitalization may be necessary to stabilize organ failure. 18,19
Nontraditional opioids and opioid analogs
The incidence and prevalence of opioid abuse has increasingly become a burden to our healthcare system and society as a whole. Traditional drugs of abuse in this class such as heroin, and prescription opioids such as oxycodone, hydrocodone, morphine, hydromorphone, and fentanyl continue to cause significant morbidity and mortality. More recently, nontraditional opioid compounds and analogs are easily purchased on the Internet as “legal highs” and are used to achieve similar effects.
Kratom
“Kratom,” derived from the tropical plant Mitragyna speciosa found in Southeast Asia, acts similarly to morphine at the µ- and δ-opioid receptors. The active ingredient in kratom is mitragynine, which interacts with opioid receptors, as well as adrenergic and serotonergic receptors, depending on dosage. This nonspecific drug interaction is uncommon, giving kratom both analgesic and stimulant-like properties. 20 Though little is known about the use of kratom outside of Southeast Asia, kratom product popularity has increased. Based on the increase in Internet searches and vendors of the product, it is speculated that kratom is most commonly used by people managing opioid withdrawal or chronic pain, without the supervision of a physician. 21,22 Due to its natural origins, kratom can be acquired on the Internet in many different formats, but this may change with the recent consideration for classification as a schedule I controlled substance. 23
Salvia
Salvia divinorum is an herb that grows naturally in Mexico. S. divinorum has been used for centuries in ritual ceremonies due to its hallucinogenic properties, caused by the active ingredient salvinorin A. 24 Although “salvia” causes mind-altering effects, salvinorin A does not act at 5-HT2A receptors as with most hallucinogens, but rather at the κ-opioid receptor. 24,25 The direct mechanism for hallucinogenic properties of salvia is still unknown, but salvinorin A has been implicated in diseases of perception such as schizophrenia and depression. Data regarding the prevalence of salvia use are limited, but based on self-report studies, salvia is most commonly used among young adults 18–25. 25 In addition, salvia use is highly correlated with concomitant mental health issues, such as anxiety and depression. 25 Salvia is currently not listed as a controlled substance in the United States and can be found at “head” shops and through the Internet, making it easily accessible to the general population, including adolescents.
Krokodil (desomorphine)
In the early 2000s, a homemade alternative to heroin named “Krokodil” gained popularity in Russia and Ukraine. 26 The active ingredient, desomorphine, is a semisynthetic opioid that interacts with the µ-opioid receptor. Opioid users in these regions rely on this substitute, which is about five times cheaper than heroin, yet has analgesic and euphoric properties 8–10 times greater than morphine. Krokodil is synthesized from codeine tablets, organic solvents, and other items commonly found in drug stores. This makes manufacturing of this drug easy, profitable, and incredibly dangerous. 26 –28 Since the drug is produced illegally, the contents and purity of Krokodil are constantly in question and can potentially contain heavy metals and other toxic by-products. Due to the short elimination half-life of desomorphine, consumers of Krokodil may use the drug more frequently than compared to users of heroin, leading to an increased risk of adverse effects.
U-47700
U-47700 is a synthetic opioid analog that was developed in the 1970s by the pharmaceutical company Upjohn. U-47700 works as a selective µ-opioid receptor agonist, with a binding affinity 7.5 times greater than morphine. 29,30 U-47700 has never been clinically tested on humans, but the drug is being diverted from laboratories to black market retailers as a recreational alternative to prescription opioids. There is limited pharmacokinetic data available regarding U-47700 and its analogs, making isolation and detection more difficult. There are also limited data regarding the users of U-47700, only case reports of near death due to consumption of the drug and online forums on “experiences during usage.” 30,31 U-47700 is available on the Internet for US$40 per gram in powdered form, which is usually taken through nasal inhalation or ingested in capsule form. 30 Due to the illicit nature of the drug, the purity and quality of U-47700 remains questionable. If the compound is contaminated with fentanyl or other opioid derivatives, more severe opioid toxicity may occur. 31 U-47700 has gained notoriety in the past year due to the potential involvement in the overdose of musician Prince. U-47700 had its peak number of Google searches in April 2016, 29 suggesting a potential new trend on the horizon for synthetic opioid abuse.
Clinical presentation
All nontraditional opioid and opioid analog intoxications can present with the typical symptoms of opioid overdose, which includes altered mental status, pinpoint pupils, bradycardia, hypotension, hypoxia, and hypothermia (Table 1). 32,33 The most concerning symptom of all however, is respiratory depression, which can be life-threatening. Clinical manifestations of kratom vary based on the dose ingested, with more stimulating effects occurring with small dosage, and analgesic effects dominating at higher dosage. Symptoms of excess kratom use include nausea, emesis, diarrhea, prolonged sedation, respiratory depression, and seizures. 34 Potential withdrawal symptoms include abdominal cramping, restlessness, muscle cramping, depression, irritability, vomiting, diarrhea, and anxiety. Administration of salvia produces vivid, short-term hallucinations, often involving synesthesias, and can cause confusion and agitation. 35 Psychological symptoms are often mild in comparison to other hallucinogens, but trauma as well as short-term confusion may require medical attention. Severe agitation and anxiety can be treated with benzodiazepines. Other symptoms will dissipate with metabolism of the salvinorin A.
Distinguishing symptoms of various nontraditional opioids and opioid analogs.

Manifestations of Krokodil use is rather devastating, with severe skin and venous damage such as ulcers and phlebitis around injection sites. With long-term use, more severe damage to injection sites occurs, including gangrene, limb amputations, and severe skin deformities. Due to heavy metal exposure, multiple system organ failure and severe neurotoxicity are common side effects of Krokodil use. 36 Organ damage or failure must be treated symptomatically. However, reversal of long-term damage is often impossible. 36
Treatment
For patients with severe respiratory depression, naloxone, the antidote for opioid overdose, should be administered immediately. The initial dose for opioid tolerant adults is 0.04 mg, although the effective dosing of naloxone is dependent on the specific opioid used, the relative affinity of naloxone to the opioid receptor, history of opioid tolerance, and the patient’s weight. 33 Higher doses may be required when treating more potent opioid analogs, such as fentanyl. Patients who experience recurrent toxicity after initial stabilization with naloxone may require a naloxone infusion, as the half-life of the antidote is much shorter than most opioids. Overaggressive use of naloxone can result in severe agitation due to precipitated withdrawal. The patient should be monitored for the duration of symptoms or anticipated symptoms, and if necessary transferred to an intensive care unit. Following stabilization, the patient should be examined for the presence of fentanyl patches, which have been implicated in delayed onset of respiratory depression. 33
Dissociative agents
Phencyclidine and ketamine
Phencyclidine (PCP, “Angel Dust,” “Rocket Fuel”) was originally created in the laboratory to be used as an anesthetic, but when severe emergence reactions limited its use, an analog with milder side effects was developed and became known as ketamine (“Vitamin K,” “Cat Valium,” “Special K”). The main mechanism of action of both PCP and ketamine is through the N-methyl-D-aspartate (NMDA) receptor where they are noncompetitive antagonists. Both also have dopaminergic, serotonergic, adrenergic, and cholinergic properties, in addition to activity at sigma receptors. The use and abuse of PCP has been observed since the 1960s, with prevalent abuse in certain areas. In fact, Washington, DC, saw more psychiatric admissions for PCP than for alcohol abuse and schizophrenia combined. The use of PCP has declined since then, but still remains a common drug of abuse. 37
Clinical presentation
Symptoms of PCP intoxication can be variable. A prospective study of 1000 cases 38 presenting to the ED found that mild to moderate hypertension and nystagmus were the most common physical findings. Almost half of patients were alert and oriented, and had behaviors that ranged from bizarre, agitated or violent, to disorganized, delusional or mute. Most patients experienced hallucinations, visual and/or auditory. Patients can also have tachycardia, hyperthermia, hypothermia, apnea, muscle rigidity, seizures, and cholinergic or anticholinergic signs. Muscle hyperactivity from combative behavior or seizures may lead to rhabdomyolysis.
Treatment
Treatment for all patients will be based on symptoms and clinical presentations, but testing of biological fluids can be done to determine the use of designer drugs (Table 2). Treatment of PCP and ketamine intoxication is mainly supportive, with a focus on ABCs and minimizing physical and psychological symptoms. Patients can be severely agitated and require sedation in order to preserve the safety of the patient and ED staff. Benzodiazepines are preferred for chemical sedation. While effective for the psychotic symptoms from PCP intoxication, butyrophenones such as haloperidol are generally avoided because they lower the seizure threshold and contribute to hyperthermia. Severely agitated patients should be hydrated with IV fluids when there are no contraindications, and also should have a creatinine kinase level checked to evaluate for rhabdomyolysis. Hyperthermia should be treated with sedation (agitation and muscle activity generates heat) and external cooling such as with ice packs and evaporating cooling strategies. 37 Furthermore, patients should have a thorough physical examination to evaluate for external signs of injury, as secondary trauma can occur as a result of psychosis, hallucinations or the patient’s own behavior while in a dissociated state.
Available urine, blood tests for drug detection.

MDPV: methylenedioxypyrovalerone; PCP: phencyclidine.
A recent case series reported that symptoms of PCP intoxication could improve enough to allow for safe discharge after a few of hours of observation for most patients. 39 However, the acute effects of PCP can last up to 36 h and there are case reports of prolonged psychosis for 2–4 weeks. 40 Ketamine produces similar symptoms but of a much shorter duration with resolution usually within 1 h, so patients may be asymptomatic by the time they reach the ED. 41 The patient should be observed in the ED, and a disposition decision made based on improvement of symptoms. Patients who have persistently abnormal vital signs, persistent severe symptoms, evidence of end organ injury, or no safe discharge plan should be admitted to the hospital.
Dextromethorphan
Dextromethorphan is an antitussive found in many cold remedies readily available without a prescription. Structurally similar to opioids yet without activity at µ- or δ-opiate receptors, dextromethorphan is an agonist at sigma receptors at low doses. At high doses, it has dissociative activity much like PCP and ketamine, including adrenergic and serotonergic properties, and NMDA antagonism. Adolescents from ages 13–19 are the most common demographic for the abuse of dextromethorphan, due to its legality and therefore “safety” as an introductory drug of abuse. 42
Clinical presentation
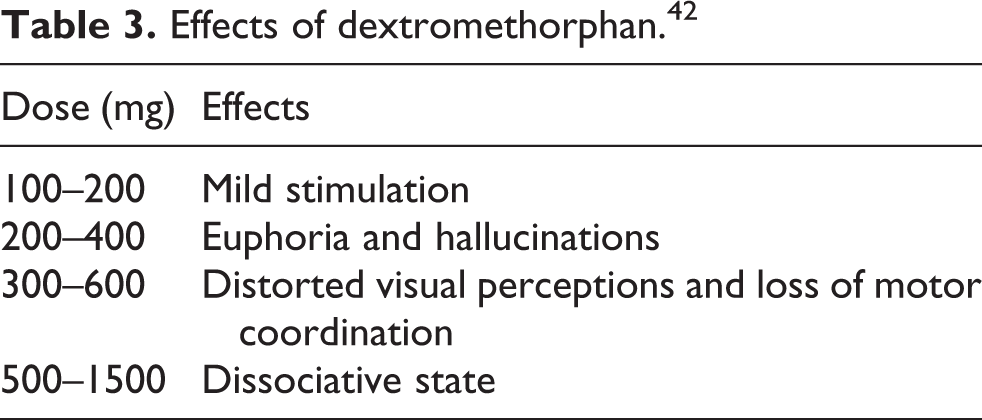
The clinical presentation of dextromethorphan intoxication depends on the dose ingested (Table 3). For lower doses, patients present with tachycardia, hypertension, mydriasis, diaphoresis, and nystagmus. With consumption of higher doses, patients present with vomiting, euphoria, and hallucinations. Moreover, at higher dosages, users will achieve an agitated or sedated dissociated state. 43
Treatment
Treatment of dextromethorphan intoxication is supportive, with a focus on ABCs. Specific to dextromethorphan is the importance of ruling out co-ingestions, as the drug is readily available in formulations containing medications such as acetaminophen, increasing risk of morbidity and mortality in overdose if intoxication is left untreated. Acetaminophen and salicylate levels should be checked in patients presenting with dextromethorphan intoxication.
All patients must be at minimum alert and oriented, with relative hemodynamic and vital sign stability and no traumatic injury to be considered appropriate for discharge. In addition, providers should assess that patients are safe, with no intention of harming themselves or others, and with adequate resources and a safe discharge plan from the ED.
Conclusion
The emergence of designer drugs has demanded emergency care settings to expand abilities to include the treatment of intoxications with these novel agents. The growing popularity of these designer drugs has the potential to increase the volume of intoxication cases seen in EDs throughout the United States. Popular designer drugs include synthetic cannabinoids (K2, Spice), synthetic cathinones (bath salts), nontraditional opioids (kratom, salvia, Krokodil), opioid analogs (U-47700), and dissociative agents (PCP, ketamine, dextromethorphan). It is evident that although these designer drugs appear clinically different in EDs, the treatment of most intoxications is similar in the need to stabilize the ABCs, maintain normal body temperature, control agitation, and manage dehydration and rhabdomyolysis. Ensuring patient and staff safety is also central to managing these cases.
This diversity of clinical presentations but similarity to common drugs of abuse will require EDs to be familiar with the new generation of drugs that are being abused, in order to provide prompt and accurate care.
Footnotes
Authors’ note
Data sharing not applicable to this article as no data sets were generated or analyzed during the current study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.