
Abstract
Acute exposure to systemic poisons represents an important challenge in clinical toxicology. We aimed to analyze the potential role of cardiac biomarkers, routine laboratory tests, and clinical scores as morbidity and in-hospital mortality predictors in patients intoxicated with various systemic poisons. We conducted a prospective study on adults acutely exposed to systemic poisons. We determined the PSS, Glasgow Coma Scale (GCS), and we performed electrocardiogram, laboratory tests, lactate and cardiac biomarkers (which were reassessed 4 h, respectively 6 h later). Of 120 patients included, 45% developed complications, 19.2% had a poor outcome, and 5% died. Multivariate logistic regression sustained lactate (odds ratio (OR) 1.58; confidence interval (CI) 95%: 0.97–2.59; p 0.066), MB isoenzyme of creatine kinase (6h-CKMB; OR 1.08; CI 95%: 1.02–1.16; p 0.018) as predictors for a poor outcome. A GCS < 10 (OR 0.113; CI 95%: 0.019–0.658; p 0.015) and 4h-lactate (OR 4.87; CI 95%: 0.79–29.82; p 0.087) predicted mortality after systemic poisons exposure. Receiver operating characteristic analysis showed that brain natriuretic peptide (area under the curve (AUC), 0.96; CI 95%: 0.92–0.99; p < 0.001), lactate (AUC, 0.91; CI 95%: 0.85–0.97; p < 0.001), and 6h-CKMB have good discriminatory capacity for predicting a poor outcome. In conclusion, these biomarkers, lactate, and GCS can be used to predict morbidity and mortality after systemic poisons exposure.
Introduction
Acute exposure to systemic poisons (which affect the entire body, with major effects manifested in at least two organs or systems) represents a life-threatening situation and an important segment of toxicological emergencies. Our previous experience showed that acute drug poisonings represent 28.43% of the total number of poisoned patients, the most frequently involved drugs being anticonvulsive drugs 8.63%, barbiturates 8.51%, and cardiovascular drugs 5.92%. 1 In the United States, poisoning with pharmaceutical products is the leading cause of accidental death, the most frequent agents involved being analgesics (including prescription opiates, acetaminophen, or combinations), street drugs, cardiovascular drugs, and sedative-hypnotics/antipsychotics. 2 Toxin or chemical exposures have a high prevalence, complication, and mortality rate among patients presented to the emergency department (ED), requiring specific care in an intensive care unit (ICU), both in our area and in the United States, where alcohols, gases/fumes, chemicals and miscellaneous hydrocarbons were associated with the largest number of fatalities, carbon monoxide (CO) being the leading cause of death among poisoning with non-pharmaceutical agents. 2 –4
The poisoning severity score (PSS), developed by the International Programme on Chemical Safety, the Commission of the European Union, and the European Association of Poison Centers and Clinical Toxicologists, proved to have a prospective value in some acute poisoning, in correlation with other clinical scales, or electrocardiogram (ECG) parameters. 5,6
General approach of a poisoned patient uses both routine laboratory tests and, in some circumstances, specific biomarkers developed for cardiac emergencies (troponins, cardiac enzymes, and natriuretic peptides).
Thus far, some investigators have used several laboratory tests as prognostic indicators to identify high-risk patients in acetaminophen, CO, or paraquat poisoning. 7 –9 Also, the prognostic utility of serum lactate to predict drug-overdose fatality was addressed retrospectively. 10 ECG parameters, especially the QTc interval, proved to have a role in predicting morbidity and mortality in organophosphate pesticide, herbicide poisoning, and in antipsychotic drugs poisoning. 6,11,12
There is little knowledge of the role of arterial lactate measurement and other routine laboratory tests or cardiac biomarkers in the risk assessment and prognosis after acute exposure to different types of systemic poisons (drugs, chemicals, gases, or plant toxins).
Our aim was to analyze the potential role of several conventional laboratory tests, biomarkers, and ECG parameters, in correlation with clinical scores, for early prediction of the need for ICU therapy, complications, short-term outcomes, and mortality in patients intoxicated with various systemic poisons, irrespective of dose or route of exposure. These parameters could be used immediately after admission, in order to identify patients at risk of a poor outcome or death, thus the management of these patients can be optimally adjusted. To the best of our knowledge, no data regarding markers of poor prognosis and death suitable for all types of systemic poisons exposures are available in literature.
Materials and methods
Study design and setting
This work was designed as a prospective, cohort study in a tertiary referral center for toxicology, admitting patients with acute poisoning from Romania. Over a period of 9 months (April 2015 to December 2015), we enrolled consecutive patients who were addressed to the hospital with acute poisoning diagnosed after exposure to a systemic poison. All subjects or their family (in the situation of an unconscious patient) signed an informed consent prior to enrollment. The study was funded by an internal research grant of the university and approved by the Ethics Committee of the university and hospital (no. 52/05.01.2015 and no. 7321/11.02.2015, respectively).
Selection of participants
The study included consecutive patients acutely exposed to systemic poisons that were referred to the ED and admitted to a medical clinic or ICU, older than 18 years, irrespective of gender. Patients were poisoned with prescription drugs (e.g. sedative-hypnotics, antidepressants, anticonvulsants, and cardiac medications), over-the-counter medicines—OTCs (e.g. salicylates, acetaminophen, non-steroidal anti-inflammatory drugs—NSAIDs, etc.), and illicit drugs (cocaine, amphetamines, opiates, cannabis, etc.), also with non-pharmaceutical agents such as pesticides, toxic gases (e.g. CO), toxic alcohols (e.g. methanol and ethyleneglycol), and plant toxins (e.g. wild mushrooms), or were exposed to multiple systemic poisons.
Patients without a signed informed consent, younger than 18 years, with a documented history of diabetes, chronic kidney disease, respiratory failure, or cardiovascular disease, with caustic poisoning, and with an acute pathology associated to poisoning (i.e. trauma, burns, etc.), or pronounced dead in the ED were excluded from our study.
Clinical and laboratory assessment
All patients who arrived in the ED after exposure to a systemic poison, diagnosed with acute poisoning after anamnesis, clinical examination, and toxicological tests (serum toxicology for ethanol, digitalis, cholinesterase, carboxihemoglobin level, and urine toxicology screens which included acetaminophen, salicylates, amphetamines, methamphetamines, opiates, benzodiazepines, cocaine, barbiturates, phencyclidine, tetrahydrocannabinol, and tricyclic antidepressants), underwent routine assessment in the ED (complete blood count (CBC), arterial lactate, glucose, electrolytes, C reactive protein, troponin I (TnI), brain natriuretic peptide (BNP), creatine phosphokinase (CK), MB isoenzyme of creatine kinase (CKMB), myoglobin, and renal and liver function profile). Selected poison concentrations were assessed the next day from the initial serum sample using gas chromatography-mass spectrometry techniques, if there was no available toxicological exam upon admission in the ED.
PSS was determined in all patients taking into account only the clinical symptoms and signs observed and not based on parameters such as amounts ingested or serum/plasma concentrations. We used the grading system described by Persson et al. 13 : (1) minor poisoning: mild, transient, and spontaneously resolving symptoms; (2) moderate poisoning: pronounced or prolonged symptoms; (3) severe poisoning: severe or life-threatening symptoms; and (4) fatal poisoning: death on arrival in ED. A 12-lead ECG (to determine rhythm, ST-T changes, and PR and QTc intervals) was recorded in the ED upon presentation. All included patients were subjected to clinical and ECG monitoring, pulse oxymetry, and non-invasive blood pressure measurements. Blood samples for arterial lactate, TnI, BNP, and CKMB analysis were collected upon presentation (0 h) and thereafter at the discretion of the attending physician, but mainly 4 h (lactate), respectively, 6 h from presentation (TnI, CKMB, N-terminal pro-B-type natriuretic peptide-NT-pro-BNP), in order to assess myocardial injury. 14,15 The blood and urine samples were analyzed using ABL 90 (Radiometer, Denmark) and GEM PREMIER 3500 (Instrumentation Laboratory, Bedford, Massachusetts, USA), Triage®Meter Pro TOX Drug Screen (Alere, Waltham, Massachusetts, USA), PATHFAST® Cardiac Biomarker Analyzer (LSI Medience Corporation, Japan), Sysmex XT-4000i-Automated Hematology Analyzer (Sysmex Corporation, Japan), and ARCHITECT c16000 clinical chemistry analyzer (Abbott Laboratories, Abbott Park, Illinois, USA). According to the manufacturer, the range of normal values for arterial lactate concentration is 0.3–0.8 mmol/L, for CKMB is 0–4.3 ng/mL, or 2–25 U/L, and for TnI is 0–0.02 ng/mL. For BNP and NT-proBNP levels, we used the cutoff limit of <100 pg/mL and <300 pg/mL, respectively, according to the guidelines. 16
The QTc was calculated using the Bazett formula and was considered prolonged if greater than 0.44 s. 17 An internal medicine specialist and a cardiologist conducted the QT interval measurements, with no statistical differences between readings.
The main outcome measure was status at hospital discharge. A favorable short-term outcome was considered in the absence of morbidity, or the presence of a complication affecting only one organ or system resolved during hospitalization. A poor short-term outcome was defined as in-hospital multiple complications or death.
Early complications were defined as follows: rhabdomyolysis (CK > 1000 IU/L); acute respiratory failure, defined as a condition requiring mechanical ventilation for correction of hypoxia, or hypercapnia, for more than 24 h; cardiovascular complications: hypotension, defined as systolic blood pressure (SBP) less than 90 mmHg, dysrhythmias with circulatory compromise, and acute myocardial injury (based on cardiac biomarkers and ECG); acute liver injury, defined as markedly elevated serum alanine and aspartate aminotransferase levels >10 times the upper limit of the normal range, accompanied by mild or moderate elevations in alkaline phosphatase levels; 18 acute kidney injury, defined as urine volume <0.5 mL/kg/h for 6 h, based on Kidney Disease: Improving Global Outcomes criteria (KDIGO); 19 and multiple complications (at least two organs or systems affected).
Statistical analysis
Data are presented as mean ± standard deviation, median with interquartile range, or frequency. Student’s t-test or Mann–Whitney U test for normal distributed variables as well as the χ 2 test and Cochrane’s statistic for categorical variables were used to perform univariate analysis. A p value < 0.05 was considered statistically significant. First, we applied simple binary logistic regression for each statistically significant variable. Then, we applied multivariate logistic regression on clusters of variables, which assess the systems and organs. Risk was expressed as odds ratios (OR) with confidence intervals (CI). Goodness-of-fit for multivariate models was confirmed using Hosmer and Lemeshow test. The receiver operating characteristic (ROC) methodology was used to analyze the discriminatory capacity of predictive variables. ROC analyses were expressed as curve plots and calculated area under the curve (AUC) with 95% CI, the associated p value representing the likelihood of the null hypothesis (AUC = 0.5). Statistical analyses were performed with SPSS (version 22.0; SPSS, Inc., Chicago, Illinois, USA).
Results
During the study period, 174 patients were admitted into the hospital after exposure to a systemic poison and 120 patients were enrolled in this study (Figure 1). The mean age of the patients included was 42.32 ± 16.88 years (range, 18–83 years). The time interval between acute poison exposure and presentation to ED ranged 0.5–4.5 h. The patients were categorized into groups according to their need for ICU therapy, morbidity, outcome, and survival. The population’s clinical, ECG, and laboratory characteristics are described in Table 1.

Flowchart of patients included in the study, their complications and outcomes.
Patients’ demographics, clinical, ECG, and laboratory parameters based on observed short-term outcomes.

PSS: poisoning severity score; GCS: Glasgow Coma Scale; HR: heart rate; SBP: systolic blood pressure; DBP: diastolic blood pressure; CRP: C-reactive protein; RDW: red cell distribution width; WBC: white blood cells; 6h-TnI: troponin I level 6 h after arrival to ED; ED: emergency department; CKMB: MB isoenzyme of creatine kinase; 6h-CKMB: MB isoenzyme of creatine kinase level 6 h after ED admission; BNP: brain natriuretic peptide; 6h-NT-proBNP: N-terminal pro-B-type natriuretic peptide level 6 h after emergency department admission.
Poisons involved (Table 2) were mainly represented by combination of toxins (30%), which included ethanol co-ingestion with antidepressants, benzodiazepines, barbiturates, antipsychotics, and prescription drugs (i.e. sedative-hypnotics—15%, antidepressants, antipsychotics and antiepileptics—12.9% and cardiovascular drugs—2.5%). Non-pharmaceutical agents involved (Table 2) were pesticides (12.5%), followed by toxic gases (6.66%), toxic alcohols, and chemicals (5%). The majority of cases (92.5%) were self-poisonings, while nine cases (7.5%) were accidental poison exposures.
Distribution of poison exposures based on short term-outcomes and mortality recorded.

OTCs: over-the-counter drugs; NSAID: nonsteroidal anti-inflammatory drug.
aWithin toxin category.
bWithin entire cohort studied.
Among the population studied, 84 patients (70%) had a positive toxicological exam on admission. For the rest of the 36 patients, there was no available technique to evidence the poison in ED, the diagnosis was made based on history of exposure, clinical and laboratory data, and confirmed the next day by serum quantitation using special techniques.
The outcome was favorable in 66 patients (55%), 23 patients experienced a poor short-term outcome (19.2%), and 21 patients needed ICU admission (17.5%). Complications occurred in 54 cases (45%). About 17.5% of patients developed multiple complications, which included myocardial damage. Cardiovascular complications alone were encountered in 8.33% of the patients. Complications were recorded mainly in poisoning with toxic alcohols (80%), pesticides (53.3%), antidepressants (46.2%), and combinations of toxins (38.9%). Within toxin category, patients in need for ICU therapy were those poisoned with toxic alcohols (80%), combination of poisons (22.2%), prescription drugs (20%), and toxic gases (12.5%).
The hospitalization was significantly prolonged in patients with a severe PSS on admission (6.39 ± 5.62 days; p < 0.001) and in patients who developed complications as a result of the poisoning (5.43 ± 4.46 days vs. 3.2 ± 1.76 days; p < 0.001).
Out of the 120 patients included, 6 patients died during hospitalization (5%) as a cause of multi-organ failure, having a length of hospital stay of 4 ± 3.22 days, non-significantly different from the survivors. Deaths were recorded in patients exposed to toxic alcohols and combination of poisons (two cases each), pesticides and antidepressants (one case each).
Distribution of variables within complication/no complication groups and survivors/non-survivors is presented in Table 3. We identified variables predictive for the need of ICU therapy, for complications and a poor outcome, which were included in logistic regression analysis (Table 4).
Patients’ characteristics in correlation with occurrence of complications and mortality.
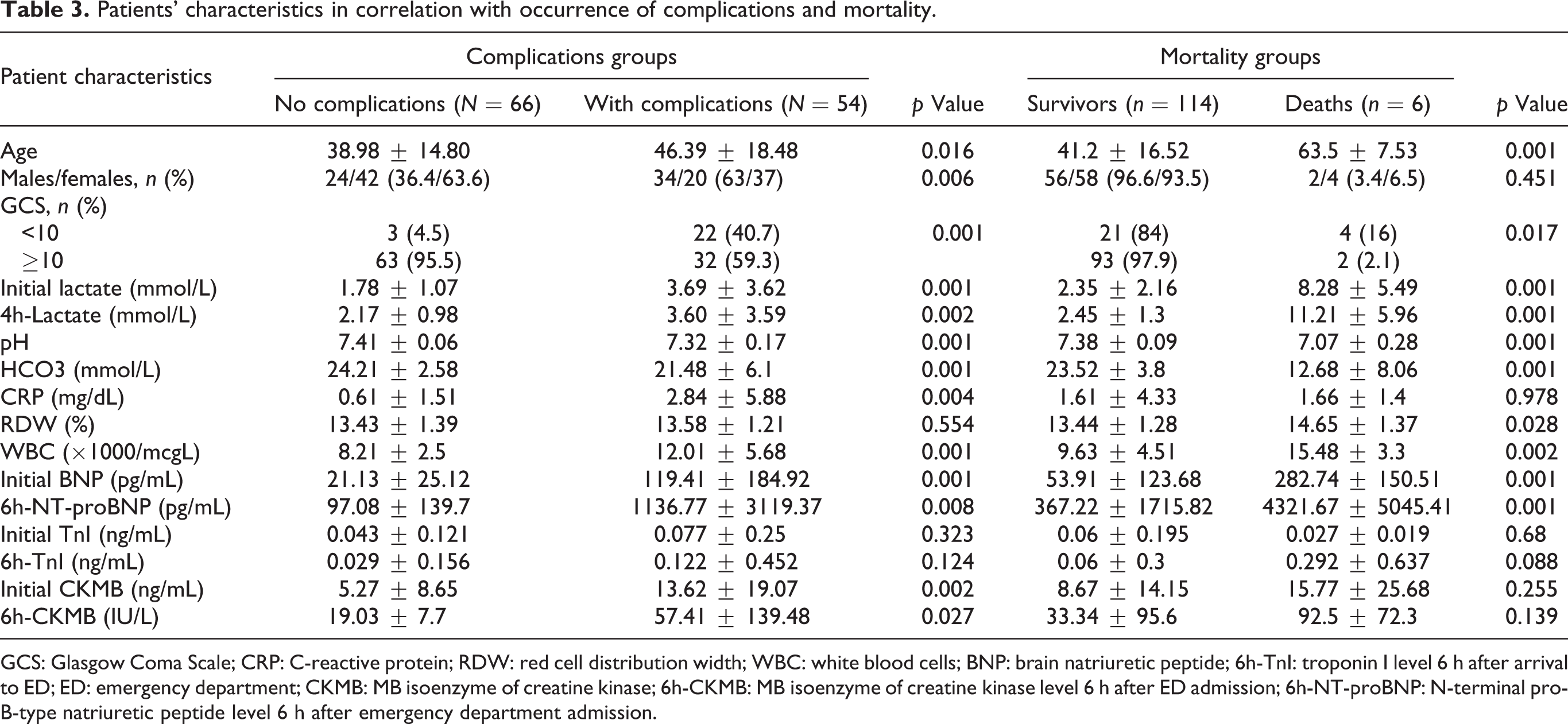
GCS: Glasgow Coma Scale; CRP: C-reactive protein; RDW: red cell distribution width; WBC: white blood cells; BNP: brain natriuretic peptide; 6h-TnI: troponin I level 6 h after arrival to ED; ED: emergency department; CKMB: MB isoenzyme of creatine kinase; 6h-CKMB: MB isoenzyme of creatine kinase level 6 h after ED admission; 6h-NT-proBNP: N-terminal pro-B-type natriuretic peptide level 6 h after emergency department admission.
Significant variables for a poor short-term outcome in acute poisoning with systemic toxins, selected using logistic regression analysis.
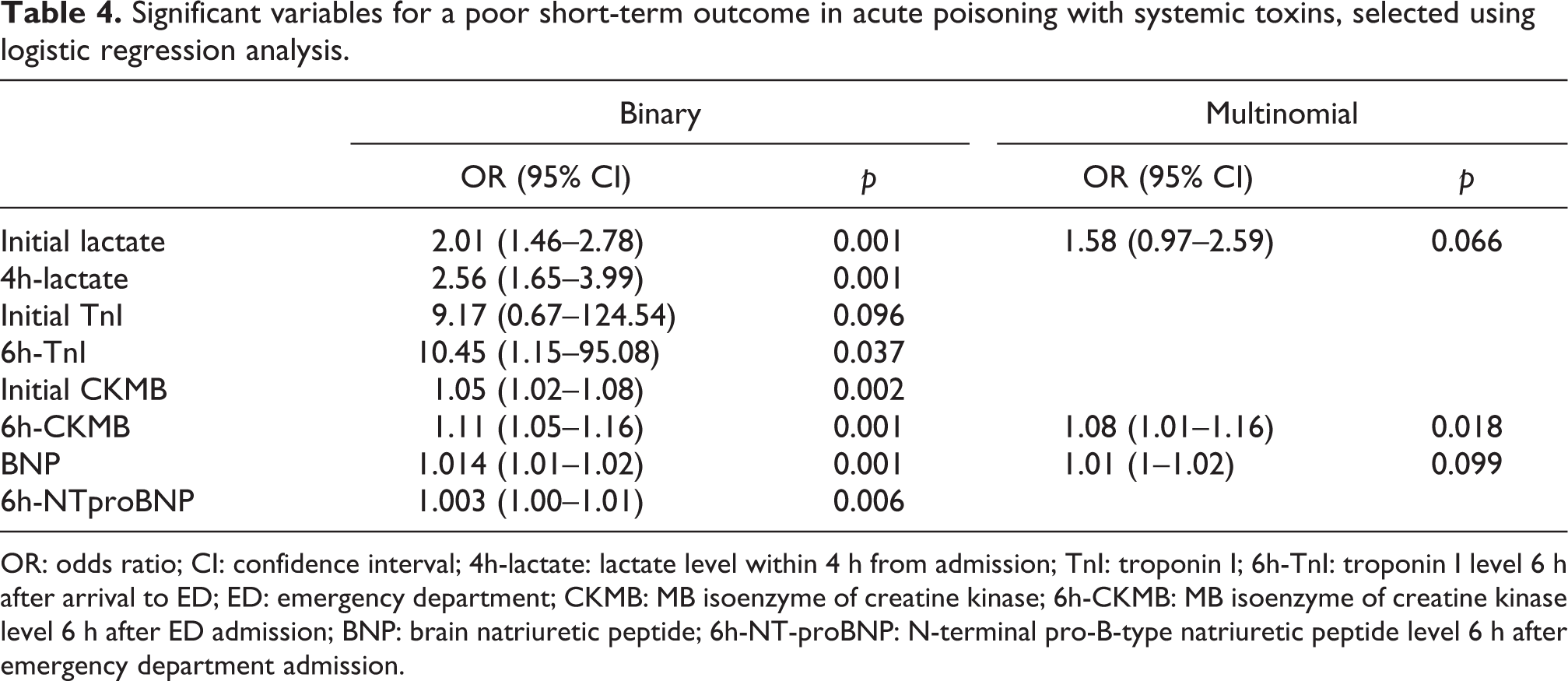
OR: odds ratio; CI: confidence interval; 4h-lactate: lactate level within 4 h from admission; TnI: troponin I; 6h-TnI: troponin I level 6 h after arrival to ED; ED: emergency department; CKMB: MB isoenzyme of creatine kinase; 6h-CKMB: MB isoenzyme of creatine kinase level 6 h after ED admission; BNP: brain natriuretic peptide; 6h-NT-proBNP: N-terminal pro-B-type natriuretic peptide level 6 h after emergency department admission.
Patients’ age influenced significantly both complications and death (41.2 ± 16.53 years vs. 63.5 ± 7.50 years, p 0.001), age > 60 years being correlated with mortality in intoxication with systemic poisons (OR 0.175; 95% CI: 0.033–0.942, p 0.042).
A severe PSS was significantly associated with the need for ICU therapy (71.4% vs. 28.6%, p < 0.001), with complications during hospitalization (92.9% vs. 7.1%, p < 0.001), and a poor short-term outcome (87% vs. 8.2%, p < 0.001). Patients with a moderate PSS were non-significantly distributed among non-complication and complication group (54.2% vs. 45.8%) and had a significant favorable outcome (46.6% vs. 13%, p < 0.001). A Glasgow Coma Scale (GCS) < 10 was significantly associated with occurrence of complications (40.7% vs. 4.5%, p < 0.001), a poor short-term outcome (65.2% vs. 10.3%, p < 0.001), and mortality (Tables 1 and 3) and predicted death in logistic regression analysis (OR 0.113; CI 95%: 0.019–0.658; p 0.015).
Cardiovascular parameters upon ED arrival, such as heart rate (beats per minute (b/min)) (102.62 ± 32.96 b/min vs. 89.48 ± 21.75 b/min, p 0.025), SBP (110.43 ± 22.83 mmHg vs. 125.72 ± 26.66 mmHg, p 0.016), and diastolic blood pressure (DBP; 67.52 ± 13.45 mmHg vs. 77.09 ± 14.73 mmHg, p 0.007) were correlated with the need for ICU admission. SBP (97.50 ± 39.13 mmHg; p 0.015) and DBP (63.33 ± 29.37 mmHg; p 0.041) were correlated with death but not with occurrence of complications during hospitalization. Among the ECG parameters analyzed using multiple logistic regression analysis, only the QTc interval was predictive for death in our cohort (OR 1.028; CI 95%: 1.01–1.05, p 0.005).
Ethanol co-ingestion had no influence on morbidity, outcome, or death in our cohort.
Red cell distribution width (RDW), reported as part of the CBC, was significantly higher in patients with a poor outcome (Table 1) and in non-survivors (Table 3), but it was not significantly different within complications groups, in toxic patients who were exposed to systemic poisons (Table 3). It showed a predictive value for mortality after logistic regression analysis (OR 1.610; CI 95%: 1.01–2.55; p .043).
White blood cells (WBC) count was significantly higher in patients who had a poor short-term prognosis, who developed complications, and in non-survivors (Tables 1, 3). Also, it was correlated with mortality (OR 1.2; CI 95%: 1.04–1.36; p 0.009) in logistic regression analysis.
After acute exposure to a systemic poison, initial arterial lactate level upon arrival at the ED was significantly higher in patients who needed ICU admission (5.29 ± 4.63 mmol/L vs. 2.12 ± 1.65 mmol/L, p < 0.001), who developed complications and in non-survivors group (Table 3). The 4h-lactate level correlated with complication occurrence, a poor short-term outcome, and death (Tables 1 and 3). Using binary logistic regression analysis, we found that both initial lactate (OR 1.46; CI 95%: 1.18–1.80; p 0.001) and 4h-lactate are predictive for mortality (OR 2.75; CI 95%: 1.49–5.04; p 0.001) as well as for a poor short-term outcome (Table 4) in patients acutely intoxicated with a systemic poison. 4h-lactate correlated with mortality also in multivariate logistic regression analysis (OR 4.87; CI 95%: 0.79–29.82, p .087).
Patients in need for ICU therapy had a significantly higher level of BNP on admission (146.53 ± 222.64 pg/mL vs. 58.67 ± 103.07 pg/mL, p 0.006). Also, BNP was increased in the non-survivors group (Table 3). The patients with a poor short-term outcome, and who developed complications had on admission a significantly higher BNP, and a higher NT-proBNP level 6 h later (Tables 1, 3). Also they presented significantly increased values of initial CKMB and 6h-CKMB (Tables 1, 3), although there was no statistical significant difference of CKMB and 6h-CKMB levels within mortality groups (Table 3). However, both initial CKMB (OR 1.06; CI 95%: 1–1.12; p 0.033) and 6h-CKMB (OR 1.06; CI 95%: 1.02–1.10; p 0.003) correlated with mortality, in multivariate logistic regression analysis. Logistic regression analysis showed a good correlation of these biomarkers with a poor short-term outcome (Table 4). Initial TnI and 6h-TnI were significantly increased within poor short-outcome group (Table 1), but the differences were not statistically significant within complication and mortality groups (Table 3), and showed no predictive value for mortality, in logistic regression analysis.
Several other variables showed significantly statistical differences between means, respectively, frequencies in the groups with and without complications, and within outcome groups (Tables 1, 3). The results of logistic regression applied to variables with significant statistical difference between outcome groups are presented in Table 4. Validation of predictive variables was performed with ROC methodology (Figure 2). We observed all predictive variables, but only four of them had a high value of AUC, demonstrating a very good discriminatory power. The optimal cutoff value for predicting poor short-term outcomes calculated from this ROC curve was: initial lactate > 2.27 mmol/L with a sensitivity of 91.3% and a specificity of 76.3%; BNP > 123.5 pg/mL with a sensitivity of 69.6% and a specificity of 94.8%; 4h-lactate level > 2.63 mmol/L with a sensitivity of 82.6% and a specificity of 70.1%; and 6h-CKMB > 31.50 U/L with a sensitivity of 73.9% and a specificity of 85.6%. Also we used ROC methodology to observe optimal cutoff value for predicting mortality in these variables: initial lactate level (cutoff point 3.3 mmol/L; AUC, 0.92; CI 95%, 0.86–0.98; p < 0.001), 4h-lactate level (cutoff point 3.7 mmol/L; AUC, 0.98; CI 95%, 0.83–0.88; p < 0.001), BNP (cutoff point 130 pg/mL; AUC, 0.95; CI 95%, 0.91–0.99; p < 0.001), and 6h-CKMB (cutoff point 35.5 U/L; AUC, 0.94; CI 95%, 0.89–0.99; p < 0.001).

Receiver operating characteristic curves validates discriminatory power of predictive variables for short-term poor outcome. Areas under the curves: Initial lactate (lactate obtained upon arrival to ED): 0.91 (95% confidence interval 0.849–0.967, p 0.001); 4h-lactate (lactate level obtained 4h after arrival to ED): 0.87 (95% confidence interval 0.789–0.947, p 0.001); BNP: 0.96 (95% confidence interval 0.921–0.992, p 0.001); 6h-CKMB (CKMB obtained 6 h after ED presentation): 0.86 (95% confidence interval 0.776–0.950, p 0.001). BNP: brain natriuretic peptide; CKMB: MB isoenzyme of creatine kinase; 6h-CKMB: MB isoenzyme of creatine kinase 6 h after ED presentation; ED: emergency department.
Discussion
To the best of our knowledge, this study is the first prospective evaluation of the different clinical scores, such as PSS and GCS, in correlation with routine laboratory tests, such as lactate level, cardiac biomarkers and ECG parameters, as predictors for morbidity, short-term outcome, and in-hospital mortality, in patients exposed to various systemic poisons (gases, chemicals, drugs, or plant toxins).
Acute poisonings represent a worldwide problem. In our area, epidemiological data suggested that 97.27% are acute drug poisoning in suicide attempts, using mainly combinations of drugs (32.92%), with a mortality rate of 0.3%. 1 The majority of drugs ingested in suicide attempts in our study were combination of drugs, sedative-hypnotics, analgesics, and antipsychotics, comparable with the distribution mentioned in reports from the National Poison Data Systems in the United States. 2 Among non-pharmaceutical agents related with mortality, both in United States and in our area, toxic alcohols, gases (including CO), pesticides, and chemicals represent major concerns. 4,20 Self-poisoning with organophosphate pesticides is a major health problem in low-income and developing countries, and 200,000 deaths occur annually worldwide. 21,22 Data in our area showed an 11% prevalence of pesticide exposures, with a mortality rate of 3.8%. 23
Some retrospective studies attempted to identify prognostic or mortality indicators in CO poisoning (RDW, lactate, cardiac biomarkers, and copeptine) or in pesticide poisoning (GCS, RDW, serum cholinesterase level, acid–base status, sex, age, and QT interval prolongation on ECG). 6,9,11,24 –29
Among clinical scores, both PSS and GCS showed a prognostic value in retrospective analysis in some acute poisoning. 6,30,31 Several studies attempted to quantify the value of GCS in predicting complications, admission to ICU, or mortality, but the results showed different levels of GCS score, with different agents, population, or outcomes studied. 32 Although GCS score is a dynamic variable which varies with time, and interventions applied on toxic patients (i.e. antidote), it was proved to be superior over Acute Physiology and Chronic Health Evaluation (APACHE II), Modified APACHE II Score, and Mainz Emergency Evaluation Scores upon ED admission of patients with mixed drug poisoning induced coma. 33
Our observations showed that a severe PSS and a GCS < 10 at admission in the ED are significantly associated with a poor short-term outcome, the need for ICU admission and early complications in acute intoxication with different types of systemic poisons (drugs, combination of toxins, pesticides, toxic gases, or alcohols). The level of GCS score < 10 is consistent with that assessed prospectively in mixed acute drug poisoning, where it proved to be associated with complication occurrence. 32 In addition, our results showed a predictive role for mortality of this score, in patients acutely exposed to a systemic poison.
An ECG parameter, the QTc interval, proved to have a predictive value for death in acute intoxication with different categories of systemic poisons, not only for pesticides (12.5% patients in cohort studied), antidepressants, or antipsychotics (5.9% cases in our population), as it was showed before in literature. 6,11,12,34
A routine test included in CBC, RDW is indicative of anisocytosis in anemias. It has been used to predict outcome in several clinical conditions, such as heart failure, acute coronary syndromes, and peripheral artery disease. 35 In clinical toxicology is an independent predictor of 30-day mortality in patients with organophosphate pesticide poisoning 25 and is indicative for the onset of complications in CO acute poisoning. 26 Our patients had normal hemoglobin levels, and a higher RDW in poor outcome and mortality groups, which we consider to be related with inflammatory processes. It demonstrated in our study a predictive value for death in patients acutely intoxicated with a wide range of systemic poisons, from plant toxins to chemicals and drugs.
A high WBC count was reported before in patients poisoned with organophosphate pesticides and CO, who developed complications. 36,37 It is probably correlated with the development of oxidative injury, and oxygen-free radicals activation, as part of a systemic inflammatory process responsible for the development of complications. 34 We recorded higher values of WBC count in poisoned patients after acute exposure to a systemic poison, in patients with need for ICU therapy, and in the complications group, and this increased the risk of mortality by 20% in our cohort, in patients who developed multiple complications before death.
Hyperlactatemia is an independent predictor of drug-poisoning mortality, with a cut point of 3.0 mmol/L (84% sensitivity, 75% specificity) conferring a 15.8-fold increase in odds of fatality (p < 0.001), based on a case-control study, which reported a 5.72% mortality rate. 10 Other authors found that a selected lactate cutoff point of 3 mmol/L is not an absolute predictor of fatality in drug overdoses, such as β-blocker acute poisoning. 38 Furthermore, acidosis caused by elevated lactate levels has been associated with a higher mortality than acidosis due to other underlying causes. 39 Several studies reported that initial arterial lactate value and 12 h lactate metabolic clearance rate are good predictive markers for the outcome of paraquat poisoning, 9 and that lactate is an useful tool for risk stratification, and predicting hospitalization and fatalities of CO or drug-poisoned patients. 10,40 Mixed acidosis influenced the outcome of patients poisoned with pesticides, and acid–base interpretation is well correlated with the severity and death in this poisoning. 29
After exposure to systemic poisons, we obtained similar correlations between the initial increased lactate level and short-term outcome, complications and death, but we did not find any correlation between lactate metabolic clearance rate and mortality or prognosis. This could be a result of the fact that we used the lactate level 4 h after admission, not 12 h later, as did other authors. 9 We aimed to identify prognostic indicators early available during the ED stay and, usually, 12 h after hospital arrival, the poisoned patient is already admitted in ICU or a medical ward. Although based on a small number of fatalities (5% in the cohort studied) which may have underpowered the analysis, our results showed that upon ED arrival, the cutoff for initial lactate predicting mortality was 3.3 mmol/L (sensitivity 86%, specificity 88%; p 0.001), consistent with other authors results, 10 and the cutoff for 4h-lactate predicting mortality was 3.7 mmol/L (sensitivity 83%, specificity 88%; p 0.001).
Specific cardiac biomarkers (such as troponins and natriuretic peptides) were experimentally studied in drug-induced poisoning. 41 In clinical toxicology, NT-pro-BNP associated with cardiac ultrasound parameters were studied only in CO exposure, where they proved to bring a significant advantage in the diagnosis of patients with myocardial damage. 27 Myocardial injury assessed in ED upon the arrival of patients severely poisoned with CO independently predicted a short-term poor outcome. 8
We aimed to estimate the utility as outcome and mortality predictors of cardiac biomarkers in acute exposures to a systemic poison and we excluded possible interferences with acute trauma, burns, and cardiovascular, renal, respiratory, or metabolic chronic diseases by including these pathologies in exclusion criteria.
In nondiabetic patients, without history of cardiovascular disease, chronic renal or respiratory failure, acutely intoxicated with systemic poisons, and assessed 0.5–4.5 h after the exposure, our results demonstrate the benefit of using initial and 6h-CKMB, BNP, and 6h-NT-proBNP as indicators for the need of ICU admission, of early complications, and a poor outcome. Both initial CKMB and 6h-CKMB represented risk factors for mortality in logistic regression analysis. However, the level of TnI showed no correlation with complications, or death.
Some indicators, such as toxicological history, GCS, QT interval, and serum lactate level, proved to be useful to distinguish between low- and high-acuity poisoned patients with deliberate drug poisoning, in order to avoid excessive morbidity, after a retrospective analysis. 21
Our prospective study provide support for the initial hypothesis that there are some indices available readily, upon the arrival of a patient acutely exposed to a systemic poison (irrespective of type, dose, or route of entrance), such as PSS, a GCS < 10, initial and 4h-arterial lactate level, BNP, and 6h-CKMB, which can early predict complications, poor short-term outcomes, and mortality, whether it is the case of a self-poisoning or an accidental exposure to a toxin. We intend to continue the study including other centers, the population aged < 18 years, and to continue analysis on categories of toxins, in order to estimate if the toxin itself could be responsible in a larger manner of complications, poor outcome, or mortality rate.
Some limitations in this study should be mentioned. Including patients from a single tertiary center in Romania implies a possible selection bias in the population studied, although the epidemiological and toxicological data are consistent with those reported in other regions. 2,21 Other prognostic markers, such as APACHE II score, were not reported. We could not calibrate the influence of toxin serum concentration. One other limitation is related to the pitfall of monitoring patients at least 30 days after exposure to systemic poisons.
We conclude that in acute intoxications with systemic poisons, there are several parameters that can be obtained fast, are less invasive, low cost, and are available in every ED, which proved to be helpful in predicting morbidity and mortality: GCS, initial and 4h-lactate level, BNP, and 6 h-CKMB. Thus, the management of these poisonings can be promptly refined in order to address the morbidity and to increase survival rate.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the University of Medicine and Pharmacy “Gr. T. Popa” Iasi, Romania (internal research grant no. 30884/30.12.2014).