
Abstract
Background:
Disability weights (DWs) are used in disease burden studies, with the calculation of the weight of the disability as years lived with disability versus years of lost life accounting for mortalities. Currently, there is a single DW score available for poisoning, which is considered to be a single health state. This makes it difficult to evaluate the differing burdens of poisonings involving various substances/conditions in comparison with other health states in countries with different patterns of substance abuse. The aim of this study is therefore to estimate the DWs of 18 common poisonings based on the expert elicitation method.
Methods:
A panel of 10 medical clinicians who were familiar with the clinical aspects of different poisonings estimated the DWs of 50 health states by interpolating them on a calibrated Visual Analogue Scale. The DWs of some poisonings, such as alcohol, cannabis and heroin, had been estimated in previous studies and so were used to determine the external consistency of our panel. As a matter of routine, the DWs could vary on a scale between 0 (best health state) and 1 (worst health state).
Results:
Statistical analysis showed that both the internal (Cronbach’s α = 0.912) and external consistency of the panel were acceptable. The DWs for the different poisonings were estimated along a range from 0.830 for severe aluminium phosphide to 0.022 for mild benzodiazepine.
Conclusions:
Different poisonings should be weighted differently since they vary widely. Unfortunately, they are currently all weighted the same.
Keywords
Introduction
Poisoning is a major public health concern worldwide, ranking within the accidents and traumas category in terms of important causes of mortality and morbidity. 1 In 2004 alone, it was estimated that 346,000 people worldwide died from unintentional poisoning. Of these deaths, 91% occurred in low- and middle-income countries. In the same year, unintentional poisoning also caused the loss of over 7.4 million years of healthy life (disability-adjusted life years (DALYs); see below for more information). Further, nearly a million people die each year as a result of suicide, with substance abuse accounting for a significant number of such deaths. 2
In Iran, it is estimated that around 3750 people die each year due to poisoning. 3 Moreover, an estimated 125,000 poisonings occur each year (thereby affecting 0.16% of the Iranian population). 4 Approximately 50,000 (45%) of these individuals intentionally abused the poisonous substance in order to attempt suicide. 5 Among them, about 65% are treated in an emergency room, while the rest are admitted to hospital. 6 Distressingly, it is estimated that a significant portion (25%) of those Iranians who attempt suicide via poisoning die before they reach medical care. 7 From these figures, it is apparent that poisonings are a worryingly common health problem, mostly involving younger and more active members of the population.
Poisonings may occur in a number of situations (i.e. unintentional, suicide and homicide). 8 Unintentional poisonings are the most common, while, in terms of intentional poisonings, general criminal cases and then homicides account for the second and third most common instances of poisoning. 9 In the United States, there are growing concerns about overdoses involving prescription drugs and the increase in the number of hospitalizations due to the intentional or unintentional misuse of these drugs. Further, suicide mortality due to poisoning by drugs or alcohol resulted in 75% of all poisoning deaths in the United States. 10 –12
Recently, rather than focusing on mortality and the prevalence of poisonings, the burden of disease has been considered to be an important indicator of a nation’s health. Such a burden of disease can be classified as the impression of a particular health problem on a studied population as measured by mortality and morbidity. It is most frequently determined according to DALYs. 2 DALYs represent both the loss of healthy years of life due to early death (years of life lost (YLL)) and the loss of healthy life years owing to disability (years lived with disability (YLD)). Consequently, one DALY denotes the loss of the equivalent of 1 year of full health. The disability weight (DW) is an index ranging between 0 (best imaginable health state) and 1 (worst imaginable health state), which represents the severity of the disability stemming from a particular health state. The YLD for a specific health state is estimated by multiplying the incidence of that health state by the average duration of the disease and the DW. 9,13
In general, DWs are estimated by experts, patients or public panels, and so they are dependent on the viewpoints of the investigators as well as the particular objectives of the study. In epidemiological studies in which DALYs are used to compare population health, expert panels are frequently relied on. 14
DWs have been estimated for many health states, 13 including poisoning (DW = 0.611 for 0–14 years and 0.608 for above 14 years.). 15 But most of abused substances, particularly the acute ones, except few ones, for example, alcohol and heroin abuse, assigned a single weight (poisoning: short term, with or without treatment equal to 0.171 (0.116–0.239). 16 But the medical toxicologists believe that even the acute poisonings, despite short course and similarities, have enough differences to encoded differently. 17
So, since poisonings arguably make a large contribution to the overall disease burden of societies worldwide, the first aim of this study is to see whether or not the DW for poisonings would vary based on expert panel elicitation. The second aim of this study is to estimate the DWs of the 18 most common poisonings, which all seem to demonstrate the necessity of being scored differently.
Materials and methods
In this study, the valuation of DWs was based on the viewpoints of a specially constituted panel of experts. First, the panellists received printed descriptions of the various health states, which they were then required to interpolate on a Visual Analogue Scale (VAS) ranging from 0 (worst imaginable health state) to 100 (best imaginable health state). For the interpolation, unless otherwise specified, the panellists were coached to evaluate the living costs associated with each health state for 1 year.
The VAS method was calibrated in a Dutch DWs study using the person trade-off (PTO) method. 18 Although the PTO method is the favoured approach in the literature, its relative complexity rendered it unsuitable 19 and so this study used the calibrated VAS method to value the health states. Such an approach has been tested and validated in other studies. 20 In addition to receiving descriptions of the 18 poisonings (Table 2), the panellists were provided with the scores of some other poisoning situations as references.
The interpolation on the VAS results in a value between 0 and 100 for each health state, with 0 representing the worst state imaginable and 100 the best imaginable health state. These interpolated values can be made to correspond to utilities on a scale from 0 to 1 by dividing them by 100. The formula for calculating DW from utility (U) is:

Panel formation
In the current study, the members of the expert panel were nominated on the basis of two criteria. First, they had to be experienced medical practitioners with expertise in medical toxicology and the clinical management of poisonings. This was essential because they were expected to value a wide range of specialized medical conditions. Second, a background in research was necessary, since understanding the meaning and applicability of the DALY is important when valuing health states. All panellists were, therefore, academic scholars. In conclusion, the panellists needed to be knowledgeable about medical toxicology and to have completed PhD, fellowship or other academic courses relevant to the clinical management of relevant medical conditions.
In total, 16 experts were invited to participate in this study. Five of them either indicated that they were unable to take part or else did not fully complete the initial surveys. The remaining 11 panellists received the set of necessary documents. The 10 experts who actually returned the documents formed the final panel for our study.
Some health states for which DWs had previously been recognized were included in this study in order to form the basis for our panel’s determinations and to be adjusted in line with previously used panels. These health states were required to characterize a broad range of DWs, as well as to be similar in terms of course and severity to the DWs of the health states we expected to measure in the current study. The selected health states were as follows: alcohol mild (0.259), alcohol moderate (0.388), alcohol severe (0.549), heroin (0.641), cannabis (0.329) and amphetamine (0.353) in our study as glass. 15
The poisonings common in our region were identified from the literature and were then used based on the International Classification of Diseases 10th Revision (ICD-10). 19 The current literature was used for extracting the clinical presentations of the included poisonings.
We selected the 18 most commonly abused substances. The clinical manifestations, signs, symptoms and outcomes of each health state were extracted from the literature and are presented here in a table (Table 1). Each form of substance abuse was also divided into two or three severity states based on outcomes (Table 2). Then, following the Delphi method, six toxicologists with clinical backgrounds (MDs) were asked about the items involved in each health states and their severity categorization.
Example definitions of each clinical manifestation.

Example form the questionnaire asking the experts to score each poisoning according to two or three disease states.

GI: gastrointestinal; CNS: central nervous system; AST: aspartate transaminase; ALP: alkaline phosphatase.
In addition, a standardized health classification derived from the EuroQol 5D, 20,21 used following approval from the EQ-5D group (the Netherlands), was added to the description. This rates the condition according to six dimensions (mobility, self-care, usual activities, pain/discomfort, anxiety/depression and cognition) on a 5-point scale (no problems to severe problems) [a full report on this will be published in another paper]. These descriptions were elicited from approximately 80 patients who were admitted to our medical toxicology service. The ratings provided a helpful clue for the panellists to be able to find clear evidence about the real situation of a patient experiencing a particular poisoning. After determining the health state of each poisoning along with the sub-items based on severity and outcome, the authors then transcribed the descriptions. The prepared documents were presented to 10 clinical toxicologists/medical doctors who have worked on a medical toxicology ward for at least 4 years (the panel). They were then asked to assign the utility measures to the health states based on the provided descriptions.
Statistical analyses
Prior to calculating the mean DWs for the 18 most common poisonings in 50 health states based on severity, the internal consistency (and thus the reliability) of the panel was assessed: (1) by calculating Cronbach’s α; (2) by calculating the Pearson correlation coefficients and (3) using paired sample t-tests. To achieve this, each panellist was compared with the mean of the other panellists in order to recognize outlier responders (and the panellists who gave significantly different valuations for certain health states were calibrated by this method). We checked the normality of data and whenever the data were not normally distributed, the non-parametric counterpart of t-test, Mann–Whitney was applied.
Next, the external consistency of the panel was determined by utilizing the health states for which DWs had previously been assessed. These DWs were compared to the DWs suggested by our panel using Pearson correlation coefficients and paired sample t-tests. All analyses were performed using SPSS 16.0. The significance level of p value was less than 0.05 and it is highlighted in each table with symbols.
Results
The majority of the panellists were male (83.4%). The mean age of the panel was 40 years (SD = 5.24) and the mean number of years in the medical profession was 12 (SD = 2.83). Some 16.4% of panellists had a research background at PhD level. The others were medical doctors with a specialty in paediatrics, internal medicine, psychiatrics or forensic medicine, while 66.6% of them had completed a fellowship in medical toxicology. All of the panellists have been routinely involved in patient care through working on a medical toxicology ward for at least 4 years.
Internal consistency of the panel
In order to assess the internal consistency of our scoring, we performed a reliability analysis between the panellists and determined that the findings were appropriate (Cronbach’s α = 0.912). We excluded each panellist one by one and no increase was seen in the overall Cronbach’s α. The statistical tests of the paired sample t-tests and Pearson correlations were compared between the panellists. The mean score of the panel demonstrated that most of the panellists exhibited an appropriate agreement with their counterparts (Table 3). Nevertheless, some panellists valued the selected health states lower or higher, although the overall deviation from the mean of the panel was not significant and so no panellists were omitted. The high level of agreement was due to the calibration process we conducted, involving holding sessions and thoroughly explaining the process of scoring to the panel members. Ultimately, the deviation identified was too small to be echoed in the Cronbach’s α for the aforementioned panellists.
Internal consistency: Paired sample t-test and Pearson correlation between the panellists and the panel’s mean.

M: mean; SD: standard deviation; r: Pearson correlation between panellist and panel mean. N = 50.
b p < 0.05.
cOr its nonparametric counterpart, Mann–Whitney.
External consistency of the panel
The paired sample t-tests and Pearson correlations of the DWs measured by our team and the corresponding DWs established in previous studies were compared. The correlations were mainly strong (range = 0.43−0.95) and the t-tests were not significantly different, indicating a reasonable external consistency (Tables 4 and 5).
External consistency: Paired t-test and Pearson correlation between each panellist and the mean DW from previous studies.
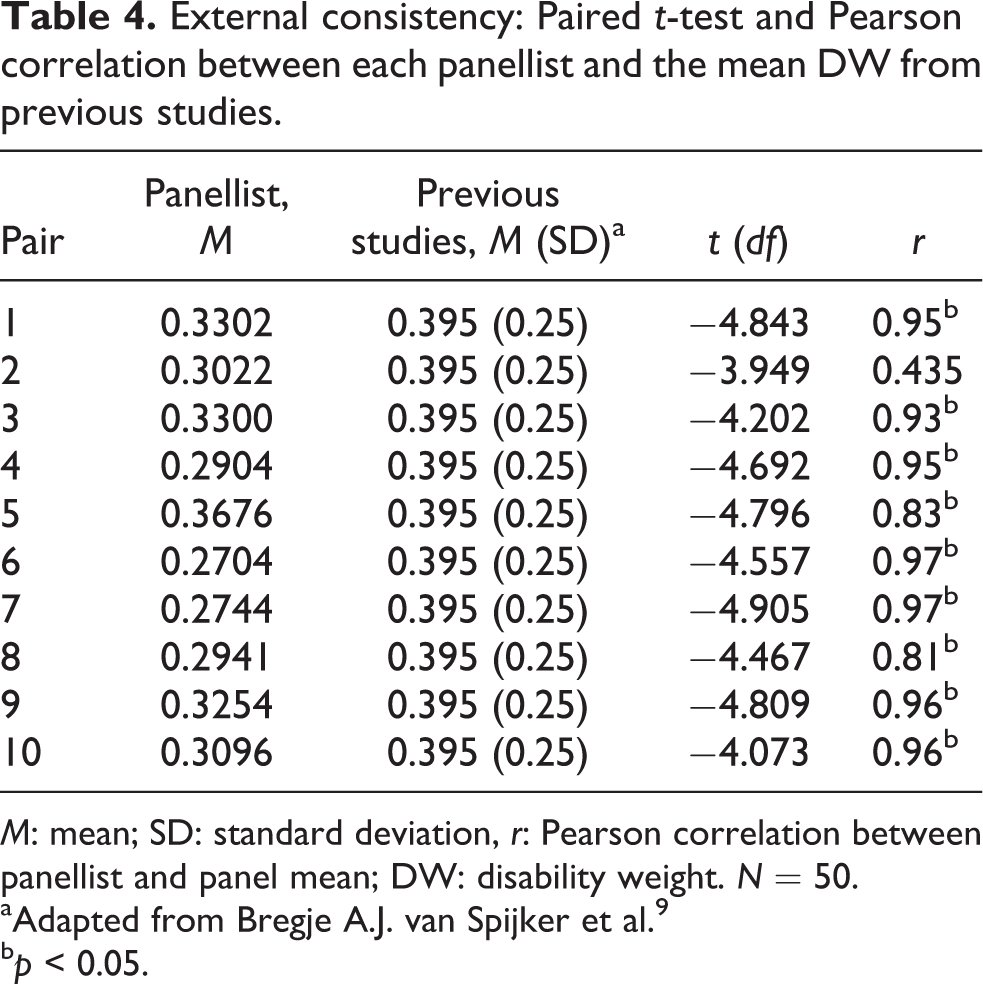
M: mean; SD: standard deviation, r: Pearson correlation between panellist and panel mean; DW: disability weight. N = 50.
aAdapted from Bregje A.J. van Spijker et al. 9
b p < 0.05.
Agreement between the DWs of previous studies and those of the current study.
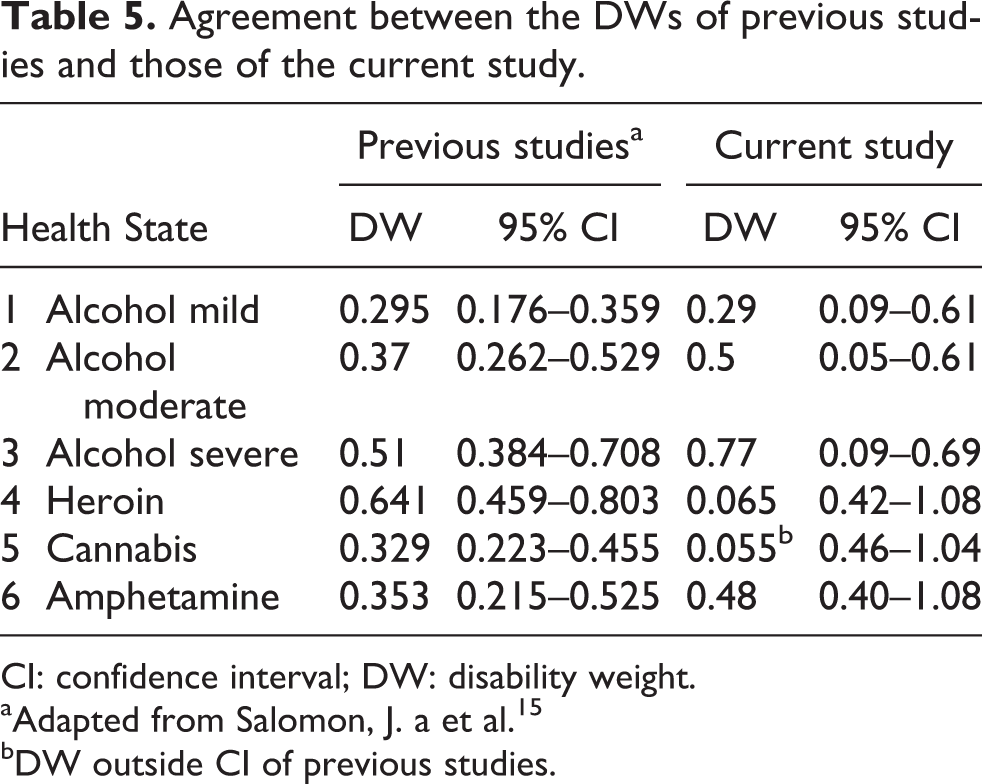
CI: confidence interval; DW: disability weight.
aAdapted from Salomon, J. a et al. 15
bDW outside CI of previous studies.
DWs for the acute poisonings in detail
As shown in Table 6, the DWs for the different poisonings vary between 0.052 and 0.83, with an average of 0.34. These DWs are presented for all 18 abused substances in 50 disease states (Table 6).
The DWs for 18 poisonings in two to three disease states based on our panel elicitation.

Discussion
According to a 2004 World Health Organization report, the total worldwide DALY for poisoning is 7,447,000 years and, in all regions, poisoning is within the injury category as the second most common cause of mortality or morbidity after road traffic accidents. This is measured based on the previously calculated DW of 0.607 and 0.611 for those above and below 14 years, respectively.
This article presents the DWs for 18 common acute poisonings after they have been divided into the mild, moderate and severe stages. It is notable that our mean DW for all of the measured DWs (0.343) is very similar to the DW estimated in an Australian burden of disease study concerning self-inflicted injuries (0.447), 13 indicating that our findings are very close to what has been measured and used in the past. In contrast, there is a very wide difference between the DWs of various poisonings, ranging from 0.022 for mild benzodiazepine abuse to 0.830 for severe aluminium phosphide used in a suicide attempt. So, it seems the DW for poisoning, whether or not it is involved in a suicide attempt, might vary from very low to relatively high based on the nature of the substance and the stage of the health condition after poisoning.
Otherwise, this study suggests that the disability stemming from a poisoning is largely attributable to the particular substance consumed/involved. When comparing the DW for poisonings with the DWs for injuries, this shows that some poisonings (e.g. moderate carbon monoxide = 0.300) are approximately as disabling as skull fracture (0.32) and cocaine dependence (0.33). 22 The DW for aluminium phosphide in even non-fatal suicide attempts starts from 0.600 and so is comparable with that of long-term stroke (0.539). 22 These DWs represent a wide range of rates comparable with those of injuries and bone fractures in terms of range. When comparing the DWs for acute poisonings, it becomes apparent that even an acute poisoning can be as disabling as chronic substance abuse, such as alcohol (0.549) and opium (0.64), in that it decreases the health status of the patient for a long time. 15 Non-fatal suicide attempts are a common cause of poisoning, especially in younger patients, and the DW for initial stage for such patients might be as low as that of a common cold or influenza (e.g. mild poisoning with acetaminophen). However, even in cases of survival, the patient might experience hepatic failure due to severe poisoning and so need liver transplantation, thereby reaching a DW of 0.737, which is much higher than that for the amputation of both legs (DW = 0.494). 15
Additionally, some researchers believe that sociality is co-morbid with or symptomatic of psychiatric disorders. 23 We also believe that suicidality should be accepted as a disorder that is accompanied occasionally by poisoning to become a co-morbidity. Of course, such poisoning might occur intentionally or unintentionally. So, in case of the former, perhaps we should consider the two illnesses together as a co-morbidity. 17
On the whole, much more empirical research is required to clarify and disentangle the co-morbidity of intentional poisoning in light of the DWs. At present, the most accepted model for dealing with co-morbidity assumes that the combination of two health states is equal to the multiplication of the DWs belonging to each of the component health states 12 :

It means that a child who unintentionally consumes acetaminophen tablets in a case of moderate poisoning (DW = 0.307) will be treated differently to when the same variety of poisoning occurred intentionally due to suicidal thoughts (DW = 0.36) with the score of:

As stated in the introduction to this article, DWs are an essential component for calculating DALYs and related metrics such as quality-adjusted life years. 24 So, wherever data are available on the necessary parameters, the DWs re-estimated in this study can be used to calculate DALYs for poisonings and, due to the high prevalence of poisoning, the estimated DALY will be more accurate and applicable than the general figure currently used. So, while using the unique DW, it would generate fixed rates for each variety of poisonings regardless of the type and severity of the clinical manifestations. Due to the aforementioned high prevalence of poisoning cases in general, this study confirms that using various DWs might provide more precise and sensitive rates of YLD, YLL and DALY than those associated with the former fixed DW.
Strengths and limitations
We can confirm validity of our findings for several reasons. First, the internal consistency of our panel was high, indicating good agreement among the experts. Second, a good level of external consistency was found. Furthermore, the similarity of the mean of our DW for poisonings with the single DW estimated in an Australian burden of disease study concerning self-inflicted injuries and poisonings 13 reinforces the reliability of our findings.
The limitations of this study include the relatively small panel of 10 experts, which resulted in broad 95% confidence intervals. Also, the fact that there is a lack of clear description or definition available for poisonings and their categories based on substance and the outcome is a limitation. Additionally, the DWs have been estimated by an expert panel, although it is also possible to generate a panel from a representative sample of the general population or people who have directly experienced the health state. Debate still exists as to the most appropriate population for health valuation. It is essential to understand that even using different kinds of panels may lead to different estimations of the DWs. Patient panels, for example, tend to rate health states better than the general public, 17 but sometimes worse than expert panels. 24 However, the level of agreement between expert panels and general public panels seems to be good. 17 We chose to use an expert panel in this study based on the fact that similar studies made use of expert panels. A final limitation might be the fact that the DWs have been generated in a middle income, eastern Mediterranean country, which limits the generalizability of the findings.
Footnotes
Acknowledgments
We would like to thank all our panellists for participating and collaborating with us. We also thank Mashhad University of Medical Sciences for supporting this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.