
Abstract
Background:
Acute poisoning is a common health problem worldwide. Traditionally, the frequency of admitted cases, number of deaths or online resources were used to measure the volume of this problem. In this study, the burden of acute poisoning is addressed for the first time.
Methods:
Data related to 44,340 poisoned patients from 2004 to 2013 were analysed. Two sources including hospital information and forensic medicine data of the Khorasan Razavi catchment area. The disability-adjusted life years (DALY) method – including years of life lost (YLL) and years lived with disability (YLD) – was used to estimate the burden.
Results:
In this period and for all acute poisonings, the mean (SD, minimum–maximum) incidence of acute poisoning was 30,485 (3049 per year). In total, 29,208 DALY were lost, including 8499 YLD and 20,709 YLL. DALY have increased from 1808 in 2004 to 4283 in 2013. Among the total DALY over this 10-year period, 17,592 (60%) were related to males. Narcotic use accounted for the largest percentage of DALY (19.6%), followed by analgesics–sedative use (16.3%) and illegal drug use (11.41%). The health loss due to these causes was large (YLD = 8499 and YLL = 20,709) and showed a rapidly increasing trend.
Conclusions:
Estimating DALY is more informative than using the frequency of death. If we expect the same ratio in the country, we would expect a DALY rate of 729,750 years for the 75,000,000 inhabitants of this country in this time period or 72,975 DALY lost per year for poisonings.
Keywords
Introduction
Acute intentional and accidental poisoning are worldwide health problems. 1 The number of poisonings has increased in recent decades in Iran. 2 In this country, the most common causes of poisoning include the use of narcotics, analgesics (e.g. benzodiazepines), nephrogenic syndrome of inappropriate antidiuresis, sedatives or carbon monoxide. Illegal drugs are the most common cause of poisoning through both intentional and unintentional use. 2,3 The national studies show an increasing trend in illegal drug poisoning and in poisoning-related mortality and morbidity. 1
The concept of disability-adjusted life years (DALY) was developed in the 1990s for the Global Burden of Disease (GBD) study. Details of the GBD study have been described by World Health Organization (WHO) 4,5 and widely used and replicated worldwide. 6 –9 The DALY concept describes the loss of healthy years of life, that is, the difference between actual and perfect health. It uses time units to estimate disease burden by combining years of life lost (YLL) due to premature mortality with years lived with disability (YLD) in incident cases. 4,5
In the present study, we endeavoured to estimate the acute poisoning burden in the northeast of Iran for the years 2004–2013 using an estimation method to account for the burden of both mortality and overall incidence and derive an estimate for national rates caused by poisoning. We also attempted to estimate the trend of these rates over 10 years and find estimates for national rates by combining the national studies data from 2004 and extending to the current rates. To our knowledge, there are no published studies considering the burden of poisonings in a single study and in detail. This study would be of international importance in considering the trend of poisonings as underestimated or ignored causes for loss of health. Since the early 1990s, in Iran, poisoning has overtaken traumas and accidents as the leading cause of death 1 with a rapidly increasing trend.
Methods
Hospital admissions and state forensic medicine mortality rates were used to quantify the poisoning burden, but these measures are often reported and analysed separately, so we attempted to merge, clean and reach the comprehensive data for our province. We also calculated the main substances causing mortality and/or morbidity based on the 10th revision of International Classification of Diseases (ICD-10) classification. Then, by comparing the urban/rural and total population proportion rate with national rates, we estimated the generalized outcome of our findings to national rates.
We calculated the DALY for acute poisoning using methods described in the GBD study, 4,5 which summed the YLL and YLD components using standard life tables introduced in the WHO website. 10 The basic formula is expressed as follows:

We computed YLL by multiplying the number of poisoning deaths by the number of years of expected remaining life at the respective age of death according to the standard life tables for the years 2004–2013, in which life expectancy at birth was 74 years for women and 72 years for men. We used this method for calculating YLL due to lack of data on other methods of life expectancy calculation. 11 Mortality data on acute poisonings for the years 2004–2013 were obtained from the referral medical toxicology services accepting all cases of the province and the state official centre for forensic medicine collecting state data on mortalities. Data were obtained from digital sources; however, to ensure accurate classification and measurements, random manual searches of the hard copies of recorded data were performed.
Next, we computed YLD by multiplying the number of acute poisoning incidents by both the average duration of poisonings (mainly 3-day hospital stays) as an acute cause of death/disability and a disability weight that reflected the severity of poisonings on a scale from 0 (perfect health) to 1 (death) derived from the 2012 GBD study. 12 We used average durations and disability weights for countries categorized by the most current GBD study. 4,5 We did not consider co-morbidities due to lack of data and lack of the possibility of follow-up due to the retrospective manner of the study. We did not consider the severity of poisoning in terms of disability for the same reason, and no particular disability weight was given according to the severity of the case. These measures were presented in terms of mean and range due to non-normality of the distribution of the variables.
Analyses were performed with Microsoft Excel 2007 including diagrams and also we used standard WHO life tables to calculate the health metrics measures used in this study based on the above formula.
Results
In total, 44,340 patients were studied, which include 43% males with a total mean age of 25 (ages ranging from 0 to 90 years) over a 10-year period. Data regarding YLD, YLL and DALY are presented in Table 1.
YLL, YLD, DALY and DALY in 100,000 population from 2004 to 2013 in northeast Iran.

YLL: years of life lost; YLD: years lived with disability; DALY: disability-adjusted lost years.
During this period, the annual frequency of acute poisoning among male patients increased from 2657 (52%) to 10,563 (43%), a fivefold increase. The annual frequency of deaths varied from 58 (70%) to 118 (64%) in the same period. These values are equal to a mean (range) incidence of 1.7 × 10−3 (0.92 × 10−3 to 3.2 × 10−3). These values are equal to a mean (range) death incidence of 3.5 × 10−5 (2 × 10−5 to 4.8 × 10−3). The mean (range) case fatality rate has decreased from 21 × 10−3 to 11 × 10−3 in this period (Table 1).
The mean (minimum–maximum) YLD was 850 (457–1850), the YLL was 2071 (1351–2442) and the DALY was 2921 (1808–4739) in both sexes from 2004 to 2013. Correspondingly, YLL, YLD and DALY rose from 1351, 457 and 1808 to 2442, 1833 and 4275 from 2003 to 2014, respectively. The DALY per 100,000 increased from 60 to 140. This is shown graphically in Figure 1.

Health metric measures of acute poisonings in northeast Iran during 2004–2013.
The poisoning burden was greatest in women due to suicide attempts, which accounted for almost 40% of total DALY. Poisoning causes the loss of 6105 DALY at ages 15–29, followed by the age range of 30–44 years with 2522 DALY lost. DALY per 1000 women for all poisonings combined was 0.79 years. The highest DALY values per 1000 women started at 0.5 in 2004 and then rose to 1.3 in 2013.
In men, the burden was greatest for overdosing and drug abuse due to dependence on the substances. The largest loss was found in the 15–29 age range (7644 DALY). DALY per 1000 men rose from 0.8 in 2004 to 1.5 in 2013. In general, DALY per 1000 in both genders ranged between 0.4 and 1.7 years for all poisonings combined, among which the highest values were 1.7 a year per 1000 for 2013 and 0.6 a year per 1000 for 2004 (Table 1).
Table 2 shows estimated DALY, YLL and YLD for poisonings in the northeast of Iran for the years 2004–2013 as 17,592 years in men and 11,598 years in women. YLL contributed to more than 70% of total DALY.
YLL, YLD and DALY for poisonings in 2004–2013 for standard age groups.
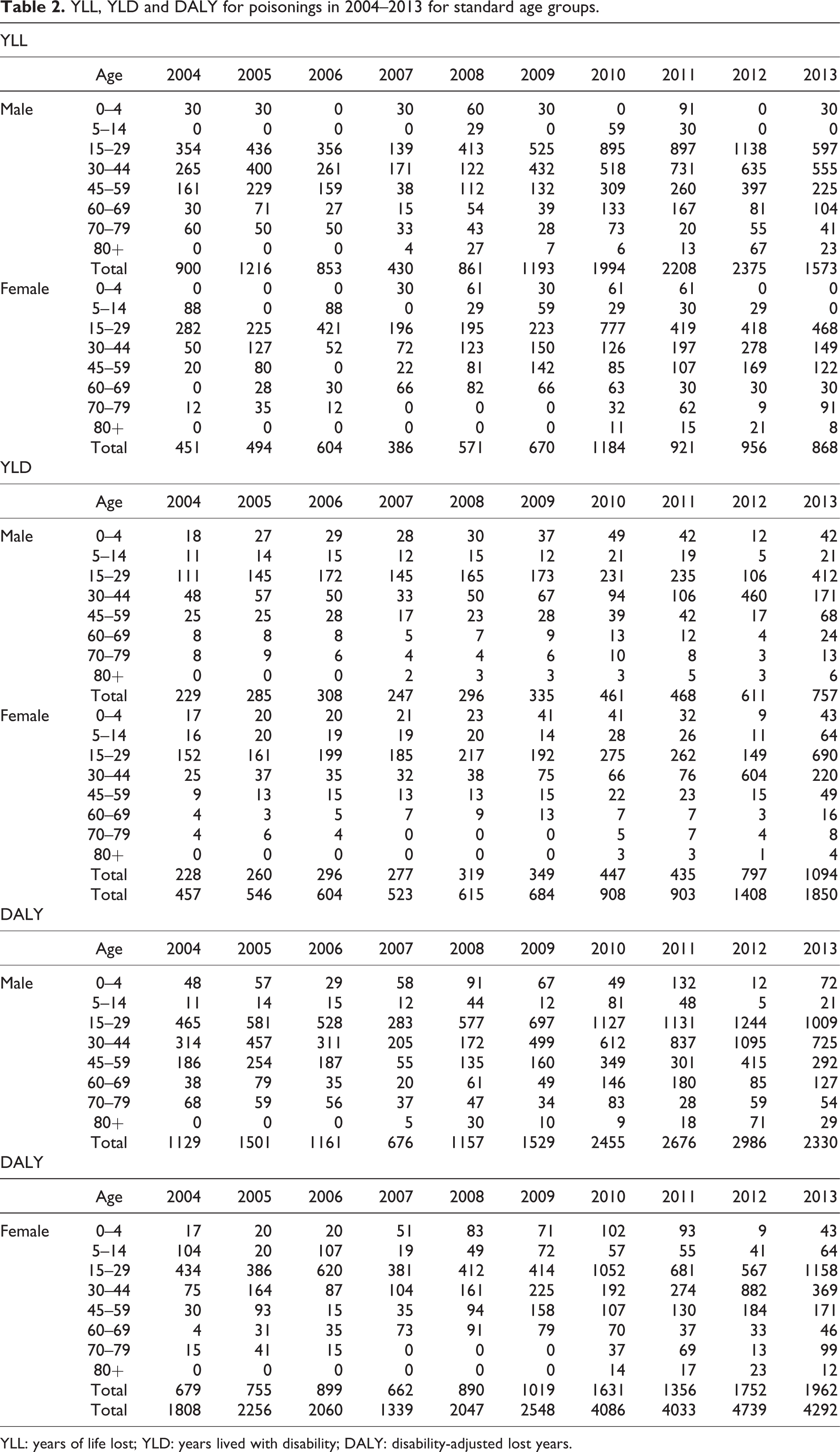
YLL: years of life lost; YLD: years lived with disability; DALY: disability-adjusted lost years.
In terms of substance abuse, Figure 2 shows the incidence during 10 years. The non-opioid analgesics group was the most prevalent ICD-10 group in terms of poisoning. In terms of mortalities, narcotics and psychodysleptics, or central nervous system (CNS) affecting substances in general, accounted for the largest proportions of the burden (Figure 3).
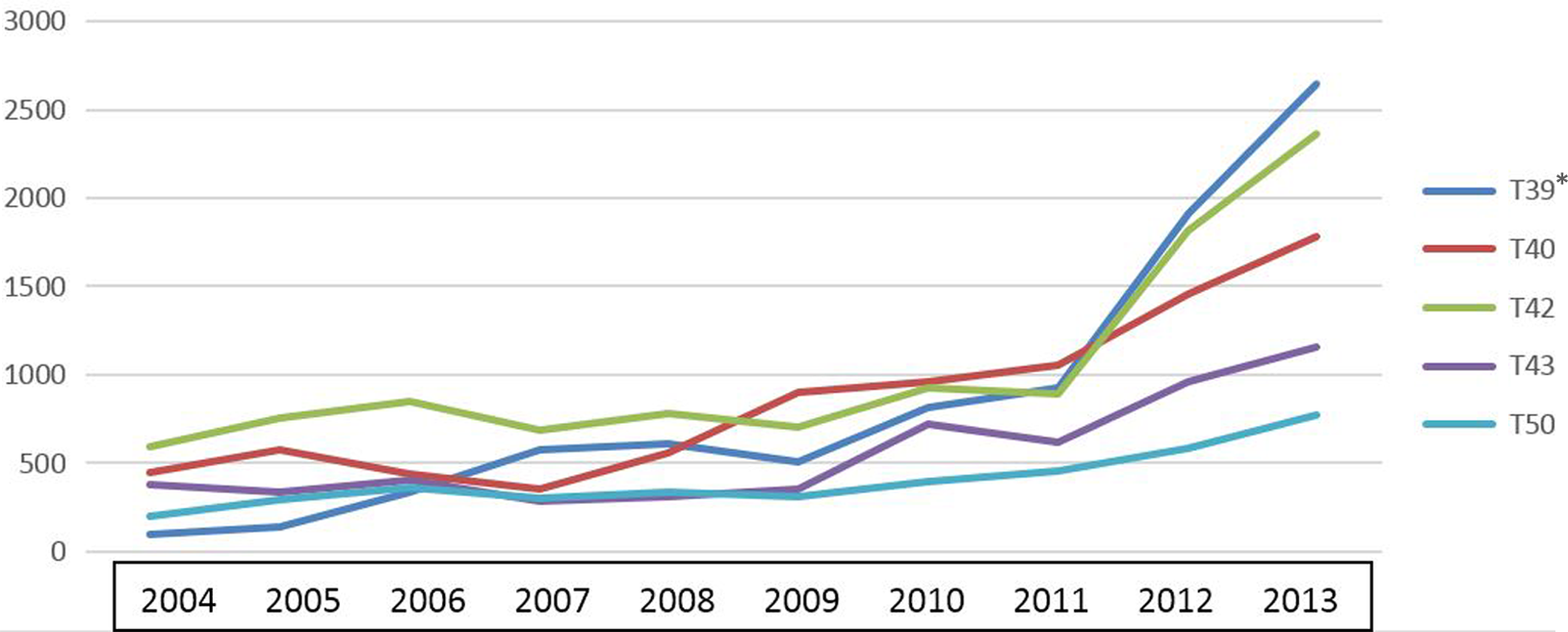
Trend of incidences due to acute poisonings during 2004–2013 (Mortalities excluded, presented in Figure 3). *ICD-10 codes for Poisonings.
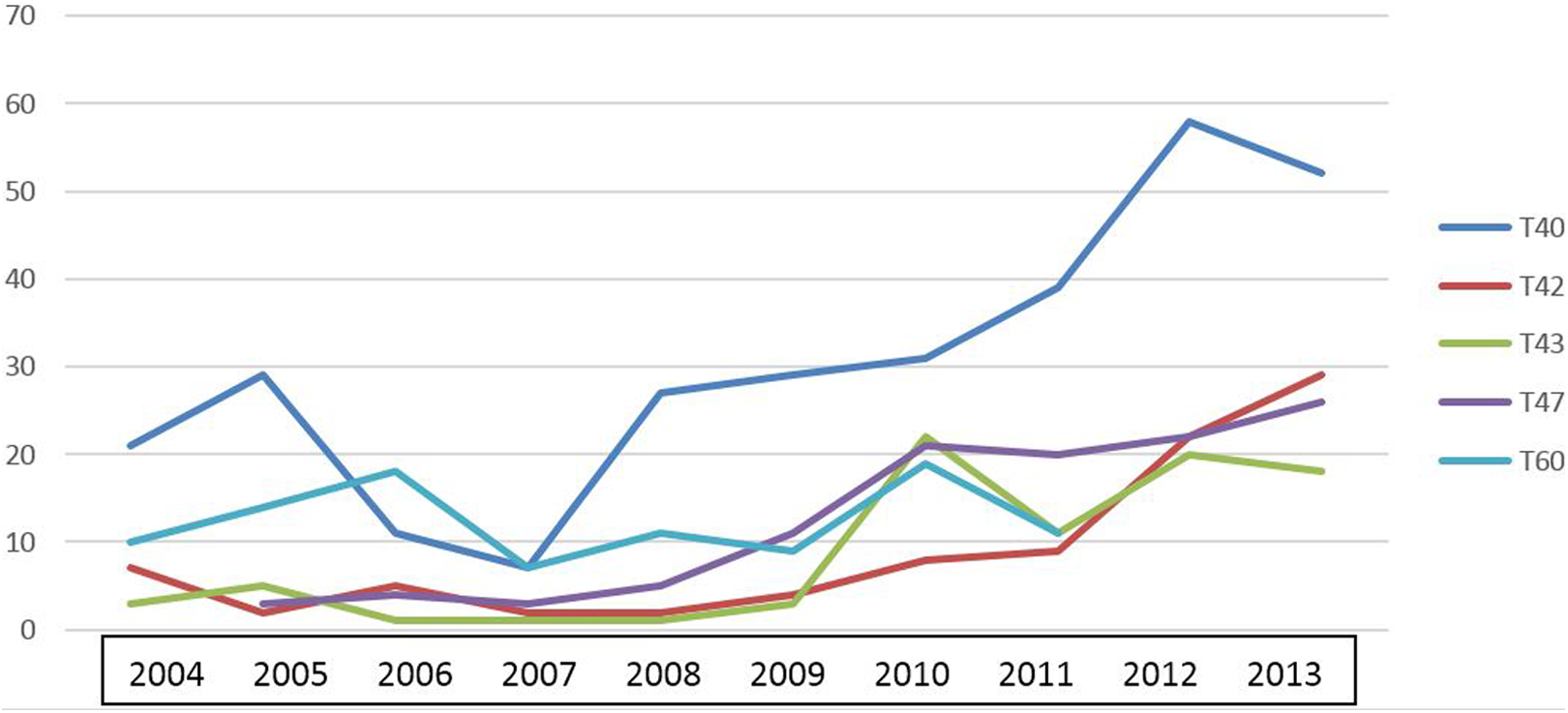
The trend of mortalities based on substance groups during 2004–2013.
Table 3 shows the incidence of substance abuse in general with four main groups, namely pharmaceuticals, chemicals, natural toxins and unknowns, respectively, having the largest incidence rate. These estimates were made within the 2004–2011 time span because in the last 2 years of the study, the classification methods of our authorities were summarized and modified, so we omitted them to be able to compare the most prevalent categories with each other. During this time, the most prevalent groups were the pharmaceuticals, affecting 23,998 incidents or about 85% of all cases. Within the aforementioned groups, CNS-affecting medicines, illegal drugs and pesticides (a subclass of the chemical group) were the most prevalent subgroups.
The abused substances based on type and frequency in total and in gender during 2004–2011.a

CNS: central nervous system; NSAID: nonsteroidal anti-inflammatory drug.
aCoding method has been modified in two recent years, so these 2 years were omitted to have comparable data in the rest of the time period.
bPercent in total.
cPercent in subgroup.
dPercent in sub-subgroup.
Discussion
We estimated the poisoning burden in Iran for the years 2004–2013 by using DALY to account for the burden of both poisoning incidence and mortality. During these years, we estimated that about 29,190 years totally or an average of 2919 years per year were lost. The trend shows a 238% increase in incidence during these 10 years. This occurred whilst the general population in this area had just about 10% increment.
A national study of the disease burden in Iran was published by the Ministry of Health and the National Center for Health Metrics in 2004. In this publication, DALY was reported as 21,572 years per 100,000 people in total. Among these DALY lost, 28% were due to injuries. Injuries accounted for the highest rate of loss in male patients, with injuries (intentional or unintentional) causing a total of 2.789 million years lost (Figure 4). 12

DALY during 2004–2013 adjusted for population based on standard age groups. DALY: disability-adjusted life years.
The same study – which was conducted in six provinces with different geographic and population demographics – reports that intentional and unintentional injuries have the same rank in DALY. Because Khorasan – which is reported on in our study – is one of these provinces, it can be assumed, with an acceptable rate of uncertainty, that our findings will help predict the poisoning burden for the rest of the country.
Based on the latest national statistics, Iran had 75,000,000 inhabitants in the middle course of our study; therefore, if we assume approximately the same rate of DALY for the population of the entire country, based on our regional data, DALY will reach about 749,210 in 10 years. That means 74,921 DALY per year or about 97.3 DALY per 100,000 people for acute poisonings. In 2004, the national study reported about 5,971, 1,310, and 904 years lost per 100,000 people due to all injuries, ischaemic heart diseases, and major depressive disorders, respectively. 12
In the same study, there is no category for poisonings. However, our estimated rate for the country falls between two categories in that publication, including ‘unintentional poisoning with substances, smokes and gases’ and ‘suicide and self-harm’ with 53,950 (81.1 per 100,000) and 137,147 (206.2 per 100,000), respectively. Therefore, we expect that from 2004, the same ratio of increase in measures of poisonings nationwide has been happening. 12
As previously stated, there are neither national studies nor global studies considering the burden of poisonings in detail. However, in 2012, a study was published considering the rate of DALY for various diseases and including poisonings from 1990 to 2010. At this time, the DALY of poisoning in global estimates varied from 11,151 to 8934 (in thousands). This indicates a decreasing trend of 19%. 13
The national 2003 study showed that 0.5% of total DALY are attributable to poisonings. However, that study also reported 1.3% of DALY attributed to self-inflicted injuries that include suicidal attempts, a category that might include some of the reported poisonings (intentional ones). This is why our study estimated that poisonings account for 0.46% of the total DALY. 13,14
However, if we assume that the increasing trend in our country will be followed at the global level, we should expect a 200% increase in the global rates from the past 10 years, although this is not possible to confirm. The DALY lost due to poisoning alone have been 7447 for both sexes. A worldwide 2014 study performed by the Institute for Health Metrics and Evaluation in Washington, DC, USA was published in The Lancet journal. This study does not report the DALY of poisoning for 2014, but the relevant mortality is reported at about 1,202,000 and 980,000 in 1990 and 2013, respectively, with a 12.7% decline in rate. This is in a wider range than our time span, but it is generally contrary to our findings, and we observed at least a twofold increase in the rate of DALY related to poisoning. 14
In a 2004 study, a 3:2 male to female ratio of DALY is reported. In our study, this ratio was approximately the same rate of 60.3 versus 39.7, that is, about 3:2. In the 2014 data, the male to female ratio is not reported for specific causes. 15 The difference in gender rates might be due to different methods used in coping with the problems (16).
In our study, the most prevalent age group for poisoning was 15–29, followed by 30–44 in both sexes and also in both YLL and YLD and so DALY. These groups had rates of 9841 (47%), 3023 (35%) and 12,864 (44%) YLL, YLD and DALY during 10 years, respectively. This shows that the largest burden of disease is given to the youngest and most active members of the population, so considering policies to reduce or better manage patients would have a large impact on social well-being. Again, here we should emphasize that due to short follow-up (just during the hospital stay period) for patients who psychologically cannot be considered healthy, the YLD of these patients might be much more than it appears when based solely on the length of hospital stay. Perhaps some age groups were poisoned more frequently due to the higher percentage of substance abusers in these age groups or more life stressors due to being in active age of life.
The most commonly abused substances are those affecting the CNS. Women primarily suffer from an overdose of medicines in suicide attempts, and men are primarily affected by overdose of illegal drugs or medicines with abuse potential. Many of the patients (especially those attempting suicide) have consumed multiple medicines that, based on ICD coding structure, they were encoded in the substance with the highest dose, or more threatening substance group. However, we suspect that health loss due to several substances is worse than health loss due to a single agent, and it might be better considered as co-morbidity. 16,17,18
Limitations
Because we have been collecting pre-recorded data from centres for the past 10 years, during this time period, some variations in coding and recording have been encountered, which leads to uncertainty and a significant probability of systematic errors. Because our final findings are in accordance with some other literature – including national and global studies – we believe that these errors have not seriously affected the findings and outcomes in general, although there are some limitations that are listed here.
Children between 0 and 14 years of age have continuously been coded within poisoning and paediatrics departments; therefore, despite our efforts to minimize mismatched or overlapping data, some uncertainty for including all poisoned young patients is expected. This uncertainty might cause the rates of these categories to vary by up to 5%. Our estimation of mortality rates for 20- to 35–year-old males seems to be another limitation. Our preliminary manual search of the records led to a higher expected rate than what is reported. This is especially problematic because some mortalities are not referred to hospitals. These mortalities include those found dead at home (e.g. poisoned by carbon monoxide) or outside (e.g. homeless addicts). To cover these mortalities, we attempted to collect forensic medical data, which records all deaths, especially suspicious ones. However, because some of the deceased are not referred to legal authorities but instead buried by relatives in regional areas (e.g. rural areas or marginal urban resorts), we expect some data loss due to these issues as well.
Finally, as in our study, the short-term YLL were calculated. Problems occurring outside of the hospital – such as complications due to consumption of poisonous substances or therapeutic modalities, after discharge problems, including the psychological impact of suicide attempts, family relationships and other relationships during the post-event period, and the continuum of the conditions leading to suicide attempts – were not taken into account.
Conclusion
Based on these local data, it seems that poisonings contribute a substantially large burden to the health of the population – at least in our society – with an increasing trend that is concerning. This burden is especially and increasingly affecting the younger and more active members of the population.
Footnotes
Authors’ note
The first author collected the data and under supervision of the second author did the statistical measurements. The manuscript was read by both authors and approved.
Acknowledgements
We thank our colleagues who participated in data gathering, data cleaning and providing access to data. We also thank the Mashhad University of Medical Sciences for funding and supporting the current study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.