
Abstract
Doxorubicin (DOX) is used in the treatment of cancer. However, cardiotoxicity is its major dose-limiting factor. Mechanism of DOX–cardiac toxicity is not completely elucidated. The aim of the current study was to explore whether the addition of subeffective dose of curcumin (100 mg/kg) to nebivolol would produce a better impact in treating DOX-induced cardiac toxicity in comparison with monotherapy.
Male rats were used and subdivided into seven groups. Cardiac toxicity was induced in 6 groups by intraperitoneal injection of DOX over 23 days; of the six groups, five groups were treated with curcumin (100 and 200 mg/kg), nebivolol (1 and 2 mg/kg), and their combination; the sixth group was the control group used for comparison.
Oral administration of curcumin and/or nebivolol attenuated DOX cardiotoxicity as manifested by increasing survival rate, improvement in body weight, heart index, and ECG parameters, increase in ventricular isoprenaline responses, and improvement in cardiac enzymes, oxidative stress, apoptosis, and histopathological picture. The addition of the current low subeffective dose of curcumin to nebivolol ameliorated DOX cardiac toxicity to a much greater extent than monotherapy showing better antioxidant and antiapoptotic effects versus the per se effect of nebivolol. Therefore, the current study encourages adding low dose of curcumin to potentiate the effect of nebivolol in the clinical management of cardiac toxicity improving the patients’ quality of life if proper clinical safety data are available.
Introduction
Clinical uses of doxorubicin (DOX) are often limited by its cardiotoxicity. 1 Initial acute adverse effects, including hypotension and transient electrocardiographic abnormalities, are reported in up to 41% of patients. The chronic adverse effects, mostly in the form of dose-dependent cardiomyopathy, account for about 50% mortality within 2 years after diagnosis. 2
Previous studies have demonstrated that antioxidant compounds have cytoprotective effects in DOX-induced cardiac toxicity. 3,4 In spite of the effectiveness of some antioxidants such as vitamin E and N-acetylcysteine, they failed to eliminate oxygen radicals clinically. 5
Curcumin is the yellow pigment of turmeric in curry, and it is derived from the plant Curcuma longa. It has been reported that it is useful in protecting against myocardial injury and preservation of cardiac function. 6 In addition, curcumin has multiple therapeutic activities that block the hepatic and renal toxicities induced by DOX, and it also possibly acts as a free radical scavenger. 4,7 Moreover, 3,5-bis(4 fluorobenzylidene)-1-[(2,2,5,5-tetramethyl-2,5-dihydro-1-hydroxy-pyrrol-3-yl)methyl] piperidin-4-one (HO-3867), a synthetic curcumin analog, has been shown to exhibit both anticancer and cardioprotective effects, indicating that combination treatment of HO-3867 and DOX is a viable option for treatment of cancer with reduced cardiotoxic side effects. 8
Nebivolol, a third-generation β-adrenoreceptor blocker (βB), is able to stimulate endogenous production of nitric oxide (NO) by inducing phosphorylation of the endothelial NO synthase (eNOS). 9 Whereas nebivolol action on NO can result in favorable outcomes at vascular levels, its effects on the heart are not so straightforwardly beneficial.
Previous studies have reported that βBs prevent the development of cardiac toxicity induced by anthracyclines in rats in the isolated perfused rat heart and in patients receiving anthracyclines. 10,11
Despite extensive research, the mechanism of DOX-induced cardiac toxicity is still not completely elucidated. Further experimental studies and clinical trials are warranted to investigate the mechanisms of beneficial effects. 12
Based on the above requirement, the present work was designed to elucidate the possible protective effects of curcumin and nebivolol. This study aimed to explore whether their combination—in low doses—will be more beneficial in treating DOX-induced cardiac toxicity in rats versus monotherapy. Positive results may lead to suggestion of a more effective treatment that limits the side effects produced by using high doses of monotherapy.
Materials and methods
Animals
The experiment was carried out using 84 male Wistar rats weighting 180–200 g purchased from The Egyptian Organization for Biological Products and Vaccines. Rats were housed in well-ventilated polypropylene cages with food and tap water ad libitum. Rats were maintained at controlled laboratory conditions of normal light and dark cycle and temperature (25 ± 2°C) and allowed to acclimatize for 1 week. All experimental procedures were carried out according to the Guidelines of Animal Care and Use Committee, Faculty of Medicine, Suez Canal University, Egypt.
Drugs and chemicals
DOX (Pharmacia and Upjohn, Italy), nebivolol, isoprenaline (Sigma-Aldrich Chemicals, Germany), and curcumin (Sekem’s Company, Egypt) were dissolved in normal saline. All chemicals and solvents were of analytical grade.
Experimental design
Rats were weighed and assigned to 7 groups with 12 animals in each group. DOX and normal saline were given by intraperitoneal (i.p.) injection, while curcumin and nebivolol were given periorally.
Group 1 received normal saline (every other day for 23 days) parallel to DOX. Cardiac toxicity was induced in the rest of animals by i.p. injection of DOX in 12 equal injections (each containing 1.5 mg/kg) every other day for 23 days to achieve an accumulative total dose of 18 mg/kg. 10
Group 2 received DOX and treated with normal saline daily; groups 3 and 4 received curcumin at doses of 100 and 200 mg/kg/day for 30 days, starting 1 week before DOX; 13 groups 5 and 6 received nebivolol at doses of 1and 2 mg/kg/day for 23 days, starting from the day of DOX administration; 14 and group 7 received a combination of curcumin (100 mg/kg/day) and nebivolol (1 mg/kg/day).
At the end of the experiment, body weights (BW) were reassessed, and the percentage change of BW was calculated using the following equation:

Survival rate was observed daily throughout the study.
Determination of ECG
Using MP150 data acquisition system (BIOPAC Systems Inc., Santa Barbara, California, USA), 48 h after the last DOX injection, the electrocardiography (ECG) was recorded for each rat to measure the following parameters: heart rate (HR) in beats per minute, QRS, ST, and QT intervals in milliseconds, ST segment, T wave changes, and arrhythmia.
While recording the ECG, ventricular arrhythmia (VA) was assessed according to the Lambeth Convention; also, ventricular premature beats (VPB), ventricular tachycardia, and ventricular fibrillation were recorded. 15
After ECG, blood samples were collected, via retro-orbital bleeding, for plasma and serum separation and stored at −80°C for further analysis.
The isolated Langendorff heart
Rats were received i.p. injection of heparin sodium 5000 IU/kg, anesthetized using ether inhalation, and killed by cervical decapitation.
16
The hearts were excised, weighed, and heart index was calculated using the following equation:

The hearts were then placed in ice-cold modified Krebs–Henseleit buffer solution and immediately cannulated in the retrograde mode according Langendorff’s technique. 17 The amplitude of ventricular contractions (inotropic effects), HR (chronotropic effects) as well as concentration response curves were recorded in response to variable isoprenaline concentrations (3, 6, and 12 µM/L) on PowerLab MP150 data acquisition system (AD Instruments Pty Ltd, Castle Hill, Australia) trough transducer connected by a hook to the apex of the heart. 18 Hearts were then kept in −80°C until biochemical analyses.
Determination of cardiac biomarkers
Plasma was prepared for estimating the cardiac troponin I concentration using VIDAS® Troponin-I Ultra assay (bioMérieux Inc., Durham, North Carolina, USA). Moreover, sera were used for the estimation of cardiac enzymes, creatine phosphokinase (CPK), and creatine kinase MB (CK-MB) using Stanbio™ kit (Boerne, Texas, USA) as described previously by Rosalki and Würzburg et al. 19,20
Determination of cardiac oxidative stress markers, MDA levels, GPx and SOD activities
Apart of the heart (0.1 g) was ice-cooled, homogenized in 1 mL phosphate buffer, and centrifuged at 3000g for 15 min. The supernatant was collected, and MDA levels 21 and GPx and SOD enzymes activities were measured as described previously. 22,23
Assay of total nitrite in cardiac tissue homogenate
Total nitrite concentration was measured as an indicator for NO production. 24 Assay kits were purchased from Bio-diagnostic® (Cairo, Egypt), and the colorimetric assays were performed using an ultraviolet–visible spectrophotometer (UV-1601-PC, Shimadzu, Tokyo, Japan).
Assessment of mtDNA integrity
Isolation of mitochondria
Heart tissue (100 mg) was homogenized in 0.25 M sucrose in 0.7 M tris(hydroxymethyl)aminomethane (Tris)–hydrochloric acid buffer. Tris–sucrose ethylenediaminetetraacetic acid (EDTA) was added to aid disruption of cells. Tissue homogenate was spanned at 2500g for 10 min to remove unbroken cells. Supernatant fluid was decanted into centrifuge tubes and spanned at 10,000g for 10 min. The pellet is gently resuspended in 10 mL Tris–sucrose buffer for washing. This washing cycle was repeated to improve the degree of mitochondrial purity. 25
Isolation of mtDNA
Mitochondrial DNA (mtDNA) was isolated using a kit from BioVision (Milpitas, California, USA). Samples were subjected to 1% agarose gel electrophoresis at 4 V/cm using 40 mM Tris–acetate and 1 mM EDTA as a running buffer. mtDNA quantity and purity were determined using NanoDrop™ 1000 spectrophotometer V3.7 (Thermo Fisher Scientific Inc, Wilmington, Massachusetts, USA). 26
DNA laddering assay
Genomic DNA was extracted from the heart tissue using Wizard® Genomic DNA kit (Promega Corporation, Madison, Wisconsin, USA). DNA was then loaded on agarose gel (15 μg/lane). DNA laddering was determined by constant voltage mode electrophoresis (4 V/cm, for 4 h) on a 1.5% agarose gel. A 1-kbp ladder (Sigma, St Louis, Missouri, USA) served as DNA base pair marker. 27 Gels were stained with 0.5 μg/mL ethidium bromide and visualized using G: Box Gel Documentation system (Syngene, Los Altos, California, USA).
Histopathological examination
The rest of hearts were preserved for 24 h in 10% neutral-buffered formalin solution. After fixation, 5 μm thick sections were cut from the ventricle and stained with hematoxylin and eosin for examination and graded under light microscope (model BX-50, Olympus Corporation, Tokyo, Japan).
Histopathological changes were used to grade cardiac injury on a scale of 1–3, 28 that is, 1 = < 5% of injured cells grade, 2.5 = 15 – < 35% grade, and 3 = > 35% grade. The grade of cardiac toxicity was scored blindly by examining six randomly chosen fields per sample at a magnification of 40×.
Statistical analysis
Data was expressed as mean ± SEM and analyzed using Statistical Package for Social Sciences program Version 20 (SPSS Inc., Chicago, Illinois, USA). Comparisons among groups were carried out using one-way analysis of variance followed by Duncan’s multiple comparison test for significance difference among groups. 29 Statistical analysis for histological data with non-Gaussian distribution were performed by Kruskal–Wallis test followed by Duncan’s test. Two-tailed value of p < 0.05 was considered statistically significant.
Results
Percentage change in BW, heart index, and survival rate
DOX resulted in a significant decrease in percentage change of BW (−8.1 ± 1.47%) versus (13.2 ± 1.13%) in the control group ( p < 0.05; Table 1).
Effect of curcumin and nebivolol on percentage change of body weight, heart index, and survival rate in DOX-treated rats.

ANOVA: analysis of variance; combination: curcumin 100 mg/kg + nebivolol 1 mg/kg; DOX: doxorubicin.
Data was expressed as mean ± SEM and analyzed using one-way ANOVA followed by Duncan’s post hoc test. n = 7–12.
a p < 0.05 versus control group.
b p < 0.05 versus DOX group.
c p < 0.05 versus curcumin 100 mg/kg group.
d p < 0.05 versus curcumin 200 mg/kg group.
e p < 0.05 versus nebivolol 1 mg/kg group.
g p < 0.05 versus nebivolol 2 mg/kg group.
Administration of curcumin 200 mg/kg, nebivolol as well as combination therapy resulted in a significant increase in percentage change of BW versus DOX ( p < 0.05).
Heart index in DOX-treated rats was significantly decreased (0.39 ± 0.01%) versus controls (0.58 ± 0.04%; p < 0.05; Table 1). Heart index values in nebivolol groups, either alone or in combination, were increased in comparison with DOX group ( p < 0.05).
Control group showed 100% survival rate, whereas DOX group showed a significant lower survival rate (58.3%). Larger dose of curcumin and nebivolol significantly increased the survival rate when compared with DOX group ( p < 0.05). The combination therapy showed 100% survival rate. The combination therapy improved BW percentage change and heart index significantly as compared to monotherapy.
Electrocardiogram changes
HR, PR, QT, and ST intervals
Figure 1(a) shows normal ECG trace recorded in normal rats. Figure 1(b) shows sinus tachycardia; Figure 1(c) showed prolonged QT and ST intervals and ST segment depression, while Figure 1(d) shows ST segment elevation.

ECG recording traces; showing normal (a), sinus tachycardia (b), prolonged QT and ST intervals and depressed ST segment (c), elevated ST segment (d). Heart rate (e), PR, QT, and ST intervals (f) in study groups. Data were expressed as mean ± SEM. n = 7–12. † p < 0.05 versus control group; ‡ p < 0.05 versus DOX group; $ p < 0.05 versus curcumin 100 mg/kg group; *p < 0.05 versus curcumin 200 mg/kg group; || p < 0.05 versus nebivolol 1 mg/kg group; and ¶ p < 0.05 versus nebivolol 2 mg/kg group. ECG: electrocardiography; bpm: beat per minute; ms: millisecond; DOX: doxorubicin; Cur: curcumin; Neb: nebivolol; combination: curcumin 100 mg/kg + nebivolol 1 mg/kg.
DOX group showed a significant increase in HR (444.6 ± 4.09 beats/min) versus control group (287.33 ± 9.35 beats/min). Curcumin 200 mg/kg and nebivolol (1 and 2 mg/kg) induced a significant decrease in HR (353.66 ± 2.15, 364.76 ± 5.02, and 325.49 ± 7.65 beats/min, respectively) versus DOX group ( p < 0.05; Figure 1(e)). Notably, the higher doses of curcumin and nebivolol resulted in a significant decrease in HR compared with the lower doses ( p < 0.05). Combination therapy could normalize HR significantly when compared with monotherapy ( p < 0.05).
Figure 1(f ) shows QT, ST, and PR intervals in study groups. DOX induced a significant increase in QT and ST intervals to 59.5 ± 1.34 and 19.7 ± 1.67 ms, respectively, and a significant decrease in PR interval to 22.33 ± 0.23 ms when compared with the control group (42.0 ± 0.68 and 10.0 ± 0.37 ms and 27.34 ± 0.45 ms, respectively, p < 0.05).
Curcumin 200 mg/kg induced a significant decrease in QT and ST intervals and a significant increase in PR interval when compared with DOX group ( p < 0.05). Nebivolol-treated rats, alone or combined, showed a significant decrease in QT and ST intervals and a significant increase in PR interval compared with DOX group without dose–response significant effect ( p < 0.05).
Duration of QRS complex, percentage of ST segment shift, VA and T wave changes
Figure 2(a) to (c) shows ECG recording traces of VPB, VT, abnormal Q wave as well as T wave changes. Duration of QRS complex in DOX group was significantly decreased (28.3 ± 0.92 ms) versus control group (34.3 ± 1.82 ms; p < 0.05; Figure 2(d)).
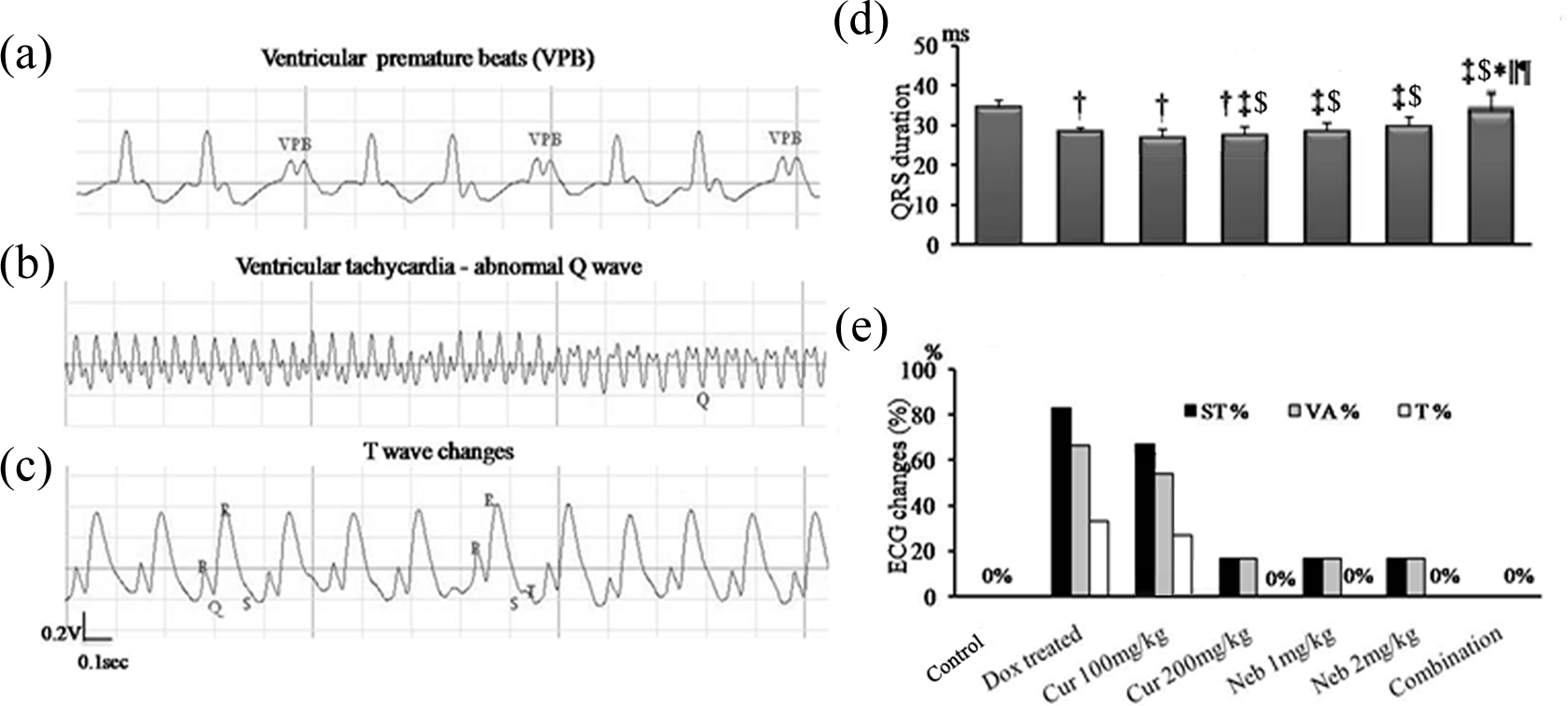
ECG recording traces for ventricular premature beats (a), ventricular tachycardia and abnormal Q waves (b), T wave changes (c) in DOX group, QRS duration (d), percentage changes in (ST segment shift, ventricular arrhythmia, and T wave changes) (e) in study groups. Data were expressed as mean ± SEM. n = 7–12. † p < 0.05 versus control group, ‡ p < 0.05 versus DOX group; $ p < 0.05 versus curcumin 100 mg/kg group, *p < 0.05 versus curcumin 200 mg/kg group, || p < 0.05 versus nebivolol 1 mg/kg group, and ¶ p < 0.05 versus nebivolol 2 mg/kg group. ECG: electrocardiography, ms: millisecond, DOX: doxorubicin; Cur: curcumin; Neb: nebivolol; combination: curcumin 100 mg/kg + nebivolol 1 mg/kg.
Curcumin 200 mg/kg and nebivolol induced a significant increase in QRS duration (37.2 ± 1.45 ms) compared with DOX and control groups, while combination therapy normalized QRS duration ( p < 0.05).
DOX induced about 83.3% ST segment shift and 66.7% VA (VPB or tachycardia). ST segment shift and VA percentages were significantly reduced to be 16.7% in curcumin 200 mg/kg and nebivolol groups as compared to DOX group ( p < 0.05; Figure 2(e)). DOX showed 33.3% T wave changes. However, no T wave changes were found in all other groups. Strikingly, no ST segment shift, VT, or T wave changes were found in the combination group.
Chronotropic and inotropic responses to isoprenaline concentrations (3, 6, and 12 µM/L) in Langendorff-perfused rat hearts
Figure 3(a) shows traces of the chronotropic and inotropic responses to various isoprenaline concentrations in Langendorff-perfused rat hearts in different groups.

Traces of the chronotropic and the inotropic responses to various concentrations of isoprenaline (3, 6, and 12 μM/L) in Langendorff perfused rat hearts (a), chronotropic (b) and inotropic (c) responses to various concentrations of isoprenaline in Langendorff perfused rat hearts in study groups. Data was expressed as mean ± SEM. n = 7–12. † p < 0.05 versus control group, ‡ p < 0.05 versus DOX group, $ p < 0.05 versus curcumin 100 mg/kg group, *p < 0.05 versus curcumin 200 mg/kg group; || p < 0.05 versus nebivolol 1 mg/kg group, ¶ p < 0.05 versus nebivolol 2 mg/kg group. bpm: beat per minute, DOX: doxorubicin, Cur: curcumin, Neb: nebivolol, combination: curcumin 100 mg/kg + nebivolol 1mg/kg.
Figure 3(b) shows ventricular chronotropic responses to different isoprenaline concentrations in Langendorff-perfused hearts. Ventricular chronotropic responses in DOX group were (65.7 ± 0.70, 65.7 ± 0.69, and 70.2 ± 0.35 beats/min) in 3, 6, and 12 µM/L isoprenaline concentrations, respectively. These measures were significantly decreased when compared with those in the control group (144.1 ± 0.88, 144.3 ± 0.67, and 147.1 ± 0.01 beats/min, respectively; p < 0.05).
Curcumin 200 mg/kg and nebivolol in different doses resulted in a significant increase in the ventricular chronotropic responses when compared with DOX and curcumin 100 mg/kg groups ( p < 0.05).
The effect of nebivolol was significantly dose dependent ( p < 0.05). Combination therapy induced a significant improvement in the ventricular chronotropic response compared with DOX group and monotherapy ( p < 0.05).
Figure 3(c) showed ventricular inotropic responses to different concentrations of isoprenaline (3, 6, and 12 µM/L) in Langendorff-perfused rat hearts in study groups. The ventricular inotropic responses were significantly decreased in DOX group (4.48 ± 0.09, 4.61 ± 0.06, and 4.67 ± 0.00 g, respectively) compared with the control group (7.93 ± 0.10, 9.68 ± 0.15, and 10.79 ± 0.11 g, respectively; p < 0.05). Curcumin 200 mg/kg or nebivolol resulted in a significant increase in the ventricular inotropic responses to all isoprenaline concentrations when compared with DOX and curcumin 100 mg/kg groups ( p < 0.05). Combination therapy resulted in significant increase in ventricular inotropic response compared with DOX group and monotherapy ( p < 0.05).
Biomarkers of cardiotoxicity
Troponin I concentration showed a sharp nine-fold increase, while CPK activity was tripled and CK-MB activity was doubled in DOX-treated animals; this indicated DOX–cardiac injury (Table 2).
Effect of curcumin and nebivolol on plasma troponin I and serum CPK and CK-MB activities, in DOX-treated rats.

CPK: creatine phosphokinase; CK-MB: creatine kinase MB; combination: curcumin 100 mg/kg + nebivolol 1 mg/kg; ANOVA: analysis of variance; DOX: doxorubicin.
Data was a expressed as mean ± SEM and analyzed using one-way ANOVA followed by Duncan’s post hoc test. n = 7–12. a p < 0.05 versus control group.
b p < 0.05 versus DOX group.
c p < 0.05 versus curcumin 100 mg/kg group.
d p < 0.05 versus curcumin 200 mg/kg group.
e p < 0.05 versus nebivolol 1 mg/kg group.
g p < 0.05 versus nebivolol 2 mg/kg group.
In contrast, curcumin 200 mg/kg, nebivolol as well as the combination regimen induced a significant reduction ( p < 0.05) in troponin I and cardiac enzyme activities in rats exposed to DOX. There were insignificant differences in the cardiac markers activity between different doses of nebivolol and larger dose of curcumin.
Combination therapy resulted in normalization of troponin I and a significant decrease in serum CPK (213.3 ± 1.22 IU/L) and CK-MB activities (48.8 ± 4.0 IU/L) in comparison with the DOX group and monotherapy ( p < 0.05; Table 2). This suggests that the former protective treatments significantly antagonized DOX toxic effect on troponin I plasma level.
Biochemical markers of oxidative stress
To investigate the effect of DOX-evoked oxidative stress, we determined MDA levels and GPx and SOD activities. Table 3 indicated that myocardial MDA level in rats that received DOX showed significant increase (130.88 ± 6.03 nM/g tissue), while GPx and SOD activities were significantly decreased (5.25 ± 0.44 and 10 ± 1.99 U/g) compared with the control (30.10 ± 0.50 nM/g tissue) and (19.45 ± 1.31 and 84.65 ± 4.45 U/g), respectively ( p < 0.05).
Administration of curcumin 200 mg/kg and nebivolol significantly ameliorated these parameters, while combination therapy normalized them ( p < 0.05).
Effect of curcumin and nebivolol on oxidative stress parameters; MDA concentration, GPx, and SOD activities and NO concentration in cardiac tissues of DOX-treated rats.

MDA: malondialdehyde; GPx: glutathione peroxidase; SOD: superoxide dismutase; NO: nitric oxide; combination: curcumin 100 mg/kg + nebivolol 1 mg/kg; ANOVA: analysis of variance; DOX: doxorubicin.
Data was expressed as mean ± SEM and analyzed using one-way ANOVA followed by Duncan’s post hoc test. n = 7–12. a p < 0.05 versus control group.
b p < 0.05 versus DOX group.
c p < 0.05 versus curcumin 100 mg/kg group.
d p < 0.05 versus curcumin 200 mg/kg group.
e p < 0.05 versus nebivolol 1 mg/kg group.
g p < 0.05 versus nebivolol 2 mg/kg group.
These results indicated that administration of curcumin and nebivolol blocked DOX-induced lipid peroxidation in heart tissue due to their antioxidant potential.
Effect on cardiac NO concentration
NO concentration upon administration of DOX was significantly increased (29.9 ± 0.15 µM/L) compared with the controls (21.2 ± 0.20 µM/L; p < 0.05; Table 3).
Cardiac NO concentration in curcumin 200 mg/kg was significantly decreased (22.6 ± 0.15 µM/L) compared with DOX group ( p < 0.05).
There was a significant difference in cardiac NO of nebivolol-treated groups compared with control group and curcumin groups ( p < 0.05). Combination therapy resulted in a significant decrease in NO (25.3 ± 0.15 µM/L) compared with nebivolol monotherapy ( p < 0.05; Table 3).
mtDNA integrity
In normal animals treated with saline, intact form of mtDNA was electrophoresed as a major band of approximately 16.5 kbp (lane 1, Figure 4(a)). While DOX markedly decreased the amounts of intact mtDNA (lane 2), mtDNA obtained from animals treated with curcumin 200 mg/kg (lane 4), nebivolol 1 mg/kg (lane 5), nebivolol 2 mg/kg (lane 6), or combination therapy (lane 7) was electrophoresed in its intact form (single band). On the other hand, decreased amounts of intact mtDNA was presented with curcumin 100 mg/kg (lane 3).

(a) mtDNA changes in study groups. Lane 1, mtDNA isolated from control animals; lane 2 mtDNA from the DOX-treated animals; lanes 3 and 4, mtDNA isolated from animals treated with curcumin (100 and 200 mg/kg, respectively); lanes 5 and 6: mtDNA isolated from animals treated with nebivolol (1, 2 mg/kg, respectively); and lane 7 mtDNA isolated from animals treated with combination therapy. (b) nDNA changes in study groups. Lane M, 100 kb DNA ladder; lane 1, intact nDNA of control animal; lane 2, nDNA of DOX-treated animal; lanes 3 and 4, nDNA from animals treated with curcumin (100, 200 mg/kg, respectively); lanes 5 and 6 nDNA isolated from animals treated with nebivolol (1, 2 mg/kg, respectively); and lane 7 nDNA isolated from animals treated with combination therapy. (c) Concentration of mtDNA in cardiac tissues in study groups. Data was expressed as mean ± SEM. n = 7–12. *p < 0.05 versus control group, ‡ p < 0.05 versus DOX group, $ p < 0.05 versus curcumin 100 mg/kg group, *p < 0.05 versus curcumin 200 mg/kg group, || p < 0.05 versus nebivolol 1 mg/kg group, ¶ p < 0.05 versus nebivolol 2 mg/kg group. mtDNA: mitochondrial DNA, nDNA: Nuclear DNA, DOX: doxorubicin, Cur: curcumin, Neb: nebivolol, combination: curcumin 100 mg/kg + nebivolol 1mg/kg.
mtDNA quantity
In DOX group, a significant decline (20.11 ± 1.71 ng/µl) was observed in cardiac content of mtDNA when compared with the control group (115.5 ± 9.2 ng/µl; p < 0.05; Figure 4(c)). However, a significant increase of mtDNA was observed upon supplementation of curcumin 200 mg/kg (69.36 ± 4.51 ng/µl). Furthermore, administration of nebivolol significantly reversed the DOX-induced decline in mtDNA content ( p < 0.05), while combination therapy normalized mtDNA content (102.22 ± 9.1 ng/µl; p < 0.05). Hence, the current data suggested a possible protective potential of current treatments against DOX-induced mtDNA damage.
Fragmentation of nDNA
Gel electrophoresis showed that nuclear DNA (nDNA) isolated from normal rats treated with saline (lane 1) showed total ladder and smear negativity. DOX induced marked decrease in the amount of intact nDNA. Moreover, a dramatic oligonucleosome length degradation of DNA was observed (lane 2; Figure 4(b)).
In contrast, appreciable fragmentation of nDNA was found in animals that received curcumin 100 mg/kg (lane 3) and no fragmentation was detected with curcumin 200 mg/kg (lane 4), nebivolol 1 and 2 mg/kg (lanes 5 and 6, respectively), or combination treatment (lane 7). These results demonstrated that the current treatments abolished the ladder pattern of nDNA cleavage; therefore, they provided protection against DOX-induced apoptosis.
Histopathological results
Cardiac muscle fibers of the control group appeared cylindrical with normal central oval nuclei and acidophilic cytoplasm separated by minimal amount of connective tissue (Figure 5(a)) and the hearts recorded grade 0 (Figure 5(a))
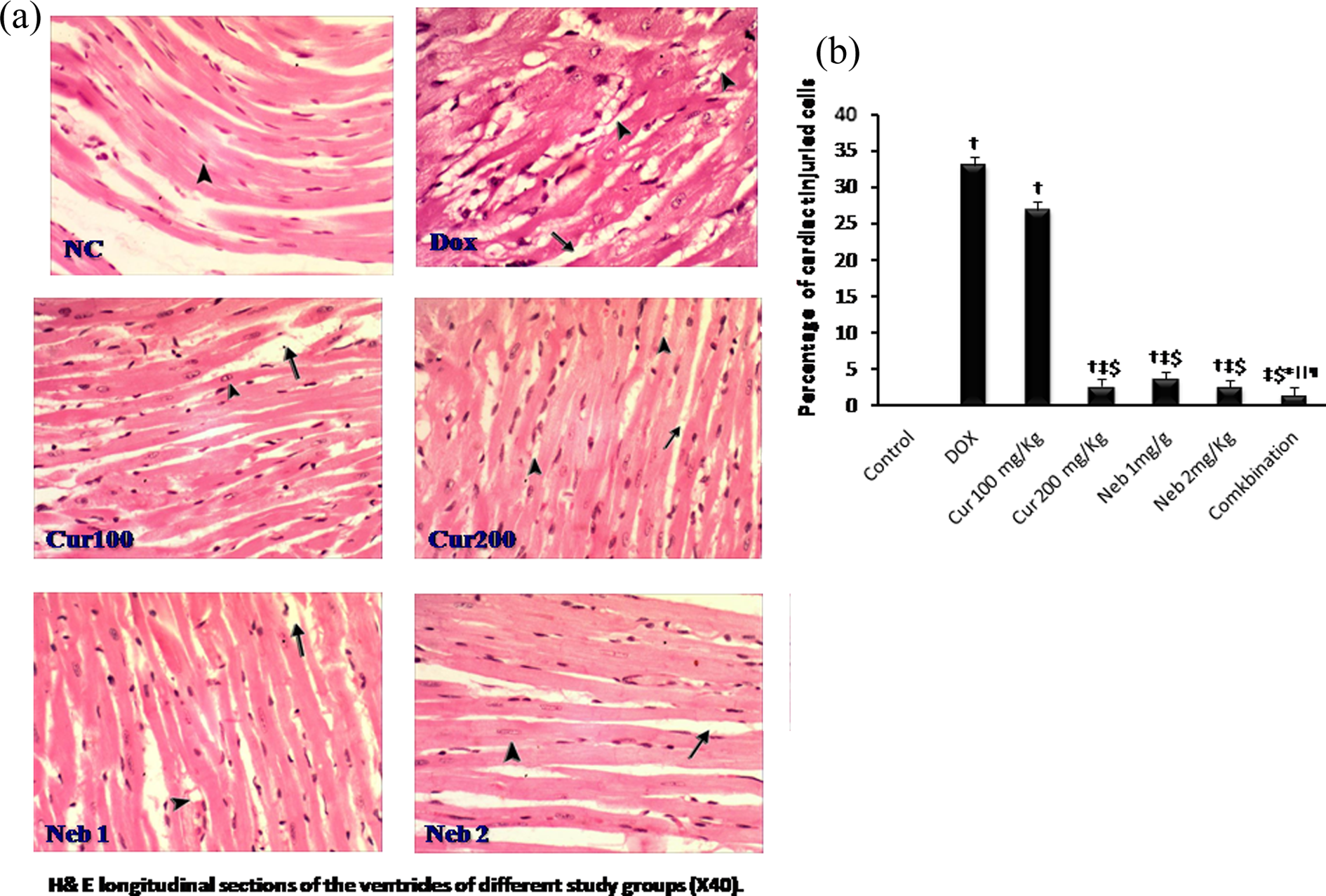
(a) H&E longitudinal sections of the ventricles in study groups (×40). The arrow head points to myocytes and myofibrils and the arrow points to interstitial edema. (b) Percentage of cardiac tissue injured cells in study groups. Data was expressed as mean ± SEM. n = 7–12. † p < 0.05 versus control group, ‡ p < 0.05 versus DOX group, $ p < 0.05 versus curcumin 100 mg/kg group, *p < 0.05 versus curcumin 200 mg/kg group, || p < 0.05 versus nebivolol 1mg/kg group. H&E: hematoxylin and eosin, NC: normal control, DOX: doxorubicin treated, Cur 100: curcumin 100 mg/kg, Cur 200: curcumin 200 mg/kg, Neb 1: nebivolol 1 mg/kg, Neb 2: nebivolol 2 mg/kg, combination: curcumin 100 mg/kg + nebivolol 1mg/kg, ¶ P< 0.05 versus nebivolol 2mg/kg group. Dox: doxorubicin, Cur: curcumin, Neb: nebivolol, C: combination; curcumin 100 mg/kg + nebivolol 1mg/kg.
Cardiac muscle fibers appeared markedly degenerated with marked vacuolization of the cytoplasm, interstitial edema, and wide separation in DOX group (Figure 5(a)) that showed the highest histopathological grade 2.5 for cardiac muscle injury with a significant increase in percentage of injured cells (33.17 ± 1.01%) compared with the control group ( p < 0.05; Figure 5(b)). Cardiac muscle fibers of curcumin 200 mg/kg and nebivolol showed mild degeneration with minimal vacuolization of the cytoplasm, mild interstitial edema, and slight separation (Figure 5(a)) with a significant decrease in the percentage of injured cells (2.67 ± 0.21, 3.67 ± 0.21, and 2.50 ± 0.22%, respectively; grade 1) compared with DOX group ( p < 0.05; Figure 5(b)).
The combination group showed the lowest cardiac muscle injury; the cardiac muscle fibers appeared less degenerated with minimal vacuolization of the cytoplasm, mild edema, and slight separation (Figure 5(a)); the percentage of injured cells was significantly decreased compared with DOX group and monotherapy ( p < 0.05; Figure 5(b)).
Discussion
The present results showed that DOX induced signs of cardiomyopathy in the form of increased mortality and decrease in BW and heart index indicating a severe dysfunction in cardiac performance as reported previously. 4 In accordance with previous studies, the ECG changes in DOX group reflected arrhythmias, conduction abnormalities, and attenuation of left ventricular function. 30,31
The response to isoprenaline of the isolated Langendorff hearts was attenuated with DOX as it decreased the number of β-adrenoceptors and reduced isoprenaline-stimulated adenylate–cyclase activity. 32
The present work demonstrated that DOX increased the most specific highly sensitive markers for myocardial cell injury; 33 cardiac troponin I as well as cardiac toxicity enzymatic indices (CPK and CK-MB).
Cardiac toxicity could be a secondary event following increased lipid peroxidation of cardiac membranes that resulted in irreversible modification of membrane structure and function with the consequent leakage of troponin I and cardiac enzymes. 34
The current study showed an increase in cardiac MDA level that could be attributed to DOX-induced generation of oxygen free radicals which evoke extensive tissue damage, reacting with membrane lipids, proteins, and nucleic acids. 35
Further, the activities of the cardiac GPx and SOD were significantly reduced in DOX group that is in harmony with the study by Dbrowska et al. 36 This can be explained on the basis of their exhaustion in combating the previously observed oxidative stress. 34 Two different ways of free radical formation by DOX have been described; the first implicates the formation of a semiquinone free radical that yields superoxide radicals and the second way produces iron–DOX complex that can reduce oxygen to hydrogen peroxide and other active species. 36,37 Free radicals are known to attack the highly unsaturated fatty acids of the cell membrane to induce lipid peroxidation and consequently damage membranes. 38
On the other hand, DOX treatment had significantly increased cardiac NO level that is consistent with the study by Wang et al.. 39 DOX is thought to increase NO by induction of inducible NOS (iNOS) expression. iNOS inhibition or deficiency has been reported to protect against DOX-induced cardiac dysfunction. 39
DOX-induced toxicity is closely related to mitochondrial injury and decrease in respiratory function. 40 In agreement with these results, the current study had revealed that DOX significantly disrupts the integrity and amount of intact mtDNA. Adult cardiac muscle cells are terminally differentiated and have lost their proliferative capacity; 41 therefore, apoptotic agents can significantly affect the function of this vital organ. In the current study, DNA qualitative analysis showed a dramatic DNA fragmentation after administration of DOX. In addition, oxidative damage to cardiac mitochondria and to cardiomyocytes has been widely implicated as a primary cause for DOX-induced cardiac toxicity. 42 The enhanced generation of reactive oxygen species by DOX may directly damage mitochondria or alter the synthesis of proteins associated with the mitochondrial electron transport chain with the subsequent inhibition of oxidative phosphorylation and decrease in cardiac high-energy phosphate homeostasis. 43 The accumulation of various deficiencies in high-energy phosphate metabolism may be a very critical step for the DOX-induced deterioration of cardiac function and for the onset of chronic cardiotoxicity. 44
The histopathological changes induced by DOX in the current study are reported previously by Bai et al. 45 DOX induces mitochondrial dysfunction and activation of matrix metalloproteinase that leads to the loss of myocardial collagen, myocyte slippage, ventricular dilatation, loss of progressive contractile dysfunction, and eventually heart failure. 45
In the present study, curcumin 200 mg/kg induced a significant amelioration of DOX-induced ECG changes and increased inotropic and chronotropic responses to isoprenaline as reported previously by Mohanty et al. 46 Fascinatingly, lipoic acid of curcumin was proven to be a potential candidate in ameliorating DOX-induced cardiac injury as it has the ability to quench free radicals that protects membrane polyunsaturated fatty acids from oxidation concomitantly, stabilizes membrane, and reduces calcium influx; in addition, it is a modulator of intracellular calcium levels and contractility in cardiac tissue. 13 In accordance, previous study demonstrated that curcumin has multiple therapeutic activities that are beneficially protective, and it has an ameliorative effect against DOX-induced cardiac toxicity and hepatotoxicity and blocks DOX-induced nephrosis and abnormalities in lipid profile. 7
In the current study, the beneficial effects of curcumin were also manifested by a significant decrease in troponin I concentration and serum levels of cardiac enzymes. Additionally, MDA level was significantly diminished, and depleted GPx and SOD activities were restored. The antioxidant potential of curcumin neutralizes the cytotoxic free radicals generated due to DOX-evoked cardiac injury, thereby protecting against the loss of membrane integrity, stabilizing the membrane with consequent inhibition of enzymes leak. 6 Curcumin inhibits lipid peroxidation by scavenging free radicals and thus blocking the lipid chain reaction similar to α-tocopherol. 13 Swarmy et al. 4 conclude that the cardiotoxicity induced by DOX is related with oxidative stress. Antiproliferative, anti-initiation, and free radical-scavenging properties of curcumin may boost myocardial integrity and attenuate the cardiac toxicity. Curcumin has shown to be cardioprotective, which may be attributed to its potent antioxidant properties.
In accordance with our results, mice treated with both HO-3867 and DOX showed a significant improvement in cardiac functional parameters compared with mice treated with DOX alone. 8 In addition, curcumin induced a significant reduction in cardiac NO level as it scavenges free radicals and inhibits iNOS activity and promotes its degradation. 47
The current study revealed that curcumin administration significantly attenuated DOX-induced mtDNA decay. Being a powerful antioxidant, curcumin reduced the formation of mitochondrial superoxide radicals. 48 Curcumin controls mitochondrial superoxide formation indirectly by regulating redox-cycling ubiquinone, 49 thus mitigating oxidative stress, and in turn reduces damage to mtDNA. Treatment with curcumin showed a significant reduction in nDNA fragmentation that might be attributed to its antioxidant action exerted against the prooxidant effects of DOX. 50 Furthermore, curcumin inhibited the site-specific degradation of deoxyribose by prooxidants due to its iron chelation ability. 50 In accordance with our results, curcumin showed increased levels of Bcl-2 similar to controls, and it increases apoptotic markers. 8 So, its combination with DOX is a viable option for treatment of cancer with reduced cardiotoxic side effects. 8
Nebivolol, on the other hand, resulted in a significant increase in the inotropic and chronotropic response to isoprenaline. Previous studies showed that patients treated with β1 blocker without intrinsic sympathomimetic activity had more adrenoceptors than control subjects and that the adenylate–cyclase activation by the β-adrenoceptor agonist isoprenaline is also enhanced in this situation. 10 The pharmacodynamic profile of nebivolol in human myocardium (high β1 selectivity, lack of ISA, and inverse agonistic activity) may be favorable for treatment of heart failure. 51
The present data showed the normalization of troponin I with a significant decrease in cardiac enzymes as well as increasing percentage of survivors. These effects could be due to membrane stabilization by nebivolol with the consequent decrease in the release of cardiac enzymes. 10
Interestingly, cardiac MDA level was decreased, while GPx and SOD enzymes activities were elevated in nebivolol treated groups. This is verifying its guardian role against DOX toxicity. 10
Nebivolol—NO-releasing βB—reduces superoxide formation, has an antioxidant effect, and preventseNOS uncoupling. 52 Nebivolol was effective in alleviating oxidative mtDNA damage. This may be attributed to the free radical-scavenging property and a regulatory action on cellular and mitochondrial membrane permeability with increase in membrane stability. 53 Nebivolol, via its vasodilating and antioxidant properties, has been shown to reduce endothelial peroxynitrite production, and this could reverse the dissipation of membrane potential, so it could protect mitochondrial function. Peroxynitrite can impair mitochondrial respiration, coupling, and decrease mitochondrial membrane stability. 54
It was also found that noradrenaline caused apoptosis in rat cardiomyocytes through downregulation of Bcl-2 and activation of caspase-2 pathways, so nebivolol may induce cardiac myocyte expression of Bcl-2 protein, which prevents permeability transition pore opening and therefore decreases cytochrome-C release. Nebivolol was also reported to increase mitochondrial SOD and nitrite/nitrate release; 10 these events might be one of the mechanisms of nebivolol-mediated stabilization of the mitochondrial membrane.
Moreover, nebivolol has shown its antiapoptotic property by abolishing nDNA fragmentation. It has also been shown that stimulation of β1-receptors increases apoptosis through the cyclic adenosine monophosphate-dependent pathway; 55 so blocking of β1 receptors may inhibit apoptosis. In harmony with our results, it was reported that nebivolol reduces myocardial apoptosis after myocardial infarction by indirect prevention of oxidative stress. 55
Conclusion
The present study selected a low dose of curcumin that per se did not significantly ameliorate cardiac toxicity. This subeffective dose was found to potentiate the effect of nebivolol in treating DOX-induced cardiac toxicity in rats. Therefore, the present results postulated that this combination may be considered as a potentially useful candidate in the combination chemotherapy with DOX to limit free radical-mediated organ injury. However, any reconsideration of the use of this combination would require a detailed review of its clinical safety data with a range of doses.
Footnotes
Conflict of interest
The authors declared no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.