
Abstract
Objective:
The aim of this prospective study was to establish the cord blood interleukin 1β (IL-1β) levels and asphyxia enzymes in term newborns and their relationship between delivery modes. We investigated whether cord blood level of IL-1β could be used as a reliable marker for detecting hypoxic stress and to determine the optimal cut-off level for IL-1β.
Methods:
The study was designed prospectively. Cord blood samples were obtained at the time of delivery from 75 noninfected full-term neonates for the purpose of measuring cord blood levels of IL-1β. Women were classified into three groups according to the mode of delivery (20 vaginal delivery, 29 urgent caesarean section (with foetal distress) and 26 elective caesarean section). All cases were followed-up by hospitalization. Umbilical cord sampling was carried out for IL-1β, umbilical artery gas parameters and other asphyxia enzymes at the time of delivery. Cord blood IL-1β was measured by enzyme-linked immunosorbent assay. The perinatal outcomes of the cases were recorded after birth. Demographic characteristics, neonatal outcomes and laboratory findings were compared in all the three groups.
Results:
IL-1β levels showed statistically significant difference between groups (p < 0.01). The relationship was found between IL-1β cord blood levels and the mode of delivery. IL-1β levels of urgent caesarean section group were significantly higher than elective caesarean section and normal delivery group (p:0.001 and p:0.001, respectively). Normal delivery levels were significantly higher than the elective caesarean group (p:0.001).
Conclusion:
Urgent section (foetal distress) and vaginal delivery (labour) were each associated with elevated IL-1β cord blood levels in noninfected full-term neonates, while only elective caesarean section was associated with decreased IL-1β levels. For the evaluation of newborns at high risk for perinatal hypoxic stress, cord blood IL-1β levels may lead the way. On the other hand, the mode of delivery may be associated with the effects on the immune system. Further investigations with larger patient groups are required to confirm our results.
Introduction
Interfering with the normal physiological process of labour and birth in the absence of medical necessity increases the risk of complications for mother and the baby. Modern obstetric units are well equipped to deal with high risk or complicated births, but the policies, protocols and physical infrastructure are not ideal for physiological birth. In the past quarter century, advances in medical technology have been accompanied by an increase in intervention-intensive labour and birth. 1
In spite of major advances in monitoring technology and knowledge of foetal and perinatal medicine, perinatal asphyxia is one of the significant causes of mortality and long-term morbidity. Perinatal asphyxia results in hypoxic injury to various organs including kidneys, lungs and liver but the most serious effects are seen on the central nervous system. Hypoxic injury is of concern in an asphyxiated neonate because it can lead to serious long-term neuromotor sequelae among survivors. The incidence of long-term complications depends on the severity of asphyxia. Up to 80% of infants who survive severe asphyxia develop serious complications, while 10–20% of them develop moderately serious disabilities. 2
A gold standard definition of birth asphyxia does not exist. It is defined by Apgar score, and blood gases, haematocrit, blood sugar, cardiac and liver enzymes values are an adjunct to assess the degree of hypoxic–ischaemic injury related to other organs. It is important to search for a more sensitive, reliable and rapid marker to accurately diagnose hypoxic injury that would be a valuable initial treatment in neonates with asphyxia.
Cytokines are small soluble peptides that were originally characterized as immune modulators but have subsequently been found to mediate a diverse array of functions in nonimmune tissues, including the central nervous system. As a consequence of this dual role, cytokines induced in response to hypoxia in the perinatal period can impact foetal neurodevelopment and immune system. 3 Interleukin-1β (IL-1β) is a key proinflammatory mediator of the neuroimmune response and have been demonstrated to be up-regulated in adult animal models of ischaemic/hypoxic brain injury. 4,5 IL-1β also act on neural stem and progenitor cells influencing proliferation and neurogenesis in response to stress, disease and injury. 6
The purpose of this study was to assess the cord blood IL-1β levels in term newborns and their relationship between delivery modes.
Methods
Between June and December 2009, a total of 75 neonates were enrolled in this study. We excluded infants who were exposed to maternal chronic diseases, smoking, diabetes, alcohol or drug use. The parents signed written informed consent, and the study design was approved by the hospital’s Ethics Committee. The term infants were born alive at Bakirköy Research and Training Hospital, Hatay, Turkey. Antenatal history, risk factors and other parameters were prospectively recorded. Neonates were classified into three groups according to the mode of delivery: urgent section group (n = 29), elective section group (n = 26) and vaginal delivery group (n = 20). Neonates were considered as noninfected when they presented with normal C-reactive protein and a good clinical course up to the seventh day of life without antibiotic therapy. Intrauterine infection, premature rupture of membranes, sepsis, congenital anomalies and neonates with pathological hyperbilirubinaemia were excluded. Cord blood samples were collected from noninfected full-term and normal for gestational age singleton neonates for laboratory analysis. Detailed neurological and systemic examination was performed. Apgar scores (1 and 5 min) were recorded. Status of the delivery room and prognosis of early postnatal adaptation were identified. For patients at high risk for neurological damage, neurodevelopmental follow-up and imaging were planned.
Cord blood samples were transported from point-of-origin to a laboratory without any loss of time for blood gases and haematocrit analysis (ABL700 Flex, Radiometer Medical A/S, Denmark). Blood sugar, cardiac and liver enzymes were measured by auto analyzer (ARCHITECT ci16200, Abbott Laboratories, Illinois, USA). Cord blood samples were centrifuged at 4°C for 10 min at 4000 r/min and aliquots were stored at −80°C for assaying. IL-1β amount was determined using RayBio® Human IL-1β ELISA KİT (Cat no: ELH-IL1beta-001) purchased from RayBiotech, Inc. (Norcross, Georgia, USA) following the manufacturer’s instructions. IL-1β levels were expressed as picogram per millilitre.
Statistical calculations were performed with Number Cruncher Statistical System 2007 Statistical Software (Utah, USA). In order to determine the relationships between the variables the following statistical tests were used: descriptive statistical methods (mean and standard deviation) as well as between-group comparisons, if variables had normal distribution one-way analysis of variance and Tukey’s multiple comparison test sub-group comparisons, if variables had abnormal distribution Kruskall–Wallis test and Dunn’s multiple comparison test sub-group comparisons, comparisons of qualitative data, χ 2 test and Pearson’s correlation test. IL-1β levels for the variable urgent section group, elective section group and the remaining areas under the receiver operating characteristic (ROC) curve were determined. At the point of prediction, sensitivity, specificity, positive and negative predictive points, accuracy and LR+ values were calculated. The values of p < 0.05 were statistically significant and 95% confidence intervals were evaluated.
Results
The clinical characteristics of the patients in all the three groups are presented in Table 1. The patients were similar in terms of maternal age, parity, gender, gestational age and foetal measurements. The groups differed significantly in terms of Apgar score, base excess (BE) and glucose levels. There were significant decreases in the Apgar scores, BE and glucose levels in urgent and elective section groups compared with the vaginal delivery groups (Table 2). According to the groups, cord blood levels of IL-1β were statistically different (p < 0.0001). Due to the varying differences in the IL-1β levels, post hoc Tukey’s honest significant test was used. The levels of IL-1β in urgent section group were found to be significantly higher than elective section and vaginal delivery groups. According to ROC analysis, the optimal cut-off level was 10.6 pg/ml for IL-1β to predict foetal distress. When IL-1β level is higher than this cut-off value, the possibility of foetal distress increases 6.5 times (positive likelihood ratio: 6.55 and area under the curve (AUC): 0.911 ± 0.04; Figure 1(a)). IL-1β levels of elective section group were found to be significantly lower than the vaginal delivery group. According to ROC analysis, the optimal cut-off level was 3.7 pg/ml for IL-1β to predict decreased immune response. (positive likelihood ratio: 18.26 and AUC: 0.983 ± 0.02; Figure 1(b)).
Demographic data of groups.

aOne-way analysis of variance test: Ki-Kare test.
bOne-way analysis of variance test: Kruskal–Wallis test.
Laboratory findings and foetal distress parameters of groups.

IL-1β: interleukin 1β; AST: aspartate transaminase; ALT: alanine transaminase; GGT: γ-glutamyltransferase; LDH: lactate dehydrogenase; CK: creatine kinase; m: minute; BE: base excess; HCO3: bicarbonate; pCO2: partial pressure of carbon dioxide.
aIL-1β levels of urgent section was higher than elective section and vaginal delivery (p:0.0001), while IL-1β levels of elective section was higher than vaginal delivery groups (p:0.0001). Apgar scores indicate higher levels for vaginal section than urgent section and elective section (p:0.009; p:0.031).
bOne-way ANOVA: Kruskal–Wallis test.
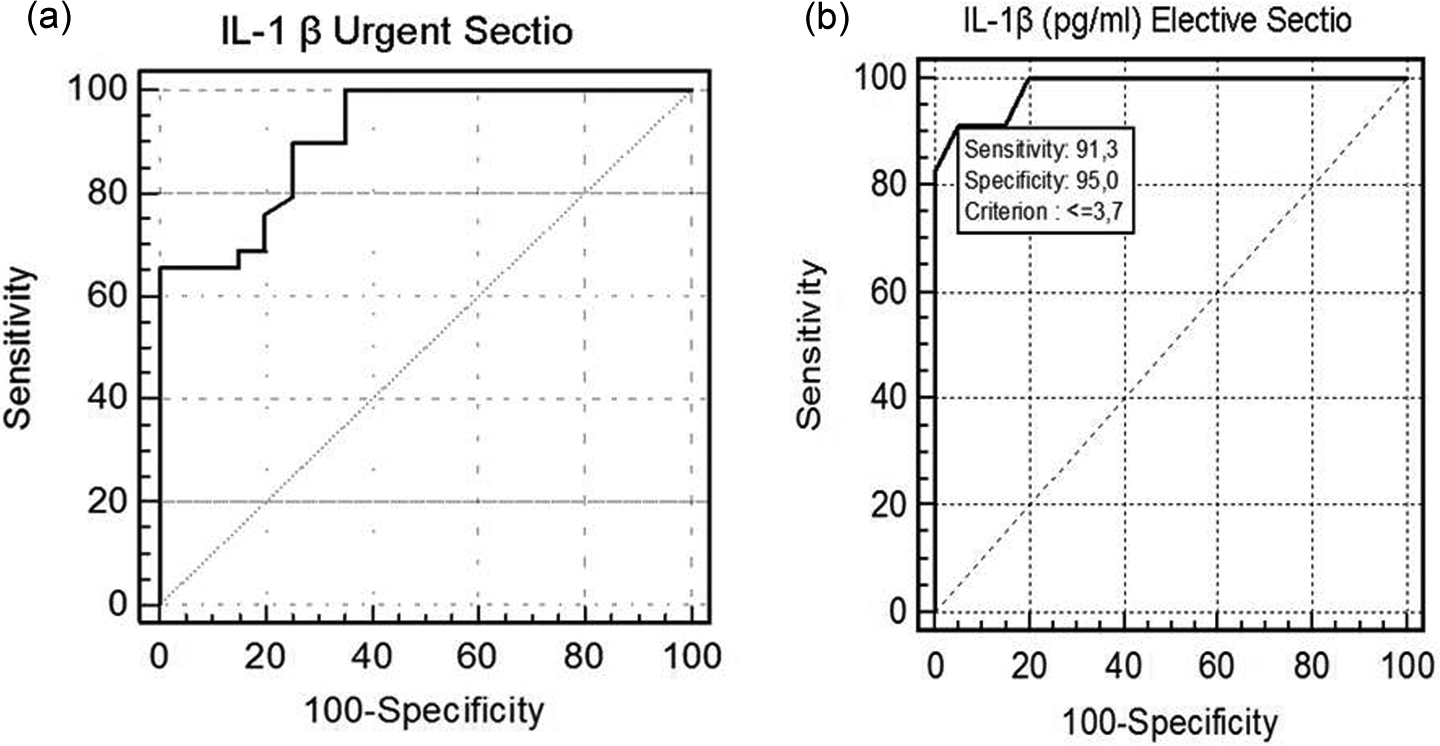
(a) ROC analysis of the risk of foetal distress for neonates born by urgent section and those by vaginal delivery. (b) ROC analysis of the risk of decreased immune response for neonates born by elective section and those by vaginal delivery. The areas under the ROC curves (mean ± SD) were as follows: a = 0.911 ± 0.04; b = 0.983 ± 0.02. ROC: receiver operating characteristics.
Discussion
Proinflammatory cytokines are thought to be involved in normal pregnancy and labour. In vitro production of cytokines depends on the duration of hypoxia and the maximal secretion occurring during reperfusion. Mechanisms of cytokine production involve reactive oxygen intermediates during hypoxia or during reperfusion. 7 Interactions between foetal distress and cytokines have been previously reported in number of clinical and research implications that centre around the role of mode and timing of delivery, maternal cooling during labour and the role of immune-modulating drugs. 8 –11 IL-1β belongs to the family of cytokines known primarily for its role in proinflammatory responses, but recent emerging evidence suggests it has interesting roles in normal learning and memory as well as changes induced by inflammation and stress. 12 In our study, neonates with foetal distress had moderate and transient hypoxia severe enough to warrant caesarean section. This condition was associated with an increase in IL-1β levels. Miller et al. found elevated cord blood levels of IL-1β in infants born by urgent caesarean section or by induced vaginal delivery but not in those born by elective caesarean section or by normal vaginal delivery. 13 Hata et al. previously found non-detectable IL-1β and IL-1 receptor antagonist levels in neonates born by elective caesarean section and vaginal delivery. 14 Buoconore et al. reported that IL-1β levels remained unchanged in cord blood irrespective of the mode of delivery. 15 In our study, IL-1β levels increased when urgent section and foetal distress were present. If prolonged perinatal hypoxia occur, foetal oxygenation can rapidly be impaired, which could account for the increased levels of IL-1β that we observed. The absence of correlation between pH values and IL-1β cord blood levels was unexpected, one explanation could be that foetal distress was not severe or long enough to induce pronounced acidosis.
Certain warnings are necessary regarding the individual criteria for the perinatal hypoxia. It may occur in utero, at birth or in the postnatal period. Furthermore, hypoxic–ischaemic insults in the recent antepartum period (measured in hours) may result in a similar obstetric and neonatal clinical picture, as well as identical brain injuries. 16 Data are commonly inaccurate and inconsistent, particularly for blood gases, Apgar scores, appropriate brain imaging and results of testing for organ dysfunction. The consensus criteria changed in the past decade, and more changes are anticipated as new research results are published.
Stallmach et al. demonstrated low and stable IL-1, IL-6, IL-8 and TNF-α cord blood levels in neonates born without labour. 17 We also reported elevated IL-1β cord blood levels in neonates born by spontaneous labour as compared to those born by elective section. At present, there is much evidence for beneficial short- and long-term effects that labour and vaginal delivery have on neonatal respiratory adaptation to extrauterine life. The increased rates of elective caesarean section, a procedure long believed to be less distressing for the foetus, have been associated with a higher risk of iatrogenic respiratory distress syndrome. 18 Reduced blood concentrations of neurohormonal and neuroendocrine markers provide additional insight in the pathophysiologic mechanism that brings a poor immune–neuroendocrine response at birth into the cascade of events that can lead to altered postnatal adaptation. 19 The evidence suggests that interfering with the normal physiological process of labour and birth increases the risk of complications for mother and the baby. The lack of significant improvements in maternal or infant mortality amid an ever rising caesarean rate in the United States suggests that more technology does not necessarily translate into better outcomes. 1
Our study underlines the fact that cord blood IL-1β levels are associated with an increase in urgent section but a decrease in elective section compared with the vaginal delivery. Even if these results do not have any immediate clinical relevance, they should serve as a stimulus to carry out further studies with the aim to follow the development of the immune system. For the evaluation of newborns at high risk for perinatal hypoxic stress, cord blood IL-1β levels may be indicative of neurological damage for which neurodevelopmental follow-up should be planned. However, the results need to be confirmed, preferably in a larger, prospective study on asphyxiated neonate, evaluating the use of cord blood IL-1β in the diagnostic process.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.