
Abstract
Purpose:
This article provides an historical assessment of the role of radiotherapy in the treatment of inner ear infections.
Materials and methods:
The research utilized a literature-based evaluation of the use of x-rays during the first half of the 20th century on the treatment of otitis media (OM), mastoiditis, and cervical adenitis and their impact on the occurrence of deafness.
Results:
X-Rays were consistently found to be effective as a treatment modality at relatively low doses, in the range of 10–20% of the skin erythema dose, rapidly reducing inflammation, and accelerating the healing process. The mechanistic basis of the clinical successes, while addressed by contemporary researchers, is evaluated in the present article in light of current molecular biology advances, which indicate that clinically effective low doses of ionizing radiation act via the creation of an anti-inflammatory phenotype in highly inflamed tissue.
Conclusions:
X-Ray treatment of OM, mastoiditis, and cervical adenitis was widely accepted in the first half of the 20th century by clinicians as an effective treatment when administered within an appropriate dosage range.
Introduction
In the early decades of the 20th century, before the discovery and distribution of antibiotics, x-rays were used to treat a wide range of diseases including gas gangrene, 1 carbuncles/furuncles, 2 various forms of arthritis, 3 –5 and numerous other serious human diseases. These historical evaluations have indicated that x-ray treatments were broadly accepted as having reproducible therapeutic success, although the data supporting such conclusions were principally based on substantial case study reports, before the development and implementation of double-blind random epidemiological methods. In contrast to the other diseases noted above, the use of x-rays has continued to be employed in Germany for the treatment of arthritis that is affecting nearly 30,000–50,000 patients per year, along with the widespread use of animal models in mechanism-based research. 5 The present assessment extends these recent efforts by evaluating the historical use of x-rays in the treatment of human diseases that have long since become the therapeutic perview of antibiotics. The present article, therefore, assesses how the medical community in the first half of the 20th century used x-rays and γ-rays to treat various types of inner ear infections such as otitis media (OM) and mastoiditis and to what extent these treatments were considered successful by practitioners of that era and possible biomedical mechanisms that may account for claimed clinical effectiveness. First, the article briefly describes the clinical features of OM, mastoiditis, and cervical lymphadenitis. Second, the historical foundations of the efficacy of x-ray/γ-ray treatments of these clinical conditions were assessed.
Background of OM and mastoiditis
OM refers to a common infection of the middle ear of viral, bacterial, or fungal origin. It can be acute or chronic depending upon the duration of infection. Inflammation of the middle ear (mastoiditis) is characterized by lymphocytic infiltration, hyperemia, pus formation, and recovery in uncomplicated cases. 6,7 Infection of the middle ear with effusion, but in the absence of acute infection, is known as OM with effusion (OME) or serous OM (SOM). Nearly 2.2 million cases of OME occur annually in the United States. 8 Persistent infections with resultant tympanic membrane perforation are known as chronic suppurative OM.
The majority of the middle ear infections follow an upper respiratory tract infection or allergy, which leads to swelling and congestion of Eustachian tubes and nasopharynx. Resultant blockage of the Eustachian tube leads to accumulation of middle ear secretions, which can further become infected by microbiological pathogens leading to acute OM. OME can result from a dysfunction of Eustachian tubes or after acute OM as an inflammatory response.
Therapeutic strategies include symptomatic relief and recovery with the use of antibiotics like amoxicillin alone or third generation cephalosporins depending upon the persistent symptoms. Tympanostomy/myringotomy (incision of tympanic membrane to drain middle ear fluid and relieve pressure symptoms) is performed for recurrent OM cases with hearing loss.
An ear drum perforation may sometimes lead to the spread of infection and subsequent inflammation to the mastoid cavity (mastoiditis), which can disrupt the honeycomb-like structure of the mastoid bone and thus add to the complications of acute OM. It is difficult to treat mastoiditis since many medications fail to reach deep into the mastoid bone, thus necessitating long-term antibiotic treatment or surgery (mastoidectomy) if routine antibiotic treatments are ineffective. Mastoiditis and intracranial complications of acute OM are common in developing countries where there may be limited access to medical care. 7
Cervical adenitis
Cervical adenitis is a clinical condition characterized by massively enlarged/swollen lymph glands in the neck area. The engorged tissue is often hard and quite painful with the patient displaying a modest to high fever. There are a number of medical conditions that have the potential to lead to the formation of such swollen lymph glands. These could be tonsillitis, dental disease, OM, scarlet fever, mumps, measles, diphtheria, and influenza. Given the close association of cervical adenitis with OM, it is included in this assessment. While most of these causes are minimized today, in the first half of the 20th century, these underlying conditions and the occurrence of lymphadenosis were not uncommon. Standard treatments for such massive swollen lymph glands during that era generally included the use of compresses and ointments, neither of which were particularly effective. 9,10
Historical foundations of radiotherapy for OM and mastoiditis
During the spring of 1920, Beattie 11 reported that there were a large number of cases of acute OM following the epidemic of influenza. In cases that did not involve typical mastoid-related symptoms, Beattie 11 routinely x-rayed these cases to assist in the diagnosis. Unexpectedly, he observed the rapid healing of what he described as “many” cases. This set of observations led him to investigate 14 additional patients with discharging ears (i.e. young children of 4–13 months); these subsequent findings supported the initial unexpected curative observations leading to the tentative conclusion that x-rays may have value in the treatment of subacute and early chronic types of OM. Beattie 11 also cited similar findings of five other contemporary colleagues. Additional supportive examples were also provided in the discussion of his article.
Nearly a decade after the initial report of Beattie, 11 Granger 12 –14 summarized the results of extensive clinical studies with infants and babies with clear signs of infection and occlusion of the mastoid who were treated with x-rays. X-Ray treatments improved clinical symptoms and facilitated a rapid and complete resolution of the condition. He further claimed that such findings were confirmed by other otologists (although no references were provided) with the x-ray treatment.
The patients treated with x-rays generally displayed a decrease in temperature, absence of pain and insomnia, reduction in the amount of discharge, and a change in the character of the discharge from purulent to mucopurulent. In the final discussion of his article, Granger 13 concluded by stating that “after seeing 50–60 patients with mastoiditis without bone destruction get well with fractional doses of the x-rays, one can not feel that this is an accident.” A confirmatory perspective was offered by Granger 14 in a subsequent publication in Radiology. The research of Granger 12 –14 was offered from the perspective of a radiologist, not an otologist.
A similar supportive assessment was provided by Schillinger, 15 an otologist, who noted that greater than 85% of cases with acute mastoiditis displayed a marked improvement within 24 h of x-ray treatment. Of particular interest were his recountings of how he linked x-ray exposure to the treatment of mastoiditis. In 1924 (some 8 years prior to the publication of his article), Schillinger observed beneficial changes in patients with acute mastoiditis after diagnostic x-ray examination. Before this time, he obtained only one plate for each mastoid. From this time onward, two plates of each side were obtained during x-ray examinations. It was only following this change in diagnostic procedure that the beneficial clinical results occurred. Based on these observations, he concluded that the amount of irradiation required to make one plate of each mastoid is less than the dosage needed for the beneficial effect. According to Schillinger, 15 a dosage between that needed for making two plates of each mastoid up to a 25% skin erythema dose (SED) provided the apparent optimum therapeutic effect.
Of particular relevance to this article is that Schillinger 15 suggested that as a prophylactic measure against mastoid disease that it would be appropriate to treat patients with acute OM using x-rays with 20–25 rad administered on day 7 of suppuration, repeated after 2–3 days (total of 3–4 exposures) following the specific scheme he outlined. He then made a strong recommendation for radiologists and otologists to work closely together on such cases.
In 1933, Levin 16 also supported the use of x-ray therapy for mastoiditis before it progressed to osteomyelitis of the mastoid bone. He argued that such treatment would often prevent the occurrence of mastoidectomy, which was a serious operation in infancy and childhood during the early 1930s. To support this conclusion, he noted a series of 119 cases of acute OM in which 29 developed symptoms suggesting mastoiditis. This group of 29 received x-ray therapy of 1–3 treatments. Of the 29 patients, 27 displayed a complete elimination of symptoms. In contrast to the effects of x-rays on acute mastoiditis/OM, Levin 16 noted that the results with chronic OM were not as marked. In a series of six cases, which had persisted for many months, the x-ray treatment was effective in only two cases.
Dowdy et al. 17 selected 27 cases of OM (purulent) treated with tympanostomy/myringotomy alone, 15 cases of OM (purulent) treated with tympanostomy/myringotomy and low-dose radiation therapy (100 rad once or twice), and 15 cases of catarrhal OM (without pus discharge) treated with low-dose radiation therapy alone (100 rad once or twice). Their results revealed that the average disease duration was lowered from 27.2 to 21.2 days in cases of OM (purulent) treated with myringotomy and low-dose radiation therapy as compared to the cases of OM (purulent) treated with myringotomy alone. They also noted a change in consistency of discharge from being thick to watery after treatment with low-dose x-rays in cases with purulent discharge. Such treatment-related changes favor drainage, providing symptomatic relief to the patients. In cases with catarrhal OM (without pus discharge), Dowdy et al. noted quick pain relief and no disease progression to a purulent state.
Table 1 provides a listing of quotes of researchers of the 1920s–1940s that supported the effectiveness of x-rays in the treatment of OM and mastoiditis. These observations and the accompanying assessment of the published literature reveal a strong association between x-ray administration and the successful treatment of patients with these conditions.
Perspectives offered on the clinical efficacy of x-ray treatment of otitis media and mastoiditis by practitioners of the 1920s–1940s.
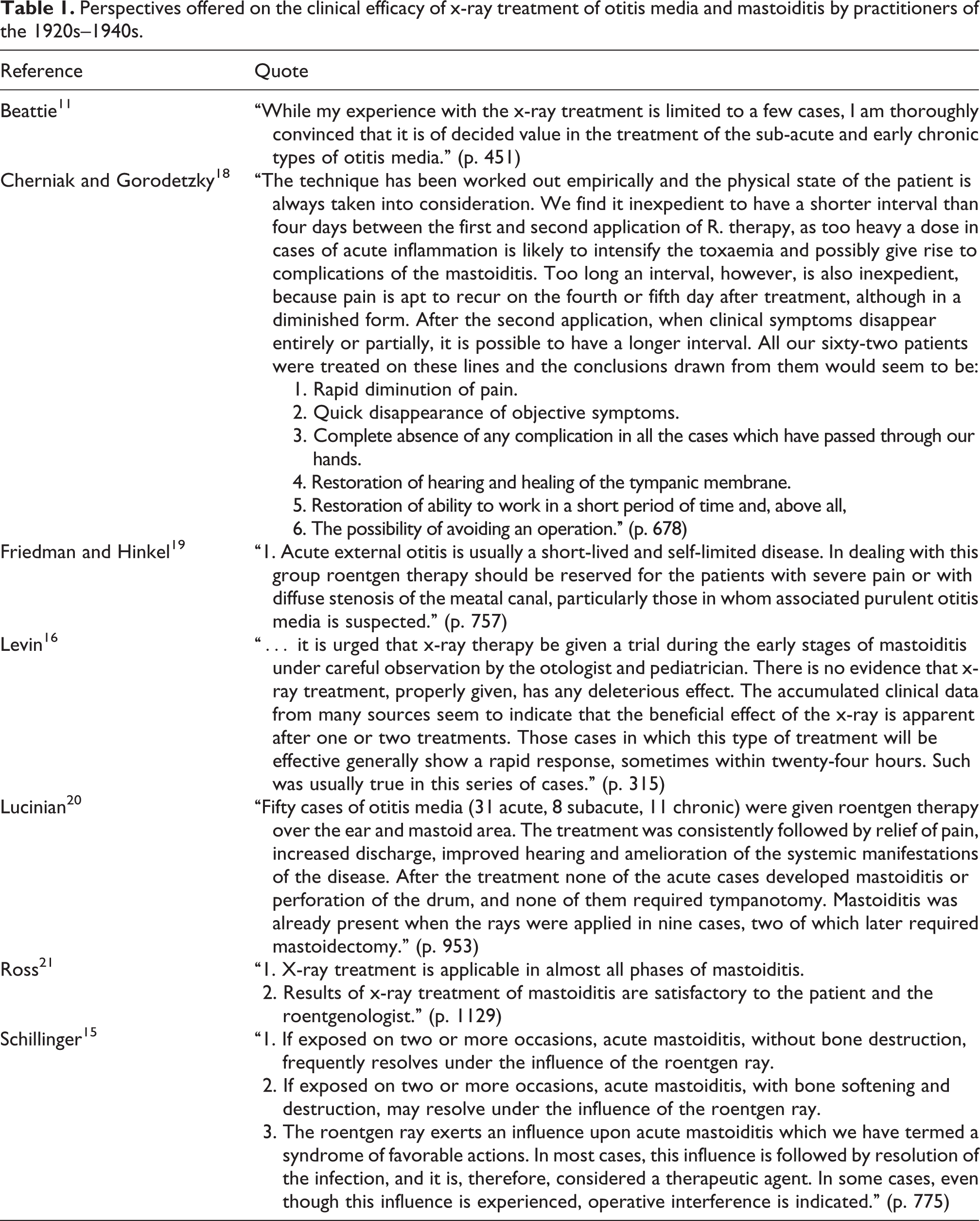
Continuing support for the use of x-ray treatment for patients with acute OM and/or mastoiditis was provided by other clinicians. 18 –22 Table 2 lists the studies with OM and mastoiditis cases by different practitioners during 1920s–1940s in which highly successful outcomes with x-ray treatments were generally reported. The majority of the studies listed provide information on the proportion of successful outcomes as compared to cases where the treatment was not effective. Of interest was the report of Lucinian since it differentiated the lessening of symptoms over time with x-ray exposure of about 15–20% of the SED. For example, pain was generally relieved after the first x-ray treatment. Fever was decreased, gradually requiring up to about 2 weeks. Following the first x-ray treatment, the swelling of the ear drum decreased. Thus, he concluded that early x-ray treatment reduces the course of inflammation and prevents drum perforation. The x-ray treatment was also shown to enhance healing of a perforated ear drum. Hearing, which is normally enhanced in these conditions, is generally improved within 24–48 h. Other clinical symptoms, such as tinnitus, extraneous noises, headaches, and dizziness, were also relieved. He noted that x-ray treatment was also effective in chronic OM and mastoiditis. On several occasions, authors attempted to generate a type of control group. In general, the x-ray treatment was far superior to the response of the controls regardless of how the controls were selected. 20 Lucinian 20 advocated (with a few exceptions) the use of smaller dosage at low voltage with light infiltration due to superficial localization and high radiosensitivity of the exudates. According to Lucinian, 20 a single 5-min dose of radiation, with a total dosage of 71.5 rad, was sufficient for the treatment of acute OM cases. A few subacute cases were also treated by a maximum of three treatments; on the other hand, chronic cases were administered with three to six treatments.
Number and/or proportion of cases of otitis media and/or mastoiditis reported during 1920–1940 successfully treated with x-rays.

Historical foundations: deafness and x-ray/radium treatment
The use of x-rays in the treatment of impaired hearing was reported in 1923 by Jarvis. 27 Although lacking in details, Jarvis 27 suggested that small doses of x-rays were useful in the treatment of ear infections and their symptoms in children and adults. He reported maximum response by the use of x-rays in the age group 25–50 years presenting with constant throat symptoms (catarrhal discharge) and frequent stuffiness of ears. This perspective was extended in 1926 by Smyth 28 who treated 100 cases of deafness with x-rays. These cases displayed redundant lymphoid tissue in the nasopharynx, near the opening of the Eustachian tube. The cases received 6 treatments, once every 10 days. The treatments were seen as generally successful. The first indication that radium could also be employed in the treatment of certain cases of deafness was noted by Stevenson and Wilson 29 in a pilot study with only eight patients.
Despite these independent advances in the treatment of hearing impairment with different forms of ionizing radiation, this area of radiotherapy was especially propelled forward by the work of Samuel J Crowe at the Johns Hopkins University with a ground-breaking publication in 1939. Crowe and Baylor 30 summarized 15 years of research on the causes and treatment of deafness involving about 15,000 patients. An area of research interest was the impairment of the hearing of high tones in children and adults. While it was generally accepted that high-tone hearing impairment was the result of nerve damage, Crowe and Baylor 30 proposed that there were some patients for whom this explanation was not satisfactory. There were children who regained their high-tone hearing following the removal of enlarged tonsils and adenoids. While this observation would rule out nerve damage explanation in such children, there were other children who did not show improved hearing after the operation. In at least some of these children, the authors observed that they had one important feature in common. That feature was the presence of excessive lymphoid tissue near the Eustachian tube.
According to Crowe and Baylor, 30 this lymphoid tissue growth may partially obstruct the Eustachian tube, leading to increased mucus production, causing tissue irritation, leading to diminished hearing capacity at the high tones. They also proposed that this effect may likely become progressive over time affecting lower octaves.
The problem with the excessive lymphoid tissue is its location. It was not possible to surgically remove it without adversely affecting the tubes. The authors recalled the earlier report of Heineke 31 that lymphoid tissue is much more susceptible than adjacent tissues to ionizing radiation. Such differential tissue susceptibility to ionizing irradiation suggested that it may be effective in destroying the excess lymphoid tissue while not affecting the surrounding tissue. Their goal was to marginally reduce the size of the lymphoid tissue while also at least temporarily inhibiting its growth. With this general concept, Crowe and Baylor 30 developed treatment methods for the use of either x-rays or γ-radiation, which were refined over time. Based on extensive clinical experience, they concluded that the most efficient treatment of hearing impairment due to excessive lymphoid tissue is irradiation with radium or x-rays. So striking were the findings of this clinical research that they claimed there was the potential to reduce the number of deaf adults in the next generation by 50%. The findings of Crowe and Baylor 30 lead to a spate of research on the effects of ionizing radiation on childhood and adult hearing loss; mild tubal disturbance, particularly in children, yielded very successful treatment outcomes, restoring hearing with no demonstrable adverse side effects. 32 –43
Of particular historical note was the application of Crowe’s treatment for the control of aero-otitis in Air Force personnel as many pilots were reported to have some hearing loss. This was probably affected by the fact that following adenoidectomy approximately 75% of patients display lymphoid tissue regrowth. Approximately 40% of patients later develop some loss of hearing. In order to prevent/relieve hearing loss, most pilots (approximately 25,000) were treated, through 1968. 44 While publications on the use of radiation to treat lymphoid tissue related hearing loss were markedly reduced by the 1960s, Loeb 45 suggested that it might still be a useful treatment option in the case of “persistent recalcitrant serious otitis with hearing loss.” Even though alternative medical developments had outcompeted the use of radiotherapy for lymphoid tissue-related hearing loss due to antibiotics and surgical advances, he noted that there still remain patients with recurrent serious otitis and others whose reconstructed middle ear surgeries had yielded poor outcomes due to Eustachian tube obstruction and some children who need repeated insertions of ventilator tubes. In these cases, he suggested that there may still be a role for radiotherapy especially with the capacity for excellent outcomes and low risk of adverse effects.
A 30-year follow-up of 28 patients by Loeb 45 on the placement of a radium applicator in the posterior nasopharynx to open the obstructed Eustachian tube revealed that 24 patients had a good response with two having a fair response with no secondary malignancies. Similarly, Hardy and Bordley 46 reported smaller adenoid tissues and improved hearing after 5 years of follow-up in a randomized trial of patients with chronic SOM who were treated with radium implants.
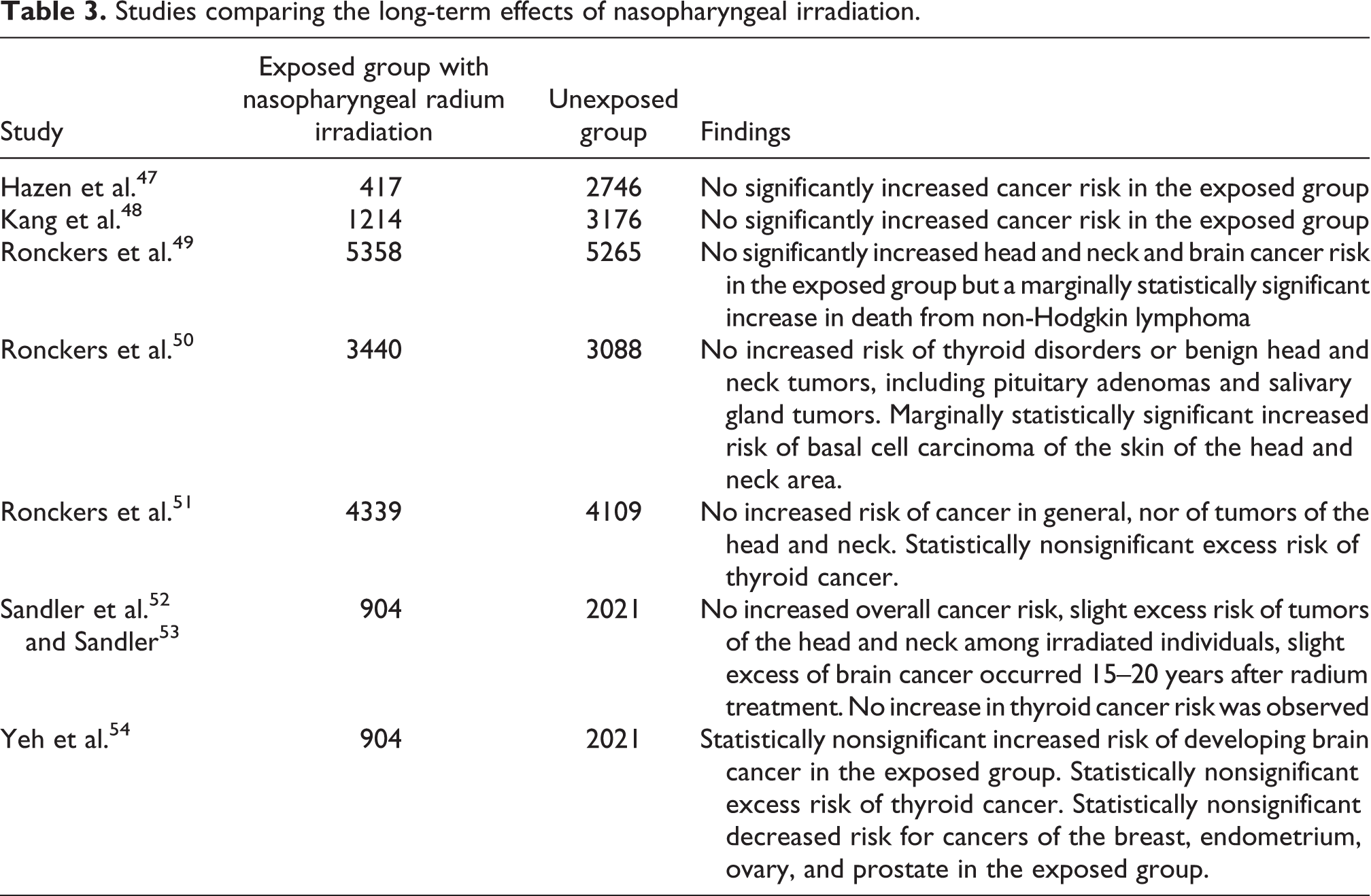
Numerous questions were raised about the technique of application, the optimal dose, and how the treatment may vary by age and between similarly aged individuals. There were also debates on whether the radiation dose should be administered once or be fractionated and the pattern of the fractionated doses. There also emerged concern over whether there might be possible long-term effects related to the exposure to the ionizing radiation. This was especially the case for physicians and their assistants who were handling the radium on a daily basis while treating many patients. Further concerns were raised with respect to the long-term effects on patients, with particular concern for brain and thyroid. Table 3 summarizes the long-term studies conducted on patients irradiated with nasopharyngeal radium to treat ear dysfunctions. Such studies did not detect a definitive link between nasopharyngeal irradiation and any disease, including cancer, suggesting the capacity to estimate an upper bound risk for such procedures.
Studies comparing the long-term effects of nasopharyngeal irradiation.
Historical foundations: cervical adenitis
In the absence of effective alternative treatments, Williams from Boston and Pusey of Chicago in 1902 were the first clinical researchers in the United States to use x-rays in the treatment of cervical adenitis. A year later, George E Pfahler, 55 the first Professor of Radiology at the University of Pennsylvania Medical School, USA, reported on 10 cases. 56 Table 4 lists quotes by practitioners of the 1920s–1940s on the clinical efficacy of x-ray treatment of cervical lymphadenitis. According to Pfahler and Kapo, 56 there was much uncertainty with the use of the x-ray exposure technique and in the type of dosing. During the first two decades, they noted that many patients were administered 30–40 fractionated x-ray doses, with each being about 10% of an SED. These doses would usually be spread over 1–2 years. However, over time the number of doses was reduced by about 80%, while the efficacy of the treatment markedly improved.
Perspectives offered on the clinical efficacy of x-ray treatment of cervical lymphadenitis by practitioners of the 1920s–1940s.

A major treatment breakthrough came from Heidenhain and Fried, 59 Heidenhain, 60 and Fried, 61 who reported treating more than 1500 patients for a broad range of acute inflammatory conditions, including acute lymphadenitis. They initially treated acute cervical lymphadenitis patients with a 20% SED. They found that reducing this dose by about 50% resulted in a noticeable improvement in efficacy and in consistency of response. They emphasized that treatment at higher doses, especially in the 20–50% SED range tended to aggravate the inflammatory response and reduce the occurrence of a successful clinical outcome. 9,58 The clinical success of the x-ray treatment was consistently reported being in the 75–90% range across all investigations over a 16-year period. Table 5 compiles the SED reported in the treatment of cervical lymphadenitis. The successful treatment would require usually one or two x-ray treatments, with the patient typically displaying a marked temperature drop within 12–48 h, along with a marked relief of pain and discomfort, reduced swelling, and a quick resolution of the medical condition. 9,10 Table 6 lists the number of cervical lymphadenitis cases reported by different practitioners during 1920s–1940s.
SEDs reported in the treatment of cervical lymphadenitis.
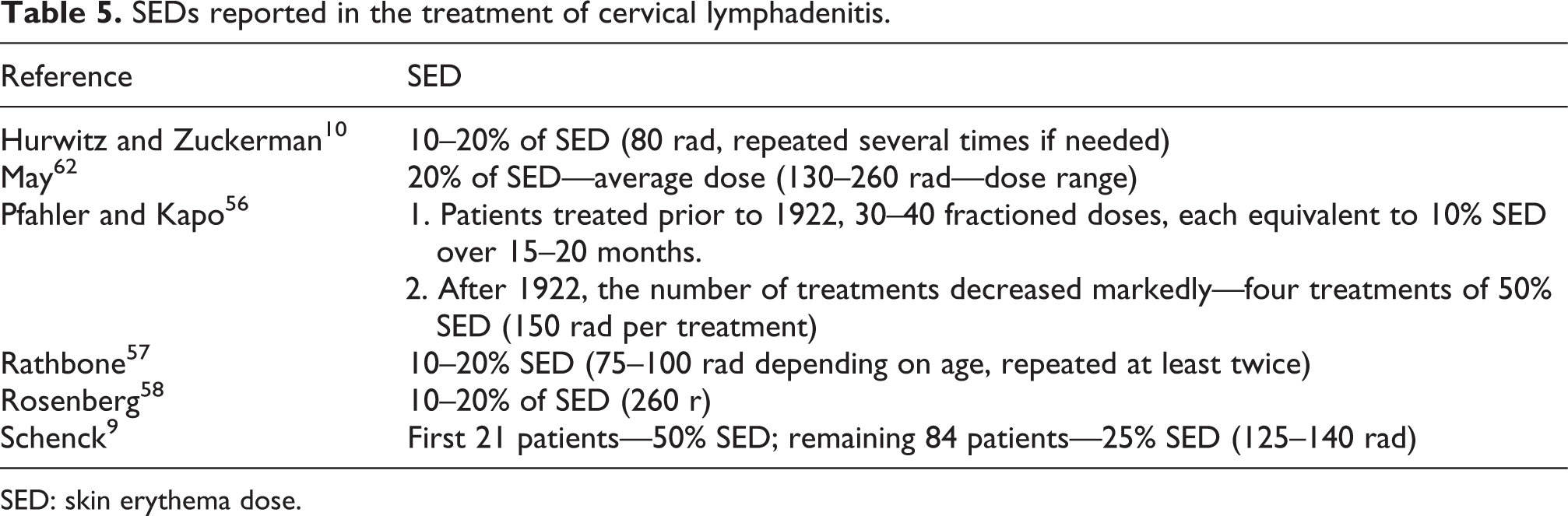
SED: skin erythema dose.
Treatment efficacy of cervical lymphadenitis cases reported by various practitioners during 1920–1940.

The success of the x-ray treatment for cervical lymphadenitis also seems to be, at least in part, dependent on how soon after the onset of the condition the treatment is provided. In general, when the treatment was given within the first 3–5 days, the symptoms tended to resolve more quickly than if applied later.
Levy 66 was impressed with the x-ray treatment of lymphadenitis in children below 4–5 years. He indicated that the benefits are often permanent. Following the x-ray treatment, children typically experienced fewer colds and the sinus rarely gets infected. In the case of older children, Crowe and Baylor 30 stated that x-ray treatment early in the course of the disease was critical to assure a normal functioning of the auditory tubes and doing so can profoundly reduce the occurrence of hearing impaired adults. Table 6 presents the treatment efficacy of cervical lymphadenitis cases reported during 1920–1940.
Discussion
The present article provides documentation that x-ray treatment of OM, mastoiditis, deafness, and cervical adenitis was widely accepted in the early half of the 20th century (Tables 1 and 3). The treatments were usually fractionated with x-ray doses of 75–200 rad depending upon the clinical condition (Table 5). For acute OM, a single treatment of approximately 70 rad (15–20% SED) was sufficient and showed marked improvement in symptoms for nearly 85% of patients, while patients displaying more chronic symptoms required three to six treatments as in the case of mastoiditis (25% SED). Similarly, six treatments (once every 10 days) were given for deafness cases with redundant lymphoid tissues near the nasopharynx. Cervical adenitis cases required 10% SED with one to two treatments and had a success rate of 75–90%, depending upon how quickly the treatment was initiated, with treatment initiation during the first 3–5 days having the best outcomes.
Reduction in pain and improvement in hearing were the most striking clinical benefits of the x-ray treatment across all conditions occurring within 24–48 h of exposure (Tables 1 and 3). Other clinical benefits included reduction/elimination of ear discharge, healing of the perforated drum, and reduction in lymphoid tissue blocking the Eustachian tubes and thus unwarranted surgeries.
The majority of the research methods used to study the effect of x-rays on OM, mastoiditis, deafness, and cervical lymphadenitis were case studies with quasi controls being used by only some of the investigators for comparison purposes. The comparisons were made with the use of antibiotics and surgical procedures.
A mechanistic understanding of how x-rays facilitated the healing process in the cases of OM and mastoiditis was not known in the early decades of the 20th century. Recent findings have emerged, which may offer insight into this matter. In general, low doses of x-rays have been shown to affect the development of a highly integrated anti-inflammatory phenotype mediated by decreases in nitric oxide/inducible nitric oxide synthase, decreases in reactive oxygen species, increases in heme oxygenase, suppression of tumor necrosis factor-α (TNF-α), increases in TNF-β, activation of several transcription factors such as nuclear factor-κB and activator protein 1(AP-1) API, as well as decreased adhesion of leukocytes and polymorphonuclear leukocytes to endothelial cells. 1,67,68 This anti-inflammatory phenotype is a consistent feature when low doses of ionizing radiation are administered to tissues with substantial inflammation. Mechanistic studies with mul-tiple animal and cell models have confirmed the consistency of these observations accounting for the protective effects of low-dose ionizing radiation in animal models with various types of inflammatory disease such as arthritis. 67,68 Further research will be necessary to clarify how the x-ray induced anti-inflammatory phenotype would affect the course of OM, mastoiditis, and cervical adenitis infection.
Despite the effectiveness of x-rays in terms of pain reduction and improved healing time, medical developments including better antibiotics and advances in surgical techniques during the latter half of the 20th century outcompeted the use of x-rays for the treatment of OM, mastoiditis, and lymphoid tissue-related hearing loss. Even though x-rays are currently not used for treatment of these conditions, it is still widely used for diagnostic purposes. The fact that x-rays are still being used in countries like Germany for pain reduction in numerous conditions 5 and that x-rays can accelerate healing processes via the development of an anti-inflammatory phenotype 69 suggest a possible discussion of the use of x-rays not just for diagnostic purposes, but therapeutically, especially in this era of antibiotic-resistant disease-causing microbial strains.
Footnotes
Conflict of Interest
The authors declared no conflicts of interest.
Funding
The research on the topic of hormesis has been supported by awards from the US Air Force and ExxonMobil Foundation over a number of years.