
Abstract
The goal of this article was to assess the historical role of radiotherapy in the treatment of selected inflammatory diseases. The specific research involved a literature-based assessment of the use of x-rays during the first half of the 20th century for the treatment of furuncles and carbuncles, the potentially serious staphylococcus infections. X-Rays were reported to be effective as a treatment at relatively low dose, about 10–20% of the skin erythema dose, which often quickly and profoundly reduce pain and accelerate the resolution/healing of the furuncles and carbuncles. These findings were based on considerable clinical experience that was generally reported in the form of case studies. The mechanism of x-ray–induced reduction of inflammation and acceleration of healing was suggested to result from a combination of immune alterations that enhanced phagocytosis as well as via an anti-localization effect on the pathogenic organism that facilitates their destruction.
Introduction
The occurrence of a pimple that becomes infected with staphylococcus bacteria has been a common occurrence in human history. While the majority of such pimples are usually successfully overcome by biological defense mechanisms, a certain proportion continues to expand in size, soreness and infectivity. As the pimple expands, it could transform into a furuncle (boil), possibly progressing into a carbuncle. A carbuncle is an abscessed Staphylococcus aureus infection, typically with multiple openings draining pus into the skin. The furuncle (boil) is an infection of the hair follicle and when clustered together can be called carbuncle. The staphylococcus infection, if unchecked, can pose a serious health concern with risks of infecting bones/joints, heart valves and the entire blood system (i.e. sepsis). In the decades before the introduction of antibiotics, severe carbuncles were often treated with surgery with varying degrees of success. Nonetheless, the mortality rate was also alarming, approaching 10% for nondiabetics and at least double that for diabetics. 1,2
The present article provides an historical summary and assessment of the use of x-rays in the treatment of furuncles and carbuncles during the first half of the 20th century, including the efficacy of such treatments and its underlying mechanisms for pain reduction and accelerated healing. It will be demonstrated that the x-ray treatment of these dermatological conditions was very widespread and a mainstream therapy, which was often seen as a superior option than surgery. This appraisal of x-ray treatment of these lesions is more than of historical relevance, especially in light of concerns over the extensive use of antibiotics and concerns with the development of resistance.
Results
First use of x-rays to treat carbuncles
Within a few years after the discovery of x-rays, physicians sought to test whether this new technology might have application in the treatment of furuncles and carbuncles. In 1906, Coyle 3 made what is believed to be the first report of the effects of x-rays on the treatment of carbuncles. In his paper Coyle noted that he had been using x-rays with good outcomes for the treatment of boils. He then indicated that he initially treated a patient with an ischiorectal abscess that was so inflamed he could not sit or walk. After he treated the abscess with x-rays, the patient reported a notable and rapid decrease in pain. The abscess also was quickly healed. These observations lead Coyle to extend his patient profile to include those with carbuncles. He then reported on five patients that were effectively treated with x-rays, quickly reducing pain and with the healing process strikingly accelerated. A year later Evler (cited in May, 19294) also reported carbuncle cases that were successfully treated with x-rays). 4
These initial findings were ignored until Dunham 5 from the University of Cincinnati reported the treatment of 67 consecutive patients with carbuncles with good clinical success. The x-ray dose used in the treatments was about 60% of a skin erythema dose (SED) and only one exposure was usually needed (The SED was used as an indicator of the quantity of radiation exposure. It was extensively used to assess and limit the exposure of workers and patients to ionizing radiation during the first half of the 20th century. For detailed review of its historical and medical foundations as well as its limitations, see studies by Belisaro and Pugh, 6 Belisario 7 and Pohle. 8 ). His clinical observations were remarkably similar to those of Coyle, that is, quick reduction in pain, along with accelerated healing of the carbuncle. This author concluded that it was important to understand how the x-ray treatment induced such a clinically significant benefit. Over the course of the next nearly three decades, there were about 20 clinical articles published on the effects of x-rays on carbuncles, reporting the findings on nearly 1000 patients in the United States. The results of another 225 patients were reported in the discussion section of some of these articles. A similar number of patients were reported in Europe, principally from Germany. 9 The last clinical study on x-ray–treated carbuncles was published in 1942, 10 reflecting how rapidly antibiotic therapy replaced the role of x-rays.
Mainstreaming of x-ray treatment for carbuncles
The physicians involved in the treatment of patients with carbuncles were part of the mainstream of the medical profession of the first half of the 20th century, being active in their regional and national medical societies, publishing their clinical findings in mainstream journals (Table 1). In the United States, the clinical investigations were reported by physicians either in private practice or in academia. The academic/institutional researchers were from Columbia, the Mayo Clinic, Harvard Medical School, Tufts Medical School, University of Pennsylvania and University of Nebraska, the city hospitals of Boston and New York and the U.S. Navy. The findings were often reported at professional Society meetings, such as the American Roentgen Ray Society, AMA, Providence Medical Association, Southern Medical Association, Norfolk County Medical Society, Baltimore City Medical Society, Radiological Society of North America, Massachusetts Medical Society and others.
Quotes on the effectiveness of x-ray treatment of furuncles and carbuncles
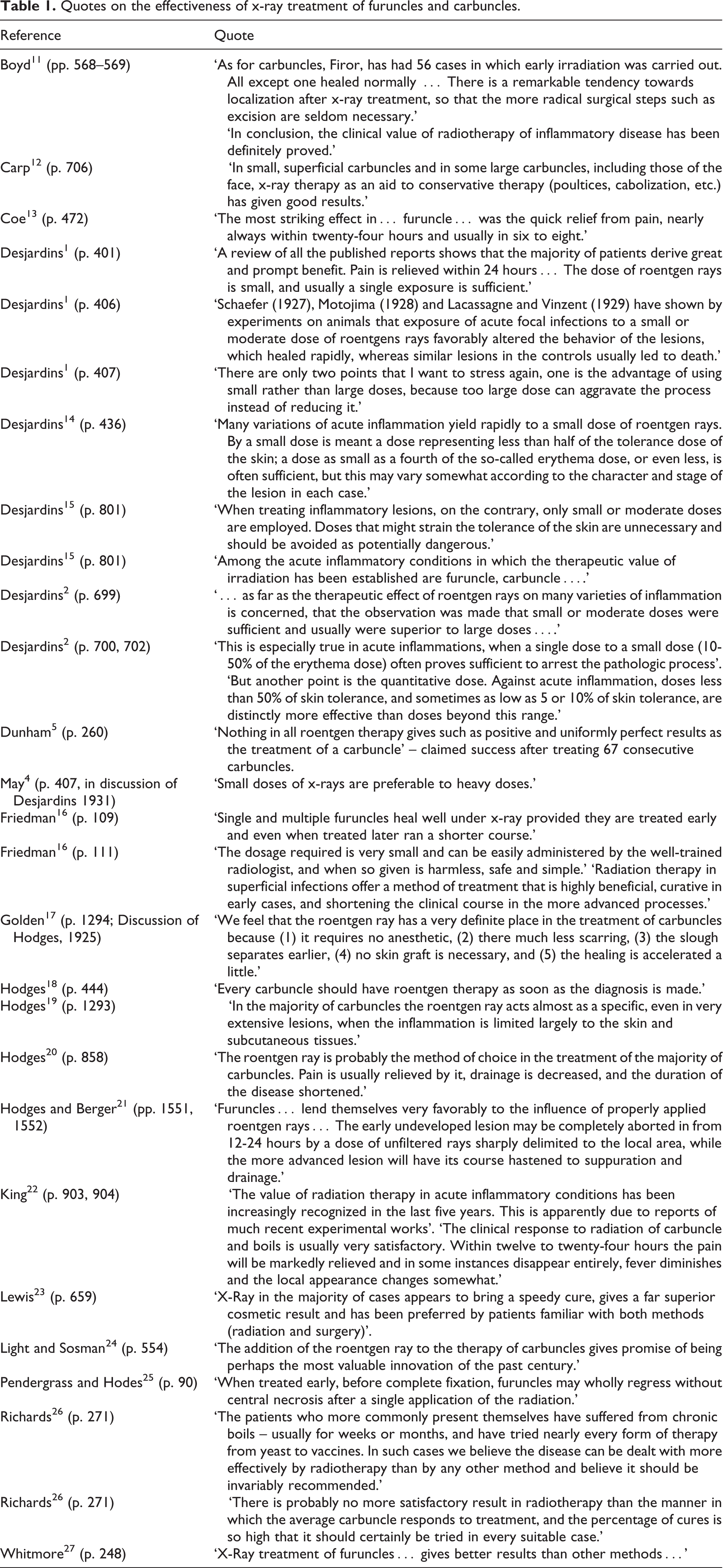
The articles written about the x-ray treatment for furuncles and carbuncles typically are principally case studies (Tables 2 and 3). Sometimes the authors indicate that the cases were not selected to illustrate the effectiveness of a treatment but, in fact, reflect their entire clinical experience during a defined period of time. In these cases, the authors noted that the cases reported were “consecutive” with no selection of best examples. For example, the Dunham 5 study noted 67 consecutive cases. This is also seen with Lewis, 23 Hodges, 19 Firor, 28 King 22 and others. Other authors have compared their “consecutive” cases with other information that could serve as a “quasi” control group. For example, Golden 17 reported obtaining 30 surgical cases for the treatment of carbuncles from his medical department and compared the results to his own cases. In several studies authors have placed different patients into different treatment groups for analysis based on how they were treated. 31 In this way the patients were placed into the allocated treatment groups via a post hoc methodology. That is, these patients were not randomly allocated prior to treatment. Other authors have compared the responses of the same person to different carbuncle treatments at the same general location at the same time or within the same year. Essentially all of the authors had considerable experience in the treatment of carbuncles using a broad range of treatment modalities. The general conclusions that these clinicians made were typically based on considerable professional experience. Major journals that published the effects of x-rays on furuncles and carbuncles are listed in Table 4.
X-Ray therapy in the treatment of major carbuncles (Source: McLaughlin, 1942) 10

Effect of x-rays on furuncle (boils)

NR: Not reported.
Journals that published the effects of x-rays on furuncles and carbuncles

The administration of x-rays was generally similar over the nearly 40 years of their treatment of furuncles and carbuncles. The treating physicians used the skin erythema dose (SED) as an upper bound exposure. The published papers on x-ray–treated furuncles and carbuncles typically did not identify the specific SED, the definition of an SED or a reference to which they based their judgment. (A detailed assessment of the historical foundation of the SED during 1920s–1930s indicated that the SED varied according to author, with the typical range being in the 350–500 R range.) The SED could also vary according to whether the x-rays were filtered or not and the degree of filtration. In the x-ray carbuncle literature, these factors were not addressed. These factors create a situation in which there is more variability among reported studies than would be apparent by the range of SED listed in Table 5. The range of reported x-ray treatment has been from 0.1 to 1.0 SED. Table 5 provides a listing of specific investigators and their reported SED use. In general, there was a trend toward somewhat lower x-ray doses from about 0.5–0.75 SED in 1920s to 0.1–0.20 SED in 1930s. Of particular significance was that the lower dose treatment was believed to be more effective than that reported at higher doses. Unfortunately, these reports of differential dose range response effectiveness were never explicitly demonstrated in any reported experimental study. The decrease of the therapeutic dose by about two- to four-fold (e.g. 0.5–0.75 to 0.1–0.2 SED) represents an appreciable decrease of exposure. It also suggests that the therapeutic zone has at least a four-fold dose range.
Skin erythema doses reported in the treatment of carbuncles a

aValue given as the proportion or fraction of the SED.
The general trend in medicine during the period of 1920–1940 found physicians from several fields, including radiology, dermatology, surgery and other specialties, converging to treat patients with carbuncles depending on the individual patient circumstances. Over the 20–25 years of x-ray treatment of carbuncles there emerged a general clinical consensus that it was an effective treatment for a relatively high proportion of the patients, including nondiabetic and diabetic individuals. The general perspective was that x-rays were effective in profoundly and quickly reducing pain and accelerating the healing process. X-ray treatment was also reported to be effective in preventing the spread of infection in many cases. It also had the distinct advantage of being noninvasive and relatively inexpensive. Table 1 provides a series of quotes from published articles in the United States expressing the views of the authors on the effectiveness of x-rays in treating the furuncle and/or carbuncle.
The scientific evaluation of the efficacy of x-rays during the period of 1920–1940 was similar for that of other contemporary treatment modalities. Thus, x-rays, surgery and other approaches were assessed in the same fashion with a strong emphasis on case studies. Treatments tended to be retained based upon empirical evidence.
A complementary approach for assessing how the medical profession in the United States in pre-1940s period considered the treatment of furuncles and carbuncles was provided by Ayres et al. 33 who surveyed 500 dermatologists (n = 250) and surgeons (n = 250). The reporting dermatologists noted about 3000 cases, with about 66% being treated with x-rays. In contrast, surgeons reported radical surgery for carbuncles for the majority of carbuncle cases (60%). X-ray treatment was used by surgeons to treat 19% of patients with carbuncles but for 38% of the patients with furuncles. According to the authors, the average duration of treatment of carbuncles using surgical methods was about twice that as reported with x-ray treatments. The mortality rates, while generally low, were about three-fold greater with the surgery method. These data tend to reflect the general findings of the clinical literature of carbuncle treatment during 1930s in the United States.
Carbuncle treatment mechanisms
Immune modulation: destruction of lymphocytes, phagocytosis enhancement
Desjardins 1 proposed that x-ray treatment destroys lymphocytes that have infiltrated a furuncle/carbuncle, doing so in a very prompt fashion, being within 30 min (Table 6). This proposal was based on extensive published research with multiple animal models that demonstrated the sensitivity of immune cells such as lymphocytes to x-rays. 44 –51 In addition to lymphocytes, the x-ray treatment was shown to destroy other infiltrated immune cells including polymorphonuclear neutrophils (PMNs) and eosinophils. As a result of such cell destruction, Desjardins 1 hypothesized that there was release of protective intracellular substances into the surrounding area, making these agents more readily available for defense functions than they were in the intact cells. This process was also proposed to be causally linked to an increase in phagocytosis that follows the disintegration of the lymphocytes. This hypothesis was further built upon observations that the regression in the rate of inflammation was highly associated with the rate at which lymphocytes are destroyed by irradiation. An alternative interpretation to these observations is that the immune response to the staphylococcus infection may often be very heightened, possibly contributing to the occurrence of the inflammatory response. Such immune-related enhancement of inflammation and toxicity is commonly reported in chemical toxicology 52 in which Kupffer cell activation, following initial toxicant-induced damage, can profoundly enhance the occurrence of agent-induced liver damage. By reducing either the biological activity of the Kupffer cells or reducing their numbers in the affected tissue the toxicity can be markedly reduced. 53,54 Such findings raise the question as to whether a similar process may occur in the case of immune response to the staphylococcus infection seen with the furuncle/carbuncle. Thus, it is possible that the x-ray–induced decrease in invading immune cells may prevent the occurrence of immune-mediated enhancement of the inflammatory response and that the x-ray–induced decrease in their numbers would serve to modulate this response. This hypothesis suggests that there might be an optimal decrease in such cells and that this would be dependent on the timing of the infection process among other factors.
Proposed mechanism/mechanisms for x-ray therapeutic effects on furuncle and carbuncle effects

Immune modulation: lymphocyte cycle acceleration
Another proposed mechanism to account for the capacity of the x-ray treatment to enhance the healing process of the furuncle/carbuncle was given by Boyd. 11 Based on the research of Isaacs, 55 he proposed that the x-ray treatment lead to an acceleration of the white cell generation and maturation, bringing about more rapid production of antibodies as well as enhanced capacity for phagocytosis. These enhanced functions were believed to lead to a faster resolution and/or localization of the inflammatory process.
Immune modulation: x-ray induced anti-localization effect
Patients with diphtheria can be treated with an antitoxin to prevent death. However, an issue is what is the best way to facilitate the effectiveness of the treatment? For example, is there a difference in effectiveness if the antitoxin is administered intravenous (IV), subcutaneous (SC), or intramuscular (IM)? In fact, Kahn 56 showed that for the neutralization of a lethal dose of diphtheria toxin in normal rabbits, five units of a given horse serum antitoxin was protective if administered IV but not so if given IM or SC. Overall, 10 units were necessary for toxin neutralization if given IM while 20 units if administered SC. According to Kahn et al., 38 it was the localization of the antitoxin by these two tissues that delayed it from reaching the toxin and for neutralization. Greater quantities of the antitoxin had to be injected to exceed the localizing capacities of these tissues. It was also demonstrated that the antitoxin-loading ratio of the SC tissue to skeletal muscle was about 10:1 in rabbits immunized with horse serum.
These findings led Kahn 37 to conclude that loose subcutaneous tissue possesses a greater localizing capacity than the tightly layered skeletal muscle, suggesting that localization is an immunological phenomenon. Further support for an immunological explanation is found by the fact that the localizing response to injected protein increases with the increase in antibody formation in immunity.
The observation of the anti-localizing effect of irradiation was extended by Kahn 37 to the migration of virulent staphylococci in irradiated and in nonirradiated areas of rabbits. The irradiated area displayed little or no lesions, suggesting the escape of the organisms from this area, while the nonirradiated area showed severe lesions, indicating that the organisms became localized. Anti-localization from radiation was only reported after the use of SC implant of horse gamma globulin in irradiated and in nonirradiated areas of rabbits. 57 The globulin escaped from the implants to a greater degree from the irradiated area than from the nonirradiated area.
Kahn et al. 38 –42 and Kahn 37 briefly explored the relationship of the anti-localization effect of x-rays that is used in therapy. Based upon these findings, it may be proposed that x-ray therapy effectiveness in the treatment of furuncles and carbuncles may be related to its capacity to induce an anti-localization effect. However, this hypothesis has yet to be assessed.
Vascular modulation: healing acceleration
Pendergrass and Hodes 25 argued that therapeutic doses of radiation were insufficient to induce much cellular damage, challenging the assertion of Desjardins that PMNs would be destroyed in the range of 75–200 r. In contrast, they proposed that the therapeutic effect of radiation was mediated via a local dilation of blood vessels. 34 Such an induction of hyperemia would lead to an increase in the rate and quantity of blood follow throughout the irradiated area. The enhanced blood flow would be most effective in the area surrounding the inflammation. This perspective was challenged by Desjardins 36 who claimed that if this interpretation were accurate then even greater changes of the same type would be predicted to occur following the application of a larger dose used in the treatment of chronic inflammation and that chronic inflammation should therefore respond more rapidly than acute inflammation but this was not what is clinically observed.
Modulation of oxidative burst and related processes
Administration of x-rays during the early phase of the infection typically prevents abscess formation, often leading to a successful resolution of the condition. These clinical observations led Schaue et al. 43 to propose that low-dose x-ray therapy modulates the excessive local response during abscess formation via diminishing the overproduction of reactive oxygen species by macrophages and other activated immune cell types. In fact, low x-ray doses (<1 Gy) markedly diminished the oxidative burst in the murine monocyte/macrophage cell line RAW 264.7 that were activated by different agents (e.g. interferon-gamma/lipopolysaccharide (IFN-gamma/LPS)). These in vitro findings were consistent with the clinical experience with treatments using x-rays in the 0.3–0.6 Gy range.
In addition to the effects of x-rays on the oxidative burst in stimulated macrophages, low doses of x-rays significantly diminish the production of nitric oxide (NO) by IFN-gamma/LPS-stimulated RAW 264.7 macrophages at doses
Kern et al.
60
reported that x-rays markedly reduced the adhesion of peripheral blood mononuclear cells (PBMC) to the endothelium at doses 0.1–0.5 Gy. Such a reduction of adhesion followed by irradiation of the PBMC was associated with the removal of
These collective findings (i.e. decrease in oxidative stress and reduction of NO production and the decrease in the adhesion of inflammation cells to the endothelium) provide an integrative mechanistic framework via the creation of an anti-inflammatory phenotype to account for the process by which x-ray therapy may diminish inflammation within a well-defined low-dose exposure protocol.
Discussion
This article provides documentation that x-ray treatment during the first half of the 20th century was used to successfully treat furuncles and carbuncles. The treatments were usually a single x-ray dose in the 75–200 R zone. These doses were about 10%–20% of an SED, a dose that would cause reddening of the skin in about 80% of subjects about 7–10 days following the dose. The proportion of the SED used would have been selected from prior published literature or clinic experiences and then applied to specific new cases. In the 1910s and 1920s, the treatment dose was typically higher, being about 50%–75% of the SED. Over time it became recognized that lower doses not only reduced the risk of x-ray–induced side effects but were more effective in the treatment of these diseases.
The most striking feature of these clinical observations was the rapid decrease in acute pain. The capacity of x-ray treatment to reduce inflammation has been widely reported 1,2,14,15 in the literature of the first half of the 20th century but also in the contemporary literature with more molecular approaches for its assessment. 61
While the research methods used to study x-ray treatment of induced furuncles and carbuncles were principally case studies and not of an experimental nature, the number of cases was very high with several thousand reported from a broad range of investigators. Occasionally, investigators were able to incorporate a quasi control for comparison purposes. The comparisons were made with other treatment procedures such as surgical approaches. In general, the x-ray treatment was found to be more effective in terms of pain reduction and the time required for healing.
Despite the success of x-rays in the treatment of furuncles and carbuncles, this treatment approach was quickly replaced in the early 1940s with the advent of chemical antibiotics, due to high effectiveness of the antibiotic treatment and fear of harm due to x-ray treatment. 62,63 Even though x-rays have not been used in the treatment of furuncles and carbuncles for nearly seven decades the fact that x-rays can have a powerful anti-inflammatory response and can accelerate the healing process is biologically interesting and potentially of clinical relevance, especially in light of modern concerns with antibiotic resistance. Furthermore, the use of low doses of x-rays for pain reduction has a potential current application in countries such as Germany for numerous disease conditions. 61,64,65 These and related findings suggest that knowledge of the past usage of x-rays in the treatment of infectious condition such as furuncles and carbuncles and other diseases is still relevant to modern patient care.
Footnotes
Declaration of Conflicting Interests
The author declares no conflict of interest.
Funding
This work on the dose–response relationships has been supported by awards from the US Air Force and ExxonMobil Foundation over a number of years.