
Abstract
CV247 (CV), an aqueous mixture of copper (Cu) and manganese (Mn) gluconates, vitamin C and sodium salicylate increased the antitumour effects of cisplatin (CDPP; cis-diamminedichloroplatinum) in vitro. We hypothesized that the antioxidant and cyclooxygenase-2 (COX-2; prostaglandin-endoperoxide synthase 2) inhibitory components of CV can protect the kidneys from CDPP nephrotoxicity in rats. CDPP (6.5 mg/kg, intraperitoneally) slightly elevated serum creatinine (Crea) and blood urea nitrogen (BUN) 12 days after treatment. Kidney histology demonstrated extensive tubular epithelial damage and COX-2 immunoreactivity increased 14 days after treatment. A large amount of platinum (Pt) accumulated in the kidney of CDPP-treated rats. Furthermore, CDPP decreased renal iron (Fe), molybdenum (Mo), zinc (Zn), Cu and Mn concentrations and increased plasma Fe and Cu concentrations. CDPP elevated plasma free radical concentration. Treatment with CV alone for 14 days (twice 3 ml/kg/day orally) did not influence these parameters. Chronic CV administration after CDPP reduced renal histological damage and slightly decreased COX-2 immunoreactivity, while failed to prevent the increase in Crea and BUN levels. Blood free radical concentration was reduced, that is, CV improved redox homeostasis. CV restored plasma Fe and renal Fe, Mo and Zn, while decreased Pt and elevated Cu and Mn concentrations in the kidney. Besides the known synergistic antitumour effects with CDPP, CV partially protected the kidneys from CDPP nephrotoxicity probably through its antioxidant effect.
Introduction
Cisplatin (CDPP; cis-diamminedichloroplatinum) is a highly effective chemotherapeutic agent used for the treatment of various malignancies. 1 –5 High-dose CDPP-based combination chemotherapy regimens are used as first-line treatment of small cell and non-small cell lung cancers. 6 –8 However, the use of CDPP is limited by serious side effects. 7,9 Despite the use of different hydration protocols allowing dose escalation to therapeutic levels, nephrotoxicity is the main dose-limiting side effect of CDPP. 10 –14 About 20% of acute renal failure cases were due to CDPP among hospitalized patients. 15,16 High-dose CDPP-induced nephrotoxicity (>25% decrease in estimated glomerular filtration rate) was diagnosed in 29% of patients, following a single dose of CDPP, and temporary elevation of serum creatinine (Crea) concentration above the upper normal limit was observed in 41% of 400 CDPP-treated patients with different solid tumours. 17 Co-morbidities in lung cancer patients greatly increased the incidence of CDPP-induced nephrotoxicity from 7.5% without co-morbidities to 20.9% with concurrent hypertension with or without ischemic heart disease and to 30.8% with diabetes mellitus and ischemic heart disease. 18 Due to the superior efficacy of CDPP against a variety of human carcinomas, intensive efforts have been undertaken to weaken the side effects of CDPP, especially nephrotoxicity.
CDPP accumulates in the kidney and, thus, by far the highest CDPP concentration is measured in the kidney after treatment. 19 Copper (Cu) transporter 1 and the organic cation transporter 2 are critically involved in CDPP uptake into renal tubular epithelial cells consequently determining nephrotoxicity. 20 –23 Oxidative stress, induction of an inflammatory response and direct DNA damage are also implicated in the mechanisms of CDPP-induced nephrotoxicity. 11,13 The importance of oxidative stress has been highlighted by numerous studies demonstrating that antioxidant agents ameliorate CDPP nephrotoxicity in experimental animals. 24 –26 Acute or chronic treatment with vitamin C produced encouraging results in rat experiments. 27 –30 Selenium (Se) 31 or co-administration of vitamin E and Se 32 or acetylsalicylic acid and sodium salicylate was also protective. 33 –35
CV247 (CV) is composed of manganese (Mn) and Cu gluconates, sodium salicylate and ascorbic acid (exact composition is given in the Methods section), which are known to have antioxidant (ascorbic acid, Mn and Cu), cyclooxygenase (COX) and tumour necrosis factor-α (TNF-α) inhibitory (sodium salicylate) effects. CV was shown to decrease the viability of six cancer cell lines in culture and to augment the cytotoxic effect of CDPP against human breast and especially colon carcinoma. 36,37 As some constituents of CV protected against kidney injury as shown above, 32,33 it may also alleviate the CDPP-induced nephrotoxicity by synergistically acting at several target sites. Therefore, the aim of this study was to investigate the net effects of CV on renal function, antioxidant status and kidney histology after CDPP treatment.
Materials and methods
Animals
The study was conducted on 40 males, 8-week-old Wistar rats weighing 175–190 g. The animals were randomly divided into four groups (n = 10/group). They were kept under standard conventional conditions according to European Council Directive 123. The study conformed to the Declaration of Helsinki guidelines and was approved by the local Animal Ethic Committee.
Test materials
CDPP (10 mg in 20 ml) was obtained from TEVA (Petach Tikva, Israel). The composition of CV (Pharmaserve Ltd, Manchester, UK) was the following: 40 mg ascorbic acid, 2 mg Mn gluconate (unique selling proposition), 2 mg Cu gluconate and 35 mg sodium salicylate per millilitre solution (www.ivymedical.com). Methyl-cellulose mucilage (Dow Chemicals, Midland, MI, USA) was prepared in distilled water (1%).
Study protocol
Rats were randomly allocated into four treatment groups. Control (C) rats received 1% methyl cellulose at 10 ml/kg body weight, orally (p.o.) by gastric gavage twice daily for 14 days. Another group of rats received CV at 3 ml/kg body weight p.o. twice daily, 12 h apart, for 14 days (CV). The dose given was 2 × 120 mg/kg/day vitamin C, 2 × 105 mg/kg/day sodium salicylate, 2 × 6 mg/kg/day Cu gluconate and 2 × 6 mg/kg/day Mn gluconate. The above dose was selected based on the previous experience in dogs and also on the results of a previous 26-week repeated dose oral toxicity study (unpublished results; IVM 001/032165, Huntington Life Sciences Ltd). Two further groups were intraperitoneally injected with a single dose of CDPP at 6.5 mg/kg body weight. CDDP dose ranged from 5 to 7 mg/kg in a majority of previous rat studies. 19,22,27 –33,38,39 CDDP was suspended in 10 ml/kg 1% methyl cellulose. CDDP-injected rats were subsequently treated with either vehicle (CDDP) or CV as above (CDDP + CV). The first CV dose followed CDDP by half hour. All rats were weighed and food and water consumptions were also measured daily.
Renal function
On day 12, 1.5 ml of blood samples was taken from all rats by retro-orbital puncture under isoflurane anaesthesia after a 20-h food deprivation. The blood was anticoagulated with citrate and centrifuged twice at 2500 r/min for 10 min at +4°C to obtain plasma. Plasma Crea and blood urea nitrogen (BUN) were determined by colorimetric tests using the commercially available kits. Rats were terminally anaesthetized with an overdose of pentobarbital on day 14. Blood was collected by aortic puncture and the kidneys were removed and weighed.
Induced chemiluminescence in the plasma
A small volume of plasma samples (50–100 μl) was assayed with a hydrogen peroxide (H2O2)/OH–microperoxidase–luminol system for 30 s as described previously. 40 Chemiluminescence was detected in a Berthold Lumat 9501 luminometer (Berthold Technologies GmbH & Co. KG, Bad Wildbad, Germany).
Metal contents in the plasma and kidney
After digestion of the samples in nitric acid (5 ml, 65%) and H2O2 (2 ml, 30%), an inductively coupled plasma (IPC) optical emission spectrometric method was used for measuring the metal content in a Spectro Genesis ICP equipment (Spectro Analytical Instruments GmbH, Kleve, Germany). 41 For the standardization of equipment and measurements of elements, Spectro multielement and Spectrum 3D standards were used. A computer-guided TraceLab 50 type polarographic–voltammetric analyzer was used for the voltammetric determination of Se at −550 mV. 42
Histology and immunohistochemistry
One kidney from all rats was fixed in 8% buffered formalin (pH 7.4), and paraffin sections were prepared and stained with haematoxylin–eosin stain. Renal histological changes were blindly evaluated using a 5-grade severity scale (0 = no change; 1 = minimal changes; 2 = mild changes; 3 = moderate changes; 4 = severe changes). The COX-2 (prostaglandin-endoperoxide synthase 2) immunohistochemistry was carried out using a mouse monoclonal COX-2 primary antibody (Novocastra, Newcastle, UK) at 1:100 dilution. The secondary antibody was a peroxidase-conjugated mouse/rabbit polymer (Dako Real™ Envision™/horseradish peroxidase, rabbit/mouse) (Dako North America, Inc., Carpinteria, CA, USA). Diaminobenzidine was used for visualization.
Statistical analysis
Means ± SD are given throughout. The statistical comparisons were performed by two-way repeated measures analysis of variance (ANOVA) with the Bonferroni post hoc test or Mann–Whitney U test using GraphPad Prism 5 for Windows or by two-way ANOVA using the SPSS 17 for Windows, when appropriate. The level of significance was set at p < 0.05.
Results
Body weight
Body weight of rats steadily increased in group C from 171 ± 8 g to 234 ± 15 g over a study period of 14 days with a drop on day 11 after the overnight food deprivation before blood sampling (Figure 1). In comparison with the baseline value, CDDP caused a 5.5% peak body weight loss (p < 0.001) from 167 ± 6 g to 158 ± 9 g on day 3 after treatment. Thereafter, body weight gain returned to a rate similar to that seen in group C. CV treatment did not influence body weight in comparison with groups C and CDDP, respectively. Consequently, on the last day of the study, body weight of rats treated with CDDP and CDDP + CV was 12–15% lower (p < 0.001) than body weight of rats in groups C and CV.

The effects of acute cisplatin and chronic CV247 administration on the body weight and daily water consumption in rats (n=10/group). Left panel: body weight. The asterisk (*) shows that from day 3 body weight was significantly decreased in the groups treated with cisplatin and cisplatin + CV247 in comparison to the groups treated with vehicle and CV247. Right panel: water consumption. The asterisk (*) shows that from day 5 water consumption was significantly increased in the groups treated with cisplatin and cisplatin + CV247 in comparison to the group treated with vehicle. The open circles show that on days 8, 9 and 11 water consumption was significantly increased in the group treated with CV247 in comparison to the group treated with vehicle. The statistical analysis was performed by two-way repeated measures ANOVA followed by Bonferroni post hoc test.
Food and water consumptions
CV consistently increased water consumption in comparison with group C (Figure 1), which was statistically significant on days 8, 9 and 11 (p < 0.05, all). CDPP caused a short, non-significant decrease in water consumption on day 2 after its administration. Thereafter, from day 4, rats in the CDDP and CDDP + CV groups drank significantly more water than rats in group C. Co-administration of CV to CDPP did not alter water consumption in comparison with the group treated with CDPP only. Neither CDDP nor CV alone or in combination with CDDP altered food consumption (data not shown).
Renal function
Crea and BUN values were within physiological limits in groups C and CV (Crea: 17.0–22.5 µmol/l; BUN: 6.63–10.48 mmol/l). CDDP increased both Crea (p < 0.001) and BUN (p < 0.01) concentrations at day 12 after its administration, while CV did not alter (p > 0.05 both) these effects of CDDP on renal function (Figure 2).

The effects of acute cisplatin and chronic CV247 administration on plasma creatinine and blood urea nitrogen concentration on day 12 in rats (n=10/group). CDDP increased both plasma creatinine and blood urea nitrogen (BUN) concentrations on day 12 of the experiment. CV247 did not alter plasma creatinine and BUN concentrations compared to those of the groups treated either with vehicle or with CDDP. Group effects of CDDP and CV247 and their interaction were obtained from two-way ANOVA.
Plasma reactive oxidant levels increased 14 days after CDDP administration, as measured by chemiluminescence. CV did not alter chemiluminescence in comparison with group C, while CV attenuated the CDDP-induced elevation in plasma reactive oxidant levels (Figure 3).

The effects of acute cisplatin and chronic CV247 administration on the free radical- and reactive oxygen species (ROS)-scavenging ability of the serum of rats measured by chemiluminescence (RLU%) on day 14 after cisplatin administration. Cisplatin increased while CV247 decreased plasma chemiluminescence. Group effects of CDDP and CV247 and their interaction were obtained from two-way ANOVA.
Metal concentrations in plasma and kidneys
Kidney Cu, iron (Fe), Mn, molybdenum and zinc (Zn) concentrations were lower in the kidney 14 days after treatment with CDDP, while cobalt (Co) and Se concentrations did not change (p < 0.05). Treatment with CV increased Mo concentrations in the kidney, while it did not change other element concentrations (Table 1). Co-administration of CV with CDDP restored renal Fe and Zn concentrations to control levels and also increased renal Cu and Mn concentrations significantly, although Cu and Mn remained below the control levels. The effect of CDDP on renal Mo concentration was restored by CV. Still, 14 days after CDDP administration, kidney platinum (Pt) concentration was 3 µg/g versus undetectable values in C rats. CV strikingly reduced kidney Pt concentration by 30% (p < 0.05).
Element concentrations of rat kidneys (μg/g) measured using ICP-OES.
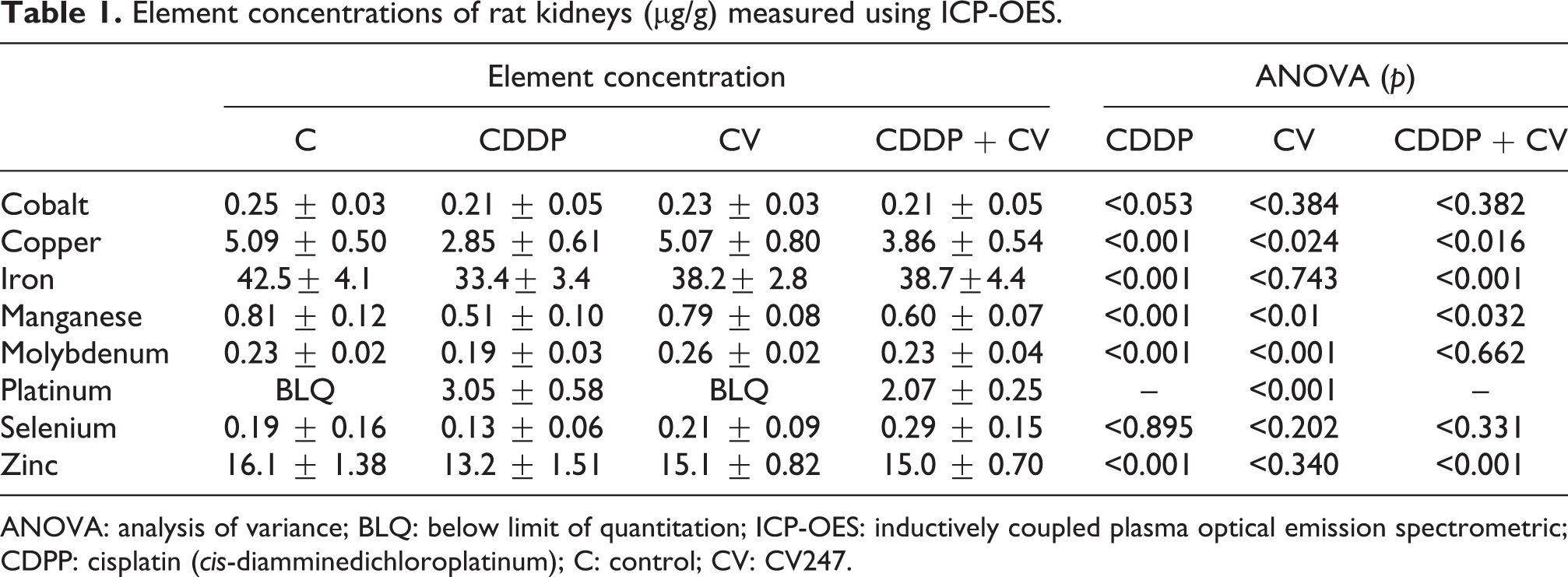
ANOVA: analysis of variance; BLQ: below limit of quantitation; ICP-OES: inductively coupled plasma optical emission spectrometric; CDPP: cisplatin (cis-diamminedichloroplatinum); C: control; CV: CV247.
Plasma concentrations of Pt, Co and Se were undetectable in untreated control animals. CDDP increased plasma Cu and Fe concentrations (Table 2). Co-administration of CV with CDDP restored plasma Fe concentrations, while CV did not alter the effect of CDDP on plasma Co concentrations.
Element content in rat plasma (μg/g) measured using ICP-OES.a

ICP-OES: inductively coupled plasma optical emission spectrometric; CDPP: cisplatin (cis-diamminedichloroplatinum); C: control; CV: CV247.
aPlasma platinum, cobalt and selenium concentrations were below the limit of quantitation in most cases.
Kidney histology and immunohistochemistry
No histological changes were seen in the kidneys in groups C and CV. Varying degrees of pathological changes were found in the kidneys of CDDP and CDDP + CV groups. Renal tubular epithelial cell atrophy was presented by cystic dilatations of the tubular lumina, in which accumulation of desquamated tubular epithelial cells were present as hialynacous material. Many tubular epithelial cells appeared apoptotic or necrotic. In addition, in the damaged tubular epithelium, atypical, regenerating cells were visible. Tubulointerstitial inflammation was indicated by the presence of lymphocytic and macrophage infiltration in the interstitial space, accompanied by interstitial fibrosis appearing as multiple focal presence of fibroblasts (Figure 4). Blind assessment demonstrated a reduction in the mean score severity of histological kidney injury from 3.67 ± 0.50 in CDDP to 2.67 ± 0.71 in CDDP + CV (p < 0.01). Immunohistochemistry revealed a moderate degree of focal COX-2 activity in the cytoplasm of the tubular epithelium in the interstitial space and in the walls of major blood vessels (score, control: 1.20 ± 0.42 and CV: 1.0 ± 0.0). Blind assessment of COX-2 activity revealed that COX-2 immunoreactivity markedly increased in the groups treated with CDDP and CDDP + CV. Treatment with CV did not alter COX-2 immunoreactivity versus C but CV slightly (3.00 ± 0.71 versus 2.44 ± 0.53, p = 0.097, Mann–Whitney test) decreased COX-2 immunoreactivity caused by CDDP (Figure 5).
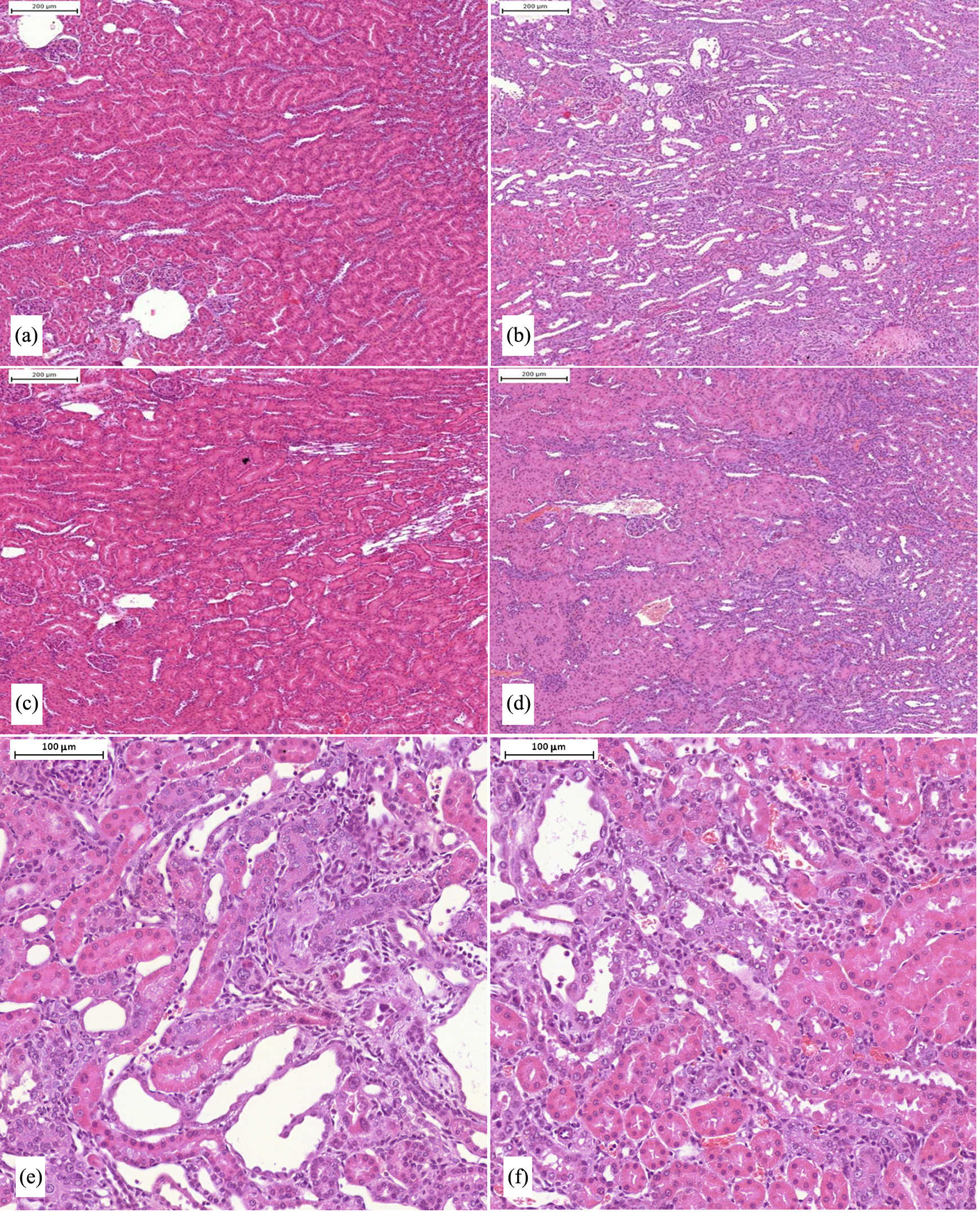
The effects of acute cisplatin and chronic CV247 administration on kidney histology (haematoxylineosin staining). The structure of the kidney was normal in the C (A) and CV groups (C). Severe degree of tubulointerstitial abnormality was present in rats treated with CDDP (B), and similar but significantly less severe (CDDP: 3.67±0.50 vs. CDDP+CV: 2.67±0.71; p<0.01) alterations were detected in the group treated with CDDP+CV (D). See higher magnification of sections from the group CDDP (E) and CDDP+CV (F). Blinded scores of histological abnormalities were statistically compared by two-way ANOVA. (a)=C, (b)=CDPP, (c)=CV, (d)=CDPP+CV, (e)=CDPP-high power, (f)=CDPP+CV-high power.

The effects of acute cisplatin and chronic CV247 administration on COX-2 immunohistochemistry in the renal cortex. Mild activity in the interstitium and tubular epithelium was present in rats treated with vehicle (A) and CV (C). CDDP increased COX-2 activity in the damaged areas of the kidney (B), which effect was almost significantly decreased (3.00±0.71 vs. 2.44±0.53, p=0.097, Mann Whitney test) by CV (D). See higher magnification of sections from the group CDDP (E) and CDDP+CV (F). Blinded scores of COX-2 immunoreactivity were statistically compared by two-way ANOVA. (a)=C, (b)=CDPP, (c)=CV, (d)=CDPP+CV, (e)=CDPP-high power, (f)=CDPP+CV-high power.
Discussion
In the present study, we demonstrated that CV, a potent enhancer of the anti-neoplastic effects of CDPP, effectively protected the kidney from CDPP toxicity as demonstrated by renal histology and restoration of redox and trace metal homeostasis. However, slight renal retention of Crea and BUN 14 days after CDDP injection was not prevented by CV. CV significantly ameliorated renal Pt accumulation, which was still obvious 14 days after CDDP injection.
Histological damage was clearly present on day 14 after CDPP injection and immunohistochemistry revealed marked COX-2 synthesis in the kidney as well as an increase in plasma reactive oxidant levels, detected by chemiluminescence in the CDDP group. CDPP decreased Cu, Mn and Zn concentrations in the kidney, which minerals are essential cofactors of several antioxidant enzymes. Chronic CV treatment reduced renal Pt concentration and offered protection against CDPP-induced nephrotoxicity demonstrated by attenuation of histological injury, restored plasma reactive oxidant levels and renal Cu, Mn, Se and Zn contents on day 14 after CDPP administration. However, small plasma Crea and BUN retentions still present 14 days after CDDP injection were not influenced by CV and renal inflammation, as revealed by COX-2 immunohistochemistry, was only slightly moderated by CV.
It has been reported that CDDP accumulated in the kidney 43 and renal Pt content decreased very slowly after CDPP administration. 38 It was an important observation in our study that chronic treatment with CV significantly decreased kidney Pt content by day 14 in comparison with the CDPP alone group. Since administration of CV did not precede that of CDPP, it can be excluded that CV interfered with renal CDPP uptake. Therefore, it seems likely that long-term administration of CV accelerated elimination of Pt from the kidney. This observation suggests that kidneys of CV -treated rats recovered faster from the CDPP -induced nephrotoxicity.
Most importantly, blind assessment of tissue pathology demonstrated that CV reduced the severity of renal histological injury. This observation seems to be in harmony with attenuation or full reversal of the CDPP-induced decreases in trace mineral content of the kidney. These changes are compatible with the assumption that the concentration of all those enzymes increased in the kidney, which use these minerals as cofactors for achieving their full activity. All these changes seem to suggest that Mn and Cu constituents of CV contributed to improve the biochemical machinery of the kidney. Although, only Mn and Cu were supplemented, it is well known that trace mineral metabolism is subjected to mutual synergisms and antagonisms. 44 Therefore, administration of one or few trace minerals may also consequently alter the concentrations of other minerals in the kidney. In fact, renal Cu, Fe, Mn, Mo and Zn concentrations were lower 14 days after treatment with CDPP, and co-administration of CV with CDPP restored renal Fe and Zn concentrations to control levels and also increased renal Cu and Mn concentrations. However, it is unclear if these beneficial effects of CV were the consequences of Mn and Cu administration or of treatment with an antioxidant and an anti-inflammatory drug. Most likely, the above factors all contributed or even synergized with each other to accelerate the recovery of the biochemical machinery of the kidney and, consequently, to improve its trace mineral metabolism after the CDPP-induced injury.
Sodium salicylate, a component of CV, inhibits the activity of COX (COX-1 and COX-2) isoenzymes. 45 COX-2 inhibition is anti-inflammatory and can be a renoprotective strategy as a highly selective COX-2 inhibitor (SC-58236) reduced urinary excretions of transforming growth factor-β, TNF-α, albumin, prostaglandin E2, 6-keto-prostaglandin F1α and Thromboxane B2 in streptozotocin-diabetic rats. 46 Our immunohistochemistry findings demonstrated that the CDPP-induced elevation in COX-2 expression was slightly reduced by chronic CV treatment. In addition, COX-2 enzyme activity (not measured by immunohistochemistry) may have been further reduced by CV as sodium salicylate inhibits COX-2. 45
The protective effect of sodium salicylate could be attributed to suppression of TNF-α production as well. 34 Treatment with acetyl salicylic acid or sodium salicylate for 4–5 days decreased plasma BUN and Crea at a daily dose similar to that given by us, 35 restored the renal concentration of superoxide dismutase and decreased oxidative stress as shown by renal malondialdehyde concentration in CDPP nephrotoxicity. 33 Such effects of sodium salicylate may help explain why CV accelerated histological recovery of the kidney from CDPP nephrotoxicity in our study.
Even a 10-min pretreatment with various doses of vitamin C restored CDPP -induced increases in plasma Crea, dose-dependently increased renal glutathione concentration and attenuated renal lipid peroxidation as assessed by malondialdehyde levels at 1 week after CDPP injection. 30 One hour pretreatment with a medium dose of vitamin C (100 mg/kg/day) restored the changes in urinary 8-hydroxy-2′-deoxyguanosine caused by CDPP suggesting that vitamin C prevented oxidative DNA damage. 29 A single high vitamin C dose given 6 h prior to CDPP also prevented the decreases in the renal cortical brush border membrane enzyme (alkaline phosphatase, leucine aminopeptidase, gamma-glutamyl transferase and maltase) activities and transport of inorganic phosphate 4 days after CDPP administration. 28 However, the dose of 250 mg/kg was most effective in attenuating CDPP-induced increases in plasma Crea and BUN concentrations but lower and especially higher vitamin C doses were less effective. 28 In a light and electron microscopic study, chronic daily treatment with vitamin C at low dose (8 mg/kg) decreased renal histological injury caused by three repeated CDPP administrations at 21-day intervals. 27 These observations were similar to those seen in our study. Collectively we can conclude that pretreatment with vitamin C at medium–high doses of 100–250 mg/kg can attenuate CDPP-induced nephrotoxicity.
Transition metal ions are ubiquitous in biological systems as they play a key role in the catalysis of redox reactions and some of them (Cu, Fe, Mn and Zn) significantly modify signal transduction. Cu, Fe, Mn, Zn and also Se are essential in the antioxidant defence since metalloproteins, such as superoxide dismutase (superoxide dismutase with copper and zinc) in the cytoplasm or the nucleus, superoxide dismutase with manganese (MnSOD) in the mitochondrial matrix, catalase with iron in the cytoplasm or peroxisomes and glutathione peroxidase glutathione peroxidase with selenium in the cytoplasm are important antioxidant enzymes. On the other hand, redox-active metal ions, for example, Fe and Cu may catalyze the production of reactive oxygen species.
The concentration and concentration ratio of transition metal elements are rigorously regulated in health but not in disease. Therefore, restoring transition metal ion balance is essential in disease states. CDPP elevated Fe concentration in the plasma, which may induce free radical reactions. 47 Treatment with CV alleviated CDPP-induced increase in plasma Fe concentration. Otherwise, plasma metal element content hardly differed from the control in the rats treated either with CV or CDPP + CV. The restoration of plasma Fe concentration in rats treated with CDPP + CV was very favourable and may explain the significant decrease in chemiluminescence intensity in the plasma.
There is always some concern whether the efficacy of a drug is impaired or not when its side effects are aimed to be reduced by administration of an adjuvant. CV has been shown to have a antiproliferative effect at the G2 phase in four malignant human cells lines (breast, prostate, colon and lung), and CV appeared to have a synergistic effect with CDPP in three breast and three colon carcinomas by increasing the cytotoxic efficacy of CDPP upto fourfold in cell culture. 36,37 These observations suggest that besides offering some protection from nephrotoxicity, CV may allow CDPP dose reduction without altering its efficacy.
CDPP also blocked the normal accumulation of Cu and Zn in the kidney. 39 CV treatment was able to inhibit the depletion of Cu and Mn, but not of Zn.
In conclusion, the current study demonstrated that chronic CV administration after treatment with CDPP offered some protection against nephrotoxicity at 2 weeks in rats. Since previous studies have shown that CV had direct toxic effects on malignant cells and also synergically increased the anticancer effect of CDPP in cancer cell lines, CV may enable dose reduction in CDPP in cancer patients. A lower CDPP dose and a partial protection against nephrotoxicity may considerably reduce the side effect of CDPP in patients treated with CV. However, further pharmacological studies are needed to demonstrate that CV also increases the anticancer effect of CDPP in whole animal cancer models.
Footnotes
Acknowledgements
We express our thanks to Dr Peter Karran, Head of Mammalian Cell DNA Repair Department, Cancer Research UK, London Research Institute, Herts, UK and to Dr Anikó Bohács, Assistant Professor, Department of Pulmonology, Semmelweis University, Budapest, Hungary for their contribution.
Conflict of interest
The authors declared no conflicts of interest.
Funding
The study was supported by Ivy Medical Chemicals Plc (Essex, UK).