
Abstract
Purpose:
We aimed to evaluate the articular involvements in pediatric patients with familial Mediterranean fever (FMF) with joint symptoms by bone scintigraphy and to correlate the involved joints with the gene mutations.
Materials and methods:
A total of 41 newly diagnosed patients in pediatric age group (28 girls and 13 boys; mean age 9.14 ± 2.91 years) with joint involvement symptoms were included in this study. Scintigraphic images were obtained at 5th min (blood pool or early phase) and starting at 3 h (late phase) after (after tracer injection) intravenous administration of technetium-99m (99mTc)-methylendiphosphonate (MDP). Genomic DNA was isolated from leukocytes using standard salting out procedure. The sequencing data were analyzed.
Results:
Of the 41 patients, arthritis was found in 21 (51.2%) patients. Of the 21 patients, there was single joint involvement in 15 (71.4%) patients and multiple joint involvement in six (28.6%) patients. The mean age of patients with joint involvement (8 ± 2.3 years) were considerably lower than the patients without joint involvement (10.35 ± 3.04 years), and this was statistically significant (p = 0.008). The most commonly involved joints were ankles and knees. Multiple joint involvements were most frequently observed in the M694V and M694I gene mutations (16.7%).
Conclusions:
We use and recommend the bone scintigraphy in patients with FMF to determine the presence and distribution of arthritis, since bone scintigraphy is inexpensive, noninvasive, easy-to-use, and also is more sensitive in the diagnosis and distribution of arthritis than conventional radiological methods and clinical examination.
Introduction
Familial Mediterranean fever (FMF) is an autosomal recessive inflammatory disease, which is also called as paroxysmal polyserositis. Recurrent attacks of fever as well as abdominal, chest, and joint pain due to inflammation of serosal membranes are the characteristic symptoms. 1,2
Janeway and Rosenthal reported the first case of FMF in 1908 as “paroxysmal unusual syndrome” (a 16-year-old girl with intermittent abdominal pain and fever). 3 However, it has remarkable clinical properties; the first description of FMF was made in 1945. 4 The primary affected population of the disease is the people living around the Mediterranean basin. In addition, FMF is now a worldwide disease due to the intercontinental trips. 5
Clinical features are the basis of diagnosis. Mediterranean fever (MEFV; the gene for FMF) was first identified in 1997 by positional cloning. 6 It is found on the short arm of chromosome 16. Four missens mutations in exon 10 were established (M694V, V726A, M694I, and M680I). 7 Pyrin/marenostrin, the product of MEFV gene, is expressed in polymorphonuclear cells and monocytes. Pyrin/marenostrin may be the regulator of inflammatory response at the level of leukocyte cytoskeleton organization. 8,9
Increased incidence of arthralgia and arthritis as well as more severe and early onset FMF are associated with homozygous gene mutation. 1,5 The estimated prevalence of FMF in Turkey is 1 of 1000 and the carrier rate is 1:5. 10 In Turkey, rate of arthritis is 40–70%, and in one third of these patients, it is the first sign of the disease. 11
Articular involvement in early onset FMF is a common finding that lasts in a few days. Self-limited, nonerosive, asymmetric monoarthritis is the general clinical presentation. 12 The arthritis occurs in larger joints like knees, ankles, wrists, sacroiliac, shoulder, and so on. 13
Bone scintigraphy is very effective technique in the diagnosis of arthritis. It is more sensitive than clinical examination or conventional radiological imaging. Scintigraphy presents a greater visualization of disease in multiple sites at once, so it provides earlier diagnosis. 14 Also bone scintigraphy has the unique capability of indicating metabolically active joints at the same time with localized joint disease. 15
In this present study, using bone scintigraphy, we aimed to evaluate the articular involvements in pediatric patients with FMF with joint symptoms and to correlate the joints involved with the gene mutations. To our knowledge, this is the first report in which bone scintigraphy has been used in the evaluation of articular involvement and genetic correlation of pediatric patients with FMF.
Materials and methods
A total of 41 newly diagnosed pediatric patients with FMF, complaining of arthritis or arthralgia, were included in this study. Bone scintigraphy was performed on all the 41 consecutive pediatric patients with FMF. At the time of scintigraphic assessment, all the patients were in the attack-free period. The study was approved by the ethical committee of the Mustafa Kemal University, Education and Research Hospital, and all the children and their caregivers gave informed consent to the study.
All of the patients were living in the southern part of Turkey. The diagnosis of FMF was determined according to the criteria described by Livneh et al. (Table 1) and was supported by genetic studies. 16 Requirements for the diagnosis of FMF are the presence of one major criterion or two minor criteria. Typical attacks are defined as recurrent (three at the same site), febrile (38°C rectal temperature), and short (lasting 12 h to few days). Incomplete attacks are defined as painful and recurrent attacks differing from typical attacks in one or two features as follows: (1) temperature is normal or lower than 38°C, (2) attacks are longer or shorter than specified (but not shorter than 6 h or longer than a week), (3) no signs of peritonitis are recorded during the abdominal attacks, (4) the abdominal attacks are localized, and (5) the arthritis involves joints other than those specified. Attacks not fulfilling this definition of typical incomplete attacks are not counted.
Criteria for the diagnosis of Familial Mediterranean fever.

Scintigraphic imaging
Radionuclide was extracted from technetium-99m (99mTc) generators (Mon-Tek, Eczacibasi Monrol, Istanbul, Turkey), and methylendiphosphonate (MDP) (Mon.MDP Kit, Eczacıibasi Monrol, Istanbul, Turkey Eczacıbaşı/Monrol) was labeled and characterized according to the manufacturer’s recommendations. Images were obtained with dual-head gamma cameras (Symbia S, Siemens Healthcare, Munich, Germany) with low-energy high-resolution dual-head parallel-hole collimators.
Scintigraphic images were obtained at 5th min (blood pool or early phase) and at 3 h (late phase) after intravenous administration of 99mTc-MDP. The 99mTc-MDP doses were estimated due to the body weights of the patients (200 µCi (7.4 MBq) × body weight (kg)). 17,18 Whole-body scanning of anterior and posterior static images were obtained at early and late-phase. In addition, static views of the entire joints with increased activity were performed. All bone and joint scan images were visually assessed.
Genetic analysis
Genomic DNA was isolated from leukocytes using standard salting out procedure, as described by Miller et al. 19 Mutations of exons 2 and 10 in the MEFV gene were amplified by polymerase chain reaction (PCR) using the commercially available forward and reverse primers (GML SeqFinder Sequencing System, Wollerau, Switzerland). Each primer was used to perform both genomic DNA amplification and sequencing reactions. PCR was performed in a total volume of 25 μl PCR mixture containing 100 ng of genomic DNA, 12.5 μl of 2× reaction buffer (GML), and 5 pmol of each primer (Biomers, Germany). After an initial denaturation step at 95°C for 10 min, samples were subjected to 35 cycles of PCR at 95°C for 40 s, at 62°C for 1 min, and at 72°C for 50 s, with a final extension step at 72°C for 7 min. Amplified products were verified by electrophoresis using 2% agarose gel. Cycle-sequencing reactions were performed in both forward and reverse directions in terminator ready reaction mixture containing Big Dye Terminator v3.1 Cycle Sequencing Kit (Applied Biosystems, California, USA) and submitted to 25 cycles at 96°C for 10 s, 50°C for 5 min, and 60°C for 4 min. After the purification of cycle sequencing products, 5 μl of the marked and purified DNA were analyzed by capillary electrophoresis on an ABI PRISM 3130 Genetic Analyser (Applied Biosystems). The sequencing data were analyzed with SeqScape 4.1 (Applied Biosystems).
Statistical analysis
Data were analyzed using the Statistical Package for Social Sciences software (SPSS Inc, Chicago, Illinois, USA) version 15.0. The frequency and distribution of descriptive data were analyzed statistically. A chi-square test was used for comparisons between nonparametric variables. Intercorrelations between the nonparameterics were computed through the Spearman’s correlation analysis, while between the parametrics were computed through the Pearson’s correlation analysis. p < 0.05 were considered as statistically significant.
Results
There were 41 pediatric patients (28 girls and 13 boys; mean age 9.14 ± 2.91 years). Age distribution by gender was homogeneous. Of 41 patients, arthritis was found in 21 (51.2%) patients. Of the 21 patients, there was single joint involvement in 15 (71.4%) patients and multiple joint involvements in six (28.6%) patients (Figures 1 and 2). There was no significant difference between the sex and the number of involved joint. The mean age of patients with joint involvement (8 ± 2.3 years) was considerably lower than the patients without joint involvement (10.35 ± 3.04 years), and this was statistically significant (p = 0.008). There was a negative correlation between age and number of involved joints (r = −0.375; p = 0.01). The most common involved joints were ankles and knees (Table 2).
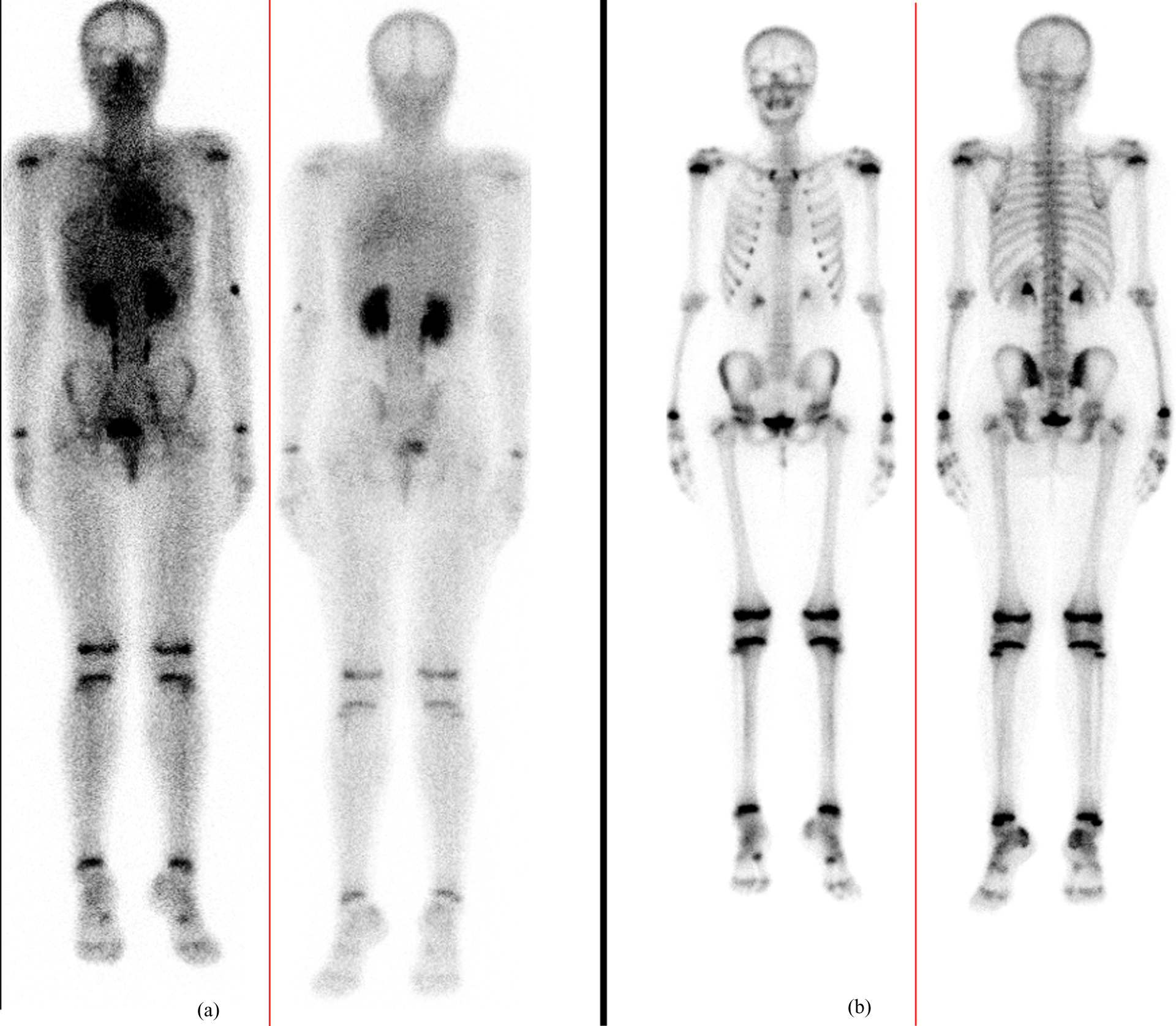
Tarsometatarsal joint involvement. (a) Whole-body blood pool image shows bilateral focal tarsometatarsal hyperemia. (b) Whole-body late-phase image shows bilateral focal increased activity of tarsometatarsal joints.
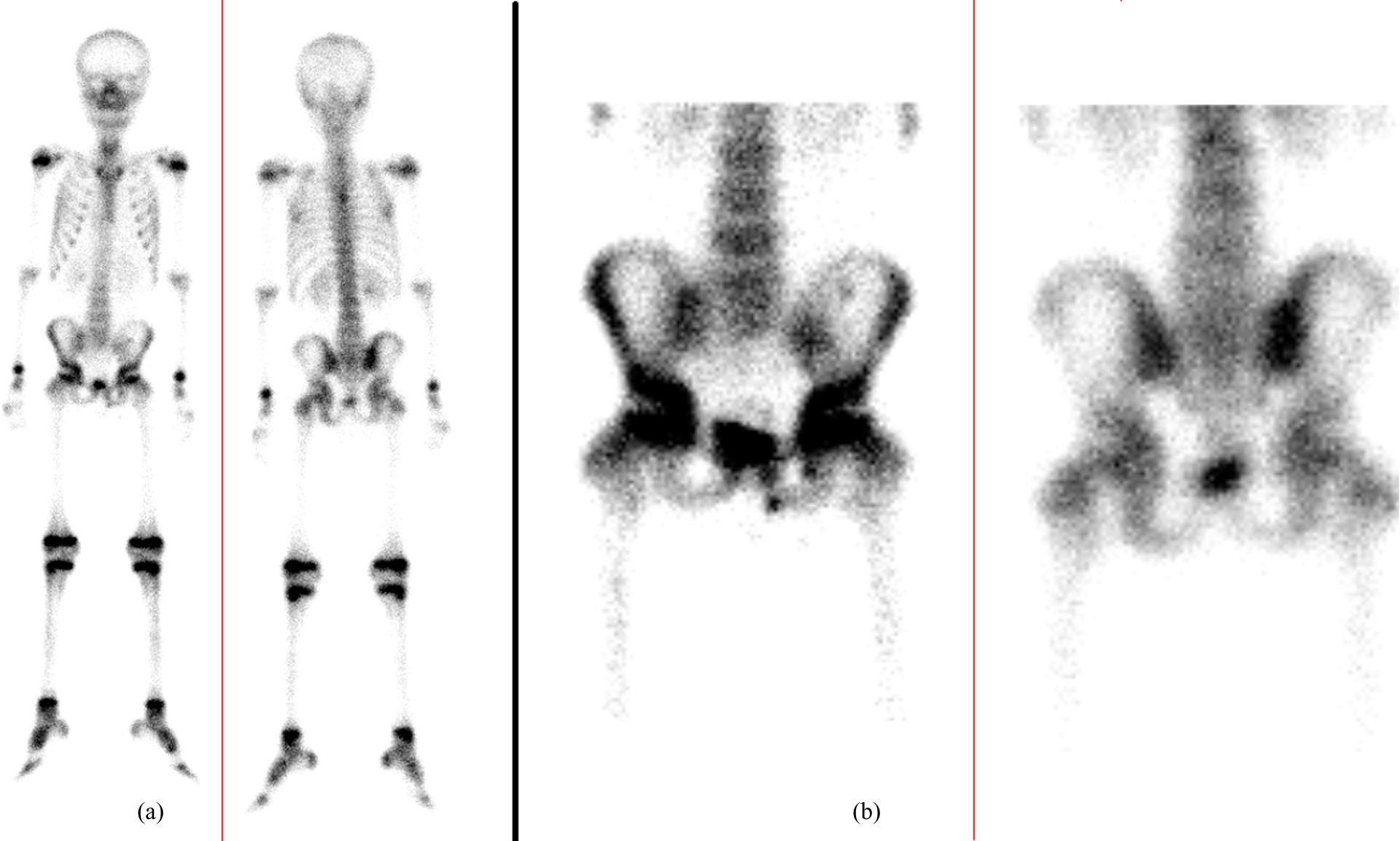
Increased activity in right sacroiliac joint: (a) whole-body scan and (b) anterior and posterior static images.
Involved joints revealed by bone scintigraphy.

Gene analysis revealed the following mutations: E148Q in 10 patients (24.4%), G138G, A165A, and R202Q in 19 patients (46.3%), M694V and M694I in six patients (14.6%), and G196W in one patient (2.4%). Gene analysis was normal in five patients (12.2%). Totally, 31 patients had a heterozygous mutation (75.6%) in the gene, while five patients had a homozygous mutation (12.2%) in the gene; 30 patients (73.1%) had mutations in exon 2. According to the gene analysis, joint involvement was evaluated with E148Q gene mutation (60%) in six patients, with G138G, A165A, and R202Q gene mutation (46.3%) in nine patients, with M694V and M694I gene mutation (50%) in three patients, with G196W gene mutation (100%) in one patient, and with normal chromosome analysis (40%) in two patients (Table 3). There was no correlation between the gene mutations and the joints affected (r = −0.104; p = 0.5). Multiple joint involvements were most frequently observed in the M694V and M694I gene mutations (16.7%).
The mutations according to the affected joints.

Discussion
Generally, symptoms of FMF through the clinical findings appear during the first decade of life. Abdominal pain is the most seen symptom of FMF, and the articular disease follows this. To reveal the arthritis, bone scintigraphy using 99mTc-MDP is one of the most preferred techniques. Arthritis may occur as synovial and intra-articular disease or with bone involvement. 20 Since synovitis may be associated with bone erosion, and primary bone disease may have an element of synovitis, there is often some overlap with primary periarticular bone disease. 20 In the inflamed joints, there is high bone turnover and this causes an increased uptake of 99mTc-MDP. The 99mTc-MDP also concentrates in the areas of increased vascularity. 21 In synovitis, anastomotic vessels from inflamed synovium to bone cause increased periarticular uptake of the 99mTc-MDP skeletal imaging agents. 22
Scintigraphic evaluation occurs before radiographic changes are evident, and this allows early diagnose of disease, although involvement in joints is asymptomatic. 14 The conventional radiographic imaging is not specific and the imaging results are reported in terms of soft tissue swelling and transient osteoporosis; in chronic cases, joint-space narrowing, osteophytic formation, and sclerosis may be observed.
In our study, joint involvement was present in 21 (51,2%) of the 41 patients with FMF. Arthritis (51.2%) was more common in our study when compared with the previous studies. Rate of arthritis was reported as 40.2–47.41% in some other studies. 10,23 This may be related to the used imaging methods. Bone scintigraphy is more sensitive in the determination of arthritis than clinical examination and conventional radiological methods; so scintigraphy allows earlier diagnosis and reveals the presence of disease in multiple sites. 24 The large joints of lower extremities are the most effected sites from the arthritis of FMF; in our study, the most effected joints were ankle and knee. The other sites that may be involved are shoulder, temporomandibular, and sternoclavicular joints. 5,6,15 Also, the involvement of sacroiliac joints, small joints, and spinal joints has been reported. 6,16 In our study, hip, shoulder, sacroiliac, and metatarsophalangeal joints were also affected. No correlation between the region of joint involvement, age, and sex was found. 24
Heller et al. reported that articular disease in FMF occurs at an early age and usually affects only single large joint. 25 In our study, the mean age of patients was lower than those who had no arthritis as other previous studies, and this was statistically significant (p < 0.05).
The identification of the FMF gene and the mutations of it maintain a great advantage for medical and genetic counseling for clinical treatment of patients with FMF and their families. 23 Most of the mutations are carried by exons 2 and 10. The most encountered mutations are M694V (more common among Jews, Turks, and Ermenians), M680I (more common among Armenians), M694I (more common among Arabs), E148Q (most common mutation in European and Turkish carriers), and V726A. 5 Of the 41 patients, 36 were identified to have at least one MEFV mutation. It is now known that the presence of M694V mutation is related to the incidence of arthritis. 26 The reports about the role of E148Q mutation in FMF are conflicting. In some studies, it was reported as a sequence variant, 27 while the others reported it as a part of complex V726A, E148Q allele, and this might had severe effects in patients.
Although joint involvement frequently occurs due to M694V gene mutations, arthritis was seen most frequently in E148Q gene mutation in our study. 26,27 The second frequent mutations causing arthritis were M694V-M694I gene mutations. Also multiple joint involvements were seen with M694V-M694I mutations in this study. There was some heterogeneity in the origin of all the patients. They were living in southern parts of Turkey, and some of them had Turkish, Arabian, Armenian, Jewish, and European origin because of the ethnic characteristics of this region. The small number of cases with joint complaint and the ethnic diversity in the region were the limitations of the study.
Conclusion
FMF is a recessive hereditary disease. It can be diagnosed according to clinical features, and genetic analyses may support the diagnosis. According to the ethnicity in the living region, FMF gene mutations may differ. FMF is often presented with lower-extremity single large joint disease such as arthritis of knee and ankle. We recommend the bone scintigraphy in patients with FMF to determine the presence and distribution of arthritis, since bone scintigraphy is inexpensive, noninvasive, and easy-to-use and also is more sensitive in the diagnosis and distribution of arthritis than conventional radiological methods and clinical examination. 23
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declared no conflicts of interest.