
Abstract
The aim of this study is to investigate the effects of the Ankaferd Blood Stopper® (ABS), on cell viability, cytotoxicity, and erythrocyte numbers in in vitro cultured human blood cells. We studied the cytotoxic effects of the ABS using lactate dehydrogenase (LDH) assay, cell proliferation (WST-1) assay and hemolytic assay. The cytotoxicity increased when cells were treated with ABS dilutions of 5%, 12.5%, 25%, and 50% (p < 0.05). Moreover, treatment of the cells with the same concentrations significantly elevated the cell number at 24 and 48 h (p < 0.05). ABS causes a significant increase (p < 0.05) in the hemolytic activity on human erythrocytes and hemolytic activity increases with increase in ABS concentrations. The red blood cell aggregation and cell membrane disruption during the coagulation process lead to induction of hemolytic activity and increase of LDH level in cell culture medium. In addition, ABS has proliferative effects on human leukocytes. Based on these results, ABS can be used as an alternative blood stopping agent safely.
Introduction
Ankaferd Blood Stopper® (ABS) is a unique folkloric medicinal plant extract. The basic principle of ABS is the formation of an encapsulated protein network providing focal points for vital erythrocytes to aggregate on. The ABS-induced protein network formation involves blood cells, particularly erythrocytes, aggregation but does not affect the physiological individual coagulation systems. 1 ABS is a standardized mixture of the plants Thymus vulgaris (dried leaf), Glycyrrhiza glabra (dried leaf), Vitis vinifera (dried leaf), Alpinia officinarum (dried leaf), and Urtica dioica (dried root; Table 1); each of these has some effects on the endothelium, blood cells, angiogenesis, cellular proliferation, vascular dynamics, and/or cell mediators.1–3
Ingredients of ampoule of ABS

T. vulgaris has antispasmodic, carminative, diaphoretic, expectorant, and sedative properties. As a mixture, extract, or infusion, thyme is frequently used in throat and bronchial problems as well as for diarrhea, chronic gastritis, and loss of appetite.4,5 G. glabra also has anti-inflammatory, antithrombin, antiplatelet, antioxidant, antiatherosclerotic, and antitumor activities.1,6 V. vinifera seed extract in particular has been reported to possess a broad spectrum of pharmacological and therapeutic effects such as antioxidative, anti-infammatory, and antimicrobial activities as well as having cardioprotective, hepatoprotective, and neuroprotective effects. 7 Ethnomedical uses for A. officinarum have been found against rheumatism, bronchial catarrh, bad breath, ulcers, whooping cough in children, throat infections, and to control incontinence. 8 Finally, extracts of U. dioica have been reported to have an acute diuretic and hypotensive effects, 9 cardiovascular effects, 10 and can stimulate the proliferation of human lymphocyte. 11
The ABS has dual diverse dynamic reversible actions on the endothelial protein C receptor (EPCR) and plasminogen activator inhibitor-1 (PAI-1), depending on the dose and concentration of EPCR and PAI-1 inside the vascular endothelial cells in the model of human umbilical vein endothelial cells (HUVECs) and have a role on numerous cellular functions as well as its hemostatic actions. Based on these findings, sudden antihemorrhagic efficacy of ABS has been attributed to its immediate enhancement of expression of prohemostatic PAI-1 and downregulated anticoagulant EPCR, resulting in the unique hemostatic effects of ABS. This mechanism could also be important to elucidate the effects of ABS in a given tissue.12,13 Also, Ankaferd has ototoxic side effects and prolonged mass effects in rats. 14
Crucial proteomic components of the ABS-induced erythroid-protein network have been revealed by Demiralp et al. 15 Proteins of plant origin in Ankaferd are nicotinamide adenine dinucleotide phosphate (NADP)-dependent-malic enzyme, ribulose bisphosphatecarboxylase-large chain, maturase K, adenosine triphosphate (ATP) synthase subunit-β, ATP synthase subunit-α, chalcone-flavanone isomerase-1, chalcone-flavanone isomerase-2, and actin-depolymerizing factor. Functional proteomic studies revealed that proteins resembling human peptides within Ankaferd have detected 35 different proteins, including ATP synthase, dynactin 5, nicotinamide adenine dinucleotide (NADH) dehydrogenase (ubiquinone) 1-α-subcomplex, mitochondrial NADP(+)-dependent malic enzyme 3, and nuclear factor 1B-type. 16
Ankaferd establishes a very fast and solid protein web and also alters the levels of transcription factors, such as activating protein 2 (AP2), androgen receptor (AR), cyclic AMP response element or activating transcription factor 1 (CRE-ATF1), cyclic AMP response element-binding protein (CREB), early growth response (E2F1-5, E2F6, EGR), globulin transcription factor (GATA), hepatocyte nuclear factor-1 (HNF1), interferon (IFN)-stimulated response element (ISRE), Myc-Max, nuclear factor-1 (NF1), nuclear factor kappa B (NF-Kb), protein 53 or tumor protein 53 (p53), peroxisome proliferator-activated receptor (PPAR), SMAD2/3, SP1, TPA response element/activating protein 1 (TRE/AP1), and Yin Yang 1 (YY1), in Human Umbilical Vein Endothelial Cells (HUVECs). 17 In another study, Albayrak et al. reported that the addition of ABS into the serum of both multiple myeloma and the control groups resulted in significant decreases in the level of total protein, albumin, immunoglobulin G (IgG), IgA, and IgM. 18
Furthermore, critical experiments are focusing on the effects of ABS in the vessels and tissues. ABS administered to experimental major arterial vessel injuries has reduced both bleeding time and blood loss under conditions of normal and elevated intra-arterial blood pressure. ABS-induced erythroid aggregation was prominent at the vascular tissue level. 19 For most patients, 1 or 2 mL of ABS was enough for adequate control of bleeding during dental extractions and periodontal surgery. 20 In the cases of severe hemorrhaging, ABS may act as a topical biological response modifier in the renal tubular cellular microenvironment. ABS induces downregulations in the expressions of apoptotic molecules. 21
ABS has been safely used in patients to treat epistaxis, 22,23 after tonsillectomy, 24 adenoidectomy, 25 and total thyroidectomy 17 or even variceal bleeding. 26 In addition, ABS has been used to control upper gastrointestinal bleeding, 27 life-threatening arterial bleeding of the digestive tract, 28 and bleeding due to solitary rectal ulcer. 29 Moreover, the levels of coagulation factors II, V, VIII, IX, X, XI, and XII were not affected by ABS; therefore, ABS might be used in patients with deficient primary hemostasis. 30 The biological and toxicological properties of biomaterials are important for their clinical usage. 31 In vitro cytotoxic screening as a primary factor of biocompatibility is determined by cell culture. The most appropriate cells (i.e. cells homologous to the human tissues of ultimate concern) should be selected for in vitro toxicity tests. 32
The aim of this study was to evaluate the cytotoxicity of ABS using lactate dehydrogenase (LDH) assay, cell proliferation (WST-1) assay, and hemolytic assay.
Materials and methods
Materials
All products used for cell culture (Roswell Park Memorial Institute (RPMI), fetal bovine serum (FBS), Ficoll,
Isolation of PBMCs
The peripheral blood mononuclear cells (PBMCs) were isolated from heparinized blood samples by density gradient centrifugation with Ficoll. For LDH and WST-1 assays, PBMC samples were incubated in RPMI1640 medium with 2 mmol/L
LDH assay
A second set of cells were exposed to the test compounds for the LDH assay, which was performed using the LDH Cytotoxicity Detection Kit (Roche). For this assay, a positive control, leading to 100% cytotoxicity by lysing the cells completely, was included. The positive control was 2% Triton X-100 solution in the assay medium, as proposed by the manufacturer. After preincubation of the cells, but before the addition of the test compounds, the growth medium was exchanged from a medium containing 5% FBS to a medium containing only 1% FBS. For testing the released LDH activity, 100 μL of culture medium was transferred to a new 96-well plate at 24 and 48 h. Reaction solution of 100 μL was added from the kit, containing the detection dye, and the catalyst was then added and absorption was measured after 30 min at 490 nm with 655 nm as the reference wavelength in an enzyme-linked immunosorbent assay (ELISA) reader (BioTek-Power WaveS, USA). A culture medium without cells was used as a blank. As for the other assays, background values from wells without cells were subtracted and average value of the six times was calculated. Means ± SD values were represented in Table 2. Cytotoxicity was then calculated according to the following equation

The cytotoxic effects of different concentrations of Ankaferd on human lymphocyte culture a
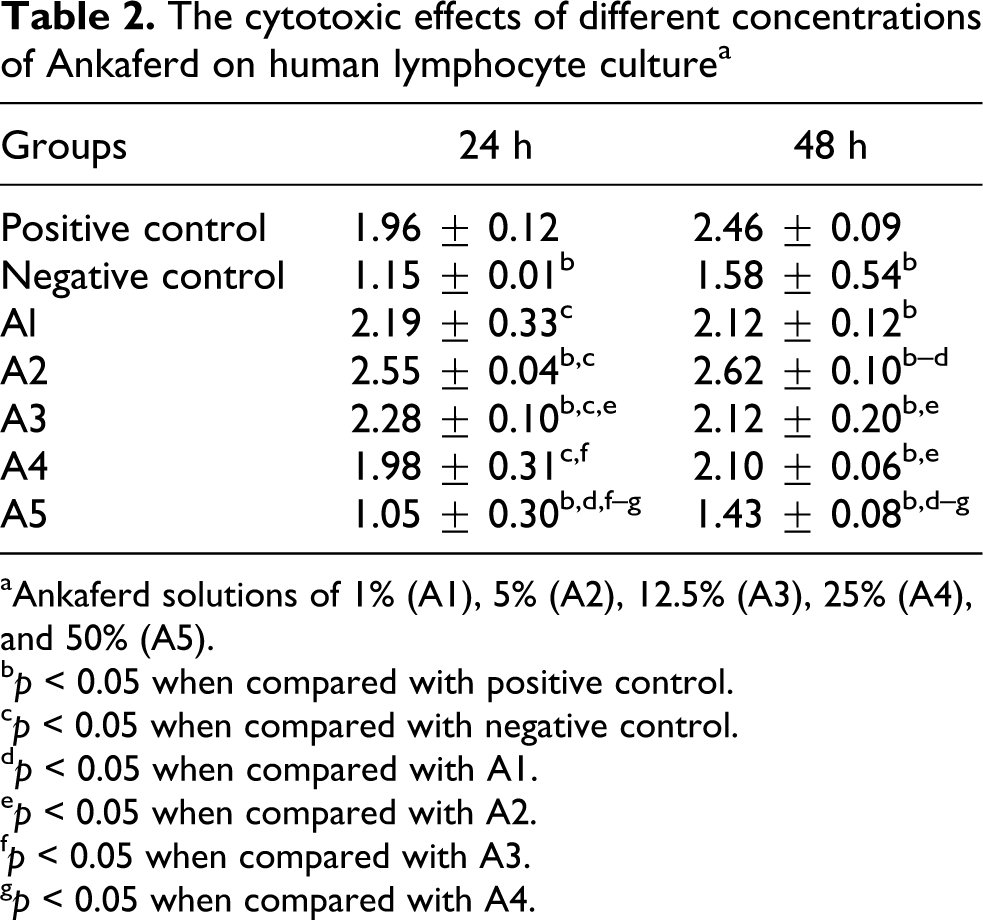
aAnkaferd solutions of 1% (A1), 5% (A2), 12.5% (A3), 25% (A4), and 50% (A5).
b p < 0.05 when compared with positive control.
c p < 0.05 when compared with negative control.
d p < 0.05 when compared with A1.
e p < 0.05 when compared with A2.
f p < 0.05 when compared with A3.
g p < 0.05 when compared with A4.
Cell proliferation (WST-1) assay
For WST-1 assay, cells were cultured in the microplates (tissue culture grade, 96 wells, and flat bottom) with a final volume of 100 μL/well culture medium in a humidified atmosphere (37°C and 5% CO2). Cell proliferation reagent WST-1 was added in a 10-μL/well volume. Cells were incubated for 4 h in a humidified atmosphere (37°C and 5% CO2). The sample absorbances were measured at 420 nm with ELISA reader (BioTek-PowerWaveS, USA). Means ± SD values were represented in the Table 3. Culture medium without cells was used as a blank.
The cell proliferation effects of different concentrations of Ankaferd on human lymphocyte culture a

aAnkaferd solutions of 1% (A1), 5% (A2), 12.5% (A3), 25% (A4), and 50% (A5).
b p < 0.05 when compared with negative control.
c p < 0.05 when compared with A1.
d p < 0.05 when compared with A2.
e p < 0.05 when compared with A3.
f p < 0.05 when compared with A4.
Hemolytic assay
Erythrocytes (red blood cells (RBCs)) were separated from plasma by centrifugation (400g at 10°C for 10 min) and washed twice with phosphate-buffered solution (PBS); then a first dilution (1:9) of erythrocytes in PBS at a final concentration of around 2.56 × 108 RBCs/mL was prepared. Cells were incubated for 15 min in 37°C and 5% CO2. After the incubation period, erythrocytes were separated by centrifugation (300g at 10°C for 10 min). A 200-mL portion of each supernatant was further transferred to a microwell plate to measure the absorbance at 405 nm into a microplate reader. Percentage hemolysis was calculated according to the following formula
Also the number of erythrocytes in the experimental groups was scored using hemacytometer.
Statistical analysis
The statistical analysis of LDH and WST-1 data was performed using the Mann-Whitney U test. A value of p < 0.05 was accepted as statistically significant. Results were expressed as mean ± SD. The statistical analysis of human erythrocyte number was evaluated using χ2 test. For these procedures, SPSS 15.0 version for Windows (SPSS Inc, Chicago, Illinois, USA) was used.
Results
LDH assay results
The cytotoxic effects of different doses of ABS on human lymphocytes at 24 and 48 h are represented in Table 2 and Figure 1. All the ABS concentrations except its 1% dilution caused the releasing LDH and cytotoxicity. Increases in the level of LDH were observed after treatment with 50%, 25%, 12.5%, and 5% dilutions of ABS when compared with negative control groups. This increase was found to be statistically significant (p < 0.05). The highest cytotoxic effect of ABS was in the 25% dilution. As seen in the Figure 2, when the ABS concentrations were increasing, the agglutination of lymphocyte was observed.

The cytotoxic effects of different concentrations of Ankaferd on human lymphocyte culture. NC: negative control; A1: 1% Ankaferd solution; A2: 5% Ankaferd solution; A3: 12.5% Ankaferd solution; A4: 25% Ankaferd solution; A5: 50% Ankaferd solution.

View of comparison effects of different concentration of Ankaferd on human lymphocyte culture cells (×10 magnification). (a): negative control group; (b): 1% Ankaferd solution; (c): 5% Ankaferd solution; (d): 50% Ankaferd solution.
Cell proliferation (WST-1) assay results
Table 3 and Figure 3 represent the results of the cell viability part of the present study, including the WST-1 assay in the control and experimental groups. Increases in the cell proliferation was observed after treatment with different concentrations of ABS. Statistical analysis showed a significant difference in cell viability between all the treated groups and the control group at 24 and 48 h. WST-1 assay results show that the cell proliferation increased when cells were treated with different ABS concentrations at 24 and 48 h (p < 0.05). ABS at a concentration of A5 (50%) significantly increased cell proliferation at all time points during the 24 and 48 h (p < 0.05) in comparison with all the concentrations and control. LDH release significantly correlated with increased cell proliferation. ABS at concentrations of A1 (1%), A2 (5%), A3 (12.5%), and A4 (25%) significantly increased cell proliferation at all time points during 24 and 48 h (p < 0.05) in comparison with control.

The cell proliferation effects of different concentrations of Ankaferd on human lymphocyte culture. NC: negative control; A1: 1% Ankaferd solution; A2: 5% Ankaferd solution; A3: 12.5% Ankaferd solution; A4: 25% Ankaferd solution; A5: 50% Ankaferd solution.
Hemolytic assay result
ABS cause the hemolytic activity on human erythrocytes (RBC) as seen in Figures 4 and 5. Such an increased was found to be statistically significant (p < 0.05). On the other hand, the number of RBCs was reduced by all the ABS concentrations. Especially, in the 12.5%, 25%, and 50% dilutions of ABS, the number of erythrocytes was found to be very low.

Hemolytic activities of different concentrations of Ankaferd on human red blood cells. NC: negative control; A1: 1% Ankaferd solution; A2: 5% Ankaferd solution; A3: 12.5% Ankaferd solution; A4: 5% Ankaferd solution; A5: 50% Ankaferd solution; a: p < 0.05 when compared with negative control; b: p < 0.05 when compared with A1; c: p < 0.05 when compared with A2; d: p < 0.05 when compared with A3; e: p < 0.05 when compared with A4.
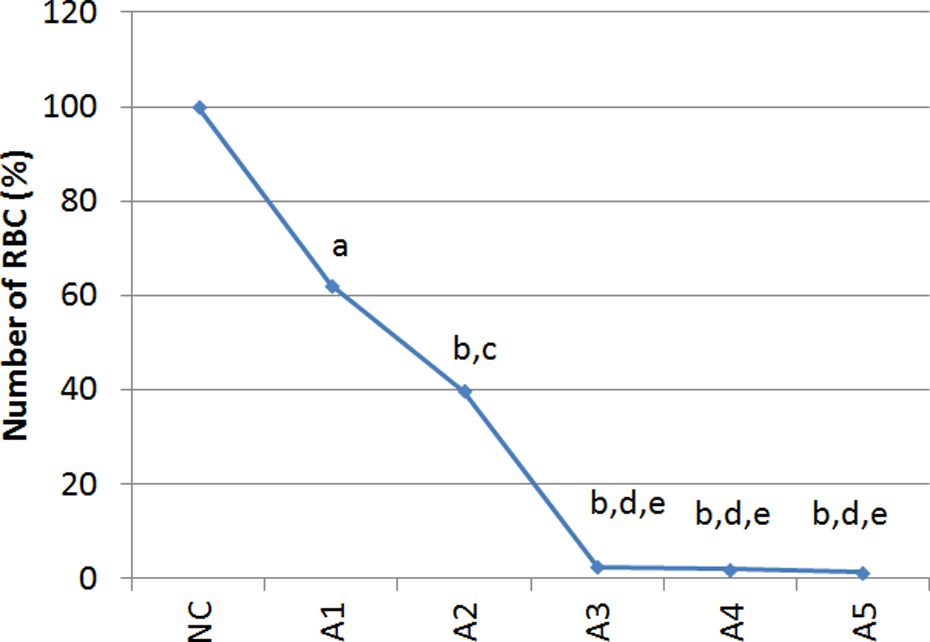
The effects of different concentrations of Ankaferd on human red blood cell numbers. NC: negative control; A1: 1% Ankaferd solution; A2: 5% Ankaferd solution; A3: 12.5% Ankaferd solution; A4: 5% Ankaferd solution; A5: 50% Ankaferd solution; a: p < 0.05 when compared with negative control; b: p < 0.001 when compared with negative control; c: p < 0.05 when compared with A1; d: p < 0.001 when compared with A1; e: p < 0.05 when compared with A2.
Discussion
Hemostatic failure, a serious problem encountered in dentistry, can cause excessive postoperative bleeding, delayed wound healing, and increased risk of infection. Currently used agents for hemostasis, like fibrinogen and plasma-derived blood coagulation factors, may carry the risk of transmission of viral infection and formation of clotting factor inhibitors. ABS may offer a convenient alternative during dental procedures. ABS might also be effective for the patients with hemophilia and/or other hemostatic defects during dental procedures as indicated in case reports later in this article. 34
The ideal hemostatic agents also should be free of cytotoxicity, but the ability of hemostasis is more important; however, after hemostasis is achieved, unused hemostatic material should be eliminated, leaving as little hemostatic agent as possible in order to avoid postoperative complications. 35
Odabas et al. studied that ABS was cytotoxic to human pulp fibroblasts by MTT (3-(4,5-dimethylthiazol-2-yl)-2, 5-diphenyltetrazolium bromide, a yellow tetrazole) assay. The influence of cytotoxicity to human pulp fibroblasts depended on the concentration of ABS. The more diluted concentrations exhibited less cytotoxic characteristics when compared with the more concentrated forms. 36
There is not any information about the components of ABS, which could induce cell proliferation and agglutination. According to Aydın et al., ABS may have some plant proteins known as lectins that bind to the cell surface and cause agglutination. Some of these plant proteins, discovered many years ago, are phytohemaglutinins because they bind to RBCs and agglutinate them. 37 Also lectins such as phytohemaglutinin, which is used as a mitogen, can induce cell proliferation. In addition, a lectin isolated from U. dioica is called U. dioica lectin, which has been found to stimulate the proliferation of human lymphocytes. 11 On the contrary, Odabas et al. 36 reported that ABS inhibited cell proliferation.
In this study, the cell membrane alteration and cell proliferation after ABS treatment on human lymphocyte were analyzed by LDH release assay and WST-1 assay. Released LDH can be a useful marker in the explanation of early cell membrane alteration.38–40 Jurisic et al. reported that the release of LDH is significantly correlated with the decreased cell proliferation induced with 10,000 pg/mL tumor necrosis factor-α (TNF-α). However, TNF-α, at lower concentrations (125 and 250 pg/mL), increased cell proliferation, nonetheless LDH released in Raji cells. 41
In our study, data indicated that an increase in spontaneous LDH release significantly correlated with increased cell proliferation induced with ABS. The maximal peak of LDH release and cell number were detected 24 h after ABS (25%) treatment. When human lymphocytes were treated with high concentrations of ABS, the agglutination increased (Figure 2). Due to the proliferation of cells, LDH released from the cells to a culture medium increased. Also ABS reduced the number of cells and hemolytic activity because of cell agglutination on human erythrocytes.
Conclusion
ABS is a herbal extract, and it has been used as a hemostatic agent in Anatolia for centuries. Although the exact mechanism of ABS still remains unknown, it is a well-known fact that plants such as ABS have certain impact on hemostatic system in various ways. For one thing, ABS might affect fibrinogen-like interactions between ABS and blood proteins as well as other proteins through the agglutination of these molecules, which are also driven by ABS itself. The presence of ABS is also effective in the aggregation of blood cells, particularly RBCs, and activated leukocytes at an increasing level. During the coagulation process, proteins and cells in blood agglutinate stop bleeding and therefore cell membrane of blood cells, particularly RBCs, get damaged by this agglutination. The results of our study revealed that cytotoxic and proliferative effects of ABS might shed light on this process outlined above.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.