
Abstract
Introduction
Carbon dioxide is naturally present in the atmosphere where its concentration is 0.027–0.038% (0.29 mmHg or 380 ppm). It is a colorless gas that is heavier than air and has a faintly pungent odor. Carbon dioxide is a normal constituent of the body arising from cellular respiration. Carbon dioxide is an important physiological gas, a metabolic product of body cell and also an asphyxiating gas. 1 Low-concentration carbon dioxide is of low toxicity, while the high-concentration carbon dioxide can cause acceleration of respiratory frequency, ventricular tachycardia, cardiac arrhythmia, conscious disturbance, coma and even death. 1
In recent years, general and occupational accidents of acute carbon dioxide poisoning have occurred and are usually associated with a high mortality rate. The corresponding therapeutic effect of oxygen therapy has already been universally recognized. However at the scene of an acute poisoning accident, it has not yet been determined which method of oxygen therapy is the most effective, the high-concentration atmospheric pressure oxygen inhalation therapy or the low concentration atmospheric pressure oxygen inhalation therapy. Probing into the question through animal experiment and research, this article will screen out the oxygen-therapy technology that is suitable for field usage.
Materials and methods
Animals and materials
There were 60 healthy male Sprague Dawley rats, whose mass is 220 ± 20 g (Laboratory Animal Centre, Academy of Military Medical Sciences); 99.9% carbon dioxide gas (Beijing Institute of Special Gas); 99.9% oxygen (Beijing Institute of Special Gas); pentobarbital sodium (Beijing Chemical Reagents Company, import from German, subpackage, batch number: 020919); poisonous tank for experimental animals (Laboratory of Centre for Disease Control and Prevention in Beijing); CPR-B portable single-gas concentration detector (Beijing Oriental Anno Biochemical Technology Co., Ltd.); portable medical hyperbaric oxygen chamber for baby (type WC11YLC0.5/1A, Nanyang Dongsen Medical Devices Co., Ltd.); GEM Premier 3000 blood-gas analyzer (American Testing Instrument Co., Ltd.) and Siemens Deling automatic biochemical analyzer (Germany Siemens Ltd.) were used in the study
Model making
Experimental animals were placed in poisonous tank of 1 m 3 in volume and allowed to inhale mixed gas of air and carbon dioxide of 20% concentration for 1 hour. The concentration of carbon dioxide in the poisonous tank was monitored using the portable single-gas concentration detector. The gas was pumped out of the tank three times for dilution, respectively, at the beginning, the middle and the end of poisoning. For the three times, the carbon dioxide concentration was determined to be 20%. If more than 80% of rats are in coma and the mortality is lower than 20%, the poisoning is considered successful.
Grouping and treatment
The rats were randomly divided into five groups: normal control group, carbon dioxide poisoning group, hyperbaric oxygen inhalation treatment group, high-concentration atmospheric pressure oxygen inhalation treatment group and low-concentration atmospheric pressure oxygen inhalation treatment group, and each group has 12 rats. No treatment was given to the rats of normal control group; the rats of poisoning group inhaled atmospheric air for 1 hour after being poisoned; the hyperbaric oxygen therapy was given to the rats of hyperbaric oxygen-therapy group after being poisoned (the portable medical hyperbaric oxygen chamber was adopted, the pressure was 2ATA (atmosphere absolute), the oxygen concentration was 100% and oxygen inhalation time was 1 hour); high-concentration oxygen inhalation therapy was given to the rats of high-concentration atmospheric pressure oxygen inhalation treatment group after being poisoned (the oxygen concentration was 50% and oxygen inhalation lasted for 1 hour); low-concentration oxygen inhalation therapy was given to the rats of low-concentration atmospheric pressure oxygen inhalation treatment group after being poisoned (oxygen concentration was 33% and oxygen inhalation lasted for 1 hour). Portable medical hyperbaric oxygen chamber is provided with pressure and oxygen-concentration monitoring systems. To monitor the oxygen-concentration of both high-concentration and low-concentration atmospheric pressure oxygen inhalations the portable single-gas concentration detector was used; gas pumped out of the tank three times at the beginning, the middle and the end of oxygen therapy was diluted, and then the oxygen concentration was measured so as to monitor the achievement of the target oxygen concentration
Determination of blood gas analysis
The animals of each group after grouping were narcotized through intraperitoneal injection of 50 mg/kg pentobarbital sodium. The abdominal aorta was extracted and 1 ml arterial blood of rats was drawn for blood gas analysis in order to inspect the levels of pH of arterial blood, partial pressure of oxygen (PO2) and partial pressure of carbon dioxide (PCO2).
Serum enzymology and electrolyte measurement
After the arterial blood of rats was taken, 3 ml intracardiac blood was centrifuged to determine serum troponin I (CTNI), creatine kinase (CK), glutamic-oxaloacetic transaminase (AST), γ-glutamyl transpeptidase (GGT), blood urea nitrogen (BUN), potassium (K), sodium (Na) and chlorine (Cl).
Pathological collections of lung tissue and brain tissue
The lung and brain tissues of rats were first extracted and 10% formaldehyde solution was applied for fixation; two pieces of lung tissues were taken, respectively, from the left upper lobe and right lower lobe in horizontal direction, one piece from vertical side of the brain midline and two pieces in the other lateral direction; then cut sections were embedded by paraffin to conduct regular haematoxylin and eosin (H&E) dyeing; finally united vision-G (UV-G) grading analysis software was applied for image acquisition and analysis.
Statistical Analysis
For statistical analysis, SPSS16.0 statistical package was used. Measurement data were expressed as mean ± standard deviation, and the method of one-factor analysis of variance was used to inspect the significance of difference among the means of various groups; if p < 0.05, there was statistically significant meaning.
Results
General manifestations of poisoned animals after treatment
During the poisoning process, rats successively had polypnea, weak and limp limbs, slow-movement and coma. The rats of various groups gradually became sober after different oxygen therapies, but there were symptoms of weakening of activity and decline in reaction capacity
The comparison of blood gas analysis of all treatment groups, normal control group and carbon dioxide poisoning group is presented in Table 1 .
The pH, PO2 and PCO2 levels of all groups rats (\bar x ± s)

PO2: partial pressure of oxygen, PCO2: partial pressure of carbon dioxide.
a p < 0.05 compared with normal control group.
b p < 0.05 compared with carbon dioxide poisoning group.
From Table 1, we can interpret that the pH and PO2 of the arterial blood of carbon dioxide poisoning group are lower than the normal control group, and the PCO2 is higher than that of normal control group (p < 0.05); pH and PO2 of the arterial blood of each oxygen-therapy group are higher than that of the carbon dioxide poisoning group, and the PCO2 is lower than that of the poisoning group (p < 0.05); pH, PO2 and PCO2 of the arterial blood of each oxygen-therapy group show no significant difference with that of normal control group (p > 0.05); pH, PO2 and PCO2 of the arterial blood show no significant difference (p > 0.05) among each oxygen-therapy group.
The comparison of serum enzymology of all treatment groups, normal control group and carbon dioxide poisoning group is presented in Tables 2 and 3.
The CTNI, CK and AST levels in rats of all groups (\bar x ± s)

CTNI: troponin I, CK: creatine kinase, AST: glutamic-oxaloacetic transaminase.
a p < 0.05 compared with normal control group.
b p > 0.05 compared with normal control group.
The GGT and BUN levels of all groups rats (\bar x ± s)

GGT: γ-glutamyl transpeptidase, BUN: blood urea nitrogen.
a p < 0.05 compared with normal control group.
b p > 0.05 compared with carbon dioxide poisoning group.
From Table 2, we can interpret that the CTNI, CK and AST levels of carbon dioxide poisoning group, low-concentration oxygen inhalation treatment group and high-concentration oxygen inhalation treatment group are higher than that of normal control group (p < 0.05); the CTNI, CK and AST levels show no significant difference (p > 0.05) when compared to the carbon dioxide poisoning group, low-concentration oxygen inhalation treatment group and high-concentration oxygen inhalation treatment group; the CTNI, CK, and AST levels of hyperbaric oxygen-therapy group are obviously lower than that of carbon dioxide poisoning group, low-concentration oxygen inhalation treatment group and high-concentration oxygen inhalation treatment group (p < 0.05).
From Table 3, we can interpret that the GGT and BUN levels of carbon dioxide poisoning group, low-concentration oxygen inhalation treatment group, high-concentration oxygen inhalation treatment group and hyperbaric oxygen treatment group are higher than that of normal control group (p < 0.05); the GGT and BUN levels show no significant difference (p > 0.05) among carbon dioxide poisoning group, low-concentration oxygen inhalation treatment group, high-concentration oxygen inhalation treatment group and hyperbaric oxygen-therapy group.
The comparison of electrolyte of all treatment groups, normal control group and carbon dioxide poisoning group is presented in Table 4
From Table 4, we can interpret that the level of serum K of carbon dioxide poisonous group, low-concentration oxygen inhalation treatment group and high-concentration oxygen inhalation treatment group is higher than that of normal control group (p < 0.05); the level of serum K of carbon dioxide poisonous group, low-concentration oxygen inhalation treatment group and high-concentration oxygen inhalation treatment group show no significant difference (p > 0.05); the level of serum K of hyperbaric oxygen-therapy group is obviously lower than that of carbon dioxide poisoning group, low-concentration oxygen inhalation treatment group and high-concentration oxygen inhalation treatment group (p < 0.05). The levels of serum Na and Cl of carbon dioxide poisoning group, low-concentration oxygen inhalation treatment group and high-concentration oxygen inhalation treatment group are lower than that of normal control group (p < 0.05); the levels of serum Na and Cl of carbon dioxide poisoning group, low-concentration oxygen inhalation treatment group and high-concentration oxygen inhalation treatment group show no significant difference (p > 0.05); the levels of serum Na and Cl of hyperbaric oxygen-therapy group are obviously higher than that of carbon dioxide poisoning group, low-concentration oxygen inhalation treatment group and high-concentration oxygen inhalation treatment group (p < 0.05).
The serum K, Na and Cl levels in rats of all groups (\bar x ± s)

a p < 0.05 compared with normal control group.
b p > 0.05 compared with normal control group.
Pathological manifestations
From the gross anatomy, it can be interpreted that the lungs of rats of normal control group have no abnormalities, while there is a large area of spotty and flaky blood stasis in lungs of the carbon dioxide poisonous group. The lung congestion situation of rats of high-concentration and low-concentration oxygen inhalation treatment groups are eased to some extent in comparison with the poisonous group, and the lungs of rats of hyperbaric oxygen-therapy group show no obvious abnormity. Under the light microscope, it can be interpreted that there is no hemorrhage and exudation in the lungs of rats from normal control group (see Figure 1); there is diffuse hemorrhage and exudation in lung tissues of rats from carbon dioxide poisonous group (see Figure 2); the hemorrhage and exudation situation in the lung tissue of rats from high-concentration and low-concentration oxygen inhalation treatment groups is eased to some extent in comparison to that of the poisonous group (see Figures 3 and 4); there is only slight hemorrhage and exudation in the lung tissue of rats from hyperbaric oxygen-therapy group (see Figure 5). The gross anatomy and microscopic findings of animal brain tissues of all groups have no distinction, and there is no significant bleeding, edema, cell degeneration and necrosis (see Figure 6).
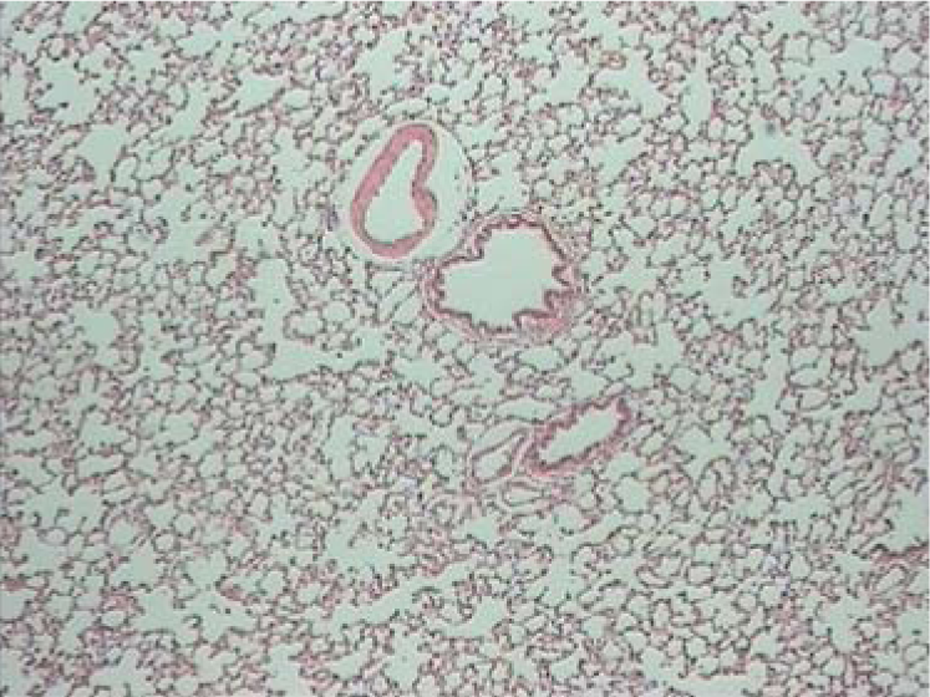
Lung pathology in rats of control group (HE × 40).

Lung pathology in rats of poisoning group (HE × 100).

Lung pathology in rats of high-concentration oxygen treatment group (HE × 100).

Lung pathology in rats of low-concentration oxygen treatment group (HE × 100).

Lung pathology in rats of hyperbaric oxygen treatment group (HE × 100).

Pathology in rats of brain tissues (HE × 100).
Discussion
Since the 20th century, there have been reports about accidents and casualties of carbon dioxide poisoning both at home and abroad. There have also been reports of high mortality rates in association with acute carbon dioxide poisoning. The United States Environment Protection Agency has investigated the deaths that occurred from 1975 to 2000 as a result of the leakage in the carbon dioxide extinguisher systems. There were a total of 51 cases, of which 72 people died and 145 people were injured. 2 Carbon dioxide is a suffocating gas but toxic action is found at the cellular level. It has been reported in the literature that inhalation of carbon dioxide gas with a concentration of more than 5% for 1 hour can cause the secretion of proinflammatory cytokine in rats. This research result indicates that the toxicity of carbon dioxide is higher than previously thought. 3 When the concentration of carbon dioxide is higher than 20%, there is a higher rate of mortality. 4 In this experiment, the rats that inhaled a mixed gas of air and 20% carbon dioxide for 1 hour went into coma, which indicates that rats have a better tolerance of higher concentrations of carbon dioxide in comparison with other living organisms.
The acute carbon dioxide poisoning can cause multisystem damage. Oxygen therapy refers to the therapeutic measures that administer oxygen, whose oxygen content is higher than atmospheric levels to treat or prevent the symptoms and manifestations caused by low oxygen. 5 The effect of oxygen therapy has been universally recognized, but currently there is still no relevant report at home or abroad regarding the best oxygen-therapy for on-site treatment of carbon dioxide poisoning. Nevertheless the timely on-site treatment is the key for patient prognosis. Through establishing rat models of acute carbon dioxide poisoning and giving them three different oxygen therapies, that is, hyperbaric oxygen therapy, high-concentration and low-concentration atmospheric pressure oxygen inhalation therapies, and by means of the observation on results of blood gas analysis, serum enzymology, etc and the characteristics of electrolyte and pathological changes, this article explores the best on-site technical solution of oxygen therapy.
The basis for causing physiological and pathological changes upon acute carbon dioxide poisoning is oxygen-poor (hypoxemia) and acute carbon dioxide retention (hypercapnia). Through the blood gas analysis of this research, we can see that rats after acute carbon dioxide poisoning become hypoxemic and hypercapnic which obviously improves after giving different oxygen therapies. However, the statistical analysis of results of the three oxygen therapies has no difference.
In human beings, when the concentration of inhaled carbon dioxide is less than 6%, the electrocardiogram will show small changes. With the increase in concentration, there will be a rise in sinus node frequency, premature systole of atrium and ventricle, ST-section change and non-Q wave myocardial infarction,6,7 and the sero-myocardial enzymes will also show corresponding changes. There have been few reports about the increase in levels of serum CK and AST in patients with carbon dioxide poisoning. 8 In this study, the levels of serum CTNI, CK and AST increased significantly in patients with acute carbon dioxide poisoning, and the level reduced to some extent after the hyperbaric oxygen therapy. Upon acute carbon dioxide poisoning, the state of severe depletion of oxygen and energy metabolic disorders will cause cell dysfunction and pathological lesion, especially in the tissues and organs such as the heart, brain, liver, etc where the metabolism is most active. The mechanism of hyperbaric oxygen therapy to treat patients with acute carbon dioxide poisoning lies in inhaling pure oxygen under the pressure of 2ATA which will enable the arterial PO2 to reach 14 times that of air inhalation under atmospheric pressure, so that it can significantly improve the dissolved oxygen level in plasma and the diffusivity in tissue as well as the permeability of cell membrane, enabling sufficient aerobic metabolism in histiocytes and reducing tissue damage. 9
Cell homeostasis depends on Na+/K+ pump, adenosine triphosphate enzyme, etc. However, the damaged buffer system of cells caused by the increase of carbon dioxide concentration leads to the rise in blood K concentration and acidosis. 1 The K concentration in the rats of carbon dioxide poisoning group in this study increased significantly. At present,there is no relevant report about the changes in serum electrolytes on the acute carbon dioxide poisoning rats applied with various oxygen therapies. In this research, through observing the situation of rats poisoned by carbon dioxide and the variations of serum K, serum Na, serum Cl after being given three different oxygen therapies, we can interpret that hyperbaric oxygen treatment has certain effects on correcting the electrolyte disorder. The possible mechanism of correcting the electrolyte disorder by hyperbaric oxygen therapy lies in that the hyperbaric oxygen can effectively improve tissue hypoxia and acidosis, increase tissue oxygen content and oxygen reserve, reduce tissue damage and cell injury and reduce the permeability of blood capillary and cell membrane.
The pathological changes of carbon dioxide poisoning include obvious hyperaemia of tracheal submucosal blood vessels, the neutrophil infiltration between the epithelium of submucosa and mucosa, pulmonary congestion and edema. From the autopsy of patients who died of carbon dioxide poisoning, we can find sporadic hemorrhage in alveolar spaces of interstitial lung and extensive emphysema. 8 The research results of Wang Jianxin et al. show that high-concentration carbon dioxide gas can cause extensive incrassation of alveolar wall of rats. The edema fluid and the small focal pulmonary parenchyma hemorrhage are visible in alveolar space. 10 In this study, from (using a light microscopy) lungs of rats with acute carbon dioxide poisoning, we can interpret that there exists extensive hemorrhage and exudation. After the high-concentration and low-concentration atmospheric pressure oxygen inhalation treatment, there was an improvement in hemorrhage and exudation, and also lung hemorrhage and exudation improved obviously after hyperbaric oxygen therapy. From the perspective of pathological changes in lungs, the therapeutic effect of hyperbaric oxygen is superior to that of high-concentration and low-concentration atmospheric pressure oxygen inhalation therapies. Hyperbaric oxygen therapy can improve the ventilation function of respiratory tract and the alveolar ventilation function, reduce the capillary permeability and improve pulmonary hemorrhage and edema. Zhang Haidong et al. have reported 16 cases of patients with acute carbon dioxide poisoning treated with hyperbaric oxygen therapy, among whom the patients with mild intoxication have been healed after oxygen inhalation for three to six times and the unconscious patients became sober after one to four times of oxygen inhalation. 11 Inhalation of carbon dioxide gas can change the functions of central nervous system, and the inhalation of 2.5–3.5% carbon dioxide for 10 minutes can make the cerebral blood flow increase by 100%. When the concentration of carbon dioxide is more than 5%, the ability to finish the complex activities is reduced. 12 Being exposed to 10–15% carbon dioxide for a short time can cause excitation, blinking, myoclonia, and dysphoria. 13 Being exposed to 10–15% carbon dioxide for a long time can cause vertigo and drowsiness.13,14 In this experiment, after the inhalation of mixed gas of air and 20% carbon dioxide for 1 hour, the rats went into coma. The pathological examination of brain showed no significant bleeding, edema, cell degeneration and necrosis. The short-term pathological changes of acute carbon dioxide poisoning mainly focus on lungs. Although the rats with carbon dioxide poisoning have nervous system symptoms, there is no significant abnormality in pathological examination of brain tissue.
In conclusion, through establishing rat models of acute carbon dioxide poisoning and giving them three different oxygen therapies, that is, hyperbaric oxygen therapy, high-concentration and low-concentration atmospheric pressure oxygen inhalation therapies, this article explores the best on-site oxygen-therapy technology. Compared with other oxygen-therapy methods, the hyperbaric oxygen therapy has certain superiority in improving the rise of serum enzymology and correcting electrolyte disorder. The pathological change in the lungs of hyperbaric oxygen-therapy group is significantly better than that of high-concentration and low-concentration atmospheric pressure oxygen inhalation treatment groups. Therefore, it is suggested that the oxygen therapy should be used for on-site treatment as soon as possible. The hyperbaric oxygen therapy shall be given to the patients as early as possible for improving the poisoning damage and prognosis once the conditions are met.
Footnotes
Acknowledgement
This study was sponsored by Social Welfare Project of Ministry of Science and Technology of China.
The authors declare that there are no conflicts of interest.
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.