
Abstract
The adjuvant for Gramoxone INTEON is composed of 20% methanol, 20% sodium lingo sulphonate, 10% alkylaryl polyoxyethylene ether, and 50% water. Although the adjuvant is a potential source of intoxication due to the widespread use of Gramoxone INTEON, there has been no prior report characterizing the acute toxicity of this adjuvant. This study evaluated the acute toxicity of adjuvant ingestion. Seven patients presenting with acute adjuvant intoxication at Chonnam National University Hospital were enrolled in this retrospective study. The patients had intentionally or accidentally ingested 20–150 mL of adjuvant. Gastrointestinal symptoms such as nausea and vomiting were most common, and no ocular symptoms were reported. Cardiovascular symptoms were limited to electrocardiogram changes such as corrected QT interval (QTc) prolongation (71.4%) and sinus tachycardia (28.6%). All patients had an elevated serum osmolar gap and lactate levels. One patient had metabolic acidosis with a high anion gap that required administration of sodium bicarbonate. These clinical symptoms were resolved within 3 days with supportive treatment without any sequelae. There were no life-threatening symptoms and no deaths. However, the physician should keep in mind the possibility of methanol intoxication in patients poisoned with this adjuvant.
Keywords
Introduction
Gramoxone INTEON is a recent formulation of herbicide paraquat (PQ) that incorporates compounds including alginate and magnesium sulphate to decrease PQ-associated toxicity. The change of alginate to a gelatinous mixture that occurs under gastric pH conditions and the purgative effects of magnesium sulphate reduce the absorption of PQ. 1
The manual on INTEON instructs the users to include a nonionic surfactant at a minimum (v/v) concentration of 0.125–0.25% to the finished spray volume for ground and aerial application, according to the concentration of the contained surfactant. 2 The surfactant reduces the surface tension of water, which increases the wettability of the hydrophobic surface of plants and, thus, penetration of foliar- applied herbicides.3,4
Some INTEON products available in Sri Lanka contain PQ and surfactants premixed in one bottle, similar to the older forms of the PQ herbicide. 5 In South Korea, the adjuvant, including the surfactants for INTEON, is bottled and sold separately from PQ. Farmers need to purchase the INTEON package including PQ separately as one bottle and the adjuvant in another bottle. The adjuvant is a combination of 50% water, 20% methanol, 20% sodium lingo sulphonate, and 10% alkylaryl polyoxyethylene ether. It is well known that methanol ingestion can cause a medical emergency characterized by metabolic acidosis with a high anion gap, visual disturbances, cardiorespiratory failure, and death in humans according to the amount ingested. 6 Surfactants are classified according to their hydrophilic polar group as anionic, cationic, amphoteric, and nonionic. 7 Alkylaryl polyoxyethylene ether is a nonionic surfactant, and sodium lingosulphonate is anionic. 8 Nonionic and amphoteric surfactants have the lowest toxicity, anionic surfactants have intermediate toxicity, and cationic surfactants have the highest toxicity. 8 However, acute renal failure has been described following the ingestion of detergent containing nonionic and anionic surfactant.9,10 The risk posed by these surfactants has prompted concern, because they are used in the INTEON adjuvant and because of the growing agricultural replacement of PQ with INTEON.
No report has yet characterized the acute toxicity of this adjuvant. This retrospective study was carried out to evaluate the toxicity of INTEON adjuvant intoxication.
Methods
This study used a retrospective design at Chonnam National University Hospital, an academic tertiary care centre, with an annual emergency department (ED) census of 30,000 patients. This centre is responsible for the health of residents of Gwangju city and the nearby Jeolla province, with a population of 3 million; 27% of the residents work in agriculture.
This study was approved by the Chonnam National University Hospital’s institutional review board.
The hospital medical record system was used to obtain the medical information of the enrolled patients. The patient selection criteria were as follows: patients over the age of 18 years that presented to the ED between June 2007 and April 2010 after the ingestion of INTEON adjuvant alone, and patients who had negative results on a urine sodium dithionite reaction test and serum PQ concentration. A total of 13 patients were identified.
However, four patients that ingested the adjuvant with another drug were excluded. In addition, a 35-year-old male who was incidentally exposed to the adjuvant and whose outcome was lost due to his discharge against medical advice 10 hours after admission was excluded. Arterial blood gas analysis upon admission was within the normal range and the patient did not develop significant symptoms during the hospitalization. Additionally, a 67-year-old female who reported intentional ingestion of 150 mL of the adjuvant was excluded because her symptoms were consistent with intoxication of a cholinesterase inhibitor. In total, seven patients were enrolled in the study.
The medical records were reviewed and the data including patient characteristics, information related to the ingestion, treatment, and outcome were collected. The estimated amount of ingestion was defined as follows: a spoon as 5 mL, a mouthful as 25 mL, and a cup as 100 mL.
11
The corrected QT interval (QTc) on the electrocardiogram (ECG) was calculated using Bazett’s formula (QTc = QT/√RR).
12
A prolongation of the QTc interval was defined as a QTc interval greater than 440 ms.
12
Tachycardia was defined as a heart rate greater than 100 beats per minute.
13
Metabolic acidosis was defined as a pH <7.35 and
The medical outcomes were assessed according to the standard American Association of Poison Control Centers Toxic Exposure Surveillance System (AAPCC TESS) definitions: no, mild, moderate, major effects, or death. 17 Minor effects included signs or symptoms that were minimally bothersome and resolved rapidly (e.g. self-limited gastrointestinal symptoms, drowsiness [Glasgow coma scale >13], skin irritation, first-degree dermal burn, sinus tachycardia without hypotension [systolic blood pressure <90 mmHg], and a transient cough). Moderate effects included signs or symptoms that were more pronounced, more prolonged, or more systemic in nature than minor symptoms, usually requiring treatment but not life threatening (e.g. corneal abrasion, acid—base disturbance, high fever, disorientation, hypotension that was rapidly responsive to treatment, and isolated brief seizures that responded readily to treatment). The major effects were defined as signs or symptoms that were life threatening or resulted in significant residual disability (e.g. repeated seizures or status epilepticus, respiratory compromise requiring intubation, ventricular tachycardia with hypotension, cardiac or respiratory arrest, esophageal stricture, and disseminated intravascular coagulation). 17
Baseline data and outcomes were summarized by frequency tabulation for categorical variables or the median and range for continuous variables. The Statistical Package for the Social Sciences version 15.0 was used.
Results
Patient characteristics
The median age of all the seven patients enrolled was 39 (range: 34–58 years), and there were 6 males (85.7%; Table 1). In all, 6 patients (85.7%) intentionally ingested the adjuvant, and 4 (66.7%) of these 6 patients co-ingested adjuvant with ethanol. Patient 6 reported that she accidentally ingested this product mistaking it for alcohol. The median volume ingested was 100 mL (range: 20–150 mL). The time interval from ingestion to hospital arrival varied from 30 minutes to 4 hours.
Clinical pictures of seven patients who were poisoned with Gramoxone INTEON adjuvant

QTc: corrected QT interval, ECG: electrocardiogram.
a Previous medical history: history of hypertension, ischemic heart disease, renal failure, or diabetes mellitus.
b Metabolic acidosis was defined as a pH < 7.30 and
Symptoms and signs
The most common ECG abnormality on admission was QTc prolongation (>440 ms; 71.4%), with a normal range of potassium, magnesium, and calcium upon admission, followed by sinus tachycardia (28.6%; Table 1). After admission, the tachycardia continued for 1 hour in one patient and 6 hours in another patient. These abnormal ECG findings did not require any specific treatment and were resolved by discharge.
All the patients with adjuvant poisoning had an increased serum osmolal gap (43–90 mOsm/kg) and serum lactate levels (normal range: 0.7–2.0 mmol/L; Table 1). They did not have hypertriglycemia or hyperproteinemia as a cause of the osmolal gap. Both the osmolal gap and lactate levels gradually decreased and normalized in all the patients by discharge. Metabolic acidosis with a high anion gap (16.3 mmol/L) was observed in one patient (14.2%) upon admission which resolved 10 hours after admission with the administration of 60 mEq/L of sodium bicarbonate. There were no abnormalities on the renal and liver function tests during hospitalization.
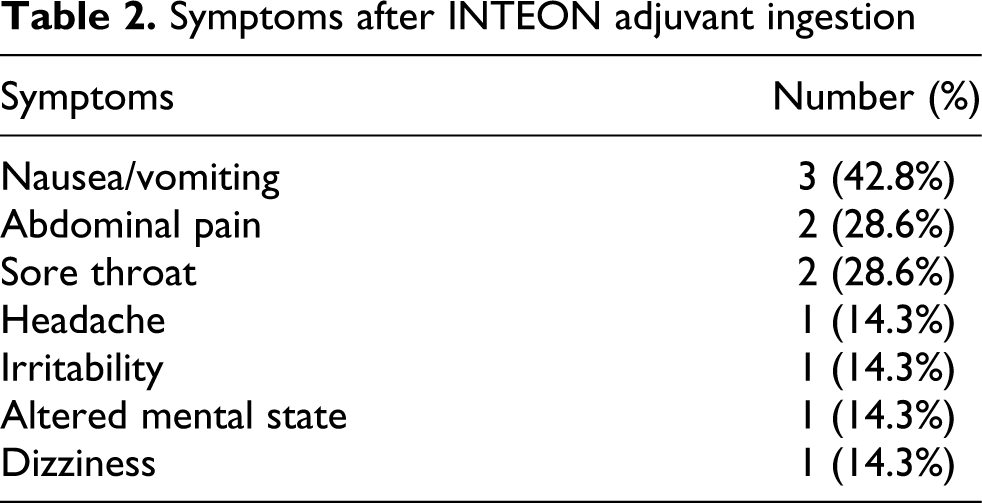
The most common symptoms on admission were nausea (42.8%) and vomiting (42.8%) followed by abdominal pain (28.6%; Table 2). The reported symptoms were resolved within 6 hours (range: 2–19 hours) after admission. One patient, a 58-year-old male who ingested 50 mL of adjuvant, had an altered mental status (Glasgow coma scale 14) and irritability upon admission. Brain computed tomography revealed no abnormal findings. The patient’s mental status returned to normal 19 hours after admission with no specific intervention. None of the patients complained of visual symptoms such as blurred vision, decreased visual acuity, or photophobia. In addition, none of the patients had dilated pupils unreactive to light.
Symptoms after INTEON adjuvant ingestion
Treatment and outcome
Gastric lavage was performed in all patients after ingestion and five patients received activated charcoal. Six patients were treated with only symptomatic care during hospitalization, and one patient needed administration of sodium bicarbonate. The median duration of hospitalization was 3 days (range: 2–3 days; Table 1). The medical outcomes were coded as the following: two cases with no effect, four cases with a mild effect, and one case with moderate effect. There were no patients with major effects and there were no deaths.
Discussion
While the number of cases is very small, this study is the first to report and analyse the toxicity of INTEON adjuvant.
Methanol ingestion commonly presents with gastrointestinal symptoms such as nausea and vomiting and can lead to central nervous system depression, visual impairment, and metabolic acidosis with a high anion gap. 18 The acute toxicity of surfactants contained in this adjuvant have not yet been reported in humans. Nonionic and anionic surfactants cause irritation to the gastrointestinal mucosa.19,20 In the present study, gastrointestinal symptoms such as vomiting were the most common symptoms after adjuvant ingestion. Methanol or surfactants might have contributed to the gastrointestinal symptoms.
Elevated serum lactate levels and osmolal gap were observed in all patients, and one patient co-ingesting ethanol and 50 mL of adjuvant had metabolic acidosis with a high anion gap at presentation. A high anion gap metabolic acidosis, elevation of lactate levels and osmolal gap are induced by methanol intoxication. 21 In particular, the elevation of serum lactate and osmolal gap (>70 mOsm/kg) in two patients without co-ingestion of ethanol suggested that adjuvant ingestion could have a potential of methanol intoxication. However, while the patients ingested amounts that could cause symptoms of methanol intoxication, and the elevated osmolal gap gradually decreased after admission, metabolic acidosis with a high anion gap did not develop during hospitalization in six patients without specific treatment targeting methanol intoxication such as hemodialysis, and continuous administration of fomepizole. In addition, the patient who co-ingested ethanol and 100 mL of adjuvant and presented later after ingestion than the patient with metabolic acidosis did not show acid–base disturbance. The absence of progression to metabolic acidosis and the discrepancy between toxic severity and the amount ingested could partially be explained by the unrevealed effects of the surfactants, and the effect of ethanol ingested aside from the difference between the ingested volume and absorbed volume due to vomiting.
Although we cannot completely exclude delayed complications of this adjuvant, because of the short hospitalization, the adjuvant did not cause abnormalities in renal and liver functions among the seven patients during hospitalization. Prabhakar et al. reported that 100 mL of detergent including surfactants caused leukocytosis and elevated creatinine and urea levels on admission. 10 The patient in their study progressed to metabolic acidosis with a high anion gap, hypocalcemia, hyperkalemia, and rhabdomyolysis. They reported that the detergent contained non-soap surfactants (nonionic or anionic); however, they did not indicate which specific surfactant detergents were involved. In another report, 100 mL of detergent including nonionic and anionic surfactants increased the serum creatinine and urea levels within 24 hours after ingestion. 9
In this study, gastric lavage was performed in all patients and five patients received activated charcoal. These treatments could affect the development of gastrointestinal symptoms that were main symptoms of patients after ingesting this adjuvant. Furthermore, when considering the time interval from ingestion to arrival at hospital and amount ingested retrospectively, the gastric lavage might have been useless or harmful in some patients. The corrosive effects in the gastrointestinal tract such as extensive necrosis, erosion, and edema were observed at autopsy of a patient who ingested detergent containing anionic surfactant and methanol. 22 In addition, because methanol is absorbed rapidly from the gastrointestinal tract, gastric lavage is indicated within 1 hour after methanol ingestion. 21 Furthermore, aspirating this adjuvant due to gastric lavage will cause acute lung injury and contribute to methanol toxicity, since aspirated methanol has a toxicity equivalent to that resulting from ingestion. 23 Therefore, we suggest that due to the potential for injury from gastric lavage, physicians should only consider gastric lavage when a patient arrives within 1 hour of ingestion of a potentially lethal dose of the adjuvant and when the patient is fully conscious or intubated. In addition, activated carbon has been shown to be effective for binding anion and nonionic surfactants during wastewater treatment.24,25 However, there is no research supporting the efficacy of activated charcoal in humans for the treatment of surfactant poisoning. In addition, activated charcoal may be of limited value because of limited binding with regard to methanol intoxication. 26 The present study had several limitations. First, it was not possible to completely exclude the possibility that ethanol intoxication may have contributed to the clinical and laboratory results in five patients who co-ingested ethanol with INTEON adjuvant, because the serum levels of methanol and ethanol were not evaluated. Due to the good prognosis of the patients with supportive treatment, we did not investigate the composition of the adjuvant until 2010, when the last patient with metabolic acidosis presented to our ED. The methanol concentration of patients with adjuvant intoxication is currently evaluated, even though it is time consuming and may not be helpful for making decisions about acute treatment. One patient who ingested ethanol and 20 mL of the adjuvant (20% methanol) showed milder elevation of serum lactate levels (4.8 mmol/L) and osmolal gap (43.0 mOsm/kg). The amount of 40% methanol that produces toxicity ranges from 15 to 500 mL. 27 When considering the small amount of methanol in this patient, the ethanol could affect the laboratory findings. However, two patients who did not ingest ethanol along with the adjuvant showed laboratory abnormalities consistent with methanol intoxication. In addition, a significant elevation of serum lactate (>5 mmol/L) in one patient who co-ingested ethanol was unlikely caused by ethanol alone. 28 These observations suggest that methanol intoxication could be caused by ingestion of this adjuvant, although it is unclear how much methanol contributes to the development of symptoms due to the absence of serum methanol level. Further research including measurement of blood methanol levels is needed to determine the component that actually causes the clinical symptoms. Second, we could not determine the minimum toxic amount of the adjuvant because of the small number of patients and the inaccuracy in self-reporting the quantity of adjuvant ingested. Further studies with larger numbers of patients are needed. Third, all seven patients had a history of exposure to the adjuvant, but the diagnosis was not confirmed by laboratory testing. Instead, only the patients that brought the bottle to the hospital from which they drank with the word ‘adjuvant’ on the package label were included in this study. Finally, this was a retrospective study. As a result, the elapsed time from ingestion to arrival to the ED and the symptoms reported may have been under- or overestimated. However, the critical symptoms were likely correctly recorded.
Conclusion
Ingestion of the adjuvant for INTEON was associated with no or mild effects, except for one case with moderate effects. However, physicians should be alert to the possibility of methanol intoxication in patients poisoned with this adjuvant. Further research with measurements of the blood level composition is needed to determine the relative contribution of methanol and surfactants to the adjuvant toxicity.
Footnotes
The authors declared no conflicts of interest.
The authors declared that this research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.