
Abstract
Styrene is a volatile organic compound used in factories for synthesis of plastic products. The pneumotoxicity of styrene in experimental animals is known. The aim of the present study was to study the effect of styrene on lung function and oxidative stress in occupationally exposed workers in plastic factory. Thirty-four male workers, between 18 and 40 years of age, exposed to styrene for atleast 8 hours a day for more than a year were studied, while 30 age- and sex-matched healthy subjects not exposed to styrene served as controls. Assessment of lung functions showed a statistically significant reduction (p < 0.05) in most of the lung volumes, capacities (FVC, FEV1, VC, ERV, IRV, and IC) and flow rates (PEFR, MEF75%, and MVV) in the study group (workers) as compared to controls. Malondialdehyde (MDA) was observed to be significantly high (p < 0.05) while ferric-reducing ability of plasma (FRAP) was significantly low (p < 0.05) in styrene-exposed subjects. Reduced glutathione (GSH) level was significantly depleted in exposed subjects as compared to control group. The mean value of serum cytochrome c in styrene-exposed subjects was found to be 1.1 ng/ml (0.89–1.89) while in control its levels were under detection limit (0.05 ng/ml). It shows that styrene inhalation by workers leads to increased level of oxidative stress, which is supposed to be the cause of lung damage.
Introduction
Plastic has become an integral part of modern society. There is tremendous growth in the use of plastic disposables such as packaging material, household goods, agriculture, electronic goods, etc. Plastic product consists of various types of component depending upon the use like teflon, polyvinylchloride, polypropylene, polyethylene, polystyrene, etc. 1 Out of these, styrene is one of the chief packaging materials being used extensively. The most common route of absorption of styrene is via inhalation of vapours, oral, and dermal.1,2 Exposure of the general population occurs at levels of micrograms per day mainly due to inhalation of ambient air and cigarette smoke and intake of food that has been in contact with styrene-containing polymers. 3 In a study, it has been reported that 2-hour exposure of styrene vapour at a level of 50 ppm showed blood levels of 6.7 nM (average) in healthy volunteers. 4 Styrene exposure seems to be associated with hypersensitivity pneumonitis, occupational asthma, diffuse cell damage involving the tracheal, bronchiolar, and alveolar epithelium. 5
Recent studies have demonstrated that important changes may occur in oxidative status and immune system in host after xenobiotics ingestion.6–9 Oxygen free radicals (OFRs) are involved in the toxicity of numerous chemicals and also pathogenesis of many diseases. These free radicals are scavenged by the reducing agents present in the body. In humans, styrene is metabolized in the liver primarily to styrene 7,8-oxide, by cytochrome P450 and possibly by other isozymes (CYP2E1 and CYP2F), which is considered to be the principal reactive and genotoxic intermediate of styrene. It was found that at low styrene concentration CYP2E1 was the main isoform, while CYP2B6 was more active at high concentration. In the lungs, CYPF1 was the most active isoform in human lung microsomes. 10
Styrene oxide conjugates with reduced glutathione (GSH), resulting in GSH depletion in liver and lung, which increases susceptibility to oxidative stress.11,12 Cytochrome c, marker of apoptosis, has been found to be associated with decreased levels of GSH. 13
This compound has a great toxicological relevance due to its genotoxicity and suspected carcinogenicity (IARC Group 2B) and the fact that styrene exposure levels continue to be high in the reinforced plastics industry. 3 Styrene oxide induces growth inhibition and massive apoptosis, as revealed by DNA fragmentation, hypodiploidism, loss of cytoskeletal organization (F-actin depolymerisation) in neuronal PC12 cells line. 14 On the other hand, styrene is known to cause overexpression of Bcl-2 and Raf-1 in human cord blood cells, which are anti-apoptotic factors, while level of Bax expression decreases after its exposure, which is apoptotic; this shows that styrene do not cause apoptosis. 3
In the modern era, where plastic is used so commonly, there is need to determine the occupational hazard associated with its synthesis. Hence, the present study is planned to investigate the lung function, oxidative stress along with cytochrome c status in occupational workers of the plastic factory exposed to styrene for at least 8 hours a day for more than a year.
Materials and methods
Sixty male workers from plastic factory occupationally exposed to styrene between the age group 18 and 40 years and working for at least 8 hours a day for more than a year but less than 10 years were shortlisted. Out of these, three declined to take part in the study and 17 refused to give blood samples. Pulmonary function test were done on the remaining 40 subjects out of these, 6 were unable to perform manoeuvre correctly so excluded from the study. Therefore, finally our study group comprised of 34 subjects. Thirty age- and sex-matched subjects not exposed to styrene served as controls. Subjects having history of respiratory illness before joining the present job were excluded from the study. Subjects and controls on medication or having upper respiratory tract infection in preceding 3 weeks were also excluded from study. Informed written consent was taken from subjects before starting the study. They were called in batches of 2–3 on two days in a week for investigation. Study was approved by Institutional Ethics Committee-Human Research (IEC-HR), UCMS, Delhi, in a meeting held on 14 March, 2009. All the subjects participating in study signed informed consent form. Detailed history along with general physical examination and systemic examination for each system was carried out. But due to ethical issue, the factory owner did not give us permission to measure the levels of styrene in blood, urine or ambient air.
Pulmonary functions test (spirometry)
The pulmonary function tests were carried out on subjects using SIBELMED DATOSPIR 120B precision portable spirometer with built-in computer program using standard laboratory methods. The program provides a set of predicted normal volumes for all the lung function variables assessed based on age, height, weight, gender and ethnicity of the subject. The software analyzes and provides a detailed interpretation of flow volume loop. The machine was calibrated daily.
The subject was tested on relatively empty stomach, i.e. about 2–3 hours after a light meal. In order to alley anxiety and apprehension associated with testing, they were familiarized with the procedure and apparatus to be used. The ambient temperature on different days varied from 18°C to 26°C. Lung function tests were done on all the subjects. To measure the pulmonary functions accurately, it is important that subject should perform the test with maximum possible effort. The end point of the test was assessed by the shape and the size of the flow volume loop. Before selecting the best, reproducibility and validity criterion were used. Subjects doing 3 consecutive inadequate respiratory efforts were excluded from the study.
Blood sample collection
Blood (5 ml) was collected in ethylenediaminetetraacetic acid (EDTA)-containing and plain vial for the estimation of GSH, MDA, FRAP and cytochrome c. Serum was then separated from the clotted blood in plain vial by centrifuging the sample at 3000 rpm for 10 min. All the tests were performed within 12 hours of sample collection.
Measurement of lipid peroxidation
The lipid peroxide levels in serum were measured using a thiobarbituric acid reactive substances (TBARS) assay, which monitors MDA production based on the method of Satoh. 15 The MDA-TBA adduct formation was measured spectrophotometrically at 532 nm. The concentration of MDA was expressed as nmol/ml.
Measurement of ferric-reducing ability of plasma
Ferric-reducing ability of plasma (FRAP) was determined by measuring the ability of plasma to reduce Fe3+ to Fe2+ by the method of Benzie and Strain. 16 The complex between Fe2+ and 2,4,6-tri (2-pyridyl)-1, 3,5-triazine (TPTZ) gives a blue color with absorbance at 593 nm. Concentration of FRAP was expressed in µmol/l.
Measurement of glutathione
Total reduced glutathione (GSH) content in blood was measured by the method of Tietze 17 using 5,5′ dithiobis-2 nitrobenzoic acid (DTNB). In this method, GSH was oxidized by DTNB and then reduced by GSH reductase, with NADPH as hydrogen donor. The oxidation of GSH by DTNB was detected photometrically by a change of absorption at 412 nm. The concentration of blood GSH was expressed as µmol/dl.
Estimation of cytochrome c
Cytochrome C was estimated by using Bender Medsystems kit, Austria (Human Cytochrome C BMS 263) as per manufacture’s protocol. Briefly, in the appropriate wells of microtiter plates, serum samples, standard and controls along with biotin-conjugate antihuman cytochrome c monoclonal antibody were added (except blank) and incubated for 2 hours at room temperature. The solutions were then aspirated, and wells were washed four times. Streptavidin-HRP was added to each well except blanks and incubated for 1 hour at room temperature. A 100 µL of stabilized substrate solution was added into the wells and incubated approximately for 10 min. at room temperature. After adding stop solution to each well, the absorbance at 450 nm was recorded using a microplate reader (Biorad-680, USA). The readings were plotted on standard curve thus obtained and expressed in ng/ml. 18
Statistical analysis
Analysis was done by SPSS 17.0 statistic package. Unpaired ‘t’ test was performed to compare lung functions and oxidative stress between styrene exposed subjects and controls. Univariate analysis of variance was applied by taking smoking as a confounding factor.
Results
The anthropometric measurements in two groups (styrene exposed subjects vs. controls) are shown in Table 1. No significant difference was observed between the two groups for age, height, and weight (Table 1).
Anthropometric measurements of controls and subjects occupationally exposed to styrene

On comparing the two groups (styrene exposed subjects and controls) for all lung volumes and capacities, the values of FVC, FEV1, VC, ERV, IRV, and IC were observed to be significantly low (p < 0.05) in subjects as compared to controls (Table 2). Flow rates when compared showed a significantly decreased PEFR, MEF75%, and MVV in the study groups as compared to controls (Table 3).
Lung volumes and capacities of controls and subjects occupationally exposed to styrene
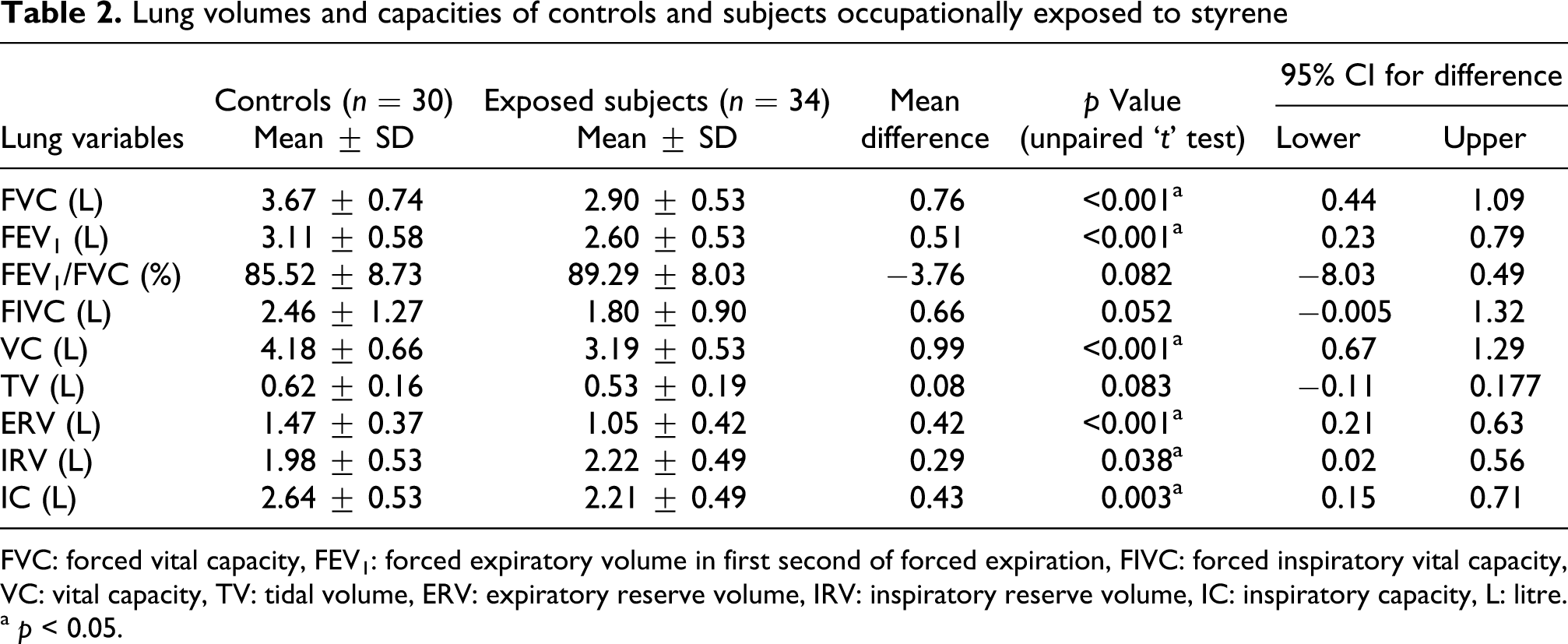
FVC: forced vital capacity, FEV1: forced expiratory volume in first second of forced expiration, FIVC: forced inspiratory vital capacity, VC: vital capacity, TV: tidal volume, ERV: expiratory reserve volume, IRV: inspiratory reserve volume, IC: inspiratory capacity, L: litre.
a p < 0.05.
Flow rate of controls and subjects occupationally exposed to styrene

PEFR: peak expiratory flow rate, MEF25%: maximal expiratory flow when 25% of forced vital capacity remaining to be expired, MEF50%: maximal expiratory flow when 50% of forced vital capacity remaining to be expired, MEF75%: maximal expiratory flow when 75% of forced vital capacity remaining to be expired, FEF25%–75%: forced expiratory flow during 25%–75% of forced expiration, PIFR: peak inspiratory flow rate, MVV: maximum voluntary ventilation, L/s: litre per second, L/min: litre per minute.
a p < 0.05.
MDA was observed to be significantly high (p < 0.05) while FRAP was significantly low (p < 0.05) in styrene-exposed subjects. GSH level were significantly depleted in exposed subject (p < 0.05) as compared to control group (Table 4). The mean value of serum cytochrome c in styrene exposed subjects was found to be 1.1 ng/ml (0.89–1.89) while in control its levels were under detection limit (0.05 ng/ml). The workers when divided on the basis of duration of exposure in the present factory (less than or more than 5 years) did not show any significant change in most of the lung function parameters, MDA and GSH, while PEFR, MEF75%, VC and FRAP were significantly low in workers exposed to styrene for more than 5 years (Tables 5 and 6).
Oxidative stress of controls and subjects occupationally exposed to styrene

MDA: malondialdehyde, FRAP: ferric-reducing ability of plasma, GSH: reduced glutathione.
a p < 0.05.
Comparing lung function test among workers exposed to styrene for less than 5 years and more than 5 years

FVC: forced vital capacity, FEV1: forced expiratory volume in first second of forced expiration, PEFR: peak expiratory flow rate, MEF25%: maximal expiratory flow when 25% of forced vital capacity remaining to be expired, MEF50%: maximal expiratory flow when 50% of forced vital capacity remaining to be expired, MEF75%: maximal expiratory flow when 75% of forced vital capacity remaining to be expired, FEF25%–75%: forced expiratory flow during 25%–75% of forced expiration, FIVC :forced inspiratory vital capacity, PIFR: peak inspiratory flow rate, VC: vital capacity, TV: tidal volume, ERV: expiratory reserve volume, IRV: inspiratory reserve volume, IC: inspiratory capacity, MVV: maximum voluntary ventilation, L/s: litre per second, L/min: litre per minute, L: litre.
a p < 0.05.
Comparing oxidative stress among workers exposed to styrene for less than 5 years and more than 5 years

MDA: malondialdehyde, FRAP: ferric-reducing ability of plasma, GSH: reduced glutathione.
a p < 0.05.
Discussion
In the present study, we observed that most of the lung volumes, capacities (FVC, FEV1, VC, ERV, IRV, and IC) and flow rates (PEFR, MEF75%, and MVV) were significantly lesser in the workers exposed to styrene as compared to controls. Earlier, Lorimer et al. 19 observed that the styrene is an irritant of upper respiratory tract and a cause of low FEV1%. He observed that 36% smokers while, 30% of non-smokers had FEV1% less than 75%. However, in our study FEV1% was not reduced, both in smokers and non-smokers but other PFT values (FEV1, PEFR, MVV, etc.) were found to be decreased in exposed subjects. It is well known that smoking affect lung function and is a causative agent of many diseases.20–22 On analyzing the two groups by univariate analysis it was found that the changes observed in pulmonary functions and oxidative stress in the present study were not due to the confounding influence of smoking. Oner (2004) observed that only one subject out of 47 workers exposed to styrene had PEFR records compatible with work related asthma despite the absence of positive provocation test with styrene. Their study was only suggestive of styrene as a causative agent of asthma but not a conclusive one. 23 Our study also indicates reduced PEFR in factory workers following styrene exposure. Exposure to styrene mainly occurs by inhalational route, lung epithelial cells are primarily involved in the toxic and/or inflammatory responses. Airway epithelial cells are known to act as immune effectors by secreting pro-inflammatory mediators. Excessive production of pro-inflammatory mediators by the airway epithelium is proposed to have a key role in the development of tissue injury during acute and chronic inflammatory conditions, implicating the airway epithelium in the pathogenesis of inflammatory lung diseases.24,25
Subjects when compared on the basis of duration of exposure, there were no significant differences in most of the lung functions in the two groups except for PEFR, MEF75%, and VC, which were found to be significantly reduced among subjects exposed to styrene for more than 5 years. Levels of FRAP were significantly reduced in workers exposed to styrene for more than 5 years and no significant difference in cytochrome c was observed among two groups. None of the lung functions were found to correlate with levels of MDA, FRAP, and GSH as well as with the duration of exposure. Cumulative exposure to styrene have not been associated with an increased mortality, in fact the risk of lung cancer was higher in workers exposed to styrene for less than 1 year as compared to workers exposed for more than 1 year. 26 Several other studies have also reported higher mortality among workers occupationally exposed to chemicals for a shorter duration.27–29 Wong and Musselman (1993) reported significantly increased mortality from lung cancers among slag wool workers employed for less than 5 years but not among those employed for 5 years or longer. 27 Gubéran and Usel (1987) reported significantly increased mortality for all causes, all cancers, lung cancer, violent deaths, and other accidents in a cohort of workers employed for less than 1 year in the perfumery industry in Geneva. 28 Similarly, McDonald et al. reported significantly increased mortality from all causes, all cancers, respiratory cancer, heart disease, and other non-malignant respiratory disease among workers at a friction products factory with less than 1 year of employment, but such increases were not found among long-term employees. 29 These authors have suggested that workers exposed to styrene for a smaller duration might have been assigned to jobs having heavier exposure and consequently, experienced a higher mortality risk. The reason for discordance of lung function derangement and duration of exposure might be that maximum damage to lungs have been caused in early period of exposure and also young workers exposed to less duration might have been assigned heavy load of works as compared to senior ones.
As during inhalational exposure to styrene, airway epithelium is first to be encountered. The airway epithelium, in response to it, releases reactive mediators, which play an important role in the inflammatory response. Since, styrene is metabolized into styrene oxide in lung and liver, it leads to generation of free radicals, which may cause toxicity via oxidative stress. 30 Excess of oxidative reactions is an important mechanism contributing to styrene oxide neurotoxicity in vitro in SK-N-MC cells and point to a role of oxidative stress in the early phase of styrene oxide triggered apoptosis in neurons. 31 When A549 cells were exposed to styrene in the presence of antioxidant N-acetylcysteine, decreased expression of inflammatory mediators is seen, which clearly suggest role of oxidative stress in styrene oxide toxicity. 30
In the present study, the levels of MDA were significantly higher (p < 0.05) and levels of FRAP and GSH were significantly lower (p < 0.05) in styrene-exposed subjects compared to controls. GSH plays a primary role in protecting cells from oxidative stress and in detoxifying foreign compound. Recently, it has been reported that GSH is a principal antioxidant in the lung epithelial lining fluid, this fall due to styrene exert a significant influence on the ability of the lung to buffer oxidative damage. 32 Existing data also indicate that both styrene and its metabolites styrene oxide (SO) may induce oxidative stress, which is known to act in concert with mitochondrial dysfunctions. Depletion of GSH was observed in different brain region of rat exposed to SO as well as SO-exposed noradrenergic PC12 cells. A lower level of GSH was found associated with increased lipid peroxidation in the liver of rodents exposed sub-chronically either to styrene or to SO. 33 It has been reported that styrene and its metabolites SO cause significant decrease in GSH level, but they have little effect on the enzymes glutathione reductase and glutathione peroxidase. 34 Daré et al. proposes that free radicals were generated when SK-N-MC cells were exposed to styrene oxide (0.3 mM for 12 h) in vitro, which damages mitochondrial membrane increasing its permeability facilitating release of cytochrome c, resulting in apoptosis of cells. 33 The depleted levels of GSH are co-related well with the increased levels of cytochrome c. 13 The redox disequilibrium consequent to GSH depletion is likely to be the direct cause for cytochrome c translocation, since the mechanisms proposed to be responsible for cytochrome c release. The level of oxidative stress markers along with cytochrome c were elevated in workers with disarranged pulmonary function test. Redox disequilibrium is responsible for cytochrome c release from mitochondria and also free radicals generation, which damages the lung parenchyma in workers. Our study is corroborated with other studies where it is shown that the mechanism of toxicity of styrene is due to free radical generation.33,35,36
It may be concluded that styrene is found to affect lung functions and cause oxidative stress in plastic factory workers. Appropriate preventive measures should be taken at the earliest by using masks, proper ventilation and antioxidants. This will ensure the purpose of study to benefit the mankind. Further studies with large sample size, along with air concentration of styrene in factory, which identify the role of other oxidative stress parameters along with assessment of hormonal, inflammatory, and immunological factors are clearly needed.
Footnotes
Acknowledgements
We are thankful to Dr Shailendra Kumar Gautam, Department of Physiology, Lady Harding Medical College, and Miss Upasana Bisht, Department of Nursing, St. Stephen Hospital, Delhi, for their assistance in factory search and sample collection. I acknowledge the support given by Dr. Vinod kumar, Dr. Parmod Kumar, Department of Physiology, UCMS, and MD Mustafa, Department of Biochemistry, UCMS.
This research received no specific grant from any funding agency in the public, commercial, or not for-profit sectors.