
Abstract
To investigate late toxic effects of sulfur mustard (SM) on the upper and lower respiratory tracts of Iranian veterans, 43 male veterans with more than 25% disability due to SM poisoning in 20−25 years after exposure, were studied. Direct laryngoscopy, pulmonary function tests, arterial blood gasses and pH, computed tomography of sinuses and lungs were investigated. The patients were aged 50.6 (8.9 SD) years with body mass index (BMI) of 26.6 (4.0) and disability of 53.2 (17.0%). The common findings of the upper respiratory tract were dysphonia (79.1%), post-nasal discharge (PND; 41.9%), lower larynx position (30.2%), limitation of vocal cords (25.6%) and mucosal inflammation of larynx (14.8%). The common lower respiratory diseases were diagnosed as chronic obstructive respiratory disease (84%), bronchiectasis (44.1%) and lung fibrosis (7.7%). Severity of disability was negatively correlated with BMI (p = 0.032), spirometric parameters (p < 0.001) and oxygen saturation (p < 0.001), but positively correlated with low-density lipoproteins (LDL <0.010), blood pressure (p = 0.008), diabetes mellitus (p < 0.001), wheezing (p = 0.0043) and bronchiectasis (p < 0.001). Delayed toxic effects of SM in upper and lower respiratory tracts were mostly inflammatory and infectious complications, SM-induced disabilities were significantly correlated with risk factors such as diabetes mellitus, hypertension, LDL and lower-respiratory complications.
Introduction
Sulfur mustard (SM) or bis (2-chloroethyl) sulfide or mustard gas is an alkylating chemical warfare agent. It was widely used during the World War One and in the Iran-Iraq conflict. 1 –4 Inhalation is the major route of exposure, which induces respiratory and systemic toxicity following absorption across the lung surface. However, SM is a vesicant or blistering agent that has direct toxic effects on the skin producing erythema, blistering, epidermolysis and necrosis. 2 The eyes are the most sensitive organs to SM, but the respiratory system is the most affected target organ in terms of toxicity, either in acute phase or in late complications. 2,5 –10
Acute toxic effects of SM on the eyes, respiratory tract and the skin are more prominent than on the other organs. However, hemato-immunological system is involved and its suppression in severe toxicity may cause death. The first symptoms of SM exposure usually occur on the eyes, such as itching, lacrimation, leading to acute conjunctivitis, blepharospasm and keratitis. But the greatest toxicity of mustard gas results from irritation and pathological changes of the respiratory system. Respiratory effects occur in a dose-dependent manner from the nasal mucosa to the terminal bronchioles. Coughing, dyspnea, chest pain and acute rhino-pharyngo-tracheobronchitis occur within hours after SM exposure. In severely intoxicated patients, bronchopneumonia and adult respiratory distress syndrome may develop several days later, causing severe morbidity and mortality. 5,11 –14
Sub-acute exposure occurred during the Iran-Iraq war and in the workers in SM munitions factories. However, this type of exposure may present as a mild acute SM intoxication or as a complication in the respiratory tract or later as a malignancy. 6,15
Delayed toxic effects of SM have been documented. The first report of delayed toxic effects in Iranian veterans was published in 1986, indicating respiratory system as the most affected organ. 6 Several articles on the delayed toxic effects and complications of SM, mainly on the respiratory system of Iranian veterans, have been published over the past decades. 7,16 –22 The focus of all these investigations were on the lower respiratory tract, reporting chronic bronchitis, bronchiolitis, obstructive and restrictive lung diseases, bronchiectasis, chronic obstructive respiratory disease and rarely lung fibrosis.
There has been only one report on sinus computed tomography (CT) scan in patients with chronic cough following sulfur mustard inhalation 10 and one on the late laryngeal complication of SM poisoning in Iranian veterans. 23 Therefore, it appears that the late toxic effects of SM on the upper respiratory tract of Iranian veterans have not previously been reported. We thus aimed to investigate the late toxic effects of SM on the upper respiratory tract of Iranian veterans and their relationships with lower respiratory tract complications and some risk factors such as body mass index (BMI), high blood pressure, diabetes mellitus and lipid profiles.
Patients and methods
Following coordination with Khorassan Razavi veteran foundation and approval of the University medical and research ethics, 43 patients with disabilities of more than 25% due to complications of SM poisoning were investigated. Disability of the veterans was calculated based on the severity complications of SM poisoning on a standard format in the veteran foundation over the years after SM exposure and reviewed whenever required. Main complications were observed on the respiratory system. Skin and eyes complications caused much less disabilities and thus did not significantly contribute. However, disabilities were estimated upon objective clinical findings and paraclinical investigations such as CT scan and arterial blood gasses.
The patients who had a history of allergy, smoking, drug abuse, occupational chemical exposure and respiratory or cardiovascular diseases prior to SM exposure were excluded.
The study was carried out in June 2009 at the Medical Toxicology Research Center (MTRC) of Imam Reza hospital. The patients exposed during the Iraq-Iran war in 1984−1988. They were admitted on fast in groups of 5−7 patients each day in the early morning. Following presentation of the aims and procedures of the study, obtaining the informed consent, 5 mL venous blood samples from the brachial vein were drawn for routine biochemical tests and then breakfast was served.
Two physicians of the research team (4th and 5th authors), interviewed and examined the patients. All demographic information, medical histories, previous documents, measurement of weight, height and results of the physical examination of the patients were recorded in pre-designed forms. All patients were examined by the experienced otolaryngologist (3rd author) and chest physician (6th author). The otolaryngologist examined all patients under direct fiber optic rhinoscopic and laryngoscopic procedures. The results were registered in case talking and physical examination form.
Pulse oximetry was done for all patients and for those who had oxygen saturation of less than 93%, arterial blood gas (ABG) was also performed. ABG was carried out in the MTRC laboratory using blood gas analyzer (Stat Profile Phox Nova Biomedical, MA, Waltham, USA). Biochemical tests including fast blood sugar (FBS), blood urea nitrogen (BUN), creatinin, uric acid, cholesterol; high-density lipoprotein (HDL), low-density lipoprotein (LDL) and very low-density lipoprotein (VLDL) was done in the central laboratory of Imam Reza hospital by auto analyzer Technicone, NY, Tarrytown, USA). CT scan of sinuses and high resolution of CT scan of the lungs (HRCT) were performed for those whom clinically indicated in the Radiology Department of the hospital using CT scanner (General Electric 9800, NY, Tarrytown, USA).
Pulmonary function tests (PFT) were carried out by an experienced technician, at the respiratory unit of the hospital, using spirometer (Spiro Lab 2, Chest Tokyo, Japan). Forced vital capacity (FVC) more than 80% and forced expiratory volume at one second (FEV1) more than 75% of the predicted value were considered normal. FVC < 80% and FEV1 < 75% described as obstructive pattern, FVC < 80% and FEV1 > 75% as restrictive pattern.
Hypertension and diabetes mellitus were considered based on their history and previous medical records. Diagnosis of upper and lower respiratory diseases were made by the otolaryngologist and chest physician based on the clinical findings, imaging, PFT and ABG results. For BMI, patients' weight in kilograms (kg) divided by their height in meters (m) squared. The patients were all on medications such as salbutamol and corticosteroid inhalers and in ethical point of view we did not ask them to stop their prescribed medicines.
The study was an observational case series. However, relevant statistical tests such as chi-square and Spearman correlation tests were applied using statistical package for social sciences (SPSS, version 11.5). Statistical significant level considered was to be 0.05 throughout the study.
Results
General
The 43 male patients studied were aged 39 to 71 years with a mean of 50.6 (8.7 SD). Age distribution of the patients is shown in Figure 1 . The BMI of the veterans varied between 18.9 and 34.0 with a mean of 26.6 (4.0). They were all married with a number of children ranging from 0 to 10 with a median of 3. Nearly half (48.8%) of them revealed a history of surgical operations, of which 8 (18.6%) patients had undergone sinus surgery and 2 (4.65%) had lung surgery. History of hypertension, diabetes mellitus, hyperlipidemia, ischemic heart disease, asthma and hemorrhagic disorders were recorded in 17 (39.5%), 8 (18.6%), 13 (30.2%), 19 (44.2%), 13 (30.2%) and 6 (14%) patients, respectively. Their disability due to complications of SM poisoning were between 25% and 70% with a mean of 53.2 (17.0%). There was a significant negative correlation between the severity of disability and BMI (p = 0.032) as shown in Figure 2 . There were significant positive correlations between the severity of disability and low-density lipoproteins (LDL; p = 0.010) or blood pressure (p = 0.008) or diabetes mellitus (p < 0.001).

Age distribution of 43 Iranian male veterans with respiratory complications of sulfur mustard poisoning. The age years were placed in the middle bottom of each column and thus the age range of the figure is between 37.5 and 72.5 years to cover all patients' ages.

Correlation between body mass index (BMI) and severity of disability (%) due to complications of sulfur mustard poisoning in 43 Iranian male veterans.
Subjective findings such as coughing (97.7%), dyspnea (97.7%), sputum (88.4%) and headache (81.4%) were more common than the objective findings. The patients were all symptomatic.
Upper respiratory complications
The common objective findings of the upper respiratory tract were dysphonia (79.1%), chronic sinusitis (55%), PND (41.9%), lower larynx position (30.2%), limitation of vocal cords (25.6%) and mucosal inflammation of larynx (14.8%).
CT scan of sinuses revealed chronic sinusitis in 55% of the patients. Sphenoidal, posterior ethmoidal and maxillary sinuses were more involved than anterior and frontal sinuses (p < 0.001). Topography of chronic sinusitis in both sides is shown in Figure 3 . Frequency of opacity in different sinuses on CT scan in each side is given in Table 1 . There were no significant differences between the involvements of right and left side sinuses. However, significant positive correlations between the chronic sinusitis on CT scan and facial pressure (p = 0.036) or popping (p = 0.024) or eye pressure sensation (p = 0.046) were obtained. No significant correlations between the severity of disability due to SM poisoning and any of the upper respiratory complications were achieved.
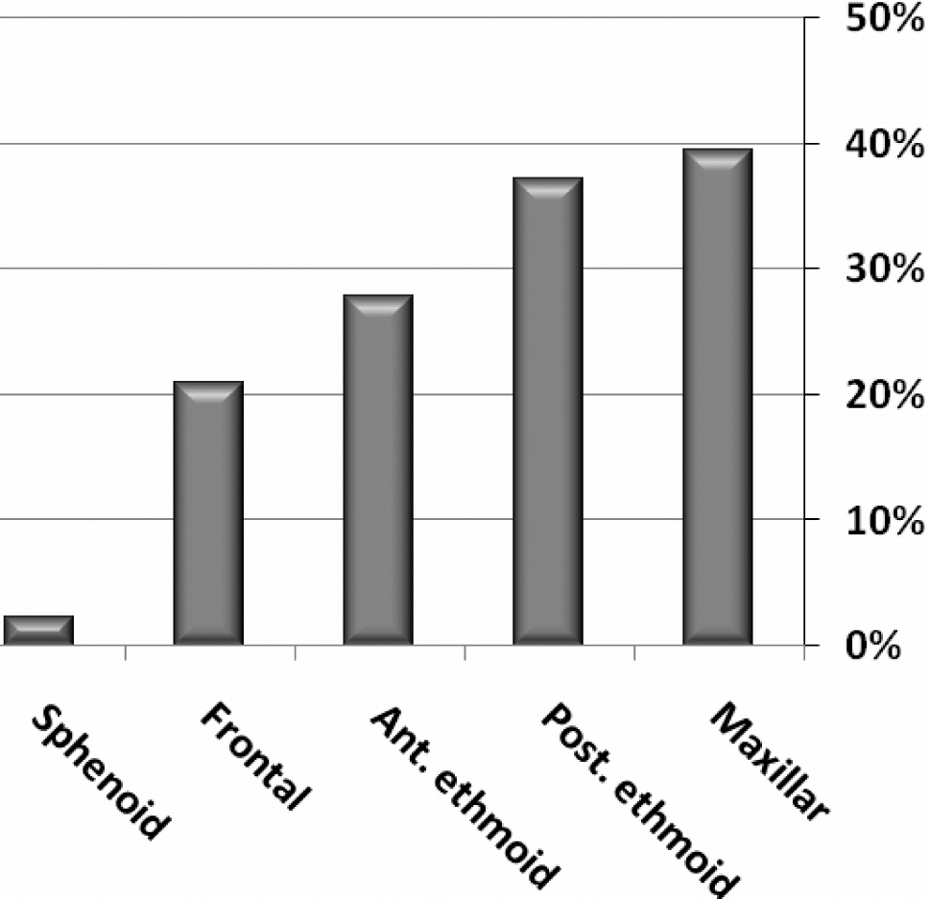
Distribution of frequencies of different sinusitis in both sides of 43 Iranian male veterans with respiratory complications of sulfur mustard (SM) poisoning.
Frequency percentages of opacity on CT scan in different sinuses of 19 out of 43 Iranian male patients with respiratory complications of sulfur mustard poisoning a
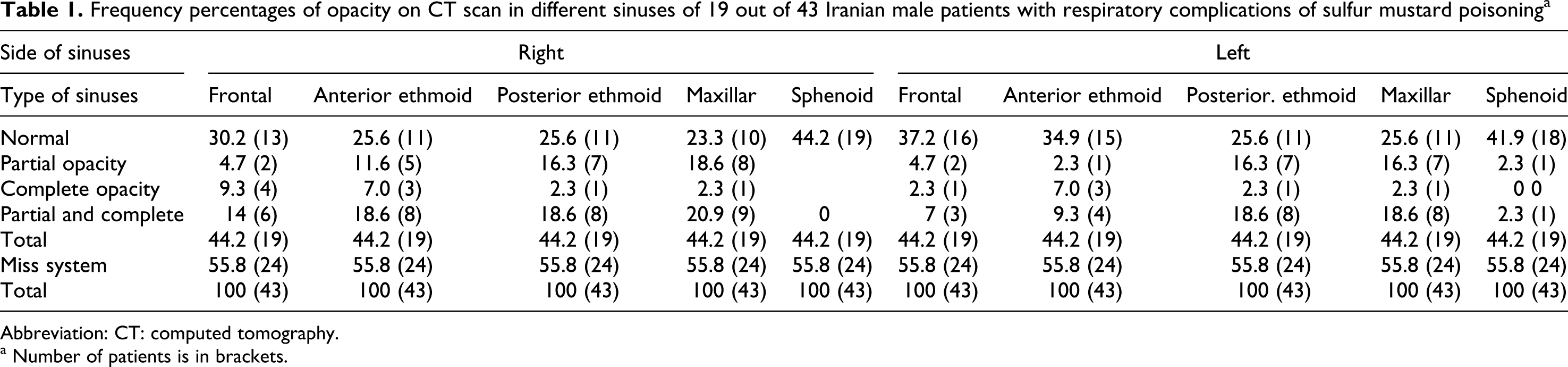
Abbreviation: CT: computed tomography.
a Number of patients is in brackets.
Lower respiratory complications
The common objective findings of the lower respiratory tract were generalized wheezing (45.2%), ronchi (45.2%) and crackle (23.8%). FVC of the patients varied between 0.97 to 4.64 L with a mean of 2.9 (1.0 SD), which were 23% to 114% of the predicted value with a mean of 71.5% (23.3%). FEV1 were recorded between 0.47 to 4.0 L with a mean of 2.1 (1.0) L, which were between 14% and 127% of the predicted value with a mean of 65.4% (32.4%). FEV1/FVC of the patients varied between 36% and 88.8% with a mean of 69.5% (15.5% SD). Overall, 35% of the patients had normal PFT, 55% obstructive pattern, 6.8% restrictive and 6.8% mixed pattern.
Arterial blood pH of the patients varied between 7.24 and 7.45 with a mean of 7.36 (0.40 SD). O2 saturations were recorded between 80% and 97% with a mean of 93.9% (3.6%). Mean PO2, PCO2 and bicarbonate were 32.14 (07.80), 55.44 (07.33) mm Hg and 39.10 (04.10) mmol/L, respectively.
HRCT of the lungs were normal in 23.5%. Bronchiectasis, air trapping, emphysema, interstitial fibrosis and tracheal stenosis were diagnosed in 44.1%, 29.4%, 20.6%, 11.8% and 5.9% of the cases, respectively.
The common lower respiratory diseases were diagnosed as chronic obstructive respiratory disease or COPD (84%), bronchiectasis (44.1%) and lung fibrosis (7.7%). There were significant positive correlations between the severity of disability and wheezing (p = 0.043) or bronchiectasis (p < 0.001). As expected, the severity of disability was reversely correlated with spirometric parameters (p < 0.001) and O2 saturation (p < 0.001).
Correlations between upper and lower respiratory complications
Mucosal inflammation of larynx was significantly correlated to FEV1 (p = 0.006), FVC (p = 0.008), FVC predict (p = 0.001), FEV1 predict (p = 0.016), FEV1/FVC (p = 0.031) as well as to bronchiectasis observed in HRCT (p < 0.001). Similarly, vocal cords movement limitation was significantly associated with FEV1 predict (p = 0.022), FEV1 (p = 0.033), FEV1/FVC (p = 0.002). FVC predict (p = 0.060) failed to be significant. Limitation of vocal cords movement was significantly correlated with fibrosis (p = 0.003). No further significant associations were found between upper and lower respiratory complications.
Discussion
General
Respiratory complications are the greatest cause of long-term disability in patients with SM poisoning. The main objective of this study was to investigate the upper respiratory complications in patients with moderate-to-severe disabilities of SM poisoning and their relationships with the lower respiratory complications and some common risk factors in the same patients. We found interesting and surprising results. For instance, although the mean BMI of the patients was in overweight level (26.6), we found a significant negative correlation between the severities of SM toxicity or disability and BMI (Figure 2). It seems that lower BMI is associated with more recurrent infections and related disabilities, although higher BMI may increase dyspnea and respiratory failure. This is a new finding and has not been previously reported. However, as expected, other risk factors such as hypertension, diabetes mellitus, LDL cholesterol, wheezing and bronchiectasis had significant positive correlations with the severity of disabilities due to SM poisoning. Parts of these findings like significant positive correlations between the lower respiratory complications and the severity of disabilities have been previously reported. 12,17,19,21 In fact, disability severity had been calculated mainly based on the respiratory complications of SM poisoning.
Upper respiratory complications
There has been only one report on the upper respiratory complication of SM poisoning, focusing on the laryngeal complications, 23 whereas we investigated all parts of the upper and lower respiratory tracts. However, there are some similarities between the two studies on the dysphonia (the most common signs in both studies), the limitation movement of vocal cords and PND (40.7% in our study and 44% in Akhavan report). Disagreements are on the mucosal inflammation of the sinuses (25.9% in this investigation and 79% in Akhavan study) and unilateral paralysis of the vocal cords in three patients (6%) of Akhavan and none in our study. In addition, Akhavan and associates found six patients (12%) with laryngeal nodules and we did not find any.
Chronic sinusitis was the most common complications of upper respiratory tract after dysphonia in our veterans as judged by the clinical observation and CT scan of the sinuses. According to our otolaryngologist clinical observation, at least one sinus of each patient was affected. However, chronic sinusitis on CT scan was diagnosed in 55% of the patients. There were agreement between the radiology report and the otolaryngologist judgment on the CT scan. Significant positive correlations between the chronic sinusitis on CT scan and facial pressure or popping or eye pressure sensation revealed that clinical observation of the otolaryngologist is in agreement with the radiology report. The authors could not find similar reports in the national or international medical literature to compare with these findings.
We found no malignancy on the upper respiratory tract in these patients, but our otolaryngologist and associates 24 have reported a case of nasopharyngeal carcinoma in a 38-year-old man 12 years after SM exposure and two male patients 34 and 36 years old with thyroid carcinoma 12 and 14 years after SM exposure, respectively. Easton and his colleagues 14 have also reported cases of laryngeal carcinoma of the British SM factories.
Lower respiratory complications
A triad of cough, expectoration and dyspnea has been found to be present in more than 80% of severely intoxicated Iranian veterans 3 years after their initial exposure. 6,20 These symptoms persist and even get worse over the years in severe cases despite continuous medical care as indicated in recent reports. 12,19,21
The main objective clinical findings of the lower respiratory tract in our patients including generalized wheezing (the most common sign), rhonchi and crackles are in agreement with the previous reports. 12,19,21
Pulmonary function testing has revealed more obstructive patterns than restriction. It was initially believed that due to lung fibrosis, obstructive pattern will change over the years to restrictive pattern, 6,16 but further investigations revealed that lung fibrosis is not a common complication of sulfur mustard poisoning. 18,21 Bronchiolitis and tracheobronchmalacia with air trapping were then introduced as a common pathology in the Iranian patients with SM poisoning. 18,20
Several studies have reported chronic bronchitis as the most common late complication of SM poisoning in Iranian veterans. 6,16,17 However, hypoxemia and hypercapnea are commonly observed in moderate-to-severe cases, leading from asthmatic bronchitis to COPD, core pulmonale and respiratory failure in the final stages of the disease. 18,19,21 COPD was found the most common lower respiratory complication in our patients, which was much higher than the previous study on these patients. 21
Infection of the respiratory tract results in bronchopneumonia at the early stage but later in the course induces bronchiectasis as was diagnosed in this study and reported earlier. 15,18,21 Direct effects of SM on the bronchial wall mucosa and more recurrent respiratory infections following SM inhalations are known to be responsible for the development of bronchiectasis. Both the severity and frequency of bronchiectatic lesions tend to increase over the long-term follow-ups, as evidenced by a study of 40 Iranian veterans with severe late complications of SM poisoning. 21 These lesions usually begin bilaterally in the lower lobes and then progress toward the middle lobe and the lingula. In severe cases with extensive bronchiectatic lesions, pulmonary hypertension and ultimately core pulmonale may occur. 21,25
We found no malignancy on the lower respiratory tract in these patients, but different kinds of lung cancer, mostly bronchial adenocarcinoma, were reported in workers of the SM factories. 15,26 Hematological and immunological disorders either in the early stage or in the long term causing high morbidities and mortalities have been reported. 27 –32 Therefore, we did not include it in this study.
Correlations between the severity of disability and upper or lower respiratory complications
Although no significant correlations between the severity of disability due to SM poisoning and any of the upper respiratory complications were found, the patients with higher disabilities revealed complications of upper respiratory tract. Since dysphonia and sinusitis were very common and the other complications such as mucosal inflammation were much less common and perhaps because of the low power of study due to the limited number of patients, we could not obtain any significant correlations.
Significant positive correlations between the severity of disability and wheezing, or bronchiectasis, are logical but have not been previously reported. As expected, severity of SM disability was reversely correlated with spirometric parameters and O2 saturation. These parameters had been used for the severity evaluation of the veteran disability due to complication of SM poisoning. 8
We could not find any significant correlations between dysphonia or sinusitis and any of the lower complications of SM poisoning. This might be due to different pathology of the upper and lower respiratory complications or even lack of power in this study as some of the findings were scarce. However, mucosal inflammation of larynx was significantly correlated to FEV1, FVC, FVC predict, FEV1 predict, FEV1/FVC as well as to bronchiectasis in HRCT. Similarly, vocal cords movement limitation was significantly associated with FEV1 predict, FEV1, FEV1/FVC. However, FVC predict failed to be significantly related to vocal cords movement limitation. This limitation was also significantly correlated with fibrosis. These correlations suggest of a similar inflammatory process in both upper and lower respiratory tracts. There has been no report on this matter in the medical literature to compare with these findings.
Limitation of the study
We could not monitor carboxyhemoglobin and toxicology screen for drug abuse. Therefore, because of the gaining, history taking from the veterans on the smoking and drug abuse has not been objectively recorded. Due to some technical problems, we were not able to perform hematological and immunological investigations in these patients, but our previous study revealed mainly leukocytosis due to recurrent respiratory infections and immunosuppression including significant decrease in natural killer cells.28,31
The power of this study might be inevitably limited for some of the scarce findings. The study was an observational case series and thus no blinding was considered. The patients were taking medication during the study and we could not stop it due their needs and ethical consideration.
Conclusion and recommendation
Upper respiratory complications of SM poisoning in the veterans including chronic sinusitis, laryngeal inflammation and displacement are common and reported for the first time in the Iranian veterans. Lower respiratory complications of the veterans have been worsened over the years as judged by more common severe diseases such as COPD in comparison with the study of 2005 on the same patients. There were some correlations between upper and lower respiratory complications of SM poisoning in the veterans, which may be suggestive for similar pathological process. Association between SM-induced disabilities and diabetes mellitus, hypertension, LDL and lower respiratory complications may raise the possibility of SM ethologic association for these complications. It seems that the delayed toxic effects of SM in upper and lower respiratory tracts were mostly inflammatory and infectious complications. However, further study with a control group and larger number of cases with more detailed investigations is recommended.
Footnotes
This manuscript was prepared exceptionally for the journal of Human and Experimental Toxicology. It has not been submitted elsewhere and will not be submitted to any other journal. Some parts of these findings have already been presented as a poster at the 12th International Congress of Toxicology on, 19-22 July 2010 in Barcelona, Spain.
Acknowledgement
Financial support of the Vice-Chancellor for Research of Mashhad University of Medical Sciences (MUMS) is acknowledged. Technical assistance of the head nurse; Mr Mohammad Rajaei and all nursing staff of the Toxicology Ward and the staff of Medical Toxicology Research Center are greatly appreciated. Co-operation of Mr Mohssen Namaei-Ghassemi and other laboratory technicians are also acknowledged.
There has been no conflict of interest for this study. The investigations were fully financially supported by MUMS.
This research was only funded by the Research Department of Mashhad University of Medical Sciences, Iran.