
Abstract
The most common delayed complication of sulfur mustard (SM) poisoning has been observed in the respiratory tracts. It was thus aimed to investigate the delayed respiratory complications in SM-exposed patients around 25 years before the study. Forty-three veterans with more than 25% disability of due to SM poisoning were investigated. Clinical examinations as well as pulmonary function test (PFT) were performed. High-resolution computed tomography (HRCT) of the lungs was done as clinically indicated. Triad of chronic cough, dyspnea, and expectoration were the most common symptoms that were recorded in 88.2%, 88.2%, and 64.7% of the patients, respectively. PFT abnormalities were detected in 44.18% of the patients. Restrictive pattern was the most common (41.86%), while pure obstructive pattern did not detect at all. Mixed pattern was significantly correlated with higher disability percentages among the veterans (p < 0.001). Significant reverse correlation between the disability percentages and forced expiratory volume in 1 s/forced vital capacity ratio was obtained (p = 0.010, r = −0.389). Air trapping was the most common abnormality in HRCTs (50%). Bronchiectasis (25%), pulmonary fibrosis (25%), and ground-glass attenuation (16.66%) were other common HRCT findings. Comparing with the previous studies on these patients, more restrictive and mixed pattern were observed. Moreover, bronchiolitis, bronchiectasis, and lung fibrosis were the main pathological findings in these patients.
Introduction
Chemical warfare agents (CWAs) were used in a large scale during the World War I for the first time. Since then, they have been used several times, of which the Iran–Iraq conflict was the most devastating chemical war. 1 Sulfur mustard (SM) is a blistering CWA, which was extensively used by Iraqi troops, against Iranian military personnel and even civilians of border cities of Iran and Iraq. 2 –4
The toxicity of SM results from irreversible alkylation of some proteins and nucleic acids, particularly DNA. SM initially forms a cyclic ethylene sulfonium ion intermediate followed by electrophilic attack on target molecules, which can result in inhibition of the proteins, nucleic acids, and adenosine triphosphate biosynthesis. 5
The major alkylating site of nucleic acids is the nitrogen residue of guanine in mammalian origin. The result is manifested in chromatid aberration and inhibition of DNA, RNA, and protein synthesis. SM can also react with proteins and phospholipids; however, the consensus had been made that DNA alkylation has an effective role in delayed complications. 5,6
Acute SM poisoning may occur as a result of both inhalation of vapor or percutaneous absorption of SM. However, the most effective route of absorption is by inhalation. Moist tissues of the eyes, respiratory tracts, axillary, and genitalia considerably increase SM absorption. 6 Nevertheless, the extent of tissue injury also depends on such factors including duration and intensity of exposure. 6,7 Compared to other CWAs such as nerve agents, SM has relatively lower acute mortality rate (2–3%) and thus it is known as “incapacitating agent.” 7 However, in cases with severe acute lung injuries, prognosis is very poor, even when sophisticated facilities and intensive care therapy are applied. 7,8
The most acute and also delayed toxicity of SM are in the eyes, the skin, and the respiratory tract which are the three major target organs of human body. 8,9 However, the respiratory system is the most vulnerable organ, which causes the most morbidity and mortality. Both upper and lower respiratory tracts are involved in SM intoxication that may develop chronic respiratory sequelae. In a study on 236 Iranian veterans with late complications of SM exposure, the most involved organs were respiratory tract (78%), central nervous system (45%), the skin (41%), and the eyes (36%). 10 Respiratory complications are the most common cause of long-term disability among SM-exposed people. 6 In the lungs, SM can induce bronchial mucosal injury, inflammation, fibrosis, and pneumonia. 2,6,11 Dyspnea, coughing, and chest discomfort are acute respiratory symptoms which may lead to acute rhinopharingotracheobronchitis. In severe intoxicated patients, bronchopneumonia, adult respiratory distress syndrome, and even pulmonary emboli may occur during the second week postexposure. 8,12,13 Triad of cough, expectoration, and dyspnea was reported in 80% of SM-poisoned Iranian veterans 3 years after single SM exposure. 8,14 Chronic objective findings are generalized wheezing, decreased lung sounds, crackles, clubbing, and cyanosis. 8,14,15
Earlier studies on SM-intoxicated patients, revealed more obstructive pattern in pulmonary function tests (PFTs) than restrictive. 5,14 –16 However, restrictive pattern has been reported to increase in longer times after SM poisoning and was even the dominant respiratory pattern in recent years. 17,18 In a retrospective cohort study by Ghanei et al. on 215 Iranian veterans with severe initial symptoms of SM exposure, forced expiratory volume in 1 s/forced vital capacity (FEV1/FVC) and FEV1% of 0.775 ± 0.123 and 80.9 ± 22.2 were recorded that did not significantly differ between mild and moderate intoxication (at the exposure time). 19
Delayed toxic effects of SM on upper and lower respiratory tracts of 43 Iranian veterans were prospectively investigated by Balali-Mood et al. 20–25 years after exposure. PFT revealed 55% obstructive pattern, 6.8% restrictive, and 6.8% mixed pattern, while 35% of the patients had normal PFT. 20 Delayed respiratory involvements of SM is also revealed in high-resolution computed tomography (HRCT). Chronic bronchitis has been reported by several studies as the most delayed finding in SM patients HRCT. 16,21 –24 Air trapping, Bronchiectasis, large airway narrowing, and pulmonary fibrosis were also evident as common delayed HRCT results in SM-exposed patients. 21 –26 In a study of 197 Iranian veterans conducted by Emad and Rezaian 10 years after initial SM exposure, the diverse effect of SM on respiratory system was explained. 17 Chronic bronchitis (58%), asthma (10%), bronchiectasis (8%), large airway narrowing (9%), and pulmonary fibrosis (12%) were reported in the veterans. 17 Balali-mood et al. in a multi-organ survey of 40 SM Iranian veterans 16–20 years postexposure (2005) reported bronchiectasis and pulmonary fibrosis as the most common HRCT findings. 16
As a result of continues threat of chemical war or terrorism, CWAs particularly SM remain to be a subject of considerable toxicological research topic. Respiratory complications, as the most cause of long-term disability among SM patients, need more attention of health-care providers. It was aimed in this study to determine the delayed respiratory complications of SM poisoning by means of physical examination, PFT and HRCT, among Iranian veterans, three decades after exposure.
Methods
Patients and setting
This cross-sectional study was conducted on 43 Iranian SM-exposed veterans that recruited from Veterans and Martyrs Affair Foundation (VMAF) of Khorasan Razavi province to Medical Toxicology Research Center (MTRC), Mashhad, Iran, during 3 months in early 2012. All the veterans had a single SM exposure via inhalation during Iran–Iraq battle and had more than 25% chemical disability percentages at the time of study, as certified by VMAF medical committee. VMAF (Janbazan foundation) is a governmental association organized to support veterans and war victims. Disability percentages are determined by a medical committee of VMAF according to the severity of complications in different organs. For each veteran, three kinds of disability are defined: physical, chemical, and total, which includes both physical and chemical disabilities. Disability percentages are updated biannually by the committee and any changes in percentages are recorded. Each veteran had only one high-dose exposure to SM during chemical bombardment; however, it was not possible to measure the initial exposed dose because of the gas spread through an indefinite area. The study was approved by the Research Ethics Committee of Mashhad University of Medical Sciences, Mashhad, Iran.
Every week, seven SM veterans who were diagnosed as moderate to severe intoxicated patients according to the latest assessment of VMAF (chemical disability percentage of more than 25%) and had signed the written informed consent, were recruited to the MTRC. As the first step, 10 mL blood samples from brachial vein were taken after 12 h of fasting for hematological and biochemical tests. Demographic data and CWA exposure information as well as clinical history and general physical examination were assessed and recorded in predesigned forms. As the second step, PFTs were carried out for all the patients by an experienced technician. Pulmonary examination as well as PFTs interpretation were carried out by an experienced pulmonologist (third author) and recorded in predesigned forms. Medical Research Council breathlessness scale was used to assess breathlessness severity in the patients, upon which the breathlessness was classified to functional classes of І–V. 27 HRCT was performed for some patients as clinically indicated.
Patients with proven systemic illnesses or any lung disease before exposure to SM and simultaneous confirmed cardiovascular or connective tissue diseases were excluded from the study. Patients who had surgery in the past 2 weeks, history of allergy, smoking or drug abuse, secondary occupational or martial SM exposure, and confirmed chemical warfare nerve agent exposure were also excluded from the study.
Blood sampling
After 12 h of fasting, 10 mL blood samples were taken from brachial vein of the patients. Blood samples were collected into sterile tubes with anticoagulant (ethylenediaminetetraacetic acid) for evaluation of hematological parameters and non-anticoagulant tubes for biochemical tests. Non-anticoagulant tubes were centrifuged at 3000 r/min for 5 min and serum samples were harvested and kept at −70°C until testing.
Complete blood count including red and white blood cell counts, hematocrit (Hct%), hemoglobin content (Hb), and platelet (Plt) count were measured with a hematology cell counter (Sysmex KX 21, Japan) in the hematology laboratory of Imam Reza hospital, Mashhad, Iran. Giemsa staining was performed for each blood smear and slides were also observed under light microscope. Liver function tests and lipid profile were measured by an auto analyzer (Abbott analyzer, Chicago, Illinois, USA) in the biochemical laboratory of Imam Reza hospital, Mashhad, Iran.
Pulmonary function tests
Spirometry was carried out for all the patients by an experienced technician, using spirometer (Spiro Lab 2, Chest Tokyo, Japan). After 15 min of resting, patients were seated with a nose clip in place and performed at least three forced expiratory maneuvers at 1-min intervals. Each patient was encouraged to give his best effort. Indices used for analysis were chosen from the one with the highest FVC. All the PFTs were analyzed by the pulmonologist. FVC of more than 80% and FEV1 of more than 75% of the predicted value were considered normal. FEV1 < 75% of the predicted value in combination with an FEV1/FVC < 70% was considered as obstructive pattern, FVC < 80% and FEV1/FVC < 70% were considered as restrictive pattern. 28 We followed criteria of American Thoracic Society during the procedure to include only valid spirometric data for final analysis. 29 Values of predicted measures were derived from the Iranian criteria. 30
High-resolution computed tomography
HRCTs were performed for some patients as clinically indicated, in radiology department of the hospital on one scanner (HiSpeed Advantage; General Electric Medical Systems, Milwaukee, Wisconsin, USA), and performed with 1.0–1.5 mm sections taken at 10-mm intervals throughout the entire thorax during both deep inspiration and full expiration, in a supine position.
HRCTs of the lungs were interpreted by a chest radiologist. Inspiratory images were read before expiratory ones. The inspiratory images were assessed for radiologic evidences of bronchiectasis. Expiratory images were assessed for the presence of air trapping.
Statistical analysis
Data on qualitative characteristics were expressed as numbers and percentage values. Data on quantitative characteristics were expressed as mean ± standard deviation.
Pearson correlation test was used to evaluate the correlation between quantitative data. The relevant statistical tests were applied using Statistical Package for Social Sciences computer software (SPSS version 16, Chicago, Illinois, USA). Statistical significant level was considered as 0.05 and the test of significance was two tailed.
Comparisons of the average laboratory tests with maximum standard levels were done by means of one-sample Student’s t-test and Wilcoxon’s test. The test of significance was one tailed for laboratory data. The analysis was carried out by Prism version 3.02 (Graph Pad software, San Diego, California, USA) for Wilcoxon’s test.
Results
General
Forty-three patients with delayed complications of SM exposure during Iran–Iraq war (1980–1988) with a mean chemical disability percentage of 47.79 ± 14.56% due to SM complications were studied. The patients were all married men with a mean age of 50.65 ± 8.24 years old. The body mass index (BMI) of the veterans varied between 19.2 and 32.4 kg/m2 with a mean of 27.17 ± 4.84 (normal <25 kg/m2). BMI of the patients was significantly over the defined normal range (p = 0.005). All the patients were exposed to single SM exposure 25.77 ± 1.49 years before the study.
All the patients had symptoms. Subjective findings were more common than objective ones. Triad of chronic cough, dyspnea, and expectoration were the most common symptoms that were recorded in 38 (88.4%), 38 (88.4%), and 28 (65.1%) patients, respectively. Twenty-one patients (48.83%) had all the symptoms of the triad. Common objective findings were generalized wheezing in 21 patients (48.8%) and crackle in 17 (39.5%) patients. Demographic data, clinical history, and physical examination data are summarized in Table 1.
Demographic data, clinical history, and physical examination data of 43 male veterans with delayed pulmonary complications of SM poisoning, Mashhad, Iran.

SM: sulfur mustard; BMI: body mass index; GI: gastrointestinal.
Pulmonary function tests
FVC of the veterans varied between 1.10 L and 5.18 L (mean of 3.16 ± 0.94 L), which were 23.50–154.20% of the predicted value (mean of 79.81 ± 25.23%). FEV1 was recorded between 0.53 L and 4.79 L (mean of 2.67 ± 0.96 L), which was between 18.70% and 177.10% of predicted value (mean of 81.85 ± 31.11%). Ratio of FEV1/FVC of the patients varied between 0.51 and 0.97 with a mean of 0.82 ± 0.11.
Abnormal respiratory patterns were observed in 23 patients (53.48%). Restrictive and mixed pattern were evaluated in 18 (41.86%) and 5 (11.62%) patients, respectively. No pure obstructive pattern was detected in the patients.
Mixed pattern significantly raised with higher chemical disability percentages among the veterans (p < 0.001). We also observed a significant reverse correlation between the chemical disability percentages of the patients and their FEV1/FVC ratio (p = 0.01, r = −0.39). Main PFT values are demonstrated in Table 2.
PFT data of 43 Iranian veterans, 25 years after exposure to SM.
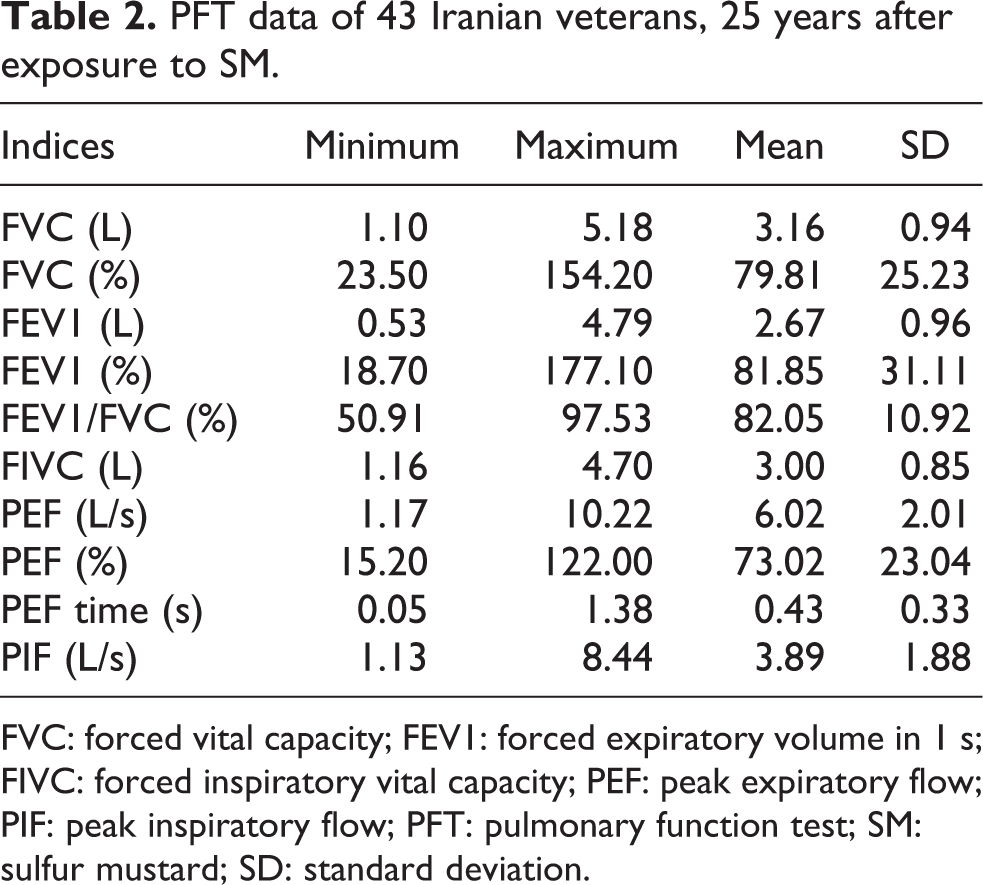
FVC: forced vital capacity; FEV1: forced expiratory volume in 1 s; FIVC: forced inspiratory vital capacity; PEF: peak expiratory flow; PIF: peak inspiratory flow; PFT: pulmonary function test; SM: sulfur mustard; SD: standard deviation.
High-resolution computed tomography
HRCT was obtained from 12 patients as clinically indicated. Nine patients (75%) had abnormal HRCT results where air trapping was the most common finding. Air trapping (score > 0) was detected in six patients (50%) in expiratory images which had heterogeneous pattern. Other common findings included bronchiectasis in three patients (25%), evidences of interstitial lung disease in three patients (25%), and ground-glass attenuation in two patients (16.66%). Scar tissue was observed in one HRCT. Homogenous mass was detected in right lung lower lobe of one patient (8.33%). We did not encounter any imaging consistent with peribronchial cuffing or large airway narrowing. There was not any significant relationship between PFTs and HRCT findings, according to the Fisher’s exact test (p > 0.05). (Figures 1 and 2)

Chest HRCT in a mustard gas-exposed case, 25 years postexposure. Diffuse cylindrical bronchiectasis is observed in lower lobes of both lungs. HRCT: high-resolution computed tomography.

Air trapping and bronchiectasis in a chest HRCT of a Mustard gas-exposed case, 25 years postexposure; consistent with bronchiolitis obliterans. HRCT: high-resolution computed tomography.
Biochemical and hematological findings
The assessment of hematological parameters did not show any significant differences with normal ranges. Among biochemical assays, the level of the lipids (cholesterol and triglyceride) was above the normal ranges but only high cholesterol level was significantly higher than normal range (p < 0.001). However, we did not find any significant changes in serum low-density lipoprotein and high-density lipoprotein cholesterol compared with normal ranges. Average cholesterol level did not show any significant correlation with neither chemical disability percentages nor BMI levels (p > 0.05). Complete data on biochemical and hematological indices of the patients are presented in Table 3.
Hematological and biochemical findings in 43 Iranian veterans with delayed pulmonary complication of SM poisoning.

SD: standard deviation; WBC: white blood cell; RBC: red blood cell; LDL: low-density lipoprotein; HDL: high-density lipoprotein; Hct: hematocrit; Hb: hemoglobin; Plt: platelet; MCH: mean corpuscular hemoglobin; MCV: mean corpuscular volume; MCHC: mean corpuscular hemoglobin concentration; MPV: mean platelet volume; SGOT: serum glutamic oxaloacetic transaminase; SGPT: serum glutamic pyruvic transaminase; LDH: lactate dehydrogenase.
aNormal ranges are according to National Health and Nutrition Survey, conducted by the National Center for Health Statistics, USA.
Discussion
The goal of this study was to determine the delayed lower respiratory complications of SM exposure in the Iranian veterans who were resident in the Khorasan Razavi province. Respiratory complications are the main cause of long-term disability among SM-exposed victims. The effects of SM on lung tissue vary according to ambient gas concentration and duration of exposure. Route of exposure, gas mask protection, wind direction, activity level of the soldier, humidity, and temperature are the other main effective factors. 7,8,31 –33 In our study, according to the document of VMAF, SM exposure was recorded in all the veterans; however, the exposed dose could not be measured during the chemical war, especially when the gas spreads through the area and the combatants remain in the field for several hours or even days. All the veterans were poisoned mainly via inhalation of mustard gas. Since the most effective route of gas absorption is by inhalation, influence of other routes of entry was considered as negligible. 34 All of the patients are still suffering from chronic respiratory complications, as the most common long-term complication of SM intoxication.
In spirometric study, restrictive pattern was the most abnormal finding that was detected in 18 patients. Mixed pattern was reported in five patients, while there was no reported pure obstructive pattern. Emad and Rezaian in a respiratory survey of 197 Iranian veterans 10 years after a heavy SM exposure stated the diversity of the effect of SM on respiratory pattern according to possible lung fibrosis over the years according to spirometric findings and lung biopsies. 17 It was previously reported that SM exposure can lead to the development of a series of chronic destructive pulmonary sequelae in such cases. 10,17,20 Nevertheless, in contrast to our results, some investigators noticed in previous studies that obstructive pattern is still the most common spirometric finding among SM-poisoned veterans. 15,35,36 In aggregate, it seems that restrictive pattern has been increased over the years and thus we observed it more than the previous researchers.
In a respiratory survey on 40 severely SM-intoxicated Iranian veterans in 2005 conducted by Hefazi and colleagues, main respiratory complications were diagnosed as chronic obstructive pulmonary disease (35%), bronchiectasis (32.5%), asthma (25%), large airway narrowing (15%), pulmonary fibrosis (7.5%), and simple chronic bronchitis (5%). The authors stated that spirometry is a valuable diagnostic tool for the evaluation of pulmonary impairment during regular follow-ups. 37 Ghanei et al. investigated the association between severity of SM exposure in Iranian veterans and late respiratory complications in three groups of mild, moderate, and severe complications. The frequency of spirometric obstructive pattern was 21% in both severe and moderate groups. It was concluded that moderate and severe exposure to SM causes an equal risk of late pulmonary complications, while mild exposure has lesser risk. 19
In our study, among 12 patients who underwent HRCT, air trapping was the most common HRCT finding (50%). Our results are in accordance with a recent study by Beheshti and colleagues. 25 In their cross-sectional study on 23 symptomatic patients with late complications of SM poisoning, air trapping (76%) and bronchiectasis (74%) were the most common findings. It was also stated in the report that in 9 lung biopsies of 14, histopathological changes were diagnosed as bronchiolitis obliterans (BO). 25 Furthermore, in an HRCT study of 50 patients with delayed SM exposure complications, air trapping (76%), bronchiectasis (74%), and mosaic parenchymal attenuation (72%) were the most frequent findings. 35 Ghanei et al. reported air trapping and tracheobronchomalacia as common delayed sequelae in SM-exposed patients and hypothesized that SM may affect both small and large airways. In their study, among 300 patients, 45.6% had various degrees of air trapping. 24 Air trapping characterized in expiratory HRCT is the most sensitive and accurate radiologic indicator for BO. 35
The toxic gas inhalation can be one cause of BO occurrence among the veterans. However, pulmonary infection (particularly viral and mycoplasmal), graft-versus-host disease following bone marrow transplantation, connective tissue disorders such as polymyositis and rheumatoid arthritis, and chronic rejection following lung or heart–lung transplantation are other possible causes. 38 –40 Two recent studies also described BO organizing pneumonia following SM exposure. 41,42 However, this diagnosis should be corroborated by histopathological studies. In aggregate, BO seems to be one of the main underlying pulmonary diseases in long-term SM exposure and depends on host response, rather than a dose–response manner. 19 Bronchiectasis was observed in 25% of HRCTs. As evidenced by a long-term follow-up study of 40 Iranian SM patients conducted by Balali-Mood, both the severity and frequency of bronchiectatic lesions tend to increase over the time. 16 Bronchiectasis usually begins bilaterally in the lower lobes and then has cephalic progression. Pulmonary hypertension and cor pulmonale were also reported in severe cases of extensive bronchiectatic lesions. 43,44
We did not find any evidence consistent with peribronchial cuffing or large airway narrowing in imagings. Airway narrowing resulted from granulation tissue and scars has been reported as a sequelae of acute injury to the trachea and large airways which occurred 2 years after exposure. 44,45 In a study of 19 SM veterans, large airway narrowing was described as tracheal stenosis in seven patients, main bronchi stenosis in eight patients, and lobar bronchi stenosis in four patients. 45 Late-onset pulmonary fibrosis has been reported in some previous SM studies 13,16,46 ; however, we did not find a clear evidence of lung fibrosis in our patients.
Bronchoalveolar lavage fluid analysis of SM-poisoned patients revealed an ongoing local inflammatory process resulting to the development of pulmonary fibrosis, years after initial exposure. 17 Diffusing capacity of the lungs can be used as an objective monitor of the degree of lung fibrosis in SM patients and also as a good predictor of prognosis. 6
It should be noted that while restrictive pattern was the most detected spirometric pattern among the veterans, air trapping was the most observed abnormality in HRCTs. Thus, some discrepancy is seen in radiographic versus spirometric findings. As air trapping has almost the same frequency as normal spirometric pattern among the veterans, thus can be attributed to the veterans with normal PFTs. Besides, high levels of drug consumption among chemical veterans due to multiple maladies could be considered for induction of fibrosis or restrictive lung disease. Drug history of the patients is illustrated in Table 1.
Two of the veterans passed away during the analysis process and article writing due to a car accident and heart attack. There was no mortality due to SM lung complications during our study.
Among hematological and biochemical assays, we observed increased levels of the lipids (cholesterol and triglyceride). Cholesterol level was significantly higher than normal range (p < 0.001). In a recent investigation by Keramati et al., 23 years after SM exposure among Iranian veterans, significant high serum levels of cholesterol, triglyceride, and gamma-glutamyl transferase activity were reported. 47
Although the first contact with SM is mostly painless, long-term complications are considerable and disturb the victims’ quality of life. The lungs, as the most affected organ, should be more considered by physicians in SM-intoxicated patients. Triad of cough, dyspnea, and sputum is still the main pulmonary symptom in delayed phase of poisoning. Most cases with delayed pulmonary complications of SM are tend to change obstructive spirometric pattern to restrictive and mixed patterns over the years. However, there should be more potent diagnostic procedures such as lung biopsies to confirm the diagnosis based on the clinical, spirometric, and HRCT results.
Spirometry is a suitable procedure for routine SM victims’ follow-ups. Yet, HRCT is imaging modality of choice in the diagnosis of SM pulmonary delayed complications. Further follow-ups with larger sample sizes are needed for assessment of the delayed SM complications on pulmonary system.
It should be noted that financial gaining (malingering) of the veterans could be a confounding variable due to their specified salary from the VMAF based on their disability percentages. There was some other limitations in the study. The current research was performed in the absence of a matched control group. Based on ethical consideration, lung HRCT was performed in only 12 patients from a total of 43, as clinically indicated. Further case–control and histological studies could be done with a matched control group of nonchemical Iranian veterans with larger case groups in order to shed light on diversity of progressive long-term pattern of lung involvement in SM-intoxicated patients.
Footnotes
Acknowledgements
The authors would like to thank all the chemical veterans for their patience and kind cooperation with this research projects of Medical Toxicology Research Center of Mashhad University of Medical Sciences that resulted to this article. The authors would also like to thank the Khorasan VMAF for coordination with the patients.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors gratefully acknowledge the financial support of the vice president for research of Mashhad University of Medical Sciences.