
Abstract
Theoretical approaches have tended to understand perinatal distress through either individual or socio-cultural factors. In contrast, Natasha Mauthner proposed a relational model that understands perinatal distress in the context of interpersonal relationships. This study aims to build on Mauthner's work to explore how women speak about their relationships in connection to their stories of perinatal distress and recovery. Eight women were interviewed for the study. All women had at least one child under the age of three and self-identified as having experienced distress in the perinatal period. Interviews were recorded, transcribed and analyzed using Voice Centred Relational Analysis. Four broad themes were identified: (i) the role of practical support, (ii) the role of emotional support, (iii) relational dynamics, and (iv) the role of socio-cultural norms. Whilst some women experienced practical and emotional support in their relationships, those who did not linked a lack of support to their feelings of distress. Relationships were also found to reinforce unhelpful social norms around motherhood and mental health, as well as offering a space to resist norms and create wider discourses about what it means to be a mother. This study suggests that organizations supporting women in the perinatal period should focus on women's relational needs and consider the cultural discourses of motherhood that they perpetuate.
Perinatal mental health is a term used to describe difficulties experienced during pregnancy and in the year after birth which are thought to affect around 10–20% of women in the UK (Russell, 2017). The majority of research in this area has looked at perinatal mental health through the medical model of disease, exploring the links between symptom presentation and biopsychosocial risk factors (Abdollahi et al., 2016; Beck, 2002). Arising out of Western European philosophy, psychological theory and research has traditionally focused on the individual, emphasizing the importance of autonomy, independence and self-determination in psychological wellbeing (Mauthner, 1998). This approach has prioritized a focus on risk factors associated with perinatal distress, such as genetic predisposition, history of mental health difficulties, personality traits and relational stress (Leigh & Milgrom, 2008; Silverman et al., 2017), and has been criticized for failing to recognize the lived experience of women (Oakley, 1980).
In response to this, the feminist approach to perinatal distress has traditionally drawn on principles of social constructionism (Burr, 1995; Foucault, 1982), focusing on how constructs of femininity and motherhood place pressure on women in the perinatal period, leading to unrealistic expectations about what it means to become a mother (Douglas & Michaels, 2004; Jebali, 1993). Feminist researchers have argued that if women struggle with these expectations, they are often pathologized and given labels such as “postnatal depression” which fail to recognize the socio-cultural factors shaping their experience (Jebali, 1993; Ussher, 2004). To avoid problematic psychiatric labels, this paper will use the term “perinatal distress” to describe women's experience of psychological difficulties in the perinatal period.
The feminist approach has, however, also been critiqued for framing perinatal distress as a normative response to motherhood, failing to explain why the majority of women do not become depressed following childbirth (Mauthner, 1998). By primarily focusing on factors impacting women at a societal level, these approaches have struggled to account for the ways in which individual women experience and make meaning of the changes that occur with the transition to motherhood, and failed to recognize the agency that women have in constructing their own narratives of motherhood (Mauthner, 1998).
In seeking to strike a balance between these two positions, Mauthner proposed a relational theory of postnatal depression, developed from in-depth interviews with 18 mothers who had experienced distress in the perinatal period (Mauthner, 1994, 1998, 2010). Following research from Gilligan and Brown, which explored how women and girls spoke about themselves in the context of their relationships (Brown & Gilligan, 1991), Mauthner explored how women who had experienced perinatal distress understood themselves and their depression in the context of their relationships. By looking at perinatal distress through Gilligan and Brown's methodology of Voice Centred Relational Analysis (VCRA), Mauthner understood it as a phenomenon that exists within the relationships people have, rather than residing within an individual person. The VCRA methodology also enables an exploration of how socio-cultural norms are enforced and resisted through relationships (Brown & Gilligan, 1991).
Since Mauthner, researchers have continued to explore relationships in the context of perinatal distress, but few have used this as an explicit theoretical approach. Quantitative studies have found an association between relational risk factors, such as marital discord and low social support, and perinatal distress (Kruse et al., 2014; Milgrom et al., 2019), whilst qualitative research has explored how relational difficulties and lack of social support were understood by women as contributing to their distress (Jackson et al., 2020; Recto & Champion, 2020). Whilst research has explored how women relate to cultural norms around motherhood, child-rearing practices and mental health (Gardner et al., 2014; Jones et al., 2014), these studies have rarely explored how relationships can reinforce socio-cultural norms. For these reasons, Mauthner's work remains relatively unique in its approach.
It has now been almost 30 years since Mauthner conducted her interviews. Since then, cultural expectations around both motherhood and mental health have changed significantly in the UK. Inclusive parenting policies have been introduced within the past 20 years (Women & Equalities Committee, 2018), and evidence suggests that fathers are increasingly taking a role in caring for children (Chung, 2021). Furthermore, a wider range of narratives regarding what it means to be a mother are available in the UK today (Heffernan & Wilgus, 2018), perhaps making it easier for women to find their own approach to parenting. However, a culture of “intensive mothering” is also increasingly prevalent, especially among middle-class parents, where pressure is placed on mothers to parent “perfectly”, which may result in greater stress in the perinatal period (Meeussen & VanLaar, 2018). Since Mauthner's work, there has also been a positive shift in public attitudes towards mental health difficulties (Henderson et al., 2020), and greater public awareness of maternal mental health (MMHA, 2021; Theroux, 2019), which may make it easier for women to be open about difficulties in the perinatal period.
Furthermore, whilst Mauthner's work considers how the general culture of mothering in both the UK and the USA may impact women in the perinatal period (Mauthner, 1994, 2002), less attention is given to how mothers’ specific cultural context might shape their social networks and thereby determine the social norms to which they are exposed.
This study aims to build on Mauthner's research exploring women's experiences of perinatal distress through a relational lens from the perspectives of mothers in the UK in early 2020. We sought to (i) explore how women speak about their relationships in connection with their stories of perinatal distress and recovery, and (ii) explore how cultural norms regarding mental health and motherhood are reinforced and resisted through women's relationships.
Method
This study situates itself within a body of feminist research that recognizes how traditional, epistemological claims of “objectivity” within research have often marginalized the voices of women and minoritized groups by framing the male voice as omnipotent (Smith, 1991). This study broadly takes a feminist social constructionism approach to epistemology, arguing that researchers and their social locations play an inextricable part in knowledge construction (Burr, 1995; Wigginton & Lafrance, 2019). Ontologically, this research seeks to understand participants’ experiences by examining their narrated selves, as this offers a way to explore subjective experience through the stories people construct about their social identities (Doucet & Mauthner, 2008). It has been argued that drawing on a narrative understanding of the self is intrinsically relational, as the stories we tell about ourselves are grounded in our interactions with others (Stanley, 1993). Rather than search for an intentional self beneath a narrated account, researchers attempt to make sense of a participant's story in a wider network of social discourse within which both participant and researcher are situated (Doucet & Mauthner, 2008). This highlights the importance of researchers being reflexive throughout the process of analysis and recognizing their own subjectivity in understanding their participants’ narrative accounts (Mauthner & Doucet, 2012).
This research seeks to listen to the “narrated selves” of participants, facilitating an exploration of how the women interviewed told stories about themselves and their relationships with others. For this reason, a decision was made to use VCRA, an approach developed to explore subjective experience by listening to individuals’ narratives and attending to the socio-cultural position in which these narratives are being told (Doucet & Mauthner, 2008).
Recruitment
After receiving ethical approval from the university ethics committee, the first author contacted co-ordinators of several perinatal community support groups in Greater London. Two group facilitators responded and contacted group participants with the information leaflet and recruitment poster, providing an email address to contact if women wanted to participate. Women were eligible to participate if they were over 18, had at least one child under three and self-identified as experiencing distress during their pregnancy or in the year after their baby was born.
Participants
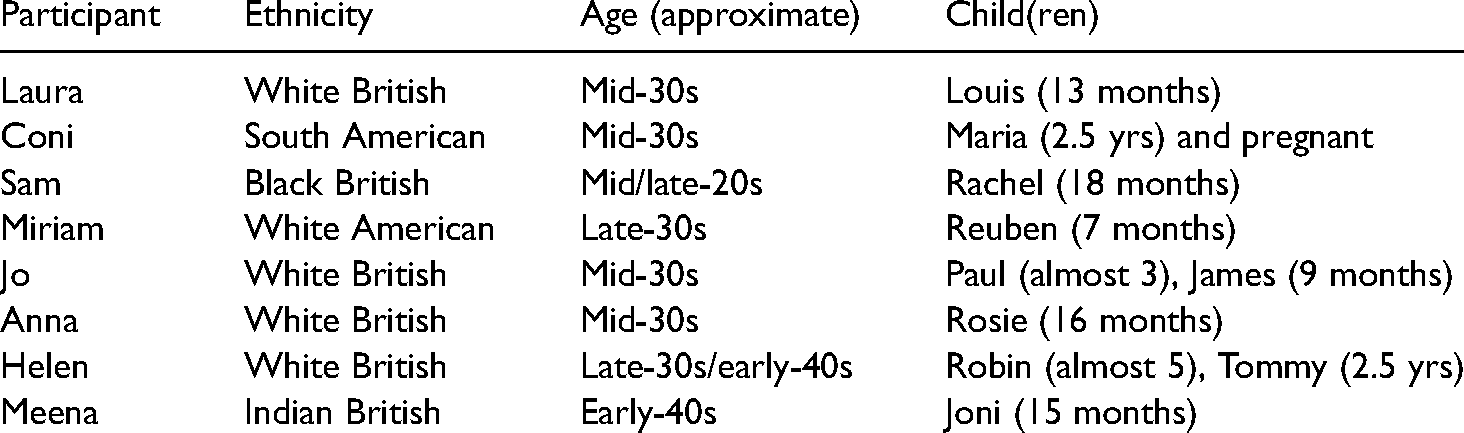
In total, eight women responded to the advert, and all were eligible to participate. Table 1 gives some basic demographic information about the sample. All women were cis-gendered and were living with their children's fathers at the time of the interview; five of the couples were married. Pseudonyms were given throughout the analytic process to protect the confidentiality of participants, their children and anyone else mentioned in the interview.
Participant demographic information.
Data collection
The first author met the women who agreed to participate and obtained written informed consent prior to conducting face-to-face interviews. This was based on an interview schedule which was developed with a support group facilitator who had lived experience of perinatal distress. All interviews took place in women's homes. The interviews explored mothers’ experiences during their pregnancy and birth, to whom they spoke about their experiences and how their experience of perinatal distress impacted their relationships. The participants were all given a voucher to honour their time.
The durations of the interviews varied (range: 50–103 minutes, median 69 minutes). All interviews were audio recorded and transcribed by the first author.
A voice centred relational method of data analysis
The data were analyzed using VCRA (Brown & Gilligan, 1991, 1993). This analysis involves reading the text four times to identify the answers to four questions: (i) who is speaking?; (ii) in what voice?; (iii) telling what story about relationships?; (iv) in what socio-cultural frameworks? (Mauthner, 1994).
Coloured pencils were used to track the four readings on each transcript and worksheets were used which documented relevant extracts of text identified in each reading, along with the first author's responses, in order to highlight the move from the narrator's actual words to the reader's interpretation (Mauthner, 1994). Following Mauthner's methodology (1994), extracts in the worksheets that looked at relationships with partners, family members, friends and other mothers were identified, which primarily involved focusing on the third and fourth readings. The author's responses to these extracts were compiled across the eight interviews and interpretative codes were generated for each extract.
Informed by the research questions, reading the wider literature and the author's ontological position, preliminary themes were generated by looking for similarities between interpretive codes, starting with the extracts where women spoke about their relationship with their partners. These preliminary themes were then used to analyze extracts where women spoke about their other relationships, including relationships with their mothers, other family members, in-laws, friends and other mothers. Themes were adjusted to capture the additional data and broadened to provide a holistic overview of the data.
Initial themes were shared with the second and third authors who provided feedback. The worksheets and some parts of the original transcripts were reread to understand what was captured with these themes and ensure that the final themes were sufficient to address the research questions.
Trustworthiness and reflexivity
VCRA allows data to be looked at across interview transcripts, I-poems, and worksheets as well at the thematic level, and its precise methodology is argued to enhance trustworthiness of the findings (Mauthner & Doucet, 2012). An audit trail including the worksheets and notes produced by the first author was audited by the second and third authors to further enhance credibility of the findings.
In keeping with the social constructionist epistemology, the lead author considered how her own socio-cultural position as a white, Ashkenazi, middle-class woman without children, as well as her personal experience of growing up with a working mother, would impact her interpretation of the data (Lafrance & Wigginton, 2019). Reflexive notes were kept throughout the analytic process, and these were discussed with the second and third authors throughout the process of transcription and analysis.
Findings
Four broad themes were identified from the interviews (i) “my dad only came once”: the role of practical support, (ii) “I’m not fine, no one's listening”: the role of emotional support, (iii) “he's never really been able to support me”: relational dynamics, (iv) “the standard subjects you can talk about … and the ones you don’t”: the role of socio-cultural norms. Each theme was explored in terms of the role it played in women's experience, both of perinatal distress and recovery from distress.
“My dad only came once”: The role of practical support
Research has highlighted how women cited a lack of practical support as central to their experience of distress in the perinatal period (Gardner et al., 2014; Jackson et al., 2020). This theme was also identified in this study, where several women spoke about how the failure of friends and family to provide practical support was central to their experience of distress. For example, one participant, Sam, was impacted by what she described as an “incompetent cervix”, which largely confined her to bedrest throughout her pregnancy. In this context, she reflected on how her family's failure to provide her with practical support impacted her.
My dad only came up to visit me once. They, they live in London, and I was lying on this chair, and my dad only came once … family members kept messaging me, it's like I actually could do with practical h-, like if someone could come around and like help … quite a lot of people said they’d come and then didn’t. So that stopped me from even asking for help anymore … it was hard.
In this extract, Sam highlights the gap between what her family said they would do and what she remembers them doing for her. This circular process highlights the interconnectedness of distress and lack of practical support, showing how Sam's experience of being let down stopped her from “even asking for help anymore”, increasing her sense of isolation and disconnect from her family during her time of need.
Another woman, Helen, spoke about how she felt incredibly overwhelmed, trying to look after two young children, and felt like her mother was not there for her.
[My mother] just was never here. And I just felt so alone. And her solution was like, well you need to get some home help in or something like an au pair or something. She said, “I’ll pay for it. I’ll pay for you to have a nanny.” And I said, “I don’t want a nanny. I don’t want someone else coming. I want you to help me, you’re family … I don’t want some stranger coming in … I just want you to be there” … I could just tell she just wasn’t interested and that made me feel really down.
This quote highlights how Helen's mother's “solution” of employing a nanny seemed unacceptable for Helen, and whilst she needed practical help, it was important that this came from her family. For Helen, her mother's failure in this regard contributed to her feeling “really down”. This links with Mauthner's research, which found that practical help, especially from women's mothers, held an emotional significance, and when this was unavailable women felt unsupported (Mauthner, 1994).
Women often spoke about the importance of receiving practical support as being crucial to their recovery from distress, as demonstrated in the following extract: My sister was a key figure as well too. Because when, when Maria was born, she was working in shifts, in a hotel. And luckily, she was like there to support me … So, she’ll be the one coming home and saying, okay, let's get out and what you need and this and that. Or just listening to me.
Coni referred to the fact her sister was physically there for her, making her a “key figure”; this involved not only offering her practical support but also providing her with an opportunity to feel listened to. This further supports the idea that practical support signifies emotional care, which plays a role in women's recovery.
Another participant, Jo, compared her experience with her first child, where her parents were living abroad, to her experience with her second child, when they were based more locally.
It's been it's been a big adjustment with [my parents] moving back [to the UK] this time. They were back two months before James was born … And it has made a big difference with coping and having James and having the extra pair of hands and all the practical support.
This quote highlights how, for Jo, ideas of “coping” are linked to the “extra pair of hands” provided by her parents. Jo never disclosed to her parents the emotional difficulties she experienced following the birth of her children; however, for her, the practical support alone helped her feel more able to “cope” with her second child.
“I’m not fine, no one's listening”: The role of emotional support
Emotional support has also been cited as crucial for mothers with experience of perinatal distress (Rodrigues et al., 2003). Whilst this may be shown through practical support, the women interviewed also spoke explicitly about the need for others to connect with their emotional experiences during the perinatal period.
The men in my family and [partner], were … trying to go, “well, what do we do to fix it?” It's like you can’t really just fix it. Well, you can support someone to recover and heal, but that's a long process with multi-faceted interventions. You can’t just go “ahh God let's just fix it”.
In this extract, Anna reflects on a gendered story of how her partner and the male members of her family wanted to focus on how to “fix” her distress rather than giving her space to explore her emotional wellbeing. This gender-difference has been reflected in the literature, where women have often spoken about partners offering practical rather than emotional support (Aiken & George, 2000; Mauthner, 2010). Anna later spoke about how this left her feeling unsupported and unheard, contributing to relational difficulties with her partner.
Other participants, including Sam, spoke about how they sought emotional support, but these conversations were shut down: The whole pregnancy was pretty traumatic. And all through it, people were kind of like, “you’ll be fine, it’ll be fine”. And I was like, no, I really want to talk about it … And people kind of dismissed it. And even like after she was born it's like, I wanted to talk about the birth and stuff. And people, other people were like “oh she's here now, you’re fine. She's here, she's fine, she's healthy”. But it's like, I’m not fine, no one's listening to me.
In this quote, Sam talks about how others’ insistence that things would “be fine” did not leave her any space to talk about her experiences, including a traumatic birth. This contrast between the baby being “fine” and Sam's experience of being “not fine” contributed to a narrative where the wellbeing of her baby was seen as primary, pushing Sam's needs to one side.
When emotional support was available, the women interviewed spoke about the key role this played in their recovery, as Meena discussed in the following extract: I felt [these friends] were my side. Um, and they really listened to me and they offered a lot of love and kindness and understanding. And one of them has had children and one hasn’t, but I think what was really helpful … was they knew me.
For Meena, having friends who showed “love”, “kindness” and “understanding” was a huge source of support. She differentiated them from her family and partner, who struggled to understand her experience and give her the support she needed. Meena spoke about the importance of having friends who “knew me”, and this was something that came up from several women interviewed. Many spoke about the importance of spending time with people who knew them before they were mothers, who helped them connect with the person they had been before they had had a child. Given how perinatal distress has often been thought about in terms of how motherhood challenges one’s identity and sense of self (Blum, 2007; Everingham et al., 2006), it follows that emotional support may be most beneficial when it bridges the gap between an old and new identity.
“He's never really been able to support me”: Relational dynamics
Relational difficulties:
It was notable that many of the women interviewed spoke about long-standing relational difficulties, both with their families and their partners. Whilst this links to literature exploring relational discord as a risk factor for perinatal distress (Kruse et al., 2014; Milgrom et al., 2019), these interviews highlighted how these dynamics played out within the perinatal period.
For example, Meena spoke about how her partner had always struggled to understand her mental health, but that took on a different meaning after she had a child. This seemed to have been exacerbated by the couple relocating during her pregnancy, leaving her feeling isolated from other sources of support.
My relationship with my partner was just really terrible … Um, he he's never really been able to support me in a way that I felt I’ve needed with any kind of mental health issues … he's not been able to really help in a way that I needed.
In this extract, Meena draws on absolute language, describing her relationship with her partner as “terrible” and stating he has “never” been able to support her; this paints a more complex picture of the interrelationship between her own mental wellbeing and her relationship with her partner.
Similar accounts of relational difficulties were found throughout the data, with Anna noting “I didn’t grow up in a family which supported, kind of, self-worth and developing self-esteem” and Jo commenting “With my parents, there's kind of a lot of deep-rooted kind of background … I’m not that close to them … I’ve never talked about emotions”, suggesting these difficulties were present for several women and came to the forefront in the perinatal period, contributing to their experience of distress as they transitioned into motherhood.
Relational change:
Mauthner explored how women's journey out of postnatal depression often involved changes in their understandings of their relationship, facilitated by them feeling more able to be open with others (Mauthner, 1994). This was also identified within the current study and, for some women, these changes seemed to be an important part of their recovery from perinatal distress, as Coni comments: I think in general with my family, I’ve always been like the organized one, the strong one, who has been in a long-term relationship … And showing myself weak to my family, was a [turning] point. … I feel like with all this, again I could show weak, I could show like I’ve got failures, I’m not perfect. Because I always have so much perfectionism that I want to get rid of. But it was good, I think, to have this. It was like, I don’t know, a rebooting system, it was like a clean-up of many things.
For Coni, her experience with perinatal distress changed the relational dynamics within her family, allowing her to show “weak[ness]” and “reboot” their relationships. In feeling able to voice the part of her that was struggling, Coni allowed her family to give her the support she needed. This challenged Coni's expectation that she needed to be “the strong one” to be accepted in her family.
Whilst many women spoke about how their experience of recovery resulted in positive changes to their relationships, others, including Sam, found that it caused additional difficulties.
I’m trying to deal with [postnatal depression]. I’ve had like therapy, I’m going to try to get some more, I’m going to the support group, I’m on antidepressants now, that helps a lot. [My partner], I don’t think he's dealt with it … He's had bereavements in his past, and I think, for him now things are kind of coming up. And he's not really himself … Our relationship's a bit like rocky now because he's like really not okay, but he won’t address it or get help.
Sam speaks about trying to “deal with” her postnatal depression and lists the tools that she has used to facilitate her recovery. Whilst she talks about how her partner has also had a difficult experience, she expressed frustration that “he won’t … get help”, and this is putting pressure on their relationship. For Sam, and two other women interviewed, it seems like their experience of perinatal distress and recovery changed them, and their partners’ failure to change with them posed a further challenge.
“The standard subjects you can talk about and … the ones you don’t”: The role of socio-cultural norms
Reinforcing socio-cultural norms:
The feminist literature on perinatal mental health highlights how socio-cultural context places unrealistic expectations on mothers, which can contribute to perinatal distress if women fail to meet these expectations (Jebali, 1993; Mauthner, 1993). For this group of women, relationships seemed to play a role in reinforcing socio-cultural norms, as exemplified in the extract below: I could hear my mum saying to my sister on the phone: “It's not normal. She's not talking to her … she's not talking to [the baby].” Cos … I didn’t do that kind of baby chit chat thing with her until she was older. And I could hear my mum saying to my sister, “I am worried. It's not normal.” And I remember hearing her say that and thinking, “oh, great, even my family are giving up on me”.
In this quote, Anna reflects on how her own mother reinforced ideas of what is “normal” in parenting which served to make Anna feel her family were “giving up” on her for not conforming to their expectations of what it means to be a mother, contributing to her distress.
As well as norms relating to motherhood, women spoke about changing norms regarding mental health. For example, Meena, of British-Asian heritage, reflected how cultural expectations from different parts of her family contributed to her distress: I had Joni out of wedlock, which was a real problem for my mum. And so, first trimester we weren’t talking. [My partner's] the kind of “pull up your socks, what's wrong with you? Just get on with it” type of attitude. Umm, “why won’t you be more positive?”… White-British um, reserve, stiff upper lip attitude.
These two quotations from Meena highlight the different cultural pressures she experienced from her South-Asian family and her white-British partner. Cultural expectations around motherhood and marriage caused difficulties in Meena's relationship with her mother during her pregnancy, whilst the “stiff upper lip” Britishness reinforced by her partner made it hard for her to turn to him for support. This sense of being stuck between competing cultural norms, neither of which made space for Meena's experience, were important in her narrative of perinatal distress.
Whilst family members played a significant role in reinforcing cultural norms, other mothers set out arguably more restrictive rules regarding acceptable discourses of motherhood, as exemplified in the two extracts below.
There are like the standard subjects you can talk about and complain and the ones you don’t. So like there's the sleep and the feed, feeding and baby crying and colic. These are fine to complain with NCT [National Childbirth Trust] group and they’re like a standard mum thing. But nobody is allowed to say resentfulness, angry, or loss of freedom or how your life changes.
And everywhere you look, you just feel like there's mums that are doing everything right and not feeling the way that you’re feeling basically … like mother and baby groups and NCT groups and classes and things actually can just make you feel really shit about yourself.
These extracts show how both the language and actions of other mothers can implicitly and explicitly shape social norms and expectations around motherhood. Coni recognizes the “standard subjects” that she can talk about, highlighting how she felt the discourse within spaces for new mothers was restricted. This limited her ability to be honest about her own experience of “angry” and “loss of freedom”. For Laura, being around new mothers triggered a sense of anxiety that they were doing “everything right”, which, by implication, made her feel like she was doing everything wrong. These women's experiences demonstrate how relationships with other mothers may reinforce broader societal norms and expectations around what it means to be a “good mother”, which can feel stifling to those whose experiences do not fit with the mainstream (Heffernan & Wilgus, 2018; Jones et al., 2014).
Whilst many mothers referred to how social norms impacted them negatively, two of the mothers from non-British cultural backgrounds spoke about how differing cultural norms allowed them to be more open about their experience of perinatal distress.
It's very common in [South America] to be open to mental health and, well, I dunno if that's the way of saying it. But at least people do go to therapy quite often and it's not such a shame or something so that people are not so, so closed to this.
Coni spoke about how her country of origin had a more open attitude towards mental health. For Coni, this helped her “to be open”, without feeling “shame”. In other parts of her interview Coni spoke about how being the “Latin one” made it feel easier to share her feelings with other mothers and try to model a different cultural approach to mental health.
Resisting socio-cultural norms:
Nearly all the women spoke about the importance of attending a support group as part of their recovery. The extracts below demonstrate how the group enabled women to expand the discourse around motherhood and tell stories which were more authentic to their lived experiences.
And I went [to the support group] and there were girls there who were like, severely anxious and like, saying things like, honestly that I’ve never heard people say. And it's like, oh finally, people being honest.
Talking to other mums about that experience was a massive, massive lifeline … Saying, “What have I done? I wish I’d never have a child. I’ve made the biggest mistake of my life. I’ve ruined my life. I don’t wanna be here.” Lots of the same sentences I’d said those words beforehand, and others were saying them -- just totally non-judgmental.
Sam reflects on how, in the support group, she heard things she had “never heard people say”; this led to a feeling of relief that this meant people were being “honest”. This suggests that in other settings Sam feels people have not been honest about their experience of motherhood and have instead capitulated to social pressure to say what is expected. For Anna, she hears her own struggles reflected in the “words” of other mothers, again highlighting the importance of hearing an alternative discourse. This offers her a “lifeline” and begins her journey of accepting her own experience. Whilst theories of perinatal distress often highlight the limited norms and social expectations surrounding motherhood (Jebali, 1993), these women have started to create their own narratives which leave space for ambivalence and disappointment.
Summary and further discussion
This study aimed to build on research by Mauthner (1994, 1998, 2010), using VCRA to explore how women speak about their relationships in connection to their stories of perinatal distress and recovery. Whilst Mauthner's (1998) work emphasized how women struggled to speak about their feelings of distress within their personal relationships which led to them silencing their voices, our study found that many of the women interviewed did voice their experiences, but the people around them did not always know how to respond and support them. This may reflect changes in understanding around motherhood and mental health that have taken place over the past 30 years (Heffernan & Wilgus, 2018; Time to Change, 2020), where a new generation of mothers, in certain contexts, feel more able to voice their distress. However, the experience of speaking out and not being listened to felt particularly challenging for some women, as it not only invalidated their experience of distress, but also reinforced tensions in their interpersonal relationships, especially when partners or family members reflected unhelpful norms around mental health and coping.
On the other hand, when friends and family were supportive and understanding, this was seen as a “lifeline” for women. Like in Mauthner's (1994) study, some participants spoke about how experiencing support from others changed their relationships, leaving them feeling closer to friends and family members. This suggests a circular relationship between women's recovery and the strengthening of their relationships, which may protect them against future experiences of distress.
Like Mauthner (1994, 1995), this study found that relationships with other mothers played an important role in women's narratives of perinatal distress, particularly the ways in which other mothers reinforced socio-cultural norms around motherhood. Whilst Mauthner (1995) found that mothers experiencing perinatal distress often felt isolated from other mothers, this was not true for most women in this study. However, those who did spend time with other mothers often felt different and out of place, suggesting these groups have not changed significantly over the past 30 years. Through its explicit emphasis on contextualized stories, VCRA allowed the authors to notice how these groups facilitated a limited discourse around motherhood which did not allow room for distress or ambivalence. Several women in this study noted how these groups were organized around a “motherhood” identity without catering to other aspects of identity, reducing women to mothers with little else in common.
This was not true for all women, and where these groups were perceived as supportive, they seemed to play an important part in women's recovery; for example, Anna spoke about how her NCT group was “debunking … the mumspiracy”, enabling a franker discussion about what it means to be a mother. Furthermore, whilst most women in the study did access therapy or medication, it was notable how many of them saw attending a peer support group as crucial to their recovery. Whilst research has evidenced the effectiveness of peer support groups (McLeish & Redshaw, 2017; Moran, 2020), this study suggests that these groups might help to broaden an acceptable discourse around motherhood, allowing women to tell their stories without judgement and facilitating acceptance of their own experiences.
In designing this study, we hoped to recruit a more diverse sample than Mauthner's (1994) original sample, which consisted of only white women, and our final sample included three women from minoritized groups, as well as one woman from the USA. We found these women tended to talk about how British cultural norms around mental health limited their ability to speak about their experiences, whilst their own cultures were more emotionally open. Whilst this is likely to relate to the sample that was recruited, it serves as a reminder to researchers to consider the unhelpful norms of the dominant culture as well as norms in minoritized groups (Nolte, 2007).
Practice implications and future directions for research
Whilst there is increasing awareness of mental health difficulties in the perinatal period and additional funding to support women at this time (NHS, 2019), these difficulties are still typically framed in terms of individual pathology, leading to a focus on individual solutions, in terms of diagnosis, one-to-one therapy and medication (Lloyd et al., 2003). Although this study is only based on a small sample of women, the challenge it poses to the medical model of perinatal distress suggests that perhaps interpersonal relationships and socio-cultural context may be a more helpful way of understanding women's experience of distress in the perinatal period.
Framing perinatal distress within a relational context may indicate that family therapy could be of benefit; this is supported by evidence from a recent meta-analysis indicating family therapy may be beneficial for women experiencing perinatal depression and may lead to improvements in family functioning (Cluxton-Keller & Bruce, 2018). Whilst there is a growing acknowledgement of the need for partner-inclusive interventions when supporting women with perinatal distress (Alves et al., 2018), these findings might suggest that including other family members, especially women's own mothers, may be beneficial, though further research is needed to explore this.
This study also demonstrated the benefits of attending a peer support group; most research investigating the benefits of peer support in the perinatal period have looked at one-to-one support (Moran, 2020), though there is some research exploring the benefits of group support (Mauthner, 2002; Montgomery et al., 2012). This study suggests that attending a support group may help to broaden the acceptable discourse around motherhood, leaving women feeling less alone in their experiences. However, much more research is needed in this area, including further exploration of why women might not want to attend a support group (Mauthner, 2002).
This study also points to the challenges created by a cultural discourse which assumes that having a baby is a joyful occasion and still sees motherhood as a natural role for women. Whilst in recent years the discourse around motherhood has been evolving (Heffernan & Wilgus, 2018), it seems like groups for new mothers, including NCT groups, may still perpetuate traditional ideas around motherhood. It could be beneficial for organizations like the National Childbirth Trust to think more carefully about the messages being given to parents and how this might feel for those who have a more challenging transition to motherhood.
Limitations
The study only involved a small sample of women who were all involved in a peer support group. Therefore, this sample may differ from one with mothers who had not engaged with peer support, particularly in their views around the importance of relationships. Furthermore, whilst the sample was diverse in ethnicity and age, all women lived with their child(ren)'s father and most were middle class and highly educated. These characteristics may have influenced participants’ experiences of relating to others and their relationships with other mothers. Future research should seek to explore the experiences of single mothers whose relationships are likely to be significantly different, as well as having a greater focus on working class-mothers.
Member checking is a useful way to both improve trustworthiness of findings and go some way to address power inequalities inherent in research (Caretta, 2016; Korstjens & Moser, 2018). Although the study design benefited from the input of a peer support coordinator with lived experience of perinatal distress, it would have been useful to draw on the expertise of those with lived experience throughout the process of analysis and interpretation.
Conclusions
This study has explored women's experience of perinatal distress from a relational framework, looking at how women speak about their relationships in connection to their stories of perinatal distress and recovery. This study has extended previous work by Mauthner (1994) and used VCRA to consider how changing socio-cultural norms around motherhood and mental health impact women today. Whilst many women found important sources of practical and emotional support in their relationships, a lack of support from close relatives, particularly their own mothers, was understood as contributing to feelings of distress. This study also highlighted how relationships, particularly with other mothers, could both reinforce unhelpful social norms around motherhood and offer a space to resist norms and create broader discourses about what it means to be a mother in the 21st century.
Footnotes
Acknowledgements
The authors would like to thank the peer support group facilitators who helped recruit participants for this study, and in particular Liz, who contributed to our thinking in developing this research project. We would also like to thank our participants who so generously shared their time and their stories. Their resilience and strength in the face of huge challenges have stayed with us and we are extremely grateful for their participation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.