
Abstract
The UK National Health Service (NHS) is one of the largest employers in the world and relies heavily on Black migrant women. Nonetheless, reports of (gendered) racism persist. This phenomenologically inspired qualitative study shares findings from empirical interview data with female Nigerian doctors and nurses working in the NHS, with a specific focus on how these women cope with the racism and gendered racism they experience in their everyday working lives. The analysis shows the extent to which they perceive the coping strategies available to them to be limited, with problem-based solutions focused on relocating themselves into geographical, professional, or organisational spaces where acute staffing shortages may curb employers’ tendency towards discrimination in recruitment and advancement. Emotion-based strategies employed were often faith-based, or relied on their national identity and understandings of what it means to be Nigerian/a Nigerian woman. The article critically considers the power differentials endemic in employment that limit these women to individualised coping strategies which ultimately result in their isolation, a known stressor itself, creating a self-perpetuating vicious circle of gendered racism.
Racism is a chronic stressor with negative physical and psychological health outcomes (Brondolo et al., 2009; Lewis et al., 2017), and there is a gendered dimension to it, with Black women experiencing a double burden of intersecting racism and sexism (Melaku, 2019; Spates et al., 2020). Yet, little is known about how Black women make sense of gendered racism, what coping mechanisms they employ, or how efficacious these strategies might be. This is particularly the case in relation to gendered racism experienced in the employment sphere, which is difficult to evade in one's everyday life. To address this gap, we report a qualitative analysis examining the coping strategies mobilised by migrant Nigerian female doctors and nurses working in the UK National Health Service (NHS), identifying and critically evaluating the strategies these participants developed to cope with the racism they perceived in their roles.
The NHS is the fifth largest employer in the world, employing 1.3 million full-time equivalent staff (Government UK, 2023), and relies on female healthcare migrants in particular to address an acute and growing staffing shortage (Adepoju, 2008; Brown, 2019). In 2018, over half of doctors joining the medical register were trained abroad (Brown, 2019), and Nigerians are one of the largest groupings (NHS England, 2022b). Yet, despite a diverse workforce and embedded equality, diversity, and inclusion (EDI) policies, the NHS continues to be structured by inequalities (Atewologun et al., 2019; Edeh et al., 2022; Healy & Oikelome, 2007, 2011; Healy et al., 2011; Joseph, 1995; Oikelome & Healy, 2013, 2007). Black Asian and minority ethnic (BAME) applicants are 3 times less likely to be appointed to a hospital job than White applicants (Jaques, 2013), are less likely to receive performance-related bonuses and opportunities to progress in their careers, and are significantly more likely to experience harassment from patients, colleagues, and managers (Jaques, 2013; Pudney & Shields, 2000). BAME doctors are also at higher risk of litigation and referral to the General Medical Council (GMC; Atewologun et al., 2019, 2022), with migration background further complicating disadvantage and risk. Inequalities based on sex are also evident: women make up 77% of NHS staff (NHS England, 2018), with 46% of doctors and 89% of nurses and health visitors being female (Balabanova, 2018); yet only 37% of all senior roles are held by women, and only 35% of consultants are women compared to over half of general practitioners (GPs; 53%; NHS England, 2018). Among nurses, senior leadership positions are mostly held by women, but a perception persists that men are favoured for promotion (Lauder, 2019). Edeh et al. (2022) show how female migrant professionals from Nigeria perceive racism and gendered racism to occur in encounters with colleagues, superiors, patients, and even law enforcement, and note the significance of professional status in understanding gendered and racialised identities at work. Within these broad patterns, research highlights intersectional effects that occur across multiple positionalities related to race, sex, and migrant and professional status, yet how female migrant professionals in the NHS cope with gendered racism is less understood despite evidence of its persistence and the NHS’s heavy reliance on female migrant staff.
Coping theories of stress and racism
A robust framework for understanding stress-related coping strategies is Lazarus and Folkman's (1984) psychological stress and coping theory, which distinguishes between two stress-related coping strategies: problem-focused strategies occur when people attempt to reduce stress by directly targeting the situation/problem, and emotion-based strategies are employed when people consider that the problem cannot be changed and so attempt to change their response to it, with the aim of reducing the intensity of negative emotions caused by the (inescapable) stress. Both can be useful, depending on the context, although emotion-based ones are more likely to be avoidant, thus leaving the stressor unchanged (Biggs et al., 2017).
Central to Lazarus and Folkman's theory are individuals’ interpretations of their stresses, because coping is understood as a process occurring between a person and their environment. This involves individuals appraising situations as harmful/beneficial and threatening/challenging, and assessing what resources they have to respond to the stressful event. Together, these appraisals produce a move towards either coping strategy. In ongoing situations like employment, if the strain persists, people may undertake cycles of appraisals to generate more efficacious coping strategies. But, as a large body of research on stress and health has demonstrated, if individuals are unable to resolve the problem, then the ongoing strain results in a range of negative effects on health and well-being (Brondolo et al., 2009). Although there are other coping theories, Lazarus and Folkman's theory is supported by a body of research showing the utility of distinguishing between problem-based and emotion-focused coping strategies, and the argument that people's ability to cope with stressors is dependent on their assessment of their environment and the resources they believe to have available (e.g., Biggs et al., 2017; Endler & Parker, 1990; Spates et al., 2020).
Coping with gendered racism and critical and Black feminist perspectives on resilience
Much of the research on coping strategies in response to racism does not explicitly examine gender issues, despite feminist scholars highlighting how Black women are “at risk of experiencing a combined discrimination known as gendered racism” (Jones et al., 2021, p. 221; also see Burton et al., 2020; Burton, 2022; Shorter-Gooden, 2004). The limited literature on gendered racism evidences a consistent and strong pattern of women of African heritage using emotion-based strategies such as social support and religion/spirituality for coping in response to racism (see e.g., Bacchus, 2008; Gentles-Peart, 2020; Greer & Cavalhieri, 2019; Hayward & Krause, 2015; Jacob et al., 2021, 2022; Outlaw, 1993; Spates et al., 2020). Within classic interpretations of Lazarus and Folkman's theory, faith is categorised as an avoidant emotion-focused strategy and, as a result, associated with negative mental and physical health outcomes (Lewis et al., 2017). In contrast, problem-based strategies are considered to be more effective (West et al., 2010), yet individuals may not have the power to change racist behaviour or organisations.
In relation to gendered racism, much is still underexplored; some argue that it requires multifaceted strategies that incorporate both problem- and emotion-focused solutions (Lewis-Coles & Constantine, 2006; Utsey et al., 2007). Modelling research suggests that spirituality positively influences how Black/African American individuals cope with adversity (Utsey et al., 2007); however, Hayward and Krause (2015) argue that findings are inconsistent and note intraethnic differences.
In their systematic review of African American coping strategies for racism, Jacob et al. (2022) highlighted that a range of strategies were used by all Black respondents, but that Black women were more likely to use strategies related to social support and spirituality that enabled them to stay optimistic by sharing experiences, reframing suffering, and creating meaning and a sense of place in the world. For these reasons, Jacobs et al. considered spirituality, along with an ethnonationalist Africultural reclaiming of identity, to be a functional coping mechanism because it changed one's emotional and mental state, despite having limited utility in reducing racism. This conclusion is supported with research showing a negative relationship between spiritual coping and psychological distress (Szymanski & Lewis, 2016; Thomas et al., 2008) and health (Lewis et al., 2017).
Spirituality is often entangled with other ambivalent coping strategies, such as drawing on one's “strong” gendered racial identity as a buffer (Lewis et al., 2017); for example, drawing strength from identifying as a “strong Black woman,” a subject position that constructs women of African heritage as independent, self-reliant, and strong, yet nurturing and willing to self-sacrifice (Watson & Hunter, 2016). Liao et al. (2020) showed how this identification was associated with negative psychological outcomes, findings that link with wider critiques over the ways in which racialised women are made responsible for coping with the experience of gendered racism—preferably in silence (Graham & Clarke, 2021; Marecek & Lafrance, 2021; Nkomo, 1998).
Lewis et al. (2012) distinguish between resistance coping (e.g., using voice as power), collective power (leaning on support networks), and self-protective coping (de-sensitisation and/or drawing on ideas of a strong Black woman/superwoman), noting how the latter in particular remains understudied. They emphasise how self-protective coping, while marking elements of agency by “choosing” not to “battle” and avoiding the associated significant impact on mental and physical health and financial stability, may instead result in de-sensitisation. This was also found in Graham and Clarke's (2021) study with British women of African Caribbean heritage, which showed how a “strong Black woman” identity allowed their participants to manage their distress, but it also meant that they minimised their feelings to avoid looking or feeling weak. “Resilience” here then also must be viewed not just as a positive and successful adaption in the face of stress, as it is often viewed in the stress-response literature (Robertson et al., 2015), but also through a critical feminist lens (see e.g., Burman & Chantler, 2003; Fine, 2011) and within a wider context of understanding how it is precisely the power differentials between women and men, Black and White workers, and between migrant and British workers, that limits the responses available to racialised women workers.
Overall, studies point to how coping mechanisms for gendered racism may be simultaneously advantageous and disadvantageous, and the need for more work to understand how gendered racial identity—for example, being a “strong Black woman” as a coping strategy—is experienced. There is limited research exploring the coping strategies of Black women in the context of having to negotiate “entangled systems of oppression” (Spates et al., 2020, p. 513), and even less work in the context of employment. The current study addresses this gap with an in-depth, phenomenological analysis of coping responses to gendered racism, thereby making an important and novel contribution to this canon of work. Centring the experiences of female Nigerian migrant doctors and nurses working in the NHS as a site for study, it addresses the following questions: What coping strategies can professional Black migrant women employ in response to experiencing gendered racism at work? And how efficacious were these coping strategies within this organisational and professional context?
Method
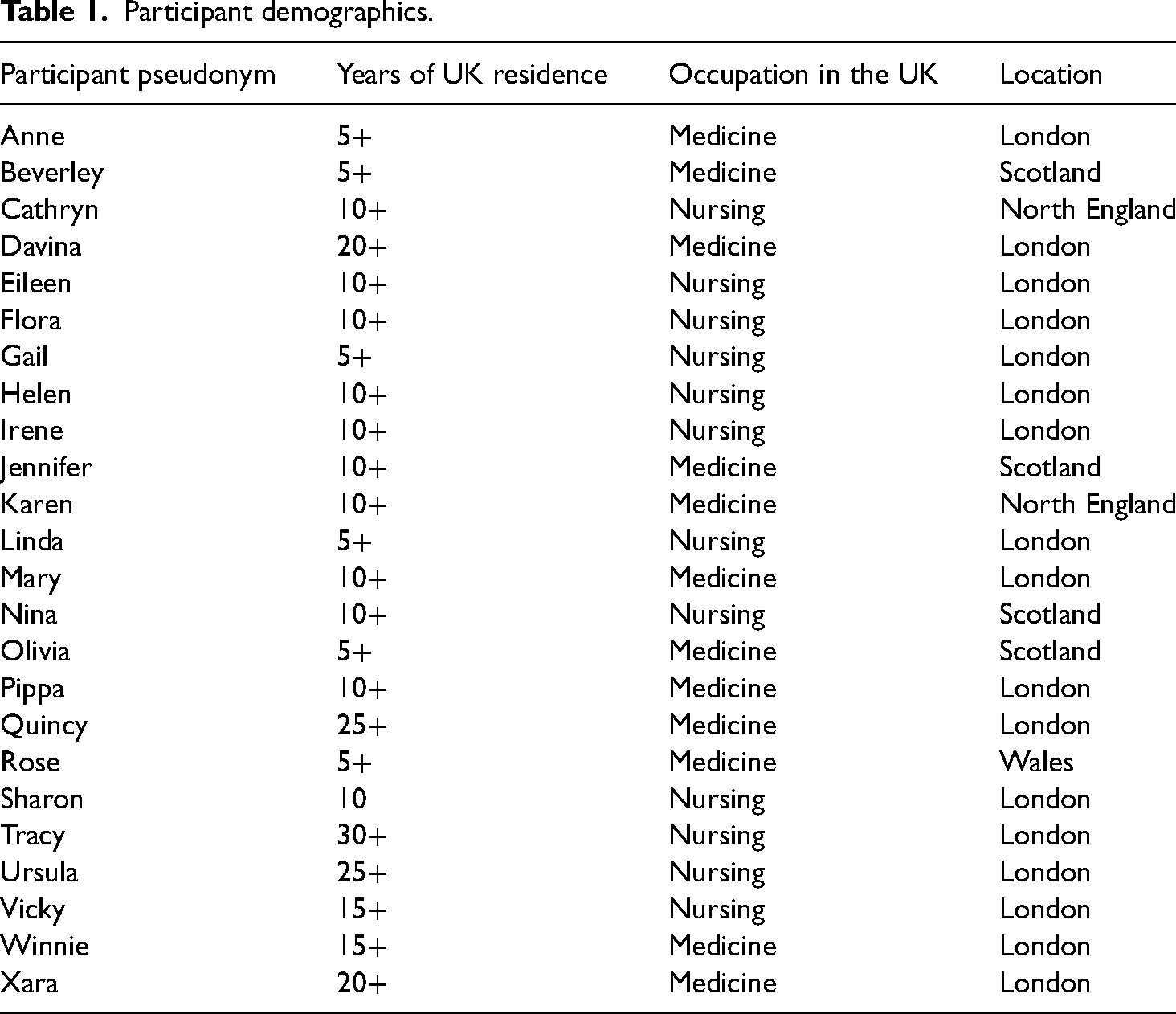
This article is part of a larger project examining the experiences of female doctors and nurses working in the NHS who migrated to the UK from Nigeria. Twenty-four Nigerian women (12 doctors and 12 nurses) working in the NHS were recruited. This included women trained in Nigeria and those who retrained after emigrating. The respondents had been in the UK between 5 and 34 years, most were married (n = 21) and mothers (n = 22). Respondents worked across the UK, in cities and regional areas, allowing the study to explore a range of experiences across this diverse organisation with regional differences in the ethnic diversity of its employees, as described in our literature review above (Tables 1 and 2).
Participant demographics.
Discussion cards featured the following words.
The first author interviewed the participants, and like her participants, is a Nigerian woman living and working in the UK. This enabled research relationships to be developed, with participants sometimes explicitly noting this, saying phrases like “you understand where I am coming from.” This shared background meant that certain practices, or the absence of these practices, could be recognised, for example, Nigerian cultural practices discourage publicly sharing difficulties. That the research participants, who were time-constrained and culturally primed not to discuss difficulties, volunteered for this project and then discussed experiences of racism is a testament to the difficulties they faced and the importance of being able to speak to somebody they thought would understand.
All respondents were interviewed once, with researchers returning to a subset of eight respondents (four doctors and four nurses) for a second interview, creating 32 interviews in total. Phenomenological psychology aims to create insight into experience through deep engagement with respondents’ sense-making, accordingly, the study design was developed to create in-depth engagement (see e.g., Callaghan et al., 2015; Cosgrove, 2000). This was operationalised through two phases of data collection and two phases of analysis (see Figure 1).
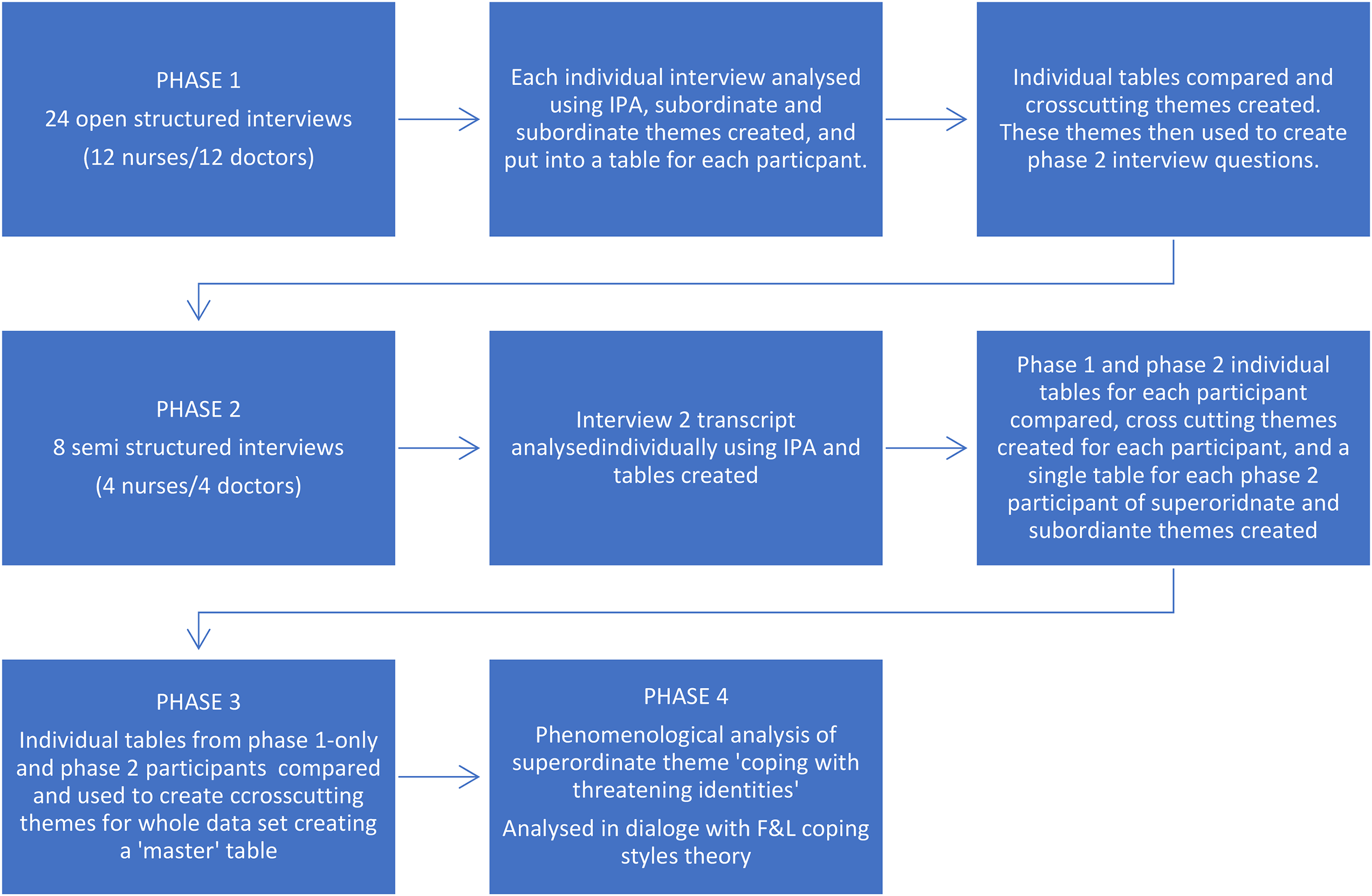
Research design.
Phase 1 used an open structured interview technique, where cards with a single word or short phrase (e.g., woman), identified from the literature review as a potentially relevant topic, were spread in front of each participant, and the participant was invited to pick any card with a topic they wanted to discuss (see e.g., Robson et al., 2022).
Some cards were left blank for respondents to introduce topics they considered relevant; this method enabled a respondent-driven interview. Each interview was subsequently analysed using the data-driven, inductive method of interpretive phenomenological analysis (IPA), following Smith et al. (2009). In this method of analysis, each individual interview is analysed separately through a systematic process of (a) creating descriptive codes summarising the content, (b) creating interpretive codes interpreting the description in light of the research question and with a view to understanding the lived experience being described, (c) bringing patterns together in themes, and (d) clustering those subordinate themes into superordinate themes (which are summarised in a table for each participant). The final stage (e) examines shared themes across respondents’ experiences, from which, cross-cutting superordinate themes are created (producing a “master” table that consolidates the individual participant tables).
The cross-cutting superordinate themes were used to create an interview schedule to focus on shared, salient experiences. A subset of eight participants (four nurses, four doctors) were interviewed for a second time (Phase 2); these interviews were analysed separately, then brought into dialogue with the analysis of their corresponding first interview. Combined, this process created 24 individual tables of analysis. In Phase 3, these tables were then compared to create an overall table summarising the participants’ shared core experiences, and interpretations of these experiences. This process allowed us to meet the quality criteria for phenomenological psychological analysis relating to idiographic analysis of individual experience and in-depth engagement with that experience, with a view to being able to say something meaningful about the nature of that experience.
A superordinate theme produced through this process, which we called “coping with threatening identities,” described how participants learnt to see themselves through racist constructs as having dis-preferred identities, a process that cultural theorist Stuart Hall (1990) referred to as becoming Black in contrast to being Black. In line with phenomenological psychology (see e.g., Hornstein, 2013; Lesch & van der Watt, 2018; Willig, 2012), in Phase 4, we explored which theories might further illuminate this superordinate theme, identifying Lazarus and Folkman's (1984) coping styles theory as not only a robust framework for understanding responses to stressors, but one that also mapped closely to our participants’ talk. We identified participants’ use of relocation (either geographically, professionally, or organisationally) as a problem-based coping strategy, and their use of religion and a national gender-racialised identity of “the resilient Nigerian woman” as emotion-focused styles. It is these strategies, analysed through a phenomenological lens that pays attention to the lived experience and the interpretation of experience, that we present in our analysis.
Finally, we note that ethical approval was granted from Aberystwyth university’s ethics committee, and ethical considerations were ongoing throughout the project, including limiting information on geographical location and medical specialism to protect the anonymity of respondents in locations where there were few Black female doctors. A range of conventional quality criteria for qualitative research was also upheld during analysis, including iterative cycles of analysis, peer review, and reflexivity.
Analysis
Relocation, relocation, relocation
A key problem-based coping strategy, employed by both doctors and nurses, was seeking out contexts with high demand for staff, the rationale being that the propensity of employers towards bias in recruitment and hiring was reduced when positions were hard to fill. Moving to where they identified such opportunities (with doctors required to apply and interview several times for posts as part of their rotational training) required the participants to relocate either geographically, professionally, or organisationally. Doctors described moving geographically or professionally into less competitive/prestigious subfields to access training or jobs, while both nurses and doctors described moving organisationally into more flexible but less secure or prestigious work to manage the demands of work and childcare.
Geographic relocation
Our doctor participants sought work where there was an undersupply when they experienced difficulties securing training opportunities and appraised the problem as a threat underpinned by discriminatory recruitment practices. This often meant relocating out of urban hubs and to more geographically regional areas. As Pippa explained: Because London is very competitive, so there are more doctors than there are jobs … but if you go up North or maybe even Scotland, it is very easy to get jobs for immigrants, if you go up to the north of England … So that was what I did, I applied in the north of England before moving back to London. (Pippa, doctor, London)
Pippa's move away from a “very competitive” London to the north of the UK is not just a step to avoid competition, rather, she explicitly links this experience to being an immigrant. She talks about this decision in a matter-of-fact way, but there is subtle distress here. She recognises herself as someone who is dis-preferred,
1
an immigrant who cannot compete against her British counterparts, moving somewhere she did not want to live, and moving back to London as soon as the opportunity arose. For the same reason, Beverley also went north for her training, but unlike Pippa, she chose to stay: Many of the people I trained with, once they finished their training, they went down to England … I stayed on because there were more opportunities here in Scotland than in England … because of the cold and everything, you know, people don’t really want to stay up here. I have never lacked a job. (Beverley, doctor, Scotland)
Beverly gives us a sense of a collective moving north to access training, and returning south as soon as possible. However, Beverly stays north, a successful strategy from her perspective, as she has “never lacked a job.” It is important to consider why these jobs are dis-preferred and only a choice “for people who under normal circumstances wouldn’t have gone there” (Jennifer, doctor, Scotland). Beverly hints at the relative harshness of conditions with her statement “because of the cold and everything,” describing the weather but also other issues in her generalising “and everything.” This generalised statement hints at things that are difficult to say, and we get a sense of what they might be from other participants who described the experience as isolating, since moving north, especially to semirural and rural communities, meant being away from Nigerian communities or communities in which diversity is comparatively high, resulting in our participants being visibly different. As Jennifer explained, “where I work, I am the only Black person so amongst the doctors, nurses, admin staff, I am the only Black person here” (doctor, Scotland).
The outcome then was a sense of isolation and lack of social support, both well-established stressors (Nelson et al., 2023). As a solution, geographical relocation thus created its own stressors. Professional status differences mattered here as the problem of securing good training opportunities is part of a structural concern for doctors specifically, who need to secure a number of roles as part of their training, while there are more job opportunities for nurses in urban hubs such as London and more streamlined training pathways.
Professional relocation
The doctors described switching to specialisms that were less popular as a problem-based solution to cope with perceived discrimination in recruitment, again seeking to take advantage of worker shortages and at the intersections of androcentric working practices and gendered racism. Quincy, for example, describes her “switch to general practice” as motivated by a need to manage childcare, combined with recruitment practices that made it “virtually impossible as a migrant and as a female” to aspire to more senior or prestigious positions in medicine: So I made a decision to switch to general practice, which was primarily to help me meet my family obligations … [And] the training hierarchy in the hospital position, it was designed, in my opinion, to be highly discriminatory, because you need to move on in the job every 6 months, so you are forever applying and interviewing to get the next position, but that seemed to heap up more, 8 times more against you once you reach the registrar position … Because to get beyond that, to the higher post, the senior registrar and the consultant post is virtually impossible as a migrant and as a female. And that also was part of my decision to move into general practice. (Quincy, doctor, London)
Quincy's appraisal of her situation is that it was “virtually impossible” for her to meet her career ambitions, and her solution was therefore to relocate professionally into general practice. She is specific in describing her decision as linked to her being a mother and a migrant. Moving into general practice was a coping strategy for many of our doctors because it is less competitive and working hours are more manageable for women who tend to assume greater childcare responsibilities than men (Kokot-Blamey, 2021, 2023; Stephens, 2012). Jennifer (doctor, Scotland) explained, “you are sure that as a general practitioner, when you finish your training, you will be accepted somewhere for you to work.” Pippa also adopted this strategy, abandoning her ambition to become a surgeon: For a job like general practice, your gender is an advantage … in other specialities like surgery for example, I find women complain about the hours, with family life it is not really good … Initially, I thought I was going to be a surgeon, but the hours were so difficult with home, so I chose to be a GP. (Pippa, doctor, London)
Other doctor participants also described understanding that race, or race and gender, limited their opportunities, shaping their appraisal of career possibilities and solutions. Such as when Rose (doctor, Wales) described her specialism choice: “paediatrics is not a field that's White-dominated, so not many Whites want to do it, so it also helped [move into this specialism].”
In this example, the “Whites” choose their speciality, determining what constitutes a less desirable area, which is then left to Black doctors such as Rose. In both cases, the problem-based solution is to move into a professional area where they can minimise these threats of recruitment bias and manage challenges of work and home life balance. However, as with the geographical relocation strategy, professional relocation comes with its own stressors, in particular having to curb their ambitions, and potentially job satisfaction.
Organisational relocation
Some of the participants shared becoming a locum
2
GP or nurse to manage the racialised and gendered challenges they faced as Nigerian mothers, thus leaving their employment status with the NHS and joining a locum agency instead. The majority of the women who were mothers saw themselves as the primary carer for their children, and some were lone parents. Below, two nurses describe how this context shapes their need for flexibility: I like the flexibility that I work for myself, because of the way they do the shifts … Especially if it is a one-parent home, like a single parent, it is not easy to get a childminder round the clock, so it is good if you are able to work for yourself and do your agency work, whereby you work when it is ok for you in your circumstances. (Ursula, nurse, London) I went into agency work because my son was still quite young at the time … Being agency, I was my boss, I could choose when I wanted to work … I can actually work with him, when he is on midterm and holidays, and do the extra shifts if I have to, just to balance my finances. (Tracy, nurse, London)
Anne describes a similar rationale for doing “locum GP” work: I am a locum GP; I work anywhere … so it is working nicely for me now … That is what I decided to do because of the family, I wanted to spend more time with the family, because I wanted to do some home runs. (Anne, doctor, London)
However, the move to locum created other stressors, such as reduced career progression, so that prioritising childcare came at a personal career cost. Eileen shares: It is difficult being a mom, isn’t it? … if your husband is posted, you wouldn’t leave a little child … a big responsibility is on me for the children, my husband is really supportive … I have to work shifts, so he has to be at home at night and look after them but still the onus is on you, and so my priorities are mainly now raising the children, so it affects my progression in my career … getting flexible working hours, those things have really helped me to be able to do my job and help me look after my children. (Eileen, nurse, London)
The ways in which the NHS is organised around the notion of an ideal worker who can prioritise work and commit to any shift pattern has been problematised already (see e.g., Ozbilgin et al., 2011; Regenold & Vindrola-Padros, 2021). The participants’ accounts showed how these gendered challenges, which many women share, are exacerbated by the intersections of their gendered and racialised positionalities as Nigerian wives and mothers. Sharon explains: Back home, you can be a housewife and your husband goes to make the money, then you can do things at home and keep the house nice and tidy, but here, you have to do everything, even though you come back at 11p.m., you are still expected to get into the kitchen and do things, that's our culture, our Nigerian mentality … in my next world, I will be a man. (Sharon, nurse, London)
They are caught in a bind where they must meet the expectations commonly laid upon Nigerian mothers but do so within a Western context—and at the same time, they are constrained by the gendered racism they perceive in their everyday working lives. Jennifer makes a similar point, stating: I think that limits women to a certain degree … in the Western world, people have little help domestically. So, you have to juggle your work life, or your profession or school life with, if you are married, being a wife, or being a mother, or being both. (Jennifer, doctor, Scotland)
Becoming a locum nurse or doctor offers some of the flexibility they need to meet the gendered demands of their home lives. Yet, this problem-based coping strategy is also a stressor in itself and, besides limiting their career progression, it isolates them organisationally and exposes them to additional risks, including the risk of litigation, already heightened by their status as Black and minority ethnic healthcare professionals (Atewologun et al., 2019). It further positions them in a dis-preferred location by themselves being seen as a risk (Chapman & Cohen, 2018; Ferguson & Walshe, 2019). While the nurses and doctors were thus seeking locum opportunities to cope with gendered and racialised constraints, these too are likely to bring along stressors themselves.
Resilience and identity
The participants described two key emotion-focused strategies: faith and national identity. Both gave participants a sense of resilience in the face of adversity, which could be experienced either separately or as intersecting. Faith gave our participants a perspective that helped them shift their emotional response to their experiences of racism. As nurse Eileen explained when talking about racist encounters with patients: “being a Christian, I try to see everyone the way God sees them, so my faith also affects my perception.” Similarly, Mary described drawing on a Christian identity as a successful coping strategy: Being a Christian sometimes makes you think about a higher power being in charge of things that happen … where you might feel that there is an obvious reaction to you on the basis of either my gender or my race or the fact that I am a migrant. Being a Christian, it kind of helps you modify your reaction, or your understanding of it, and your ability to cope with it. (Mary, doctor, London)
Participants understood the use of their Christian faith as an emotion-focused solution to dealing with racism as not just an individual strategy, but a response that is culturally constituted. Jennifer (doctor, Scotland), for example, described her own reliance on faith as part of a broader ethnic emotional strategy: “I depend on God and my faith is very strong … that is a driving force for Black and ethnic people, specifically Black Africans.” Participants connected their Christian identity with their national identity as Nigerians, creating an understanding of themselves as resilient, as Sharon (nurse, London) says: “by God's grace … we Nigerians … survive in any condition we find ourselves in.” This account was developed further by Cathryn: As a Nigerian … we all know we can make something out of nothing … the background already, you know, prepares us for whatever situations we find ourselves … to achieve what we want to achieve … We Nigerians, Christians, we believe in God that something is going to be possible regardless of all obstacles. Definitely, you will achieve your aim if you keep pushing. (Cathryn, nurse, North England)
In these examples, we show how participants drew on their spirituality, nationality, and/or sense of African ethnicity, often entangled, to create emotion-focused solutions. Resilience can be conceptualised as a trait, a process, or an outcome (Robertson et al., 2015). In our study, resilience was made sense of within both nature and nurture frameworks, seen as both a trait inherent in Nigerians and a product of Nigerian upbringing, as when Rose (doctor, Wales) explained, “from being a child, you are always told the person that came first [in the school test]—does he have two heads? … So, all those things help build resilience.”
Resilience was thus described as related to their heritage, passed down from their family, and part of their Christian and African (or specifically Nigerian) culture; one that grounded them in a common experience and collective way of dealing with challenges. Resilience as an identity works as an emotion-focused solution by moving from the appraisal of stressors as harmful or threatening towards an understanding that the participants were people who had the strength to meet challenges such as these. Nonetheless, this utilisation and adoption of resilience leaves the problem of racism intact and keeps the onus on the participants to manage their responses.
Discussion
Contributing to the wider existing literature on racism and gender in employment, we examined how female Nigerian healthcare workers cope with the racism, sex discrimination, and structural inequalities they encounter working in the NHS (Atewologun et al., 2019, 2022; Edeh et al., 2022). We were interested in learning about what coping strategies the women adopted, whether they were effective, and the extent to which these were mediated by professional status. Our approach considered how nurses and doctors responded in different or similar ways, and how the gendered constraints of being a Nigerian mother aligned the coping strategies of these two groups.
Lazarus and Folkman's (1984) distinction between problem- and emotion-based coping was evident in the participants’ talk, and facilitated the final stage of the analysis. Problem-based coping was evident in how the majority of participants relocated themselves geographically, professionally, and/or organisationally to negotiate the racism that they perceived to structure their employment opportunities. However, this resulted in isolation and/or relinquishing of ambitions. There was also a broader social cost to the doctors’ geographical relocation strategies, since Nigerian communities in London were less likely to access a female Nigerian doctor or see role models for their children who might aspire to be doctors.
Africultural coping (Utsey et al., 2007) was prevalent as an emotion-based coping strategy. This echoed findings by Graham and Clarke (2021), who problematised the “strong Black woman” stereotype with which Western cultures burden women of African heritage, but from which their respondents also drew strength. Our respondents too referred to their faith, but also their strong sense of being a Nigerian, when being Nigerian was associated with resilience and one's ability to “survive in any condition” (Sharon, nurse). Being Nigerian and being Christian were interwoven.
Spirituality and a sense of having support from a higher power can provide an emotion-based solution that enables individuals to overcome challenges and difficulties in their person–environment relationship; and here, we were able to explore this from an employment perspective. Both doctors and nurses were aware of the extent to which they were facing difficulties that their White, male, and/or British peers did not face, yet felt able to cope with these challenges, and this was to do with their positionality, their upbringing, and their faith. In addition, participants’ religious doctrine provided them with alternative ways to respond to those who discriminated against them, practicing a Christian forgiveness that facilitated a sense of resilience. Jacob et al. (2022) also describe religion/spirituality as a common emotion-focused coping strategy for Black Americans responding to racism. Being Nigerian itself also offered our participants an identity associated with resilience, giving them an emotionally strong standpoint from which they could meet their challenges. Unlike the problem-focused solutions, which consistently created further stressors, the emotion-based coping strategies were effective in moderating the responses to difficult situations they could not change, albeit leaving the problem itself—that is, gendered racism—unchallenged and placing the burden of coping on individual women.
Our research demonstrates how gendered racism is particularly pervasive in its effects, because it does not allow for the possibility of tackling the problem itself due to the lack of power of those experiencing discrimination and how endemic these conditions are both in employment and the wider society. The problem-based solutions the Black women in our study shared with us were focused on changing the environment–person relation by considering demand and supply, and repositioning themselves accordingly to reduce the likelihood of racist bias by employers. This is a coping mechanism that has also been reported by other demographic groups facing institutional racism. For example, Raghuram et al. (2016) found that South Asian doctors recruited into the NHS from the 1970s onwards were channelled into less popular specialities. Forty-five years later, our respondents did not need to be channelled—they moved themselves towards specialisms, geographies, and organisational pathways that they understood “not many Whites want to do” (Rose, doctor), curbing their own aspirations in the process. Similarly, the emotion-based strategies—relying on their Christian faith and their Nigerian or African identity—to manage the challenges they found, left the problem of gendered racism unchallenged.
The coping mechanisms described are individualised solutions to collective problems. Here, we find no sisterhood (Gentles-Peart, 2020) nor “collective power” to coping (Lewis et al., 2012). Like the respondents in Jacob et al.'s (2022) systematic review of African American women's coping strategies, which reported few “overt” strategies directly confronting racism, our participants rarely perceived collective responses or support networks available to them. Only one participant described using organisational structures to make a formal complaint (another had considered it, but the outcomes were too detrimental, and so she withdrew it). Instead, our respondents’ problem-focused strategies represented individualised solutions in line with neoliberal citizenship related to self-regulation and following market forces, which, in this context, meant moving out of the way and managing their feelings by affirming their sense of being a Nigerian who can cope, and their sense of being a Christian who can forgive.
The gendered and racialised NHS worker then also is an example of what feminists such as Scharff (2016; also see Riley et al., 2019) dub the entrepreneurial self: “responsible for managing opportunities and constraints, the entrepreneurial self only has itself to blame if something goes wrong” (p. 115). But this comes at a cost. By relocating themselves professionally, geographically, or organisationally, our respondents encountered isolation (a known stressor; Cacioppo & Cacioppo, 2014; Hall et al., 2012) from other Black Nigerians while in White suburban and regional locations; curbed their aspirations for their careers; and assumed a dis-preferred and vulnerable status as locum doctors and nurses. To overcome this isolation, they rely on their effective use of emotion-based coping.
Our findings evidence how institutional racism in advanced capitalism is pervasive and self-perpetuating—the respondents were conscious of the institutionalised racism that has been well-documented and which they had experienced and came to expect (“as a foreign-trained graduate, as a woman, and a Black person, I am the last on the list who will be seen as someone to get a number so I can train as a surgeon”; Jennifer, doctor). And it is precisely the dissonance in power and their racialised and gendered positionalities that mean that they sense that their only way to cope effectively is to adopt an avoidant coping mechanism—by getting out of the way (problem-based coping) and coping with the fall out of these only ever partially effective problem-based coping mechanisms through emotional self-regulation (emotion-based coping). This study also provides further evidence for the persistence of gendered racism and other structural inequalities in the NHS, highlighting the intersecting and complex challenges experienced by the Black, female migrant workers that the NHS relies on so much. We show the costs of coping not just with the experience of racism, xenophobia, and sex discrimination in the workplace, but also the isolation and silencing that come from the limited coping strategies available to them as a result, completing a vicious circle.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.