
Abstract
This study tested the effects of a new cognitive-bias modification (CBM) intervention that targeted an approach bias for alcohol in 214 alcoholic inpatients. Patients were assigned to one of two experimental conditions, in which they were explicitly or implicitly trained to make avoidance movements (pushing a joystick) in response to alcohol pictures, or to one of two control conditions, in which they received no training or sham training. Four brief sessions of experimental CBM preceded regular inpatient treatment. In the experimental conditions only, patients’ approach bias changed into an avoidance bias for alcohol. This effect generalized to untrained pictures in the task used in the CBM and to an Implicit Association Test, in which alcohol and soft-drink words were categorized with approach and avoidance words. Patients in the experimental conditions showed better treatment outcomes a year later. These findings indicate that a short intervention can change alcoholics’ automatic approach bias for alcohol and may improve treatment outcome.
A central paradox of addiction is that addicted people continue their self-destructive behavior despite knowledge of the consequences (Wiers & Stacy, 2006). Recent research on implicit or relatively automatic processes provides clues to understanding this paradox. The essential notion is that behavior is partly governed through relatively automatic processes that may exert their influence outside conscious control (Stacy & Wiers, 2010). From this perspective, addictive behaviors are conceptualized as an imbalance between strong impulsive or associative reactions to drug-related cues and relatively weak reflective or controlled processes, and this makes the individual susceptible to sensitized cues triggering action tendencies leading to the addictive behavior (Bechara, 2005; Volkow, Fowler, & Wang, 2004; Wiers et al., 2007). This can be reflected in different cognitive biases: an attentional bias for alcohol-related stimuli (Field & Cox, 2008), a memory bias for the automatic activation of alcohol-related associations (Wiers, Van Woerden, Smulders, & De Jong, 2002), and a bias toward automatically activated action tendencies to approach alcohol (Palfai & Ostafin, 2003). If people are not willing or able to counter these biases, the addictive behavior is likely to continue (Wiers et al., 2007).
Recently, researchers have developed new methods to directly target cognitive biases: cognitive-bias modification (CBM). CBM is used for two purposes. The first is to test the causal role of the bias (MacLeod, Rutherford, Campbell, Ebsworthy, & Holker, 2002). Second, CBM can be clinically applied to reduce maladaptive cognitive biases, as the first successful clinical trials of attentional-bias modification have demonstrated for anxiety (e.g., Amir, Beard, Burns, & Bomyea, 2009) and addiction (Fadardi & Cox, 2009; Schoenmakers et al., 2010).
The present study focused on the manipulation of a bias in the action tendency to approach alcohol. Past research has demonstrated this bias in problem drinkers using different experimental tasks (Field, Kiernan, Eastwood, & Child, 2008; Palfai & Ostafin, 2003). We recently developed the alcohol approach/avoidance task (alcohol-AAT; Wiers, Rinck, Dictus, & Van den Wildenberg, 2009). In the alcohol-AAT, participants are instructed to respond with an approach movement (pulling a joystick) to pictures of one type and to respond with an avoidance movement (pushing a joystick) to pictures of another type. Pulling on the joystick increases the size of the picture, and pushing on it decreases the size. This zooming effect generates a sensation of approach or avoidance, respectively. 1
In the first study using the alcohol-AAT, heavy drinkers showed an approach bias: They were faster to pull than to push in response to alcohol pictures, but this was not the case for general positive or negative pictures. This effect was genetically moderated: Carriers of the OPRM1 G-allele showed the strongest alcohol approach bias (Wiers et al., 2009). In the first preclinical CBM study targeting an alcohol-approach bias (Wiers, Rinck, Kordts, Houben, & Strack, 2010), students’ action tendencies were experimentally modified: Half of the participants were trained to avoid alcohol, and the other half to approach alcohol. This manipulation changed students’ approach bias outside their subjective awareness, with generalization to new pictures in the alcohol-AAT and to a different task (an Implicit Association Test, IAT, which uses words rather than pictures). Successful retraining was associated with congruent changes in alcohol consumption in a taste test.
The present study was the first to test this new CBM method in a clinical sample. We designed a randomized controlled experiment, in which 214 alcoholic patients were randomly assigned to one of two experimental or one of two control conditions. Patients in the experimental conditions were trained to consistently make avoidance movements in response to alcohol pictures and approach movements in response to pictures of nonalcoholic drinks, with the two experimental conditions varying only in whether they were explicitly trained to avoid alcohol pictures or not. Patients in the control conditions were either not trained to avoid alcohol at all or received sham training.
All patients followed regular cognitive-behavior treatment for inpatients. A year after treatment discharge, patients’ treatment outcome was assessed. We predicted that the minimal CBM intervention (four sessions preceding regular treatment) would change alcoholic patients’ approach bias for alcohol, and we investigated whether this would have an added effect on treatment outcome.
Method
Participants
Two hundred fourteen alcohol-dependent patients were recruited from the Salus Clinic, Lindow, Germany. Patients were provided with general information about the study and told they could withdraw without any implications for their treatment. All patients signed informed consent. The study had the necessary institutional review board approvals. Criteria for inclusion in the study consisted of a primary diagnosis of alcohol dependence, which was assessed with the computerized version of the Composite International Diagnostic Interview (Robins et al., 1988). Participants with insufficient German language abilities or neurocognitive problems were excluded from the study. Individuals with severe neurological disorders, such as Korsakoff’s syndrome, had been excluded at entrance to the clinic. Use of other drugs was not an exclusion criterion, although such use was modest. No participant received anticraving drugs, and 39% (84 participants) received other medication (mainly antidepressants; see Table 1 for characteristics of the sample).
Mean Characteristics of the Sample
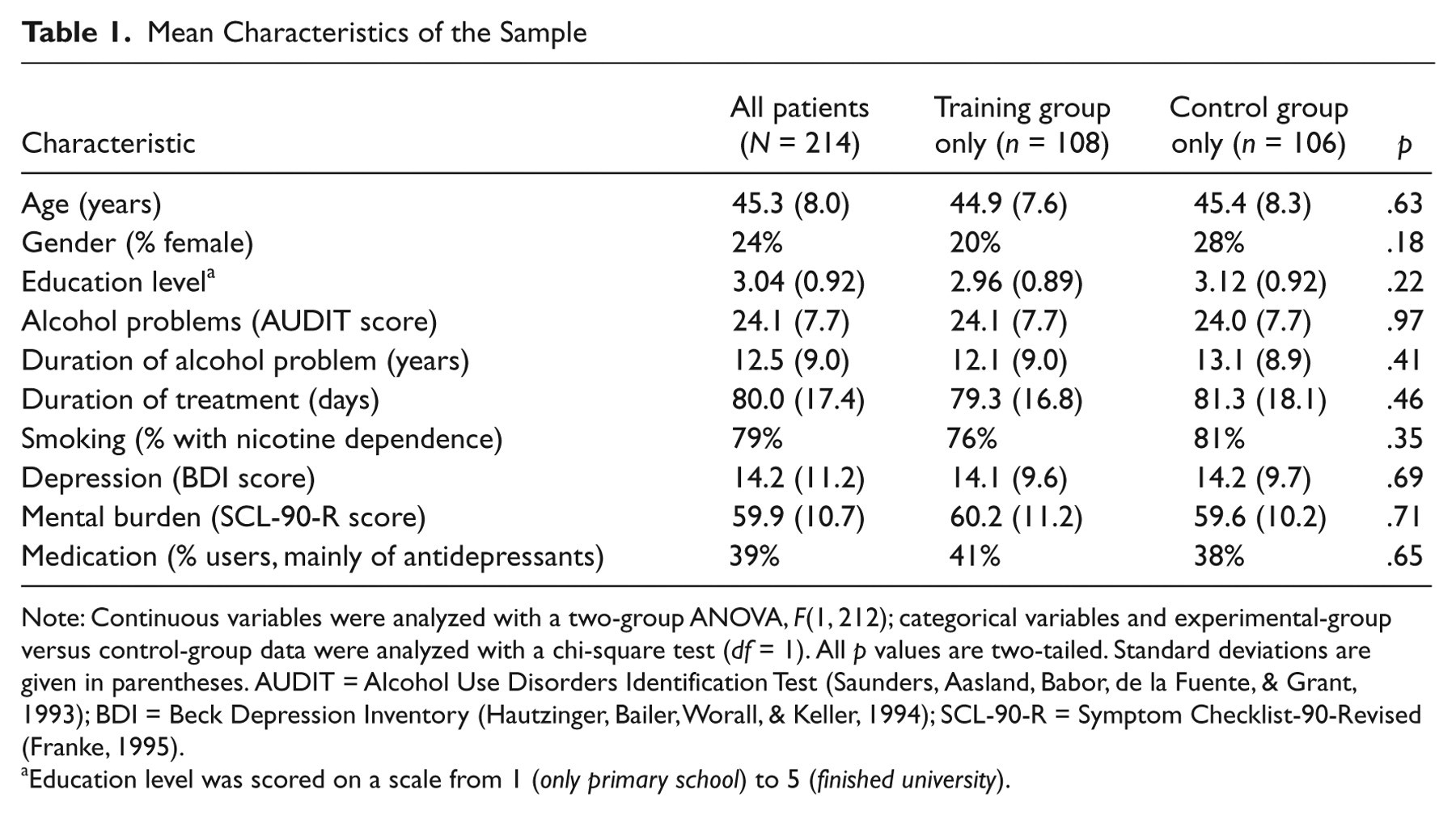
Note: Continuous variables were analyzed with a two-group ANOVA, F(1, 212); categorical variables and experimental-group versus control-group data were analyzed with a chi-square test (df = 1). All p values are two-tailed. Standard deviations are given in parentheses. AUDIT = Alcohol Use Disorders Identification Test (Saunders, Aasland, Babor, de la Fuente, & Grant, 1993); BDI = Beck Depression Inventory (Hautzinger, Bailer, Worall, & Keller, 1994); SCL-90-R = Symptom Checklist-90-Revised (Franke, 1995).
Education level was scored on a scale from 1 (only primary school) to 5 (finished university).
Assessment and outcome measures
At intake, clinical psychologists diagnosed patients using the Composite International Diagnostic Interview. The Alcohol Use Disorders Identification Test (AUDIT; Saunders, Aasland, Babor, de la Fuente, & Grant, 1993), Beck Depression Inventory (Hautzinger, Bailer, Worall, & Keller, 1994), and Symptom Checklist-90-Revised (SCL-90-R; Franke, 1995) were also administered.
Experimental tasks at pretest and posttest
Craving
Patients rated the pictures used in the alcohol-AAT (alcohol and soft drinks) on a 6-point Likert-scale ranging from I don’t want to drink this at all to I would love to drink this now.
IAT
The IAT is a measure of the strength of association between concepts. It consists of a speeded classification test, in which stimuli (presented consecutively on a computer screen) are sorted into two target categories (in this case, alcohol and soft drinks) and two attribute categories (in this case, approach and avoidance) while using only two response keys, one on the left and one on the right. In the first combined block, alcohol and approach stimuli were categorized together on one side (with soft drink and avoidance stimuli on the other side; see Fig. S1 in the Supplemental Material available online). In the second block, alcohol and avoidance stimuli (and soft drink and approach stimuli) were categorized together. The extent to which participants responded more quickly to the first combined sorting condition than to the second was used to estimate the relative strength of alcohol-approach associations. The IAT has demonstrated good predictive validity across many areas of research and, compared with self-report measures, has added unique variance to the prediction of outcome behaviors (Greenwald, Poehlman, Uhlmann, & Banaji, 2009). Varieties of the IAT have been shown to differentiate heavy drinkers from light drinkers (Palfai & Ostafin, 2003; Wiers et al., 2002), with heavy drinkers performing faster on sorting conditions involving alcohol and approach combinations than on sorting conditions involving alcohol and avoidance combinations (Ostafin & Palfai, 2006; Palfai & Ostafin, 2003).
In the study reported here, we administered a standard IAT with seven blocks (Greenwald, Nosek, & Banaji, 2003; see Table S1, Table S2, and Fig. S1 in the Supplemental Material). After three practice blocks, the two combined sorting conditions were presented in balanced order: one combining alcohol with approach (and soft drink with avoidance), and one combining alcohol with avoidance (and soft drink with approach). Participants received the same version of the IAT in the pretest and the posttest to minimize error variance (cf. Wiers, Van de Luitgaarden, Van den Wildenberg, & Smulders, 2005).
Alcohol-AAT
The alcohol-AAT used pictures of 20 alcoholic and 20 nonalcoholic drinks. These pictures were adapted for familiarity (i.e., common drinks in the region of the clinic were used) and presented equally often in landscape and portrait format. Participants were instructed to respond with the joystick to the format of the presented pictures: They pulled the joystick to approach pictures in portrait format or pushed the joystick to avoid pictures in landscape format (as in Wiers et al., 2009; see Fig. S2 in the Supplemental Material). In this assessment task, the required response was unrelated to the picture’s contents. The required responses were practiced with neutral rectangles.
Conditions and experimental manipulation
Patients were assigned randomly to one of four conditions. The study had two experimental conditions and two control conditions. In the first experimental condition (explicit instruction), patients were instructed to respond to pictures of alcohol by making an avoidance movement (pushing the joystick) and to pictures of nonalcoholic soft drinks by making an approach movement (pulling the joystick; see Fig. S3 in the Supplemental Material).To distinguish the task from the assessment task used during pretest and posttest, in which all patients were instructed to react to the format of the picture, we presented all pictures in this experimental condition in the same square format. Patients in the second experimental condition (implicit instruction) continued to respond as in the pretest, but all alcohol pictures were presented in the format they were avoiding (i.e., landscape), and all soft-drink pictures were presented in the format they were approaching (i.e., portrait). Patients were trained in four sessions.
Patients in the control conditions were not trained to avoid alcohol. One control group received no training at all, and the other received four additional sessions of the assessment task (sham training), which required an equal number of approach and avoidance movements to both alcoholic and nonalcoholic drinks. In all training (real or sham), half of the alcohol-AAT pictures were used (10 alcohol and 10 soft-drink pictures, counterbalanced across participants). This allowed us to test for generalization of training effects (cf. Wiers et al., 2010). During training, participants had to correct errors, such as when they pulled the joystick when they should have pushed it. Two hundred training trials were presented with a short break halfway through. Each training session took approximately 15 min.
Procedure and study design
Pretest measures were administered in a fixed order (craving, IAT, alcohol-AAT) to all patients at least 3 weeks after detoxification. The CBM then took place during the standard neuropsychological checkup before treatment. Therapists were blind to whether the training was real or sham, but they knew which group was the no-training control group. Training groups (the experimental groups and sham-training control group) performed four training sessions on 4 consecutive days. One week later, all participants performed the posttest, which was identical to the pretest.
After the brief CBM intervention, all participants received treatment as usual, which consisted of abstinence-oriented inpatient CBT-based treatment, including both individual and group sessions, for an average of 3 months (Lindenmeyer, 2005); this training followed all standards and guidelines of the German Addiction Society (Schmidt, Gastpar, Falkai, & Gaebel, 2006). Average treatment duration was 80 days (range = 28–119 days), with no significant differences between experimental and control groups (Table 1). Fourteen patients relapsed during treatment, with no significant difference between the groups, χ2(1, N = 214) = 1.14, p = .41. In intention-to-treat (ITT) analysis, these participants were classified as relapse. One year after treatment discharge, all patients received a follow-up questionnaire inquiring about their use of alcohol and other substances. Participants who did not return the questionnaire were reminded by mail and telephone. In cases involving death or relapse, information was obtained from patients’ relatives.
Data analysis
There were three primary outcome measures of this study: changes in action tendencies (as registered on the AAT), alcohol-approach associations (as measured on the IAT), and subjective craving (as measured on the 6-point Likert scale). The main clinical outcome variable was treatment outcome 1 year later. Both the AAT and IAT effect scores are, in essence, differences in latencies between two types of responses: approach alcohol and avoid soft drink, and avoid alcohol and approach soft drink.
Until now, the AAT effect has been calculated as the difference between the median scores for pushing pictures of one category (alcohol or soft drinks) and the median scores for pulling pictures of that category (medians are used to minimize the influence of outliers; cf. Rinck & Becker, 2007; Wiers et al., 2009, 2010). However, Greenwald et al. (2003) have developed an improved scoring algorithm for the IAT, which standardizes the difference in response latencies by dividing an individual’s difference in response times by a personalized standard deviation of these response latencies. The advantage of such standardized scores over difference scores is that they are less vulnerable to biases due to differences in average response time (Sriram, Greenwald, & Nosek, 2010). We present these standardized D scores for both the AAT and the IAT as primary outcome variables. We verified all results for the original scoring algorithms. For the IAT, there was never a difference in the pattern of significant results between the scoring algorithms, but results for the AAT were in the same direction but less strong with the original algorithm (see Table S3 in the Supplemental Material).
We collapsed the results of both experimental conditions together and both control conditions together because we found no significant differences in any of the analyses between the two experimental conditions or between the two control conditions (see Table S4 in the Supplemental Material). The analytical sample for the AAT was 173: 27 participants (13 in the experimental group and 14 in the control group) missed one of the two assessment AATs, and the data of another 14 participants (6 in the experimental group and 8 in the control group) had to be discarded because of excessive errors (> 35% error rate in at least one AAT; chance performance would have yielded a 50% error rate). The analytical sample for the IAT was 181: 18 participants (10 in the experimental group and 8 in the control group) missed one or two IATs, and another 15 participants (7 in the experimental group and 8 in the control group) had to be discarded because of excessive errors (> 35% error rate in at least one IAT).
The 1-year follow-up data were analyzed for successfully retrieved outcomes and with ITT. Following guidelines of the German Addiction Society, we used success as a binary outcome variable. Success was defined as no relapse or a single lapse shorter than 3 days that was ended by the patient without further negative consequences. No success was defined as relapse or death, and in ITT analyses, no information and refusal were included in this category.
Results
Alcohol-approach tendencies (alcohol-AAT)
The effects of condition on AAT scores were tested with a 2 (time: pretest, posttest) × 2 (drink: alcohol, soft drink) × 2 (stimuli: trained, untrained) × 2 (condition: experimental, control) mixed ANOVA. There were main effects of time, F(1, 171) = 24.9, p < .001, η p 2 = .13; drink, F(1, 171) = 132, p < .001, η p 2 = .44; and trained stimuli, F(1, 171) = 6.07, p = .015, η p 2 = .034, and interactions between drink and condition, F(1, 171) = 10.1, p = .002, η p 2 = .056, and drink and time, F(1, 171) = 15.3, p < .001, η p 2 = .082; these interactions were superseded by a Drink × Time × Condition interaction, F(1, 171) = 23.0, p < .001, η p 2 = .12. All other effects were nonsignificant (Fs < 2.1, effect sizes < .013).
Follow-up analyses were performed for both drink types separately using the same mixed ANOVA but with drink removed. For alcohol, there were main effects of time, F(1, 171) = 35.9, p < .001, η p 2 = .17, and trained stimuli, F(1, 171) = 5.40, p = .021, η p 2 = .031, and a significant Time × Condition interaction, F(1, 171) = 9.07, p = .003, η p 2 = .05. The Time × Condition effect was significant for trained stimuli, F(1, 171) = 8.26, p = .005, η p 2 = .046, and for untrained stimuli (generalization), F(1, 171) = 4.78, p = .03, η p 2 = .027. Patients in the experimental condition changed from a small approach bias to a strong avoidance bias for alcohol, and the control group changed from a small approach bias for alcohol to no bias (Fig. 1). For soft drinks, the only significant effect was a Time × Condition interaction, F(1, 171) = 10.4, p = .002, η p 2 = .06; the three-way interaction of Time × Condition × Trained Stimuli was the only other effect with an F value greater than 2, F(1, 171) = 2.3, p = .13, η p 2 = .01. For trained stimuli, the Time × Condition effect was not significant, F(1, 171) = 2.4, p = .12, η p 2 = .01, nor was the main effect of time (F < 1). For untrained stimuli, the Time × Condition effect was significant, F(1, 171) = 11.7, p = .001, η p 2 = .07, combined with a small main effect of time, F(1, 171) = 2.87, p = .09, η p 2 = .02.
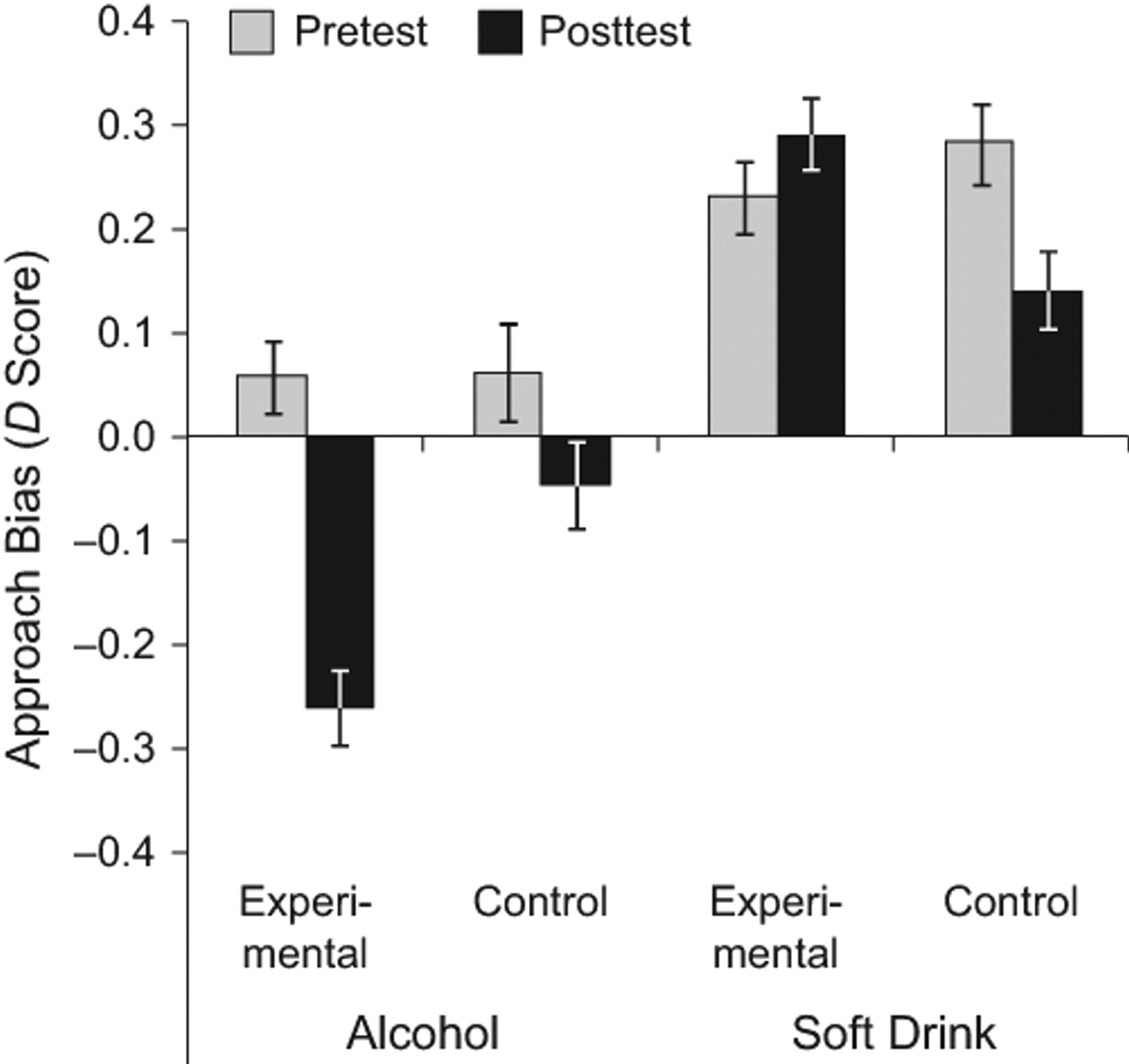
D scores on the alcohol approach/avoidance task for participants in the two groups (experimental and control) as a function of the type of picture (alcohol or soft drink). D scores were derived at pretest and posttest from the difference between mean response latencies for avoidance movements to pictures (pushing a joystick) and approach movements to pictures (pulling a joystick); a positive value indicates an approach bias, and a negative value indicates an avoidance bias. Error bars indicate ±1 SEM.
Patients in the experimental group showed a small increase in their approach bias for soft drinks, and the approach bias for soft drinks in the control group decreased (Fig. 1). Hence, in the control group, the approach bias for both alcohol and soft drinks decreased. However, in the experimental condition, the approach bias for alcohol changed into a strong avoidance bias, which generalized to untrained stimuli and was accompanied by a small increase in the approach bias for soft drinks.
IAT
IAT scores were analyzed with a 2 (time: pretest, posttest) × 2 (condition: experimental, control) ANOVA. A main effect was found for time, F(1, 179) = 21.9, p < .001, η p 2 = .11, qualified by a significant Time × Condition interaction, F(1, 179) = 26.2, p < .001, η p 2 = .13. At pretest, both groups demonstrated strong alcohol-approach associations. At posttest, the experimental group showed strong alcohol-avoidance associations, but the control group still showed strong alcohol-approach associations (Fig. 2).
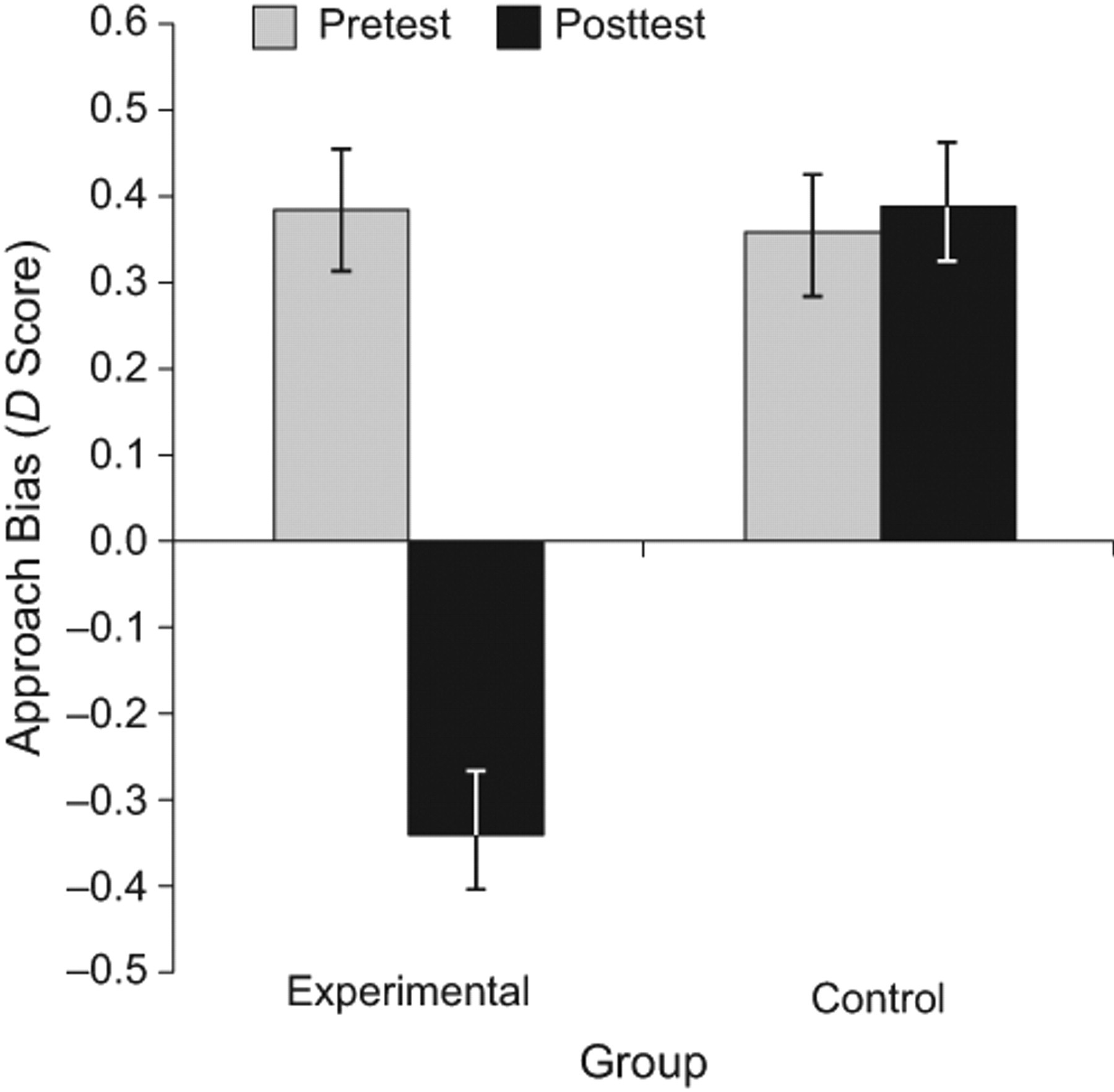
Mean D scores on the Implicit Association Test for participants in the two groups (experimental and control) at pretest and posttest. D scores were within-subjects standardized difference scores, in which the speed of classifying alcohol and approach words together and classifying soft-drink and avoidance words together was subtracted from the speed of classifying alcohol and avoidance words together and classifying soft-drink and approach words together. A positive value indicates an approach bias for alcohol, and a negative value indicates an avoidance bias. Error bars indicate ±1 SEM.
Craving
Subjective craving was analyzed with a 2 (time: pretest, posttest) × 2 (drink: alcohol, soft drink) × 2 (condition: experimental, control) ANOVA. There were significant main effects for time, F(1, 194) = 6.1, p = .014, η p 2 = .03, and drink, F(1, 194) = 364, p < .001, η p 2 = .65, and interactions between drink and time, F(1, 194) = 16.8, p < .001, η p 2 = .08, and drink and condition, F(1, 194) = 6.1, p = .014, η p 2 = .03. The interaction between drink, time, and condition was marginally significant, F(1, 194) = 3.4, p = .069, η p 2 = .02. Follow-up analyses (see Fig. 3) indicated that craving for alcohol went down in the experimental group, t(99) = 2.01, p = .047, d = 0.20, but remained constant in the control group. However, the corresponding interaction between condition and time was not significant (p = .13, η p 2 = .012). Craving for soft drinks increased in both groups—experimental: t(99) = 3.80, p < .001, d = 0.38; control: t(95) = 2.81, p = .006, d = 0.29; there was no significant interaction between condition and time (p = .20, η p 2 = .01). Note that subjective craving for alcohol was low, as is often observed in clinical studies (cf. Schoenmakers et al., 2010).
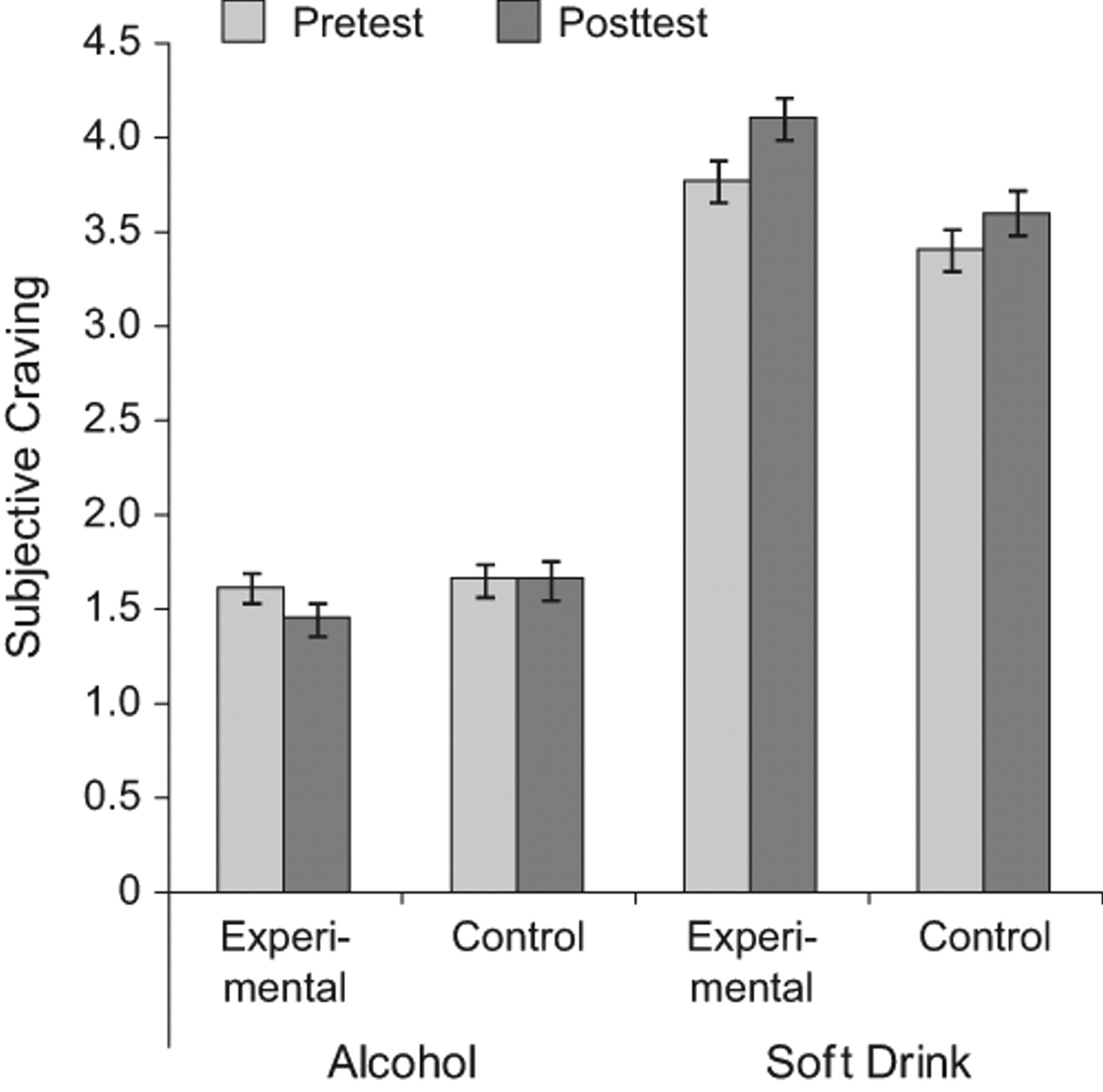
Mean subjective craving scores for alcohol and soft drinks at pretest and posttest for participants in the two groups (experimental and control). Error bars indicate ±1 SEM.
Clinical outcome
One-year clinical outcomes were obtained from 86% of the patients. Conservative ITT analysis indicated that 59% (63 of 106 patients) of the control group, and 46% (50 of 108 patients) of the experimental group had relapsed, χ2(1, N = 214) 3.71, p = .057. This marginally significant difference in outcome could have been caused by many variables, including the experimental CBM. A logistic regression analysis was performed; this analysis included gender, psychopathology (determined using the Beck Depression Inventory and SCL-90-R), and alcohol-related variables (Table 2). Gender and condition were significant predictors of relapse, with women doing better than men and with patients in the experimental group doing better than men and patients in the control group. 2 The interaction between gender and condition was not a significant predictor of outcome (p > .40).
Logistic Regression Results for Treatment Outcome 1 Year After Treatment Discharge
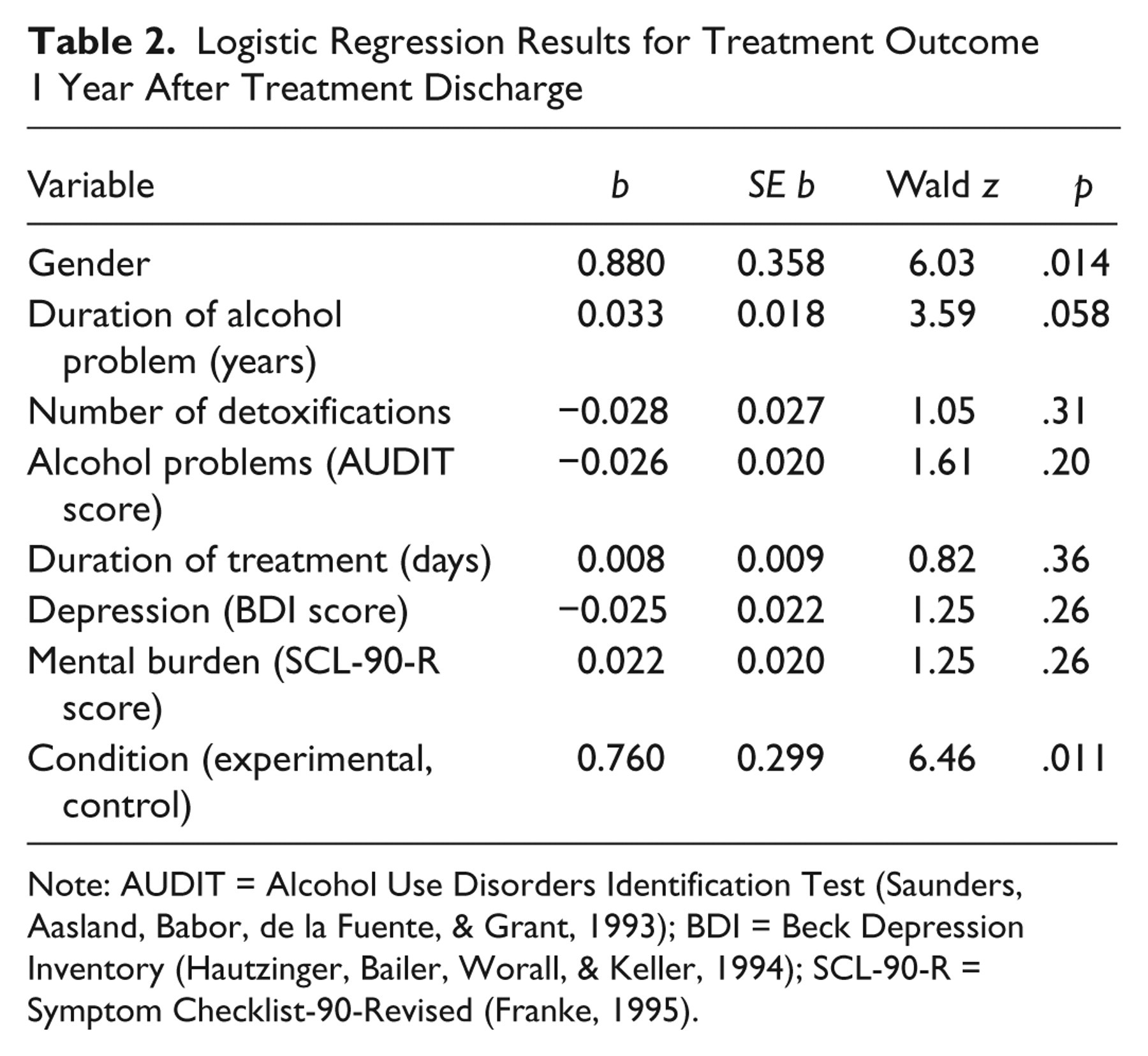
Note: AUDIT = Alcohol Use Disorders Identification Test (Saunders, Aasland, Babor, de la Fuente, & Grant, 1993); BDI = Beck Depression Inventory (Hautzinger, Bailer, Worall, & Keller, 1994); SCL-90-R = Symptom Checklist-90-Revised (Franke, 1995).
Finally, we tested whether the change in cognitive variables (AAT or IAT) mediated treatment outcome (MacKinnon, 2008). Although treatment group significantly predicted the mediators (results in line with the group differences described previously), these potential mediators did not significantly predict treatment outcome when added to the logistic regression (for both variables, p > .50). Hence, mediation of the effect of condition on treatment outcome by changes in cognitive variables was not confirmed.
Discussion
Taken together, our results indicate that a brief CBM intervention aimed at modifying automatically activated action tendencies in alcoholic patients changed their approach bias for alcohol to an avoidance bias, with generalized effects across stimuli and measures. In addition, this minimal intervention appeared to improve treatment outcome a year later. This finding adds to the recent evidence that CBM may have clinical utility in treating anxiety (Amir et al., 2009) and alcohol abuse and dependence (Fadardi & Cox, 2009; Schoenmakers et al., 2010).
How could this brief CBM intervention have such strong effects? The brief CBM was successful in changing automatic approach tendencies, with generalized effects. A similar generalization of training effects to a different assessment procedure was not found in attentional retraining in alcoholic patients, although closer generalization to untrained stimuli within the same task was found (Schoenmakers et al., 2010). Perhaps retraining of action tendencies has stronger effects than retraining of attentional bias. This was also suggested by our recent study, in which generalized effects were found in students after a single session (Wiers et al., 2010), an effect not found for attentional retraining (Field et al., 2007; Schoenmakers, Wiers, Jones, Bruce, & Jansen, 2007). Targeting action tendencies may have strong effects because they relate to a motivational state at the heart of an emotional response (Frijda, 1986, 2010).
A related question concerns the crucial ingredient of the CBM procedure used. One possibility is that the pushing movement on the joystick is crucial, a notion in line with theories of embodied emotion and cognition. These findings have been explained by the bidirectional nature of associations (Strack & Deutsch, 2004). In the domain of alcohol consumption, men who were action primed by lifting a glass of beer drank more in a subsequent taste test than men who leaned toward the glass (Palfai, 2006). However, other researchers have argued that not movements, but associations between the object and the concepts of approach or avoidance are crucial (Krieglmeyer, Deutsch, De Houwer, & De Raedt, 2010; Lavender & Hommel, 2007). There is some evidence that heavy drinkers are ambivalent, holding both appetitive-approach and negative-avoidance associations (Stritzke, McEvoy, Wheat, Dyer, & French, 2007). The finding that the alcohol-avoidance training with the AAT had strong effects on the IAT suggests that the effects are indeed to be found in changes in relative accessibility of alcohol-avoid versus alcohol-approach associations, but this interpretation leaves unanswered whether the arm movement or zooming feature of the AAT is crucial to inducing this effect.
The next question is how this change in automatically activated approach tendencies may have caused a beneficial change in treatment outcome. First, it should be noted that we did not find evidence that the change in approach tendencies mediated the change in treatment outcome. Until now, very few studies on CBM reported significant mediation by the changed cognitive process (MacLeod, Koster, & Fox, 2009). One reason for this failure to find mediation may lie in the nature of the assessment instruments, which can discriminate groups but are not yet optimal for detecting change within an individual (MacLeod et al., 2009). In addition, in the present study, the outcome variable was binary, which reduces the power to detect mediation, and adequate data on the change in cognitive bias were missing from 15% to 20% of the patients. Hence, it is conceivable that mediation of clinical outcomes by changes in cognitive processes can be detected in future studies, but until then we can only speculate about the working mechanism underlying the training’s effect on clinical outcome. One possible mechanism could be that it made patients profit more from other treatment components.
Although the present study found promising results, two limitations should be noted. First, the study was primarily designed as an experimental study on cognitive-motivational mechanisms, and mediation of clinical outcomes by changes in cognitive processes was not found. Therefore, results regarding clinical outcomes should be regarded as promising and in need of further experimental testing, including estimation of survival curves. Second, we did not assess action tendencies for alcohol later during treatment or at follow-up, which would be interesting for future studies to investigate.
The present findings raise a number of follow-up issues at different levels of description. First, given our previous finding of genetic moderation of the approach bias (Wiers et al., 2009), it would be interesting to test whether training outcomes are also genetically moderated. Second, follow-up studies could investigate neurocognitive effects of the training. Third, the measures used to assess relatively automatic approach tendencies for alcohol are not process pure and could be decomposed to investigate the differential effects of training on the associative and controlled processes involved (Sherman et al., 2008). Fourth, it would be fruitful to study the extent to which modification of one bias (e.g., approach bias) also changes a related bias (e.g., attentional bias).
The present findings also raise a number of practical questions for further clinical applications. For example, what is an optimal number of training sessions, and how should they be optimally spaced in time? Moreover, the fact that CBM is computerized generates new possibilities: for example, the Internet could be used to reach many more patients in need of intervention. The findings reported here may give rise to new intervention studies in which alcoholic patients are first retrained in the clinic and then continue at home over the Internet, a process which may help in the transfer from the clinic to the outside world. Finally, retraining procedures can also be tested for other addictive behaviors if similar cognitive biases are found. In conclusion, a brief intervention can successfully change alcoholic patients’ alcohol-approach bias and may improve treatment outcome.
Footnotes
Acknowledgements
The authors thank Maarten Koeter and Brian Nosek for statistical advice; Frank Leonhardt for programming; and Malte Friese, Thomas Gladwin, Wilhelm Hofmann, Kristin Lindgren, Elske Salemink, Jason Sharbanee, Alan Stacy, and Marcella Woud for comments.
The authors declared that they had no conflicts of interest with respect to their authorship or the publication of this article.
Reinout W. Wiers is supported by Vici Award 453.08.01 from the Netherlands Organisation for Scientific Research (NWO).
1.
In addition, the zooming effect disambiguates the alcohol-AAT. Without the zooming feature, pushing the joystick in response to a picture of alcohol, for example, can be interpreted as avoidance (with respect to the body) or as approach (with respect to the alcohol). However, with the zooming feature, this ambiguity no longer exists (see Rinck & Becker, 2007, for more detail).
2.
In addition to the ITT analysis, we analyzed treatment outcomes for patients for whom we had 1-year follow-up results. This analysis yielded the same conclusions (see Table S5 in the Supplemental Material).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.