
Abstract
Recent years have seen a surge in the popularity of interventions that target common distortions in thinking (cognitive-bias modification, or CBM). Although there is evidence of their effectiveness as add-ons to regular treatment in alcohol addiction, the effects are typically small, and recent findings from lab studies have called into question the dominant theoretical underpinnings of CBM. We provide a novel theoretical approach in terms of automatic inferences that integrates previous findings and suggests ways to improve CBM into ABC training. In ABC training, patients are trained in the context of personally relevant antecedents (A) to make behavioral choices (B) that accord with patients’ health goals in light of their consequences (C). We discuss preliminary evidence suggesting that ABC training might be a useful tool in the treatment of addictions and related disorders.
Keywords
Addictions are among the most frequent mental disorders, with tremendous costs for the individual and society (Effertz & Mann, 2013). Yet current treatment approaches are limited. For example, the majority of patients treated for alcohol use disorders relapse within a year (Cutler & Fishbain, 2005). Not surprisingly, researchers are trying to develop more effective interventions based on advancements in psychological science. One promising class of new interventions concerns varieties of cognitive-bias modification (CBM). These procedures were initially based on the notion that addiction is often maintained through automatic processes (Stacy & Wiers, 2010; Tiffany, 1990). CBM was developed to change automatic cognitive biases, which could supplement treatment targeting more controlled cognitive-motivational processes.
Despite its promise, the empirical evidence supporting CBM’s effectiveness has been mixed. As a consequence, both the underlying mechanisms of CBM as well as its clinical value have been questioned. We review recent findings and propose a new theoretical framework that addresses previous concerns and suggests ways to improve CBM. Specifically, we propose a novel approach to CBM that involves training personally relevant behavioral choices (B) triggered by personally relevant antecedent cues (A) that have health-relevant consequences (C).
Theoretical Background of CBM and Clinical Effects
CBM was initially developed as a research tool to test the role of cognitive biases (i.e., systematic distortions in mental processes) in predicting abnormal behavior (originally in the context of anxiety). Addiction research had demonstrated biases in selective attention, memory retrieval, and action tendencies (Stacy & Wiers, 2010; Wiers, Gladwin, Hofmann, Salemink, & Ridderinkhof, 2013). Different methods have been developed to manipulate these biases to experimentally test their impact on addiction-relevant behaviors (for a review, see Wiers et al., 2013). For example, in initial studies, healthy volunteers (students who drank) were trained to selectively focus attention away from, instead of toward, alcohol-related cues. Training attention away from alcohol cues reduced consumption in an ensuing taste test (Field & Eastwood, 2005). Subsequent studies of CBM effects in clinical samples (the next phase of intervention development; Sheeran, Klein, & Rothman, 2017; Wiers, Boffo, & Field, 2018) demonstrated that adding CBM to the treatment of alcohol use disorders reduced relapse (Eberl et al., 2013; Rinck, Wiers, Becker, & Lindenmeyer, 2018; Schoenmakers et al., 2010; Wiers, Eberl, Rinck, Becker, & Lindenmeyer, 2011).
Despite these encouraging findings, a first meta-analysis (summarizing results over multiple empirical studies) suggested that CBM influenced cognitive biases (e.g., the relative speed of approaching vs. avoiding images of alcohol) but that these changes did not translate into clinically relevant outcomes (Cristea, Kok, & Cuijpers, 2016). However, this meta-analysis combined qualitatively different types of studies: proof-of-principle studies (with student volunteers not motivated to change) and randomized controlled trials (RCTs) in clinical samples. These represent two different phases of intervention development (Sheeran et al., 2017; Wiers et al., 2018). Whereas proof-of-principle studies test potential mechanisms, clinical RCTs provide additional insights into factors to be considered for effective treatments. Indeed, when considered separately, RCTs in clinical samples showed that adding CBM to treatment resulted in long-term improvements of treatment outcomes (Wiers et al., 2018). A recent Bayesian meta-analysis including only clinical RCTs (Boffo et al., 2019) confirmed these findings. Thus, CBM appears to be more effective in clinical samples than in proof-of-principle studies with nonclinical volunteers. Preliminary evidence further indicated that CBM is less effective when provided online than in a clinical context (Wiers et al., 2018). This suggests that additional factors (i.e., motivation for change, clinical context) should be considered when developing and implementing CBM.
In the current article, we build on previous findings and on basic research into cognitive mechanisms underlying CBM and provide a new theoretical perspective that addresses previous inconsistencies while offering new guidelines to improve the effectiveness of CBM. In what follows, we describe this perspective and provide preliminary evidence to support it. We then discuss its relevance for the development of more effective CBM applications and suggestions for further research.
New Theoretical Perspective on CBM’s Mechanisms
Initial CBM research was rooted in dual-process models and developed to target distortions in automatic mental processes drawing on associative representations (Stacy & Wiers, 2010; Wiers et al., 2013). Accordingly, CBM would change dominant associations underlying mental disorders (e.g., stronger links in memory between representations of alcohol and approach tendencies than between alcohol and avoid tendencies; Fig. 1, top row). However, recent studies yielded results that do not fit well with associative explanations. For instance, repeated avoidance of addiction-related stimuli in the lab does not always translate to changes in addictive behavior. Rather, the effects depend on important moderators such as beliefs about the implications of the learned relation (e.g., the belief that avoiding alcohol helps one refrain from drinking; see Van Dessel, Hughes, & De Houwer, 2019). Moreover, approach–avoidance effects can be based on verbal instruction rather than on extensive training (Van Dessel, De Houwer, Gast, & Smith, 2015), and change requires awareness of relevant contingencies (Van Dessel, De Houwer, & Gast, 2016).
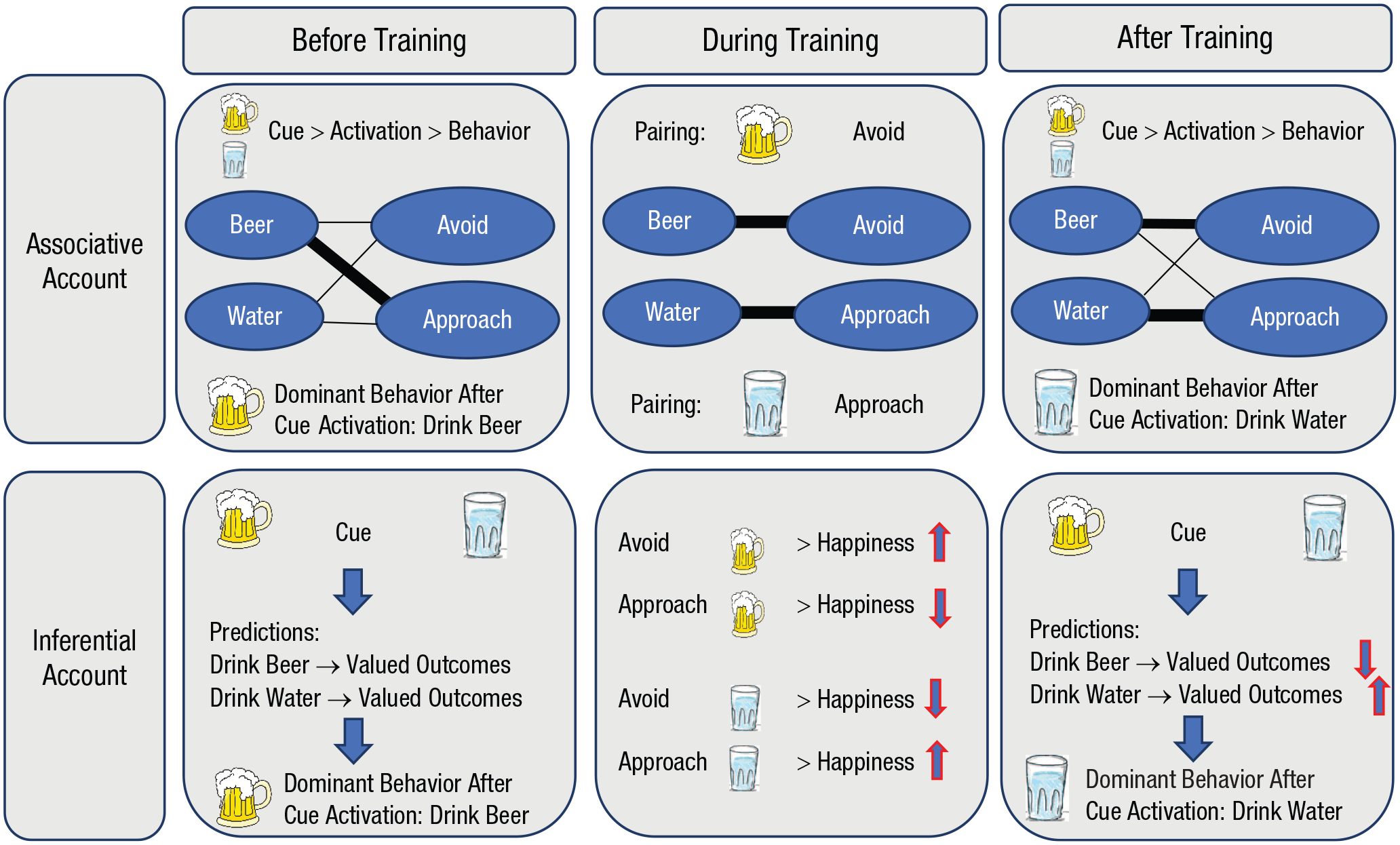
Associative and inferential accounts of the effects of cognitive-bias modification on alcohol consumption.
These findings are difficult to reconcile with an associative account and are more in line with an inferential account (for a review, see Van Dessel et al., 2019). Accordingly, CBM works not by replacing one association (alcohol approach) with a new association (alcohol avoidance) but through changes in propositional representations containing information about how concepts are causally related. Specifically, CBM (e.g., alcohol-avoidance training) invokes propositions about the contingencies between stimuli (e.g., alcohol), responses (e.g., avoidance), and outcomes (e.g., positive effects) that translate into behavior. From the inferential perspective, maladaptive behavior does not reflect automatic activation of mental associations between stimuli and responses as suggested by associative accounts (and the compulsive-habit accounts of addiction; see Hogarth, 2020). Rather, it reflects goal-driven inferences that are learned and evoked on the basis of beliefs about their instrumental relevance to people’s goals (cf. Kruglanski & Szumowska, 2020; Moors, Boddez, & De Houwer, 2017).
From this perspective, contextual cues, which can be external (e.g., the sight of beer) or internal (e.g., stress, in case the person often drinks to cope with stress), might automatically trigger approach tendencies in a heavy drinker because of expected desirable outcomes (e.g., positive affect; Fig. 1, bottom row). Although current CBM interventions based on associative accounts are intended to evoke automatic changes in associations through repeated pairings (e.g., alcohol–avoid), the inferential approach suggests that CBM interventions might be more effective if they are designed to automatize adaptive goal-directed predictions (Van Dessel, Hughes, & De Houwer, 2018). For instance, during alcohol-avoidance training, participants may learn new inferences about action tendencies (e.g., alcohol avoidance) that would result in valued outcomes (e.g., abstinence or recovery). These inferences can facilitate the implementation of similar actions (e.g., avoid) when participants are confronted with similar contextual cues (e.g., alcohol) in the future. When the inferences are well practiced (i.e., automatized), they will be more readily available and translated into behavior.
In the following section, we explore the implications of this inferential account for the development of more effective CBM interventions in clinical settings.
Toward More Effective CBM: ABC Training
We propose three theory-based adaptations of original CBM and explain them in relation to approach-bias retraining. This variety of CBM started with a proof-of-principle study (Wiers, Rinck, Kordts, Houben, & Strack, 2010) in which students were trained to avoid alcohol and approach nonalcohol drinks. Specifically, using a joystick, they pulled or pushed pictures that appeared on a computer screen depending on the format of the picture (e.g., pull landscape-format pictures, push portrait-format pictures). The movement was followed by a congruent zoom effect: zoom in after pulling (approach) and zoom out after pushing (avoidance). In the experimental condition, participants pushed away (avoided) most alcohol pictures and pulled (approached) most soft-drink pictures. In the other condition, this was reversed. The results showed that (a) participants who had pushed alcohol pictures were faster to categorize alcohol words with avoidance (in an Implicit Association Test) than participants who had pulled alcohol pictures and that (b) heavy-drinking students who had successfully been trained to avoid alcohol drank less alcohol in a subsequent taste test than students trained to approach alcohol. In subsequent clinical RCTs, alcohol-avoidance training was tested in patients treated for alcohol use disorders (Eberl et al., 2013; Rinck et al., 2018; Wiers et al., 2011). In these large RCTs, patients were trained during multiple sessions (4–12) to avoid alcohol in addition to receiving standard treatment. One year later, the relapse rate was around 10% lower among patients who received alcohol-avoidance training compared with patients who received no training or sham training. A recent small independent clinical RCT indicated that CBM effects could be stronger when done during detox (Manning et al., 2016). In contrast, findings for traditional CBM as an add-on to smoking-cessation interventions have been less positive (e.g., Kong et al., 2015; Wittekind et al., 2019). We argue that this difference can be understood from the inferential account and propose three ways to improve CBM.
Change 1: goal-relevant alternative behaviors
In alcohol CBM, a universally relevant behavioral choice is trained: the choice between an alcoholic or nonalcoholic drink. Yet in other addictions, such universally relevant choices are typically not available (e.g., there is no universal alternative to smoking). This might explain why standard CBM was primarily found effective in the treatment of alcohol use disorders, in which a universal alternative choice was trained that fulfills the goal of remaining abstinent. By contrast, in CBM studies of smoking cessation, visually matched alternatives have been used (e.g., somebody holding a pen rather than a cigarette). Although this contrast makes experimental sense, it is hard to imagine how holding a pen represents an alternative goal-relevant behavioral choice. Indeed, when behavioral alternatives were personalized (i.e., smoking was contrasted with alternative actions that address the goals otherwise served by smoking, e.g., running to reduce stress), effectiveness of the intervention increased (Kopetz, MacPherson, Mitchell, Houston-Ludlam, & Wiers, 2017). Hence, the first improvement for CBM is to include a goal-relevant behavioral choice (the B in ABC training): Behaviors leading to personally relevant desirable outcomes should be trained.
Change 2: personally relevant consequences
A second aspect of CBM is that behavioral choices have consequences. Building on the idea that behavior is determined by the automatic prediction of relevant action consequences in relation to current goals (Clark, 2013), we suggest that CBM effects might require learning relevant consequences of behavioral choices. In other words, the person should be able to experience the effectiveness of the alternative behavior to accomplish his or her goals. In clinical treatment in which alcohol-avoidance training is effective, the negative consequences of continued drinking and the positive consequences of abstinence are highlighted. However, this may not be the case outside the clinical context (e.g., in online training independent of treatment). This might explain why regular CBM is more effective in clinical than in nonclinical contexts (Wiers et al., 2018). It further points out that CBM might be more effective if it includes real-life goal-relevant consequences. In a recent proof-of-principle study, this idea was applied to unhealthy eating (Van Dessel et al., 2018), a domain in which regular CBM has proven largely ineffective. Participants performed a task in which they were asked to maximize the health of an avatar representing themselves. On each trial, they would see the avatar stand in front of a refrigerator with healthy or unhealthy food items, and they decided to approach or avoid the items. Crucially, approaching unhealthy foods resulted in negative effects, and approaching healthy foods resulted in positive effects concerning the avatar’s health. Participants who learned these consequences during training were able to implement it successfully in real life: Unhealthy eating was significantly reduced in the consequence-based CBM training compared with a standard avoid-unhealthy-food CBM training and a no-training control condition. This illustrates that adding a relevant consequence (C) might significantly improve the effectiveness of CBM. These consequences can be personalized to fit with people’s goals. For instance, in smoking cessation, in addition to health, other goals might be important, such as saving money or maintaining a more attractive physical appearance. Hence, the second improvement concerns adding consequences to actions in CBM tailored to the patients’ own goals.
Change 3: personally relevant antecedent context
The study discussed above (Van Dessel et al., 2018) suggests a third change that could improve CBM: the antecedent context (A). Participants completed the CBM task in a simulated real-life context in which they were standing in front of a refrigerator. Incorporating these real-life context cues (A: refrigerator) in association with the behavioral choice (B) and the action consequences (C) might facilitate transfer to real life. The real-life antecedent can be a simple stimulus (e.g., a familiar drink, as in original CBM), but it can also be extended to high-risk situations, as they are typically identified during treatment (e.g., a specific location, friend, moment). Importantly, multiple relevant antecedent contexts (and relevant behavioral alternatives) can be identified and trained as part of the intervention, the third proposed change.
To summarize, our proposed ABC training represents a novel, theory-based variety of CBM that involves training goal-relevant behavioral choices (B) triggered by antecedent cues (A) and followed by positive or negative action consequences (C) for the pursuit of specific goals (Fig. 2). Thus, instead of training specific associations determined a priori (e.g., cue-avoidance training in the original CBM, Fig. 1), ABC training aims to automatize behavioral choices relevant to an individual’s goals in specific contexts. All elements (antecedent contexts, behavioral alternatives, and consequences) can be personalized with the help of experienced clinicians in the domain.
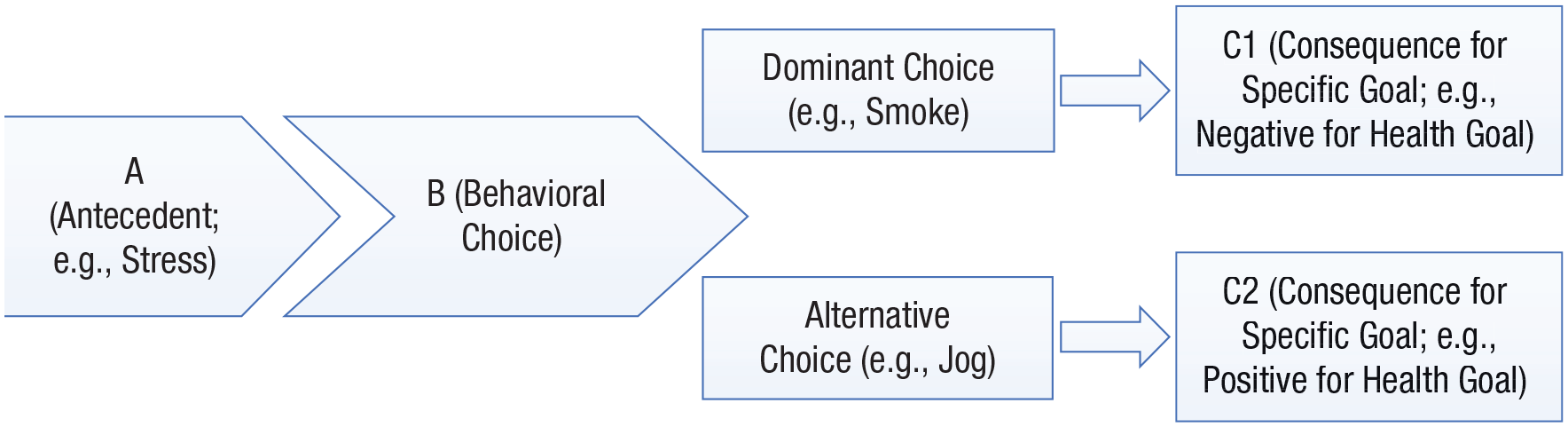
Components of ABC training.
ABC Training Compared With Alternative Therapies
ABC training bears resemblance to (a) cognitive behavior therapy (Beck & Dozois, 2011) and (b) treatments that involve analysis of maladaptive behavior as a function of the antecedents that precede it and consequences that follow it (Dyer, 2013). Despite the apparent resemblance, ABC training might significantly enhance the effectiveness of these treatments. First, it combines these two approaches. Second and more importantly, it targets automatization of adaptive inferences and related behaviors, which may be crucial in revising habitual behavior that is difficult to change (cf. Marien, Custers, & Aarts, 2019). From this perspective, patients’ goals and personally relevant means to achieve these goals should be identified and related to risk situations. At this point, personally relevant ABC training can be implemented to automatize inferences about goal-relevant action–outcome combinations in relevant contexts. Similar approaches that attempt to create specific if-then plans for risk situations (implementation intentions) have proven effective in several domains of health behavior (Gollwitzer & Sheeran, 2006). However, the implementation of such action plans is effortful, at least in the initial phases. By contrast, ABC training involves practice that aims to automatize behavioral choices and to reduce the amount of effortful control required. This is particularly important because a common problem in traditional therapy is that patients (like students) often experience difficulties doing their homework, in this case, practicing alternative adaptive-choice behaviors. Because ABC training can be delivered online, it increases the chance that patients practice the relevant alternative behaviors.
Compared with traditional CBM, which is often experienced as rather meaningless by patients, personalized ABC training would seem a more meaningful complement to therapy. The large majority of people suffering from addictions do not seek professional help, but many do seek e-therapy. Current e-therapy is effective for participants who complete the intervention, but premature dropout is the rule rather than the exception (Riper et al., 2018). Furthermore, the effects of conventional online CBM in addiction are weak at best (Wiers et al., 2018). By adding ABC training to guided e-therapy, a more engaging and effective intervention could be created. Clearly, further research is needed to test the effects of ABC training in clinical and online contexts, but the theory-based ingredients and preliminary results show promise (Kopetz et al., 2017; Van Dessel et al., 2018).
Conclusion
CBM training has shown promise as an add-on to the clinical treatment of alcohol addiction. However, recent findings are difficult to reconcile with the original theoretical perspective. To address these issues, we propose a new theoretical perspective based on an inferential account that integrates previous findings and suggests new implications for the development of effective CBM interventions. Specifically, we suggest that training can be optimized in a manner in which contextual antecedents (A) trigger an adaptive behavioral choice (B) in light of goal-relevant health-related consequences (C). New ABC training might serve as a tool in regular therapy to foster automatic behavioral choices in line with patients’ health goals. This suggestion is supported by preliminary findings but awaits empirical support from large clinical trials.
Finally, it is important to note that our perspective does not imply that nonvoluntary processes play no role in addiction. There is clear evidence that addiction-related cues, like other rewards, attract and capture attention (Anderson, 2016; Watson, Pearson, Wiers, & Le Pelley, 2019). The effects of CBM appear to go beyond these initial attentional processes (Wiers, van Gaal, & Le Pelley, 2020). For example, the first small RCT on attentional retraining (a type of CBM) in alcohol-dependent patients found no effect of training on speeded detection (200 ms) but did find an effect on later attentional capture (500 ms) and on relapse (Schoenmakers et al., 2010). Thus, early cognitive biases may be difficult to change, but by training participants to respond differently to cues, CBM may improve clinical outcomes. It is an interesting question for further research whether long-term abstinence and related changes in one’s priorities and life goals could also change these early-stage cognitive biases.
Recommended Reading
Boffo, M., Zerhouni, O., Gronaua, Q. F., van Beek, R. J. J., Nikolaou, K., Marsman, M., & Wiers, R. W. (2019). (See References). A meta-analysis of cognitive-bias modification (CBM) studies in addiction (including only studies with a behavior-change goal) that showed a small effect of CBM as an add-on to regular treatment on bias and relapse.
Kopetz, C., MacPherson, L., Mitchell, A. D., Houston-Ludlam, A., & Wiers, R. W. (2017). (See References). The first CBM study with personalized alternatives to smoking.
Van Dessel, P., Hughes, S., & De Houwer, J. (2018). (See References). The first proof-of-principle study directly comparing CBM with consequences with regular CBM.
Van Dessel, P., Hughes, S., & De Houwer, J. (2019). (See References). A theoretical article comparing the inferential account with the associative account of cognitive training.
Wiers, R. W., Boffo, M., & Field, M. (2018). (See References). An article on the importance of distinguishing between proof-of-principle studies in healthy volunteers and clinical trials in patients when integrating research results in CBM and other domains.
Footnotes
Acknowledgements
R. W. Wiers and P. Van Dessel contributed equally to this article.
Transparency
Action Editor: Robert L. Goldstone
Editor: Robert L. Goldstone