
Abstract
Keywords
Introduction
When the human immunodeficiency virus (HIV) emerged, people living with HIV (PLHIV) were stigmatized, rejected, and discriminated against even by health professionals who initially had limited knowledge about the course of this disease. 1 This adversely affected individuals, considering nurses and physicians played a fundamental role in addressing not only the physical health needs but also, the social and spiritual needs of these patients, as Ajisegiri et al 2 mentioned. In other words, the health professionals’ knowledge, attitudes and beliefs primarily determined the success of the care provided to these patients.
Stigma related to HIV infection and Acquired Immunodeficiency Syndrome (AIDS) is closely associated with social determinants of health, social power structures, and prejudices among different socioeconomic statuses. It is also associated with how disease disproportionately affects these populations, contributing directly to increased inequality between these communities. Therefore, social factors such as economic poverty, cultural norms, and gender are facilitators of stigma. On the other hand, minority groups such as ethnic, sexual, and immigrants are widely associated with HIV-positive status, even if they do not have the disease. 3
The current literature highlights relevant reports about this subject. For example, in a study published by Sufiawati et al 4 about the knowledge and attitudes of dentists towards PLHIV, the authors found that, in general, attitude and expertise were right, still they report that 1.5% of participants believed that PLHIV should be isolated, 21% would stop treating a patient if they found out they were living with HIV, and 30% felt uncomfortable with these patients. Another study by Sallam et al 5 informed that 27.8% of participants had negative attitudes toward PLHIV. A logistic regression analysis showed that lack of knowledge about the infection was significantly associated with a negative attitude towards them.
Although some studies have demonstrated good attitudes of health professionals towards PLHIV, other studies of the health care setting have shown that stigma attitudes are still notorious. For example, in a survey, 29% of participants did not feel safe buying food from a PLHIV, 31% mentioned that they did not feel comfortable sharing a bathroom with them, and 31% considered that in case of acquiring HIV, their partners would leave them.6,7
In Chile, HIV prevalence has increased in recent years, standing at 0.5 × 105 in the population aged 15 – 49, according to Joint United Nations Programme on HIV/AIDS (UNAIDS) figures. Chile is the country in the Americas region with the most significant increase in cases in the last 5 years, as reported by the Chilean Academy of Medicine, mortality is above the goal proposed by the World Health Organization.8–10 Medical care in Chile for PLHIV is provided through a national strategy that allows universal, quality, and opportunely access, it includes medical care and drug dispensing regardless of whether the patient is affiliated with the public or private health care system. This strategy allows patients to receive care from infectious disease specialists at specialized levels of care but also from general practitioners, family medicine, and other professionals such as nutritionists, nurses, and dentists. 9
Research in Medline and Scielo databases about the attitudes of health professionals in Chile toward PLHIV shows a total of 102 manuscripts. Unfortunately, only one addressed this issue,identifying that interviewees did not express explicit stigmatizing attitudes; still, there was some prejudice towards homosexual subjects, considering them the primary transmitters of HIV. Therefore, the aim of this study was to describe the knowledge and attitudes of health professionals working in Chile toward people living with HIV.
Materials and methods
The reporting of this study conforms to The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines that were created to aid the authors in ensuring high-quality presentation of the observational studies. 11
Study design and data collection
Prospective cross-sectional study. The study was carried out in Chile from January 30, 2021 to December 30, 2021.
Survey questionnaire and study sample
The calculation of sample size was by Convenience Sampling Method. For analysis and considering that the number of professionals registered in the Chilean Ministry of Health exceeds 10,000 individuals, the infinite population equation was used, finally having a representative sample of 384 health professionals.
n = Z2.p.q/d2; n = Z2.(p). (1 − p)/d2; n = (1.96)2. (0.5). (1 − 0.5)/(0.5)2; n = (3.84). (0.5). (0.5)/.0025; n = 0.96/0.0025; n = 384
n = sample size. Z = critical Z score-value, or confidence level. d = absolute precision. p = approximate proportion of the phenomenon under study in the reference population. q = proportion of the reference population that does not present the phenomenon under study (1-p).
Selection criteria were established to carry out the survey, including both national or foreign health professionals working in Chile during the study period who expressed freely and voluntarily interest in participation. Health science students and professionals who performed purely administrative tasks and had no contact with PLHIV were excluded.
The “HIV/AIDS Questionnaire for Health Care Providers and Staff”, developed by the International Planned Parenthood Federation (IPPF), which has been validated numerous times and translated into different languages, was used.12,13 Additionally, a pilot test was conducted with 50 participants, and internal consistency was measured by exploratory and confirmatory factor analysis, finding the same structure proposed in the original study. Likewise, Kaiser-Meyer-Olkin measure of sampling adequacy was 0.88, and Bartlett’s test of Sphericity with a significance <0.001. The anti-image correlation matrix had all values above 0.89, verifying construct validity. In addition, internal consistency was measured by Cronbach's alpha of the questionnaire, which was 0.89.
The instrument was configured in a Google form and distributed through social network groups on platforms such as WhatsApp, Instagram, Facebook, and LinkedIn. These particular social networks were exclusively chosen for the study, and access to the associated accounts was restricted solely to the authors. To protect participants' confidentiality, identification data was not requested and email address was not stored.
Bias
To reduce the risk of measurement bias. the questionnaire was validated qualitatively and statistically. To reduce the risk of random error, a sample by sample was used for convenience with a sample calculation that was representative of the target population.
Statistical analysis
The normality of quantitative variables was tested using the Kolmogorov–Smirnov test. Data were presented as mean ± standard deviation (SD) for continuous variables and median (interquartile, IQR) for skewed variables. Qualitative variables were summarized using frequency and percentages. Data were analyzed with IBM SPSS (Chicago IL) statistical software version 29.
Ethical statements
This study was approved by the institution ethics review board. The protocol was implemented in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines.
Results
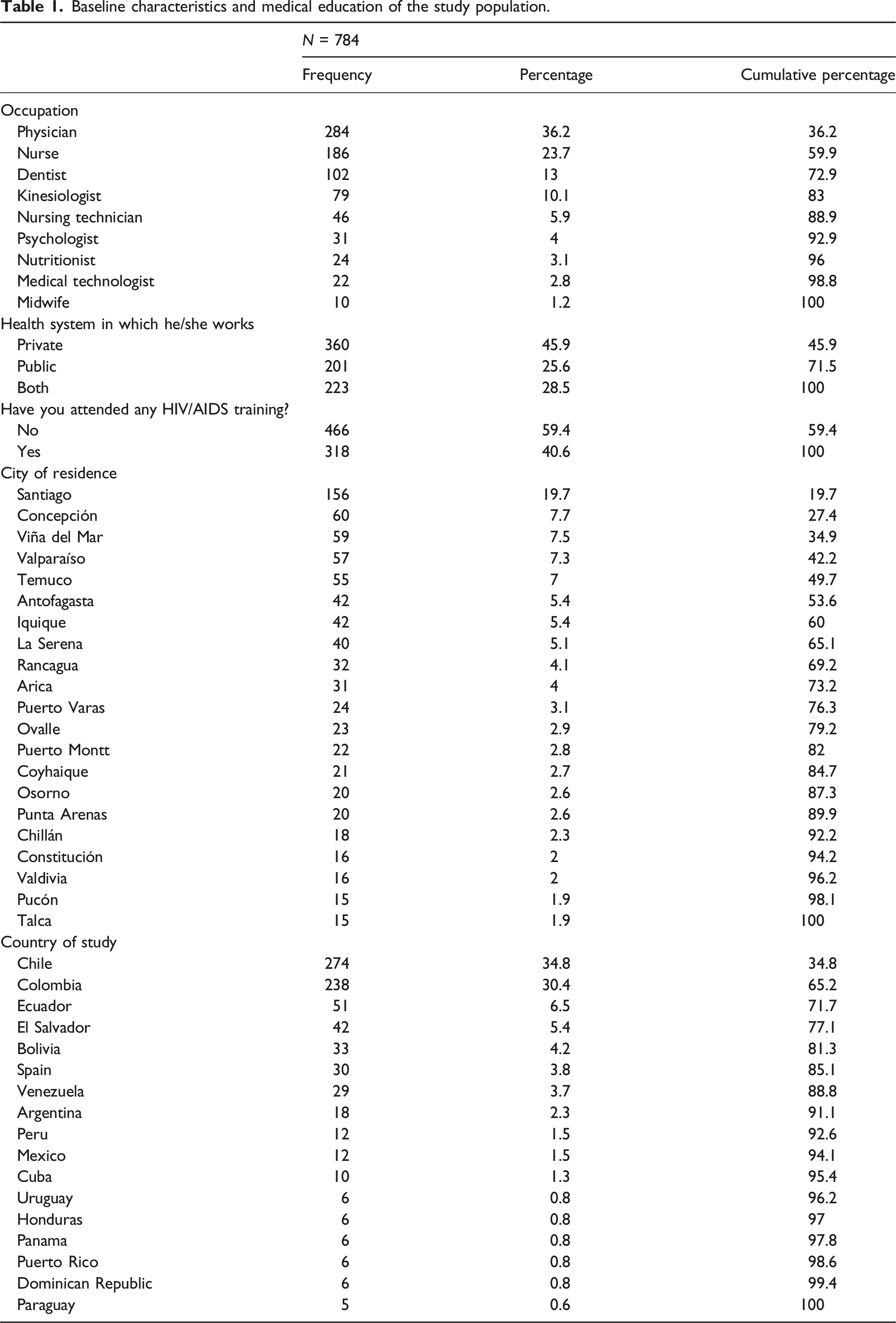
A total of 810 health professionals responded to the questionnaire. Due to incomplete data, 26 forms were excluded, resulting in 784 forms available for the subsequent statistical analysis. Among the participants, 68.4% (n = 536) identified as female, 29.1% (n = 228) as male and 2.6% (n = 20) as other, Age exhibited a nonparametric distribution with a median of 34 years (IQR 24 – 44), and also the years of professional experience with a median of 8 years (IQR = 0 – 16). Regarding professional distribution, 36.2% (n = 284) were physicians, 23.7% (n = 186) nurses, 13% (n = 102) dentists, and the remaining percentage were kinesiologists, midwives, nutritionists, psychologists, nursing technicians, and medical technologists. 45.9% (n = 360) worked in the private health system and 25.6% (n = 201) in the public system. Most participants were from the city of Santiago, with 19.9% (n = 156), Concepción 7.7% (n = 60), 7.5% (n = 59) from Viña del Mar, and 7.3% from Valparaíso (n = 57) (Figure 1). Concerning the participants' countries of study, 34.9% (n = 274) did so in Chile, 30.4% (n = 238) in Colombia, and 6.5% (n = 51) in Ecuador (Table 1). Distribution of participants according to the Chilean region to which they belong. Baseline characteristics and medical education of the study population.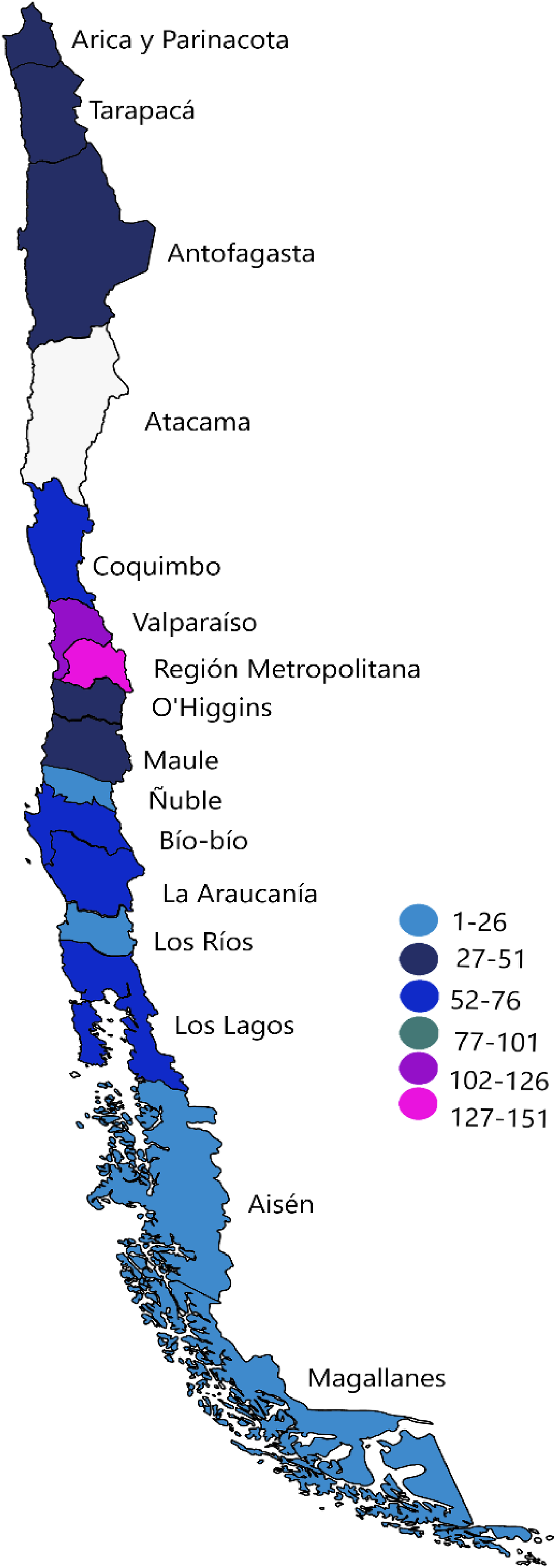
When asking participants if they had met PLHIV outside their professional practice, 70.8% (n = 555) answered yes. When asked about their preparedness to interact with PLHIV in their workplace, 50% (n = 392) felt somewhat prepared, 49.1% (n = 385) very prepared, and 0.9% (n = 7) not at all prepared. In addition, 92.2% (n = 723) commented that they would attend if offered HIV/AIDS training or awareness sessions at work. Also, 98.2% (n = 770) said they had heard about antiretroviral therapy at some time.
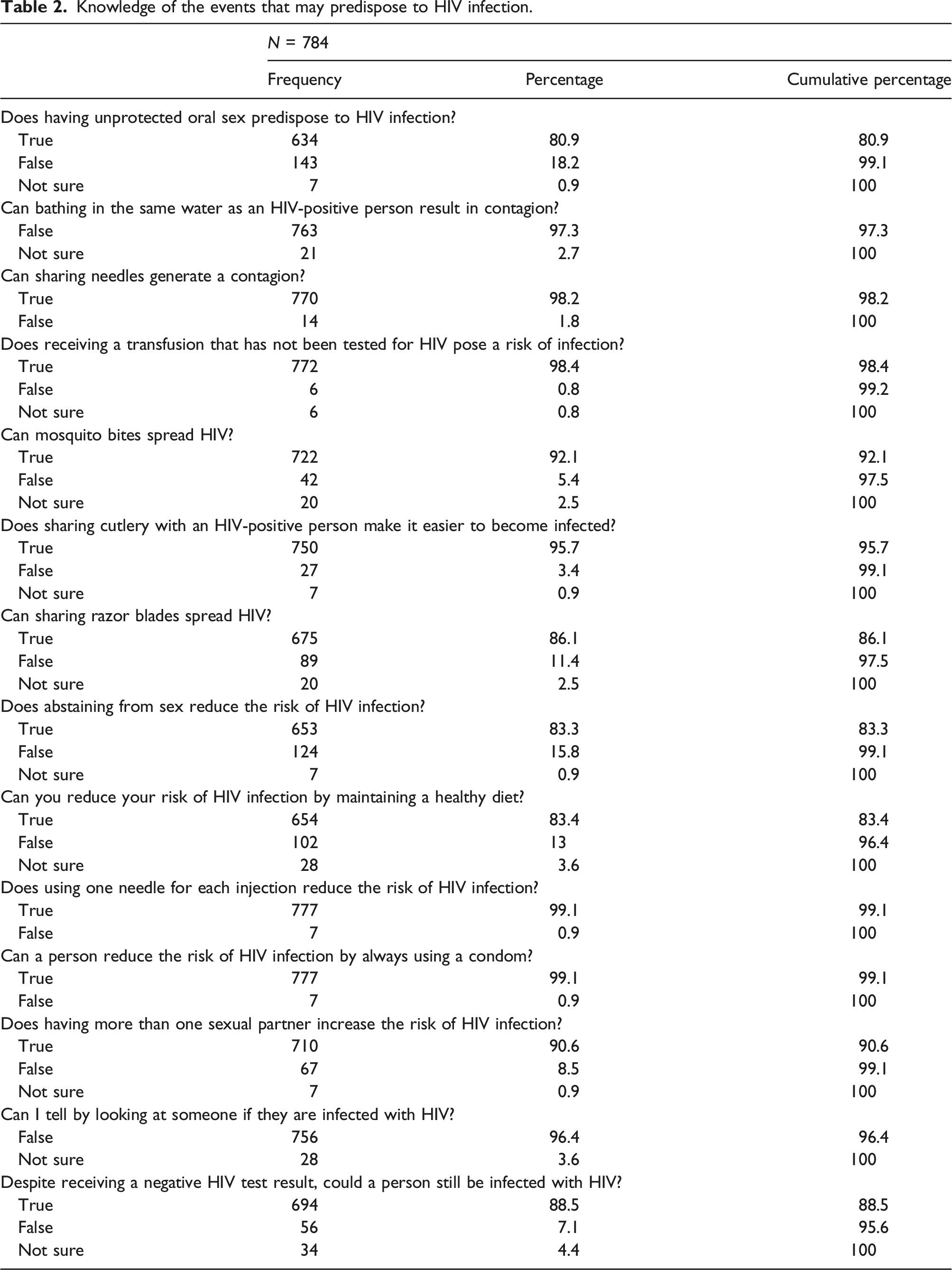
Knowledge of the events that may predispose to HIV infection.
To the question: “If a patient tests positive for HIV, do you think the clinic should inform the patient?”, 100% (n = 784) of respondents agreed. When asked whether the clinic should inform the patient's family, 95.7% agreed, and only 4.3% disagreed. Regarding the opinion of whether or not a woman living with HIV has the right to become pregnant, 86% (n = 674) strongly agreed, and the remaining percentage disagreed or had neutral thinking on the subject. In response to the query of whether an teacher living with HIV should be permitted to continue teaching, 100% (n = 784) agreed. Concerning the belief that HIV infection is due to irresponsible behavior, 26.3% (n = 206) agreed with this statement, 20.7% (n = 162) had neutral attitudes, and 53.1 (n = 416) disagreed.
Among the respondents, 93.8% (n = 736) expressed a willingness to care for a family member with AIDS in their home, and 81.7% (n = 640) would not mind sharing a bathroom with a person with HIV/AIDS. In addition, 21.5% (n = 169) believed that their partners would leave them in case of acquiring HIV infection, while 40.9% (n = 321) thought this would not happen, 77.6% (n = 608) said they would not mind if they found out their food and vegetable provider was living with HIV, while 11.2% (n = 88) had neutral attitudes about this. Also, they were asked whether they considered AIDS God's punishment for immorality, with 99.2% (n = 777) of surveyed disagreeing with this judgment.
Since the participants in the study were healthcare professionals, they were asked about their concerns about the potential for acquiring HIV while providing care to PLHIV. The finding revealed that 69.4% (n = 544) were not concerned, 6.6% (n = 130) had neutral attitudes in this regard, and the remaining 14% (n = 110) expressed worry about acquiring the infection. In addition, 98.3% (n = 771) agreed that health professionals should take the same biosecurity measures with all patients regardless of their HIV status. Furthermore, 86% (n = 674) of participants said they were not concerned that other patients would not want to be attended by them if they knew they care for people with HIV/AIDS. Also, 92.2% (n = 723) were not concerned that other people would think they had HIV because they treated PLHIV. Likewise. 95.5% (n = 749) mentioned that they were not anxious about knowing that the next patient on their care list was living with HIV, and 76.9% (n = 603) of the respondents felt safe taking blood samples from PLHIV.
In inquiring about patients' sexual orientation, 67% (n = 525) considered it necessary. Also, patients' sexual behavior was rated as essential by 82.3% (n = 645). 81.5% (n = 639) of participants felt prepared to inform a patient about a positive HIV test result. Regarding patient counseling, 68% (n = 533) considered women living qith HIV should be advised to use barrier methods such as condoms and other additional contraceptive methods. In addition, 90.4% (n = 709) believed that women living with HIV receiving treatment with antiretroviral drugs during gestation could reduce HIV transmission during pregnancy. Likewise, 80.7% (n = 633) considered that the risk of transmission to the child is reduced if the mother undergoes prenatal check-ups and HIV serology testing.
According to the knowledge about antiretroviral therapy (ART), 96.4% (n = 756) mentioned that this treatment helps people with HIV to live longer, although 90.4% (n = 709) said it could not cure them. 93% (n = 729) answered that ART could decrease the risk of HIV transmission and 39.4% (n = 309) said that this therapy has side effects that make patients feel sick.
Discussion
This study showed that health professionals in Chile have good attitudes and a high level of knowledge about people living with HIV/AIDS. However, when contrasted with the world scientific literature, a study by Dhanya et al 14 involving 206 dentists in India showed that about 70% considered that they would run a higher risk and it would be challenging to manage with personal fears when dealing with patients living with HIV. In contrast to findings of the present study, 86% of participants were not concerned about being thought to be living with HIV themselves because they treat patients living with HIV. In the Indian study, 46.4% of participants agreed that caring for PLHIV might lead other patients to skip their check-ups because of fear. 14 A study by Sufiawati et al, 4 involving dentists from Indonesia, showed that 53% of the respondents had a positive attitude towards patients living with HIV/AIDS, and an equal percentage exhibited positive behavior towards these individuals.
In China, Wu et al 15 revealed that of the 1783 healthcare workers who completed questionnaires, 90% knowledgeable about HIV transmission through blood transfusion, 89% knew about sexual transmission, 90% were aware of perinatal transmission, and only 33% correctly identified that mosquito bites could not transmit HIV. In the study by Sufawati et al 4 mentioned above, 97.6% of the dentists knew that HIV transmission can occur through blood transfusions and 90.9% understood the risk of mother-to-child transmission during pregnancy, delivery and breastfeeding. Shah et al 7 informed that while 74% of those knew that using a condom mitigated the risk of contracting HIV, and 86% knew that PLHIV generally had a healthy appearance, only 69% correctly answered questions about HIV transmission through food, beverages, and mosquito bites. These findings are far from the present study. As previously reported, 98.5% of Chilean health workers knew there is a risk of transmission through transfusions, 99.1% knew that using condoms can avoid sexual transmission, and 92.1% stated that mosquito bites could not transmit HIV. These findings align closely with the results from a survey conducted in South Africa by Famoroti et al 16 reported in a survey made in South Africa, where approximately 98% of the participants exhibited accurate knowledge of HIV transmission, and 91.6% correctly excluded vectors as agents of transmission.
In the present study, 98.3% of participants considered using biosecurity measures regardless of patients’ serological status; similar to reports by Huq et al, 1 where 94% favored this consideration. The same questionnaire was used by Shahar et al 6 in Israel, identifying that 88% of surveyed individuals felt prepared to interact with PLHIV. Of this group, 35% reported feeling very prepared, while 53% indicated being somewhat prepared. These figures were higher in the present study, where 49.1% of professionals feeling very prepared and 50% feeling somewhat prepared to interact with patients living with HIV/AIDS.
Concerning the modes of transmission, in both the Israeli and this study, most participants considered that using a new needle for each injection and using condoms during genital and oral sex can reduce transmission. However, in the Israeli study, 29% of respondents believed that the bite of vectors could transmit the infection. Other statements, such as motherhood in women living with HIV, if a teacher living with HIV should be allowed to teach, or if they were willing to care for someone living with HIV/AIDS in their house, were answered with high acceptance in both studies. 6 Perhaps the most contrasting study found was that by Kabbash et al, 17 where only 24% of surveyed individuals had previously previous contact with patients living with HIV during their work, and 21.3% were concerned about touching the clothing of PLHIV. In addition, 26.4% of participants were worried about dressing the wounds of PLHIV, and 27.4% did not want to obtain a blood sample from these patients. Also, 40% of respondents were unwilling to treat PLHIV. Finally, the same study reported that 78.7% of participants considered PLHIV should be ashamed of themselves.
Other works highlight that professionals who cared for more patients living with HIV for a more extended period and had greater knowledge about HIV/AIDS were less likely to show stigmatizing attitudes towards PLHIV. 18 Additionally, significant improvements have been seen following educational interventions in both the knowledge and attitudes of professionals who have received training in epidemiology, transmission, and treatment of HIV, as well as in the rights of PLHIV, the duties of health professionals, and the use of biosecurity measures.19–21
It is important to comment that the study carried out by Cianelli et al (2011), 12 investigated HIV-related stigma among health workers in Chile. This study showed that there were two main issues related to stigma: the social stigma of discrimination against people living with HIV, and HIV-related health system policies. In the first case, health workers did not recognize stigmatizing attitudes or discriminatory behaviors. Although they recognized that these behaviors and attitudes existed among health professionals, they were mainly motivated by fear of getting sick or contagion. Regarding the second aspect, they stated that changes were needed in the specific policies of continuing education on HIV to allow them to be trained in particular aspects of the disease. 12
This study from 11 years ago, which is of a purely qualitative typology, cannot be compared objectively (quantitatively) with the current one. However, it can be identified that the fear of contagion is still present among health professionals since close to 20% of those interviewed expressed their concern in this regard. Regarding stigma, in general, health professionals had good attitudes toward people living with HIV. But, it is necessary to highlight situations such as that close to 20% believed that their partner would leave them if they acquired HIV; Also, a quarter of those surveyed believed that HIV infection was due to irresponsible sexual behavior and 14% were concerned that patients would not want to see them if they found out that they treated patients living with HIV.
The primary results framed in the objective, which were to describe the knowledge and attitudes of health workers working in Chile towards people living with HIV, were resolved through this study, since the instrument used has a validation for the population, as well as a representative sample size of the population, so it is considered to have internal and external validity. Secondary results, such as stigma situations, could be better addressed from a qualitative approach and, in general, this study could be replicated in other countries, taking into account that the questionnaire must be adapted to each population as it not only requires the language version of each region, but also that some variables may differ from one country to another.
The limitations of this study include the lack of participation from health professionals in certain regions of the country, particularly Atacama and the Island territory, which have their own social and educational characteristics and could have enriched this study. It is also important to emphasize that this study adopts a cross-sectional descriptive approach, rendering it susceptible to biases. Likewise, the findings cannot represent causality and should be interpreted cautiously. Despite this, it is an innovative study for the country that can provide a first assessment of this issue in the region. However, it is important to highlight that this is one of the few studies that have evaluated, with a representative sample, the knowledge and attitudes of health caregivers towards patients living with HIV in Latin America. The study’s findings are of practical importance, providing a foundation for the development of strategies and future projects to improve health care for patients with HIV/AIDS.
Conclusion
Chilean health professionals have good knowledge about HIV and its mode transmission. Also, their attitudes are generally favorable toward people living with HIV. It was observed that professionals in the Chilean health care setting do not have stigmas towards PLHIV, nor do they object against functions such as their job performance or maternity. It also became clear that they are not concerned about caring for these patients, not about being recognized for this work or being associated with PLHIV.
Footnotes
Author contributions
Y.A.P.J., I.D.L.M., J.E.O.C., J.M.F., M.P.B.R. and O.F.M. were responsible for the design of the study and interpretation of data. YAPJ and JEOC led data collection and interpretation. Y.A.P.J., J.E.O.C. and I.D.L.M. performed data analysis. I.D.L.M., J.M.F., M.P.B.R. and O.F.M. participated in the design of the study and interpretation of data. All authors participated in writing the initial draft of the manuscript. All authors participated in writing the final manuscript. All authors read and approved the final manuscript before submission.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.