
Abstract
The aim of the study was to investigate clinical features of patients with AIDS having respiratory symptoms as initial manifestations and help in the early diagnosis. Eighty-eight patients admitted to the Shanghai Pulmonary Hospital were included in the study. General data, clinical manifestations, laboratory tests, chest computed tomography (CT) imaging features, treatments, and prognosis were analyzed. Peripheral leukopenia, lymphopenia, hypoxemia, and reduced percentage of CD4+ T lymphocytes were found in 25.6%, 43.6%, 27.5%, and 94.9% of the patients, respectively. Pneumocystis jirovecii pneumonia (PCP) was the most frequent cause of opportunistic pulmonary infection. Patients with PCP had more bilateral lung involvement and ground-glass shadow in CT manifestations. A follow-up of the 43 patients transferred to the Public Health Center showed improvement in 27 (62.8%), stabilization in 4 (9.3%), worsening in 1 (2.3%), and death in 11 (25.6%) patients. Detailed medical history recording, screening of human immunodeficiency virus antibody, and flow cytometry would improve the diagnostic efficiency of AIDS in patients with diffuse ground-glass shadow in chest CT. Early and empirical treatment could improve the prognosis.
Introduction
Acquired immunodeficiency syndrome (AIDS) is a disease involving cellular immune dysfunction caused by the infection of human immunodeficiency virus (HIV). The diagnosis of AIDS should be made with a comprehensive analysis of the epidemiological history, clinical manifestations, and laboratory tests. Adults, adolescents, and children aged more than 18 months can be diagnosed if they are positive for HIV antibody screening test, supplement test, or HIV isolation test. 1 It is characterized by T lymphocyte damage. HIV mainly invades CD4+ T lymphocytes and consequently induces the reduction or even failure of human immunity. Therefore, patients with AIDS are at high risk of various opportunistic infections and complications of malignant tumors. Pulmonary infection is the most frequent type of opportunistic infection, which includes P. jirovecii pneumonia (PCP),1–3 pulmonary tuberculosis, 4 and other fungal infections. 5 The clinical manifestations of patients with AIDS accompanied by pulmonary infections are generally severe, and the mortality rate of these patients is as high as 20%. 6 Some of these patients are initially admitted to respiratory departments, as the initial manifestations are respiratory symptoms. However, the largest study of patients with AIDS having respiratory symptoms as initial manifestations in mainland China included only 42 patients, 7 and the prognoses of patients during the follow-up were generally not reported. In addition, the other international studies in such patients were rare. In this study, the clinical characteristics, laboratory tests, and imaging features of 88 patients with AIDS having respiratory symptoms as the initial manifestations, who were treated at Shanghai Pulmonary Hospital, were retrospectively analyzed. The findings provided evidence to help in the early diagnosis and timely empirical treatments of these patients, thereby improving disease conditions and winning time for the consequent treatment.
Methods
Patient screening and data collection
The patient screening process is shown in Figure 1. All the patients admitted to the Respiratory Department of Shanghai Pulmonary Hospital from January 2014 to December 2016 received HIV antibody primary screening; 91 patients tested positive and 88 patients positive for confirm test and who met the diagnostic criteria of AIDS were included in the study. 43 patients were transferred to the Public Health Center for further treatment. Three patients were followed up in the outpatient department of the hospital, while 42 patients lost to follow up. The follow-up of the patients via telephone calls was conducted until 30 September 2018. The clinical characteristics, including general data, clinical manifestations, laboratory examination results, and treatments, were obtained from medical records. All patients underwent pulmonary computed tomography (CT), and two experienced radiologists jointly concluded the CT features. Images were reevaluated until consensus was reached when disagreement occurred. The institutional ethics committee of Shanghai Pulmonary Hospital approved the study (2014fk04), and written informed consent was taken from all the participants. Flow diagram of this study.
Diagnostic criteria
Diagnostic criteria of AIDS 8 : AIDS was diagnosed according to the “Guidelines of diagnosis and treatment for AIDS” issued by the AIDS Group, Chinese Society of Infectious Diseases, Chinese Medical Association, in 2011. Enzyme-linked immunosorbent assay was used for the initial screening, and Western blot analysis was used to confirm the results.
The clinical diagnostic criteria of PCP were as follows 9 : (1) patients who met the diagnostic criteria of HIV/AIDS 8 ; (2) patients with a CD4+ T lymphocyte count of <200/μL; (3) patients with chronic fever, cough, progressive dyspnea, cyanosis, and hypoxemia; (4) patients with chest images showing manifestations of interstitial pneumonia, or pulmonary CT scanning showing ground-glass shadows, assessed by two chest imaging specialists individually; and (5) patients who responded well to cotrimoxazole treatment.
Arterial blood gas, blood routine, and flow cytometry measurements
After hospitalization, an arterial blood gas examination was conducted for all the patients immediately at room air, and fasting venous blood was obtained on the second day after hospitalization for blood routine examination and flow cytometry. An Epics XL flow cytometer (Bechman Coulter, USA) was used for the measurement, using anti-human CD3-FITC antibody, anti-human CD4-RD1 antibody, and anti-human CD8-ECD antibody (Bechman Coulter). The samples were preprocessed as follows: 100 μL of whole blood was obtained, into which 10 μL of the corresponding antibody was added and then incubated for 20 min in the dark at room temperature. Subsequently, 500 μL of hemolysin was added, and the mixture was incubated for another 10 min in the dark at room temperature. Afterward, 500 μL of dilution solution was added, followed by incubation in the dark at room temperature for 10 min, and then, the percentages of CD3+, CD4+, and CD8+ T lymphocytes were measured by flow cytometry within 2 h.
Pathogenic measurement
Sputum culture: All the patients were asked to rinse the mouth with normal saline in the morning on the day after hospitalization. The sputum was collected and sent to the bacterial laboratory within 2 h for sputum bacterial culture, fungal culture, acid-fast staining and smearing, and mycobacterial culture. The sputum sample should meet the following criteria: squamous epithelial cells <10 per visual field (low magnification), white blood cells >20 per visual field (low magnification), or ratio of squamous epithelial cells to white blood cells <1:2.5. A medium containing blood agar and eosin–methylene blue was used for the bacterial culture, Sabouraud medium was used for the fungal culture, and modified Lowenstein medium was used for the mycobacterial culture. If the results of two or more consecutive sputum cultures of the same patient were consistent, one pathogen was recorded. However, if the two consecutive sputum cultures showed inconsistent results, the cultured pathogens were recorded separately.
Detection of P. jirovecii: If characteristic trophozoites or cysts were found in the sputum samples or the characteristic cysts were observed by Giemsa staining or methenamine silver staining in the sputum samples, the result was recorded.
Treatment
The conditions of patients with PCP were generally severe. Empirical cotrimoxazole treatment was conducted within 5 days after hospitalization according to the clinical manifestations and CT imaging results. For the patients with PaO2 <70 mmHg, glucocorticoid therapy was administered, and the dose was gradually decreased. Oxygen treatment was conducted to all patients with hypoxia, using a nasal catheter or a face mask. In addition, corresponding anti-infection therapy was provided to patients associated with bacterial or fungal infections. All the patients diagnosed with AIDS were transferred to the Shanghai Public Health Center for highly active antiretroviral treatment.
Outcome assessment criteria
The treatment efficacy was assessed according to the improvement in clinical symptoms, signs, CT imaging manifestations, and arterial blood gas results. The outcomes were generally assessed 1–2 weeks after hospitalization (before discharge) and classified into four categories as follows: (1) improved, indicating evident improvement in clinical symptoms and signs after the treatment, and the CT imaging findings showing absorption of the lesions; (2) stabilized, indicating no evident change in clinical symptoms, signs, and CT imaging manifestations after the treatment; (3) worsened, indicating worsening of clinical symptoms, signs, or CT imaging manifestations; and (4) death. The patients were followed up via telephone calls before 30 September 2018, to assess the disease conditions and survival of the patients for the second time.
Statistical analysis
SPSS 22.0 software was used for the analysis of all data. Qualitative data were described with frequencies and percentages. Quantitative data were presented as mean ± standard deviations (SD). The differences in frequencies between groups were analyzed using the χ2 test. The Yates’ correction was employed if fewer than five patients were positive within a group. The Fisher’s exact test was employed if fewer than one patient was positive within a group. A value of p < 0.05 was considered statistically significant.
Results
General characteristics
Clinical characteristics of enrolled patients with respiratory symptoms.

HIV = human immunodeficiency virus.
Clinical manifestations
The initial manifestations of the patients in this study were respiratory symptoms, and all initially visited the respiratory department. The major clinical symptoms included cough (69, 78.4%), dyspnea (52, 59.1%), and fever (50, 56.8%). The most frequent systemic symptoms included body weight loss (22, 25.0%), anorexia (17, 19.3%), and fatigue (14, 15.9%). In addition, 22 patients (22.7%) also had thrush, and the results are shown in Figure 2. Initial symptoms of the 88 patients with HIV infection.
Laboratory results
Laboratory results.

WBC = white blood cell; L = lymphocytes; PaO2 = oxygen partial pressure; PaCO2 = carbon dioxide partial pressure; SaO2 = oxygen saturation; P(A-a)O2 = differential arterial oxygen partial pressure.
Opportunistic pulmonary infection
The pathogenic tests were conducted after the hospitalization of the patients, and the types of opportunistic pulmonary infections were diagnosed in combination with the CT features. Figure 3 shows that PCP was the most frequent type of opportunistic pulmonary infection, followed by tuberculosis infection. In total, 43 patients (48.9%) had PCP, which was diagnosed according to the clinical diagnostic criteria
9
described earlier (pathogenic results of sputum were negative). In addition, 28 patients (31.8%) had a tuberculosis infection, which included pulmonary tuberculosis, lymphatic tuberculosis, and abdominal tuberculosis, and some patients had more than one type of tuberculosis infection. Twenty-two patients (25.0%) had other fungal infections, such as Candida albicans, Aspergillus, Candida krusei, and Cryptococcus; the infection of C. albicans (18, 20.4%) was the most frequent type of other fungal infection. In addition, five patients (5.7%) had bacterial infection and three patients (3.4%) had non-tuberculous mycobacterial (NTM) infection. It is noted that many patients had multiple opportunistic infections at the same time. Types of opportunistic pulmonary infections; Abbreviations: PCP, Pneumocystis jirovecii pneumonia; NTM, non-tuberculous mycobacterial.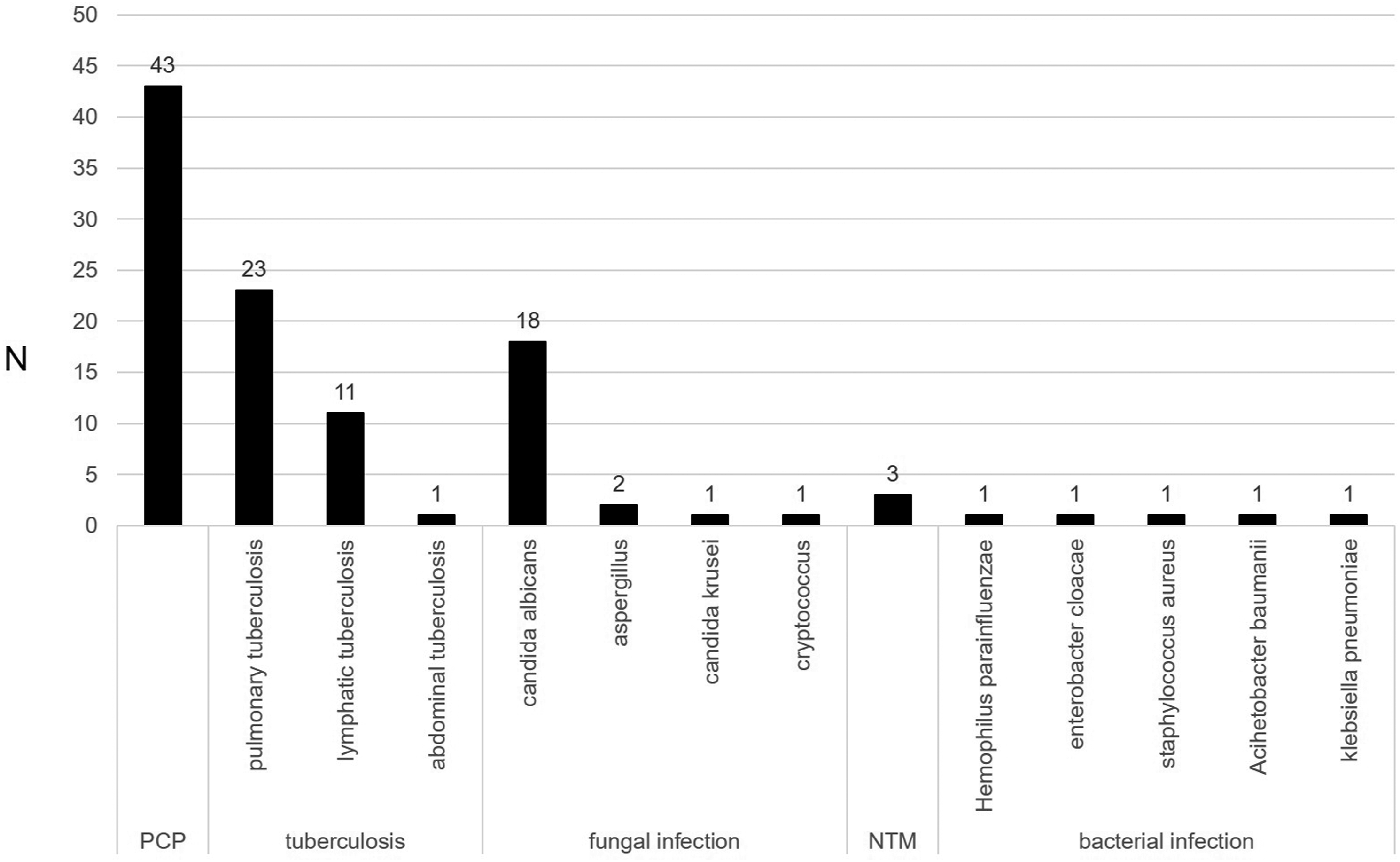
Chest CT imaging characteristics
Chest CT images of 88 patients.

CT = computed tomography; PCP = pneumocystis pneumonia.
aIncluding tuberculosis (N = 28), other fungal infections (N = 22), bacterial infections (N = 5), and non-tuberculous mycobacteria (N = 3). Some patients had two or more types of infections.
bCompared with other infections, patients with PCP had more significantly CT manifestation of bilateral lung involvement and ground-glass shadow changes, p < .001.

Chest CT imaging manifestations of typical PCP. Typical Chest CT imaging manifestations of PCP (a–c), showing diffuse ground-glass shadows in bilateral lungs, with uneven densities and unclear margins.
Treatments and outcomes
Sulfamethoxazole combined with trimethoprim (SMZ-TMP) was provided in time for 43 patients after the diagnosis of PCP, and the SMZ-TMP treatment was initiated within 0–5 days after hospitalization (1.3 ± 1.3 days). The treatment lasted for 5.3 ± 3.0 days. For the patients with PaO2 <70 mmHg, glucocorticoid treatment was also conducted. The treatment was initiated within 0–3 days after hospitalization (0.9 ± 1.2 days; with the doses ranging from 40 to 320 mg/d according to the disease severities) and lasted for 4.1 ± 3.8 days. Voriconazole treatment was provided to 12 patients who also had a fungal infection. The treatment was initiated within 0–5 days after hospitalization (1.5 ± 1.5 days) and lasted for 3.1 ± 2.7 days. Treatment efficacy was assessed for all the patients before discharge, using the methods described earlier. The results showed that the disease conditions improved in 32 patients (36.4%) and stabilized in 56 patients (63.6%) before discharged. Among these 88 patients, 82 patients were discharged within 7 days after hospitalization but were suggested to be transferred to the Public Health Center for antiretroviral therapy treatment. These 82 patients were mostly followed up in the Public Health Center. Three patients were followed up and re-examined in the study hospital, and their posttreatment CT scanning showed that the pulmonary lesions were evidently absorbed and improved (Figure 5). Anti-tuberculosis treatment was provided for all 28 patients with pulmonary tuberculosis. Chest CT changes in patients with PCP before and after treatment. (a and b) Chest CT images of a patient with PCP before treatment, showing the diffuse ground-glass shadows in bilateral lungs. (c and d) Chest CT images of the lungs after 1 week of anti-fungal and antiviral treatments, showing that the ground-glass shadows in bilateral lungs were evidently absorbed.
Forty-three patients who received antiviral treatment were followed up by telephone call until 30 September 2018. According to the efficacy assessment criteria, the outcomes were as follows: improvement in 27 patients (62.8%), stabilization in four patients (9.3%), worsening in one patient (2.3%), and death in 11 patients (25.6%).
Discussion
Patients with AIDS having respiratory symptoms as the initial manifestation are generally initially diagnosed with “diffuse pulmonary disease” and admitted to the respiratory department. Such disease can be easily misdiagnosed or underdiagnosed if physicians do not have enough experience. In addition, clinical manifestations in such patients generally lack specificity, while the most frequent symptoms include cough, dyspnea, and fever in about 84.2%, 64.5%, and 64.2% of the patients, respectively. Chest CT images of patients have certain features, and a diffuse ground-glass shadow in bilateral lungs was the most frequent manifestation (39.8%). Peripheral leukopenia and lymphopenia are found in 43.6% of patients. In addition, hypoxemia is found in severe cases, which can even progress to type I respiratory failure.
Patients with AIDS are at high risk of various opportunistic infections due to immune impairment. PCP is the most common type of opportunistic infection found in clinical practice in patients with AIDS. 10 In this study, 48.9% of the patients had PCP, which was also one of the major causes of deaths in patients with AIDS. 11 PCP mainly occurred in patients with a CD4+ T lymphocyte count of <200/μL. When clinical manifestations of patients with AIDS are fever and hypoxemia, or CT chest imaging shows ground-glass shadows, the possibility of PCP should be considered. In this study, all the patients were initially admitted to the respiratory department for the respiratory symptoms. Among these patients, the initial diagnosis of 64.8% patients was diffuse pulmonary lesions after hospitalization, and the chest CT image manifestation of most patients (76.7%) was a diffuse ground-glass shadow in bilateral lungs. In addition, some patients also had an oral fungal infection, which was of significance for the diagnosis of complications of PCP in patients with AIDS. Early HIV screening and CD4+ T cell measurements should be conducted to confirm the diagnosis of PCP. In theory, the final diagnosis of PCP depends on pathogenic examinations, which require the detection of P. jirovecii in sputum, bronchoalveolar lavage fluid, and lung tissue biopsies. However, such examinations are very difficult to be conducted in clinical practice. The P. jirovecii examination of all the patients enrolled showed negative results, and PCP were diagnosed according to the clinical diagnostic criteria. 9 Therefore, for the patients who met the clinical diagnostic criteria, empirical anti-infection therapy, especially SMZ-TMP treatment, was conducted in time, to win time for the consequent antiviral treatment. For patients also having hypoxemia, early treatment with glucocorticoids should be conducted within 72 h after the diagnosis, if possible.
Pulmonary tuberculosis is also an opportunistic infection that frequently occurs in patients with AIDS, with an incidence of about 20%–50%. 12 In this study, 28 patients with AIDS (31.8%) also had pulmonary tuberculosis; of these, 22 (39.2%) had simple pulmonary tuberculosis or lymphoid tuberculosis. As HIV infection could lead to immune suppression, the tuberculin test and T-SPOT test would be showed negative in patients already having a tuberculosis infection. Therefore, tuberculosis infection should not be ruled out for patients with AIDS having negative results of the tuberculin test and T-SPOT test.
The pathogens of other opportunistic infections included C. albicans, non-tuberculous Mycobacterium, and Aspergillus. When diagnosing AIDS, the infection of such pathogens was also diagnosed according to the pulmonary CT imaging findings and pathogenic examination results. When the pathogens of the opportunistic infections were identified, the corresponding anti-microbial treatments should be conducted as early as possible to control the infection and inflammatory responses, thus winning time for the consequent early antiviral therapy.
Studies have shown that the rate of improvement among patients with AIDS can be as high as 62.8% after early antiviral therapy. In this study, 43 patients were transferred to CDC and received antiviral therapy, and the disease conditions in 72% of them improved or stabilized. In recent years, the incidence of HIV-related opportunistic infection has reduced to a certain degree, which can be associated with early diagnosis and early antiviral therapy for HIV.6,13,14
This study suggested that the history of visiting prostitutes and drug injection should be reviewed for patients with diffuse ground-glass shadows in bilateral lungs who were initially admitted to the respiratory department. Moreover, the preliminary HIV screening and sputum examination should be done as early as possible for patients highly suspicious of AIDS combined with pulmonary infection. As the pathogenic evidence is generally difficult to be obtained from most of the patients, early initiation of empirical anti-inflammation and anti-infection treatment can win valuable time for the consequent antiviral therapy and help in improving the prognosis.
However the study had some limitations. It was a retrospective study in a single center. Patients were timely transferred to CDC for antiviral treatment after being diagnosed, so as to the follow-up was relatively difficult, which might have impacted the integrity of the data. In this study, sputum culture was the only examination for detecting P. jirovecii, and pathogenic results of sputum were negative in all cases; it may be one of the limitations. New experimental techniques such as next-generation sequencing will be used in our future study.
Conclusions
The most common chest CT manifestation of patients with AIDS having respiratory symptoms as the initial manifestations was a diffuse ground-glass shadow in bilateral lungs. For patients with such CT manifestations, a detailed medical history recording, screening of human immunodeficiency virus antibody, and flow cytometry test would improve the diagnostic efficiency of AIDS. It may help in the early diagnosis of AIDS for respiratory physicians and win tine for the treatment.
Footnotes
Author Contributions
H Li, X Chen, and Y Zhou supported in conception and design. H Li is an administrative support. X Chen and Y Zhou supports provision of study materials or patients. X Chen and Y Zhou supported in collection and assembly of data. All authors supported forarticle writing and final approval of the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from the National Science Foundation of China (No: 81730002, 81670055, 81670056, 91442103, 81500052, and 81570057), the Ministry of Science and Technology of the People’s Republic of China (No: 2016YFC1100200 and 2016YFC1100204), the National Science Foundation of Shanghai (No: 18ZR1431400), the Shanghai Hospital Development Center (No: 16CR3054 A) and Dream Mentor-Freshman Training Program in Shanghai Pulmonary Hospital (No: fkxr1901).
Ethics approval
The authors are accountable for all aspects of the study in ensuring that questions related to the accuracy or integrity of any part of the study are appropriately investigated and resolved. The institutional ethics committee of Shanghai Pulmonary Hospital approved the study (2014fk04).
Informed consent
Written informed consent was taken from all the participants.