
Abstract
Background
Contextually tailored, arts-based HIV prevention strategies hold potential to advance adolescent sexual health and wellbeing. We examined HIV prevention outcomes associated with arts-based sexual health workshop participation with Northern and Indigenous adolescents in the Northwest Territories (NWT), Canada.
Methods
An Indigenous community-based youth agency delivered arts-based workshops in school settings to adolescents aged 13-18 in 24 NWT communities. Pre and post-test surveys included socio-demographic characteristics, sexually infections (STI) knowledge, HIV/STI risk perception, sexual relationship equity, condom use self-efficacy, and safer sex efficacy (SSE). Latent change score models were conducted to assess pre-post differences and factors associated with these differences.
Results
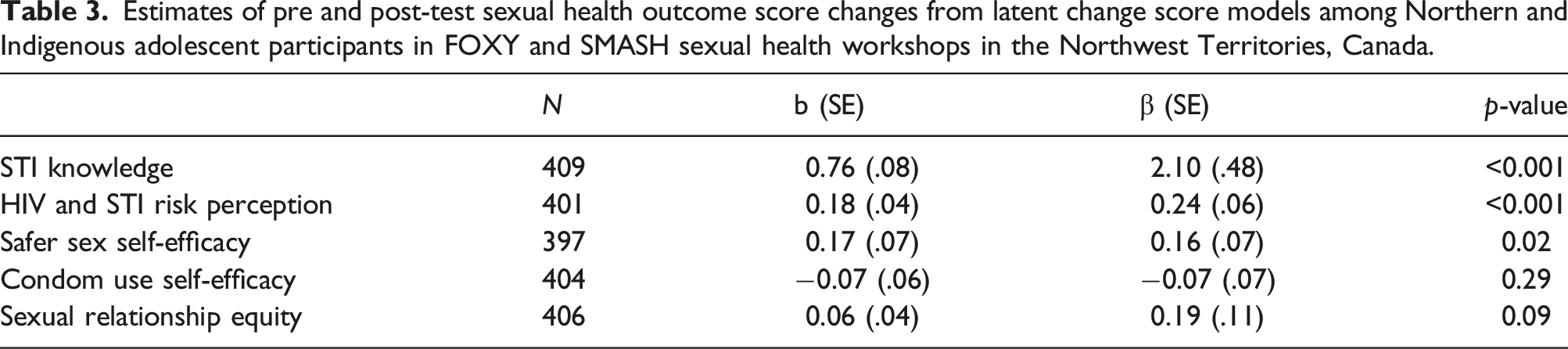
Among participants (n = 344; mean age 14.3 years, SD: 1.3; Indigenous: 79%) most (66%) had previously attended this workshop. Latent change score models revealed a significant and large effect size for increased STI knowledge (β = 2.10, SE = 0.48, p < .001) and significant and small effect sizes for increased HIV/STI risk perception (β = 0.24, SE = 0.06, p < .001) and SSE (β = 0.16, SE = 0.07, p = .02). The largest increases across several outcomes occurred with first time workshop participants; yet previous workshop participants continued to report increases in HIV/STI risk perception and SSE.
Conclusion
Arts-based HIV prevention approaches show promise in advancing STI knowledge, risk perception, and SSE with Northern and Indigenous youth.
Keywords
Introduction
Northern Canada is disproportionately affected by sexually infections (STIs) compared to other regions in the country. 1 Reports from the Public Health Agency of Canada reveal that rates of chlamydia and gonorrhea in the Northwest Territories are among the highest in Canada. 2 Indigenous peoples account for 14% of HIV infections in Canada while only comprising 4% of the Canadian population. 2 This and other health inequities experienced by Indigenous peoples in Canada are largely due to structural factors including colonization and related assimilation policies that marginalized Indigenous peoples and practices from mainstream Canadian society. 3 Systemic marginalization and discrimination present barriers for Indigenous peoples’ engagement in healthcare. 4
Researchers have called for sexual health programs to employ youth-centered approaches to effectively prevent HIV and STIs in Indigenous communities. 5 Such approaches align with data showing that Indigenous peoples in Canada are more likely to be diagnosed with HIV at a younger age than non-Indigenous counterparts. 2 The stigma experienced by Indigenous youth diagnosed with HIV between the ages of 15 and 29 has been cited as a barrier to accessing sexual and reproductive health (SRH) services and as a stressor for mental health. 6 Moreover, low knowledge levels about HIV prevention and testing among Indigenous youth contribute to low uptake of SRH services. 7 Low HIV and STI risk perception among Indigenous youth at elevated risk of HIV exposure (e.g. persons who use drugs and alcohol, exchange sex for money, or practice condomless sex) further compounds the low uptake of SRH services.7,8
Past health intervention research has identified arts-based methodologies as an effective route for engaging Northern and Indigenous youth and collecting data on topics related to sexual health.9,10 Specifically, arts-based methodologies can enable participants to perceive phenomena in novel ways, are likely to be more memorable and accessible to audiences with low literacy levels, can enhance understanding of complex experiences by reducing verbal communication barriers, and can encourage dialogue on challenging or stigmatized topics. 10 Further, arts-based methodologies can advance strengths-based approaches, acknowledging and confronting the persistent effects of colonialism on the health of Indigenous youth, while also emphasizing participants’ unique resiliencies, strengths, and resources through culturally relevant activities including poetry, storytelling, traditional hand drumming and singing, and sharing circles.9–12 Arts-based sexual health programming has the potential to facilitate empowerment through building leadership skills and self-efficacy, nurturing social connections, enhancing confidence, and promoting a greater sense of control of one’s life and environment.9,10,13 Notably, in the Northwest Territories, arts-based methods have been linked with increased STI knowledge and safer sex self-efficacy among Indigenous youth.14,15
Although previous studies have evaluated the ability of community-led arts-based programs to improve sexual health among Indigenous youth in Northern Canada, key knowledge gaps remain. Firstly, scant evidence evaluates the impact of arts-based approaches on Indigenous youth’s HIV and STI risk perception, which is a key determinant of SRH service uptake among youth in other contexts. 16 Secondly, limited studies explore the role of gender on shaping STI knowledge, risk perception and safer sex self-efficacy among Indigenous youth in Canada, despite evidence in other contexts showing that gender inequities harm all youth, yet specifically elevate HIV vulnerabilities among adolescent girls and young women. For instance, in Canada, Indigenous girls and young women are more likely to be diagnosed with HIV than Indigenous boys and young men 2 —which may be linked with gender inequitable norms whereby adolescent girls and young women having less decision-making power over sex and condom use than their boy and men counterparts. 17 Additionally, adolescent boys and young men may be less likely to be medically and socially encouraged to test for STIs than adolescent girls and young women. 18 Third, there is a need to explore the various factors that can either promote (e.g., resilience) or hamper (e.g., depression) the sexual health of Indigenous youth in Northern Canada. Finally, the sexual health benefits of repeated exposure to arts-based sexual health programs are understudied.
In this study, we explore sexual health outcomes among Northern and Indigenous youth associated with participation in arts-based sexual health workshops in the Northwest Territories.14,15 Specifically, we explore associations between STI knowledge, HIV and STI risk perception, condom use self-efficacy, safer sex self-efficacy, sexual relationship equity, with participation in arts-based sexual health programs among Northern and Indignenous youth in the NWT.
Methods
Participants
This is a community-based research program led by Fostering Open eXpression among Youth (FOXY), an Indigenous sexual health agency in the NWT. Project staff recruited students aged 13-17 years old across 24 communities in the Northwest Territories (Aklavik, Behchoko, Deline, Fort Good Hope, Fort McPherson, Fort Providence, Fort Resolution, Fort Smith, Gamèti, Hay River, Inuvik, Kátł’odeeche First Nation, Łutselk’e, Kakisa, Norman Wells, Sambaa Kʼe, Tsiigehtchic, Tuktoyaktuk, Tulita, Ulukhaktok, N'Dilo, Wekweètì, Whatì, Yellowknife) attending secondary school in the 2018-2019 academic year. Recruitment methods included school outreach, use of volunteers, and word-of-mouth referrals. All participants needed to be able to provide informed consent and agree to attend a workshop by FOXY, for young women and non-binary participants, or its counterpart Strengths, Masculinities and Sexual Health (SMASH), for young men and non-binary persons.
Procedures
The study was conducted using a single-group pre- and post-test design within secondary schools. FOXY and SMASH are interactive sexual health education programs that address sexual health, HIV and STIs, sexuality, and healthy relationships with various activities, including group work, visual word maps, question boxes, group discussions, charades, and role playing (detailed program content has been previously published).
14
Professional facilitators, in conjunction with trained adolescent peer facilitators, lead workshops for groups of 8-15 participants. The program consists of seven workshop activities, each lasting one to two hours, conducted over the course of one or two days. A range of arts-based approaches were employed across session activities, including body mapping10,19 (see Figure 1 for a description) as well as youth participants creating and naming groups with a logo/symbol to work together on session content (see Figure 2 for an example). Overview of body mapping methodology. Arts-based approach with youth group name and symbols.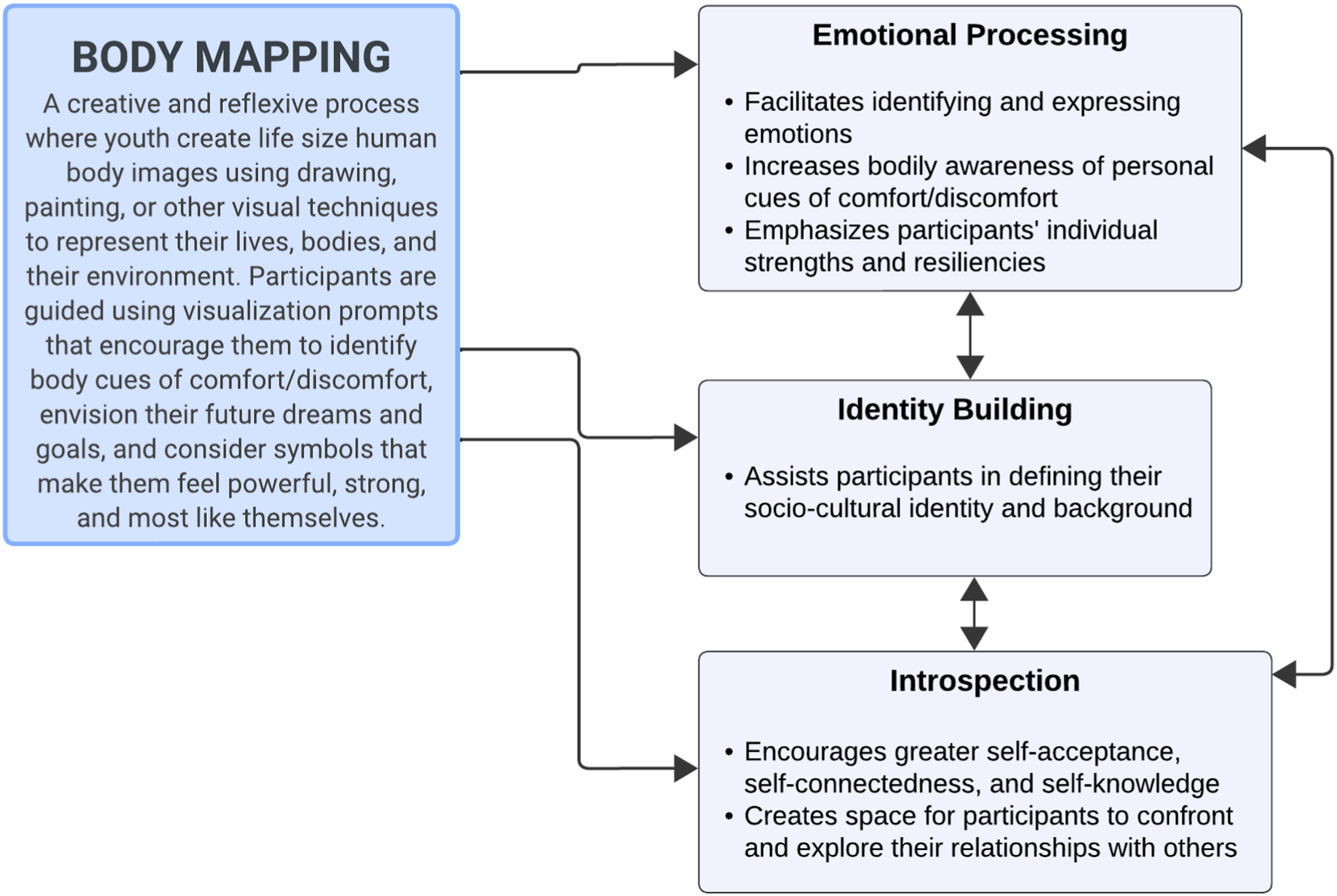

Participants completed a baseline survey immediately before (pre-test) and another survey immediately after completing the program (post-test). Surveys included questions about sociodemographic characteristics, STI knowledge and self-efficacy, and other sexual health related outcomes (e.g., risk perception, equitable sexual relationship attitudes). Participants were compensated with a $25 gift for their participation. All youth participants provided informed assent, and parents provided reverse informed consent. All research procedures were approved by the Research Ethics Board of the University of Toronto and Aurora Research Institute.
Measures
Sexually transmitted infections knowledge
Understanding of STIs and their symptoms was assessed using a 15-item, true or false scale adapted from a previous measure. 20 Total scores were calculated as the percentage of responses answered accurately (Cronbach’s alpha = 0.79; range = 0%–100%).
Self-perceived human immunodeficiency virus and sexually transmitted infections risk
Self-perceived risk was assessed by having participants rate how likely they thought they were to contract either HIV or an STI on a 4-point Likert scale ranging from 1 (Not Likely at All) to 4 (Definitely). Total scores were calculated as the average of the two items (Cronbach’s alpha = 0.95; range = 1-4).
Safer sex self-efficacy
Participants’ confidence in their ability to have safe sex in various contexts was assessed using a 5-item scale assessing situational safer sex self efficacy by Redding and Rossi. 21 Participants rated their level of confidence from 1 (Not Confident at All) to 5 (Very Confident) and scores were calculated as the average across five items (Cronbach’s alpha = 0.92; range = 1-5).
Condom use self-efficacy
Participants’ confidence in their ability to use condoms was assessed using a 5-item scale assessing condom use self-efficacy by Brafford and Beck. 22 Participants rated their level of agreement on a 5-point Likert scale and scores were calculated as the average across five items (Cronbach’s alpha = .89; range = 1-5).
Sexual relationship equity
Participants were asked to rate their level of agreement (1 = ‘I agree’, 2 = ‘I kind of agree’, 3 = ‘I do not agree’) with the 8-item Sexual Relationship Domain of the Gender Equitable Men’s (GEM) 23 Scale about inequitable gender norms reflecting men’s dominance (e.g., “It is the man who decides what type of sex to have”). Scores were calculated as the average across all items, with higher scores indicating a greater sense of gendered sexual relationship equity (Cronbach’s alpha = 0.83; range = 1-3).
Covariates
Participants reported on their age, gender (cisgender women, cisgender men, transgender, nonbinary), sexual identity (lesbian, gay, bisexual, queer [LGBQ] vs. heterosexual), ethnicity (Indigenous or not), whether they lived in an urban (Yellowknife) or rural (other) community, food insecurity (how often they go to sleep hungry without being able to eat), and whether they were sexually active. In addition, we assessed two aspects of social functioning and adjustment. We measured resilience using the Child and Youth Resilience Measure, 24 an 11-item scale on which higher scores indicate a greater availability of individual, relational, communal and cultural resources (Cronbach’s alpha = 0.90, range = 11-55). We assessed participants’ mental well-being using the 9-item Patient Health Questionnaire (PHQ-9) where higher scores indicated higher levels of depression (Cronbach’s alpha = 0.88, range = 0-27). 25 Finally, as some participants had attended these FOXY or SMASH school-based workshops in previous years, we asked participants to report how many FOXY/SMASH workshops they had previously attended.
Data analysis
Descriptive statistics were used to explore the characteristics of the sample and the distribution of outcome variables. We calculated pre-post differences by subtracting pre scores from post scores for each outcome. Due to the nonnormality of outcome variables, Wilcoxon’s signed-ranks tests were used to assess pre-post differences. However, given that the paired-samples t test is robust to nonnormality with large sample sizes, 26 t-tests were also conducted for comparison. To assess the extent to which change in outcomes was associated with various participant characteristics, Spearman rank correlations and Kruskal-Wallis tests were conducted. For all these tests, list-wise deletion was used.
To strengthen our findings, especially given the large amounts of missing data, latent change score models were also used to assess pre-post differences, using full-information maximum likelihood estimation. 27 We evaluated the goodness of fit of these models using the Comparative Fit Index (>0.95), Tucker Lewis Index (>0.95), root mean square error of approximation (<0.08), and standardized root mean square residual (<0.08) indices. 28 Modification indices were used as needed to improve fit. These models also have the benefit of allowing us to test for factors that explain interindividual differences in change within the model.29,30 For the model with binary indicators (i.e., STI knowledge), we used a theta parametrization and fixed the threshold for the first indicator at each time point in order to be able to estimate the mean latent change. For all outcomes, we tested for an association between the latent change score and each of the covariates individually, and those that were significant at the 0.10 level were considered for inclusion in a multivariate model. In the multivariate model, only those significant at the 0.05 levels were retained. All reported p-values are two-tailed. Data were analyzed using Stata 15 and Mplus 8.1.
Results
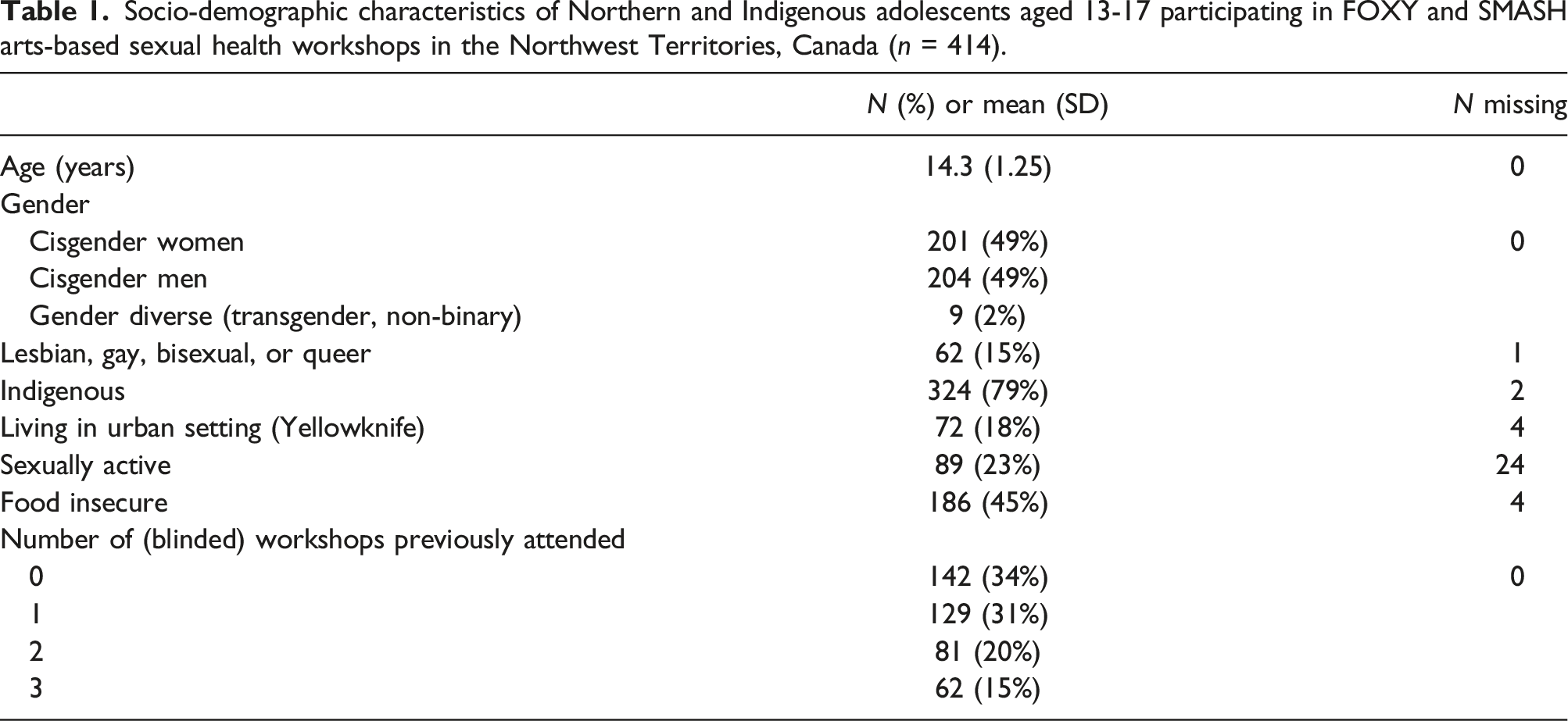
Socio-demographic characteristics of Northern and Indigenous adolescents aged 13-17 participating in FOXY and SMASH arts-based sexual health workshops in the Northwest Territories, Canada (n = 414).
Pre-post outcome score differences
Pre-and post-test differences in scores following participation in FOXY and SMASH sexual health workshops among Northern and Indigenous adolescents in the Northwest Territories, Canada.
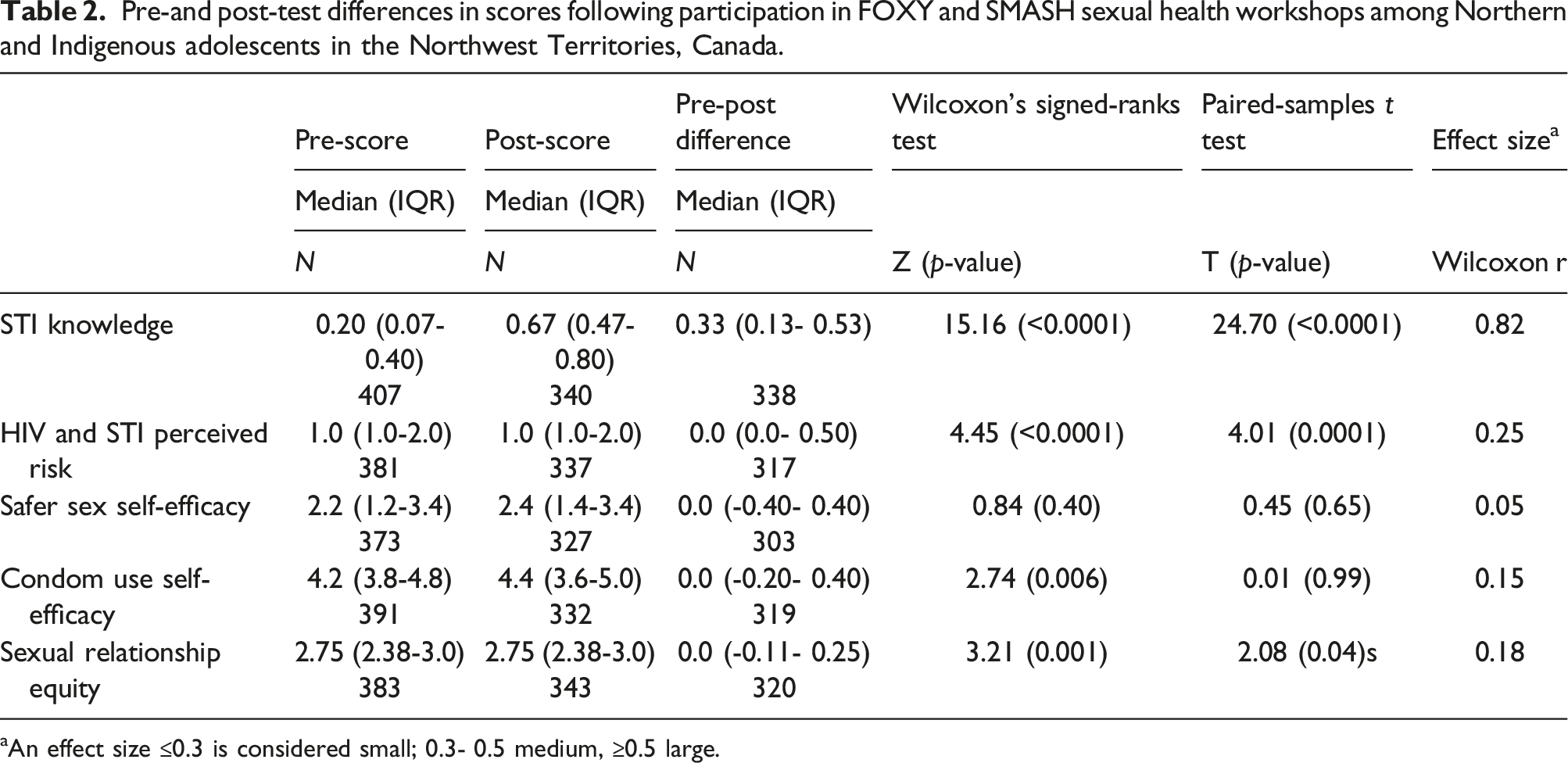
aAn effect size ≤0.3 is considered small; 0.3- 0.5 medium, ≥0.5 large.
Latent change score models
Estimates of pre and post-test sexual health outcome score changes from latent change score models among Northern and Indigenous adolescent participants in FOXY and SMASH sexual health workshops in the Northwest Territories, Canada.
Differential effects
Models in which the latent change scores were regressed on covariates indicated that workshop participation was associated with differential outcomes for different populations (fit statistics for these models in Supplementary Table 4). Specifically, individuals with higher resilience scores reported greater increases in STI knowledge following the workshop (β = 0.13, SE = 0.06, p = .02). Participants who exhibited more depression symptoms at baseline reported greater increases in safer sex self-efficacy (β = 0.13, SE = 0.06, p = 0.02). Indigenous participants experienced smaller increases in safer sex self-efficacy (β = −0.16, SE = 0.02, p = .003). Workshop participation was also associated with greater increases in sexual relationship equity for individuals who identified as cisgender women (β = 0.23, SE = 0.06, p < .001) or having a transgender or nonbinary gender identity (β = 0.13, SE = 0.06, p = .02), individuals from urban regions (vs. rural) (β = 0.15, SE = 0.06, p = .005), and those with higher resilience scores (β = 0.13, SE = 0.06, p = .02). While there were independent effects of food insecurity and gender identity (cisgender women) on HIV/STI perceived risk, neither remained significant in a multivariate model. Finally, associations between workshop participation and condom use self-efficacy were not significantly moderated by any socio-demographic characteristic.
Discussion
This study investigates the potential of arts-based sexual health workshops in the NWT to improve STI knowledge, safer sex self-efficacy, and attitudes that reflect sexual relationship equity. Findings reveal an important post-intervention increase in STI knowledge, and small but statistically significant increases in safer sex efficacy. This corroborates previous research that notes the utility of arts-based methods at improving STI knowledge and safer sex self-efficacy among Indigenous youth.14,15
Most significantly, we found that workshop participation was associated with increased STI knowledge across all demographics. This supports existing research that highlights the importance of arts-based methods in increasing STI knowledge. For instance, a study in Australia with multicultural youth demonstrated improved sexual health knowledge and a positive shift in attitudes towards sexual health resulting from participation in a theatre- and arts-based intervention. 31 Importantly, we found that youth with higher resilience scores showed a greater increase in STI knowledge. While this study highlights the transformative potential of arts-based interventions, more research should be conducted to examine how to bolster resiliency among Northern and Indigenous youth to support sexual health knowledge uptake.
Small but significant increases in HIV and STI self-perceived risk and safer sex self-efficacy were also observed following workshop participation, corroborating findings from prior studies.14,15,32 Compared to non-Indigenous youth, however, Indigenous participants reported smaller increases in safer sex self-efficacy. This may be explained by the systemic marginalisation that can disconnect Indigenous people from health systems. 4 Despite these workshops’ integration of Indigenous knowledge and teachings, the relatively lower increase in safer sex self-efficacy highlights the need for further research to understand barriers and faciltiators to Indigenous youths’ safer sex self-efficacy which includes but extends beyond knowledge to encapsulate confidence and skills.
Post-workshop changes in attitudes toward sexual relationship equity were not statistically significant. However, we noted that cisgender women and non-binary persons reported improved attitudes toward sexual relationship equity. These findings validate research that shows that women/non-binary individuals may have more emotional investment in gender equity than men, and women may also seek to engage more actively in promoting positive outcomes towards women’s sexual agency.33–35 It also signals the need to explore how gender transformative approaches can be tailored for young men in the NWT to improve their attitudes toward gender equitable relationship norms.
The limitations of this research includes a limited generalisability of the findings due to a lack of control group as well as convenience sampling methods. Second, the survey used in this study measures intention to apply sexual health related strategies and practices, which may not translate to their actual application in real life. This study could be substantiated with longitudinal work to address application of intended sexual health changes to real world sexual practices. Third, qualititative data could be integrated to create a more comprehensive understanding of post-intervention sexual health outcomes, particularly when we did not find significant changes.
A significant contribution of this study was identifying the continued benefit of sexual health workshop participation in increasing HIV/STI risk perception and safer sex self-efficay among former participants. This signals the need for annual booster sessions to reinforce HIV and STI risk perception and safer sex self-efficacy among adolescents in the NWT. These factors—unlike STI knowledge which is based on factual and technical learning—are relational and may be shaped by contextual factors such as relationship power dynamics and other socio-environmental influences. From this perspective, sexual health promotion strategies can be dynamic and evolve alongside youths’ learning and growth.
Despite the limitations of this study, the FOXY/SMASH arts-based sexual health workshops show the potential to improve sexual health outcomes among Indigenous youth in NWT. Importantly, this study investigated the potential role of gender, Indigeneity, and other sociodemographic characteristics in shaping sexual health outcomes, and noted that booster sessions are beneficial for continued sexual wellbeing. Our studies add to a growing body of research11,12,14,15,36 that highlights the transformative potential of arts-based interventions.
Supplemental Material
Supplemental Material - Human immunodeficiency virus prevention outcomes associated with arts-based sexual health workshop participation among Northern and Indigenous adolescents in the Northwest Territories, Canada
Supplemental Material for Human immunodeficiency virus prevention outcomes associated with arts-based sexual health workshop participation among Northern and Indigenous adolescents in the Northwest Territories, Canada by Candice Lys, Carmen H Logie, Anoushka Lad, Nina Sokolovic, Kayley Inuksuk Mackay, Aryssa Hasham, and Kalonde Malama in International Journal of STD & AIDS.
Footnotes
Acknowledgements
This grant was supported by the Canadian Institutes of Health Research (CIHR), Social Sciences & Humanities Research Council of Canada (SSHRC), Public Health Agency of Canada, and Arctic Inspiration Prize. Authors declare no conflict of interest. C. Logie was also supported by the Canada Research Chairs Program, Canada Foundation for Innovation, and Ontario Ministry of Research and Innovation. We would like to thank all FOXY and SMASH staff, peers, and participants.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ontario Ministry of Research, Innovation and Science (ERA), Social Sciences and Humanities Research Council of Canada (Insight), Canada Foundation for Innovation, Institute of Aboriginal Peoples Health, Canada Research Chairs (Tier 2), Public Health Agency of Canada, and Prix Inspiration Arctique.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.