
Abstract
In this paper, we present a narrative review of primary research on the health impacts of extreme weather events in urban informal settlements published between 1990 and June 2021. We include 54 studies and examine the health impacts of extreme weather events and how these were determined. We find that these events impact health directly by causing mortality, injury and disease and through indirect pathways by impacting livelihoods, access to healthcare, coping strategies and adaptive capacity. Drawing on the social determinants of health framework to frame our analysis, we find that health impacts are determined by multiple intersecting factors, relating to individual circumstances, material conditions, health status, and political and socio-economic context. Consequently, vulnerability varies between and within informal settlements. Overall, we show that responding to and minimising these health impacts requires an intersectional approach to understand and address these contextual root causes of vulnerability.

I. Introduction
The impacts of human-induced climate change are already being experienced, particularly through extreme weather events.(1) There is now considerable evidence that climate change has resulted, and will continue to result, in increased extremes, including increased frequency and intensity of heatwaves and heavy precipitation, increased droughts and major tropical cyclones.(2) Climate change, including extreme weather events, will have overwhelmingly negative consequences for human health,(3) through both direct and indirect effects.(4)
The impacts of climate change in cities, including those on health, will particularly affect those living in informal settlements, who are widely recognised to be especially vulnerable to the impacts of climate change.(5) Residents in informal settlements already experience ill health disproportionately compared to other urban dwellers and these inequalities will continue to be reproduced by climate change.(6) The vulnerability of informal settlements to these health impacts is widely accepted, including by the Intergovernmental Panel on Climate Change (IPCC).(7) However, specific evidence on the impacts of weather and climatic changes on health in informal settlements is lacking(8) and in general the impacts of climate change in informal settlements is a major research gap.(9)
First, there has been a lack of synthesis of this research. To our knowledge, there has been to date only one formal review of the literature, that of Borg et al.(10) Although insightful, this review provides only a cursory discussion of the health impacts in informal settlements, based on just 15 studies.
Second, there has been limited discussion of how vulnerabilities are determined and differ within and between informal settlements. It is estimated that approximately one billion people live in informal settlements.(11) Although there may be similarities between such settlements,(12) definitions and preferred terminologies, which can be imprecise, vary by country. Moreover, within these settlements, the degree of informality and exclusion varies.(13)
Discussions of the vulnerability of informal settlements to climate change are often broad and sweeping, thereby missing the complex, fine-grained variations between and within informal settlements. It is widely known, for instance, that locations on or near hillsides or in low-lying or river-adjacent areas can expose settlements to landslides and flooding respectively.(14) Vulnerability is widely considered to be determined by material and physical circumstances such as poor housing, inadequate sanitation, lack of infrastructure and overcrowding.(15) The interaction of these factors with markers of disadvantage, such as income, age and gender, have been noted in the literature(16) along with the wider political determinants such as government neglect and lack of access to services.(17) However, there has been no synthesis of the literature on health and climate change that considers these determinants of vulnerability and how they cause health impacts to vary at the sub-settlement level. Knowledge of the impacts on individuals, households and communities is vital to inform policy responses.(18)
Here we present the results from a narrative review of the literature on extreme weather events, health and informal settlements through the lens of vulnerability. We focus on extreme weather events (flooding, extreme temperatures, droughts and storms) rather than climate change more broadly as the need to understand the impacts of extreme weather events is particularly pressing. Using a more comprehensive search strategy than Borg et al.,(19) we include 54 studies in our review.
We begin in the next section by outlining the conceptual framework underpinning this review, before detailing the methodology used. We then present an overview of the search results and outline the health impacts of the extreme weather events reported in these studies. We find these events impact health and mortality directly through injury, disease, and their implications for mental health; and indirectly through their effect on livelihoods, access to healthcare, coping strategies and adaptive capacity. Finally, we examine the reported determinants of these health impacts, showing that vulnerability is determined by multiple intersecting factors at the level of the individual, settlement and wider socio-economic and political context. Overall, we argue for a broader, more intersectional approach to researching and responding to the health impacts of extreme weather events and climate change in informal settlements.
II. Conceptual Framework
Here we follow the IPCC, which considers climate change risks and impacts as the result of the interaction between hazards, exposure and vulnerability.(20) Hazards are defined as the potential occurrence of events or trends that may cause adverse impacts, and exposure is defined as presence in places or settings that could be adversely affected.(21) Vulnerability, defined as the “propensity or predisposition to being adversely affected”,(22) is not solely understood as an outcome of exposure to hazards, but as a contextual starting point encompassing sensitivity, susceptibility and the ability to cope and adapt,(23) also considering the socio-economic and political context.(24) Based on this conceptualisation, the extent to which extreme weather events will impact people and vary among populations depends not only on hazard and exposure, but also on the factors that shape vulnerability. Risk is the “potential for adverse consequences” resulting from the interaction between hazards, exposure and vulnerability, and impacts are the consequences when risks are realised on both natural and human systems, including on health and well-being.(25)
To analyse the health impacts of extreme weather events in informal settlements through this lens of contextual vulnerability, our conceptual framework draws on the World Health Organization’s (WHO) social determinants of health (SDH) model which emphasises how wider structural and intermediary determinants define and underpin health.(26) The SDH framework has been effectively applied to urban areas, including informal settlements, showing how multiple determinants shape health including place of residence (situated within a socio-political context), socio-economic status, gender, race and ethnicity, and education.(27)
To fully understand the health impacts of extreme weather events in informal settlements, the context in which hazards, exposure and vulnerability interact to create risks and impacts needs to be understood.
III. Methodology
The overall aim of this study was to critically review existing research on the impacts of extreme weather events on health in informal settlements. The specific research questions were:
How do extreme weather events, which are expected to increase in frequency, intensity and duration with climate change, impact health in urban informal settlements?
What factors contribute to the vulnerability of people living in these settlements?
How does vulnerability to these health impacts vary within informal settlements?
A narrative review was chosen as it allows an extensive, broad and holistic overview of the current state of knowledge and enables the critical analysis of existing research to identify themes and gaps. This review further used the guiding principles of a systematic review, including a defined research aim and objectives, a focused search strategy, and framework for analysis.(28)
The LSTM (Liverpool School of Tropical Medicine) EDS Discover tool and additional systematic searches of Medline, CINAHL, Global Health, Web of Science, Cochrane, PubMed databases and Google Scholar were used to identify relevant literature. Searches followed a comprehensive strategy based on three key ideas: urban informal settlements, health and extreme weather events related to climate change (see Table 1). Initial searches were conducted in May–June 2020 and updated in July–August 2021.
Search strategy for LSTM EDS Discover Search, CINAHL, Medline, Global Health, Web of Science, PubMed, Cochrane databases and Google Scholar
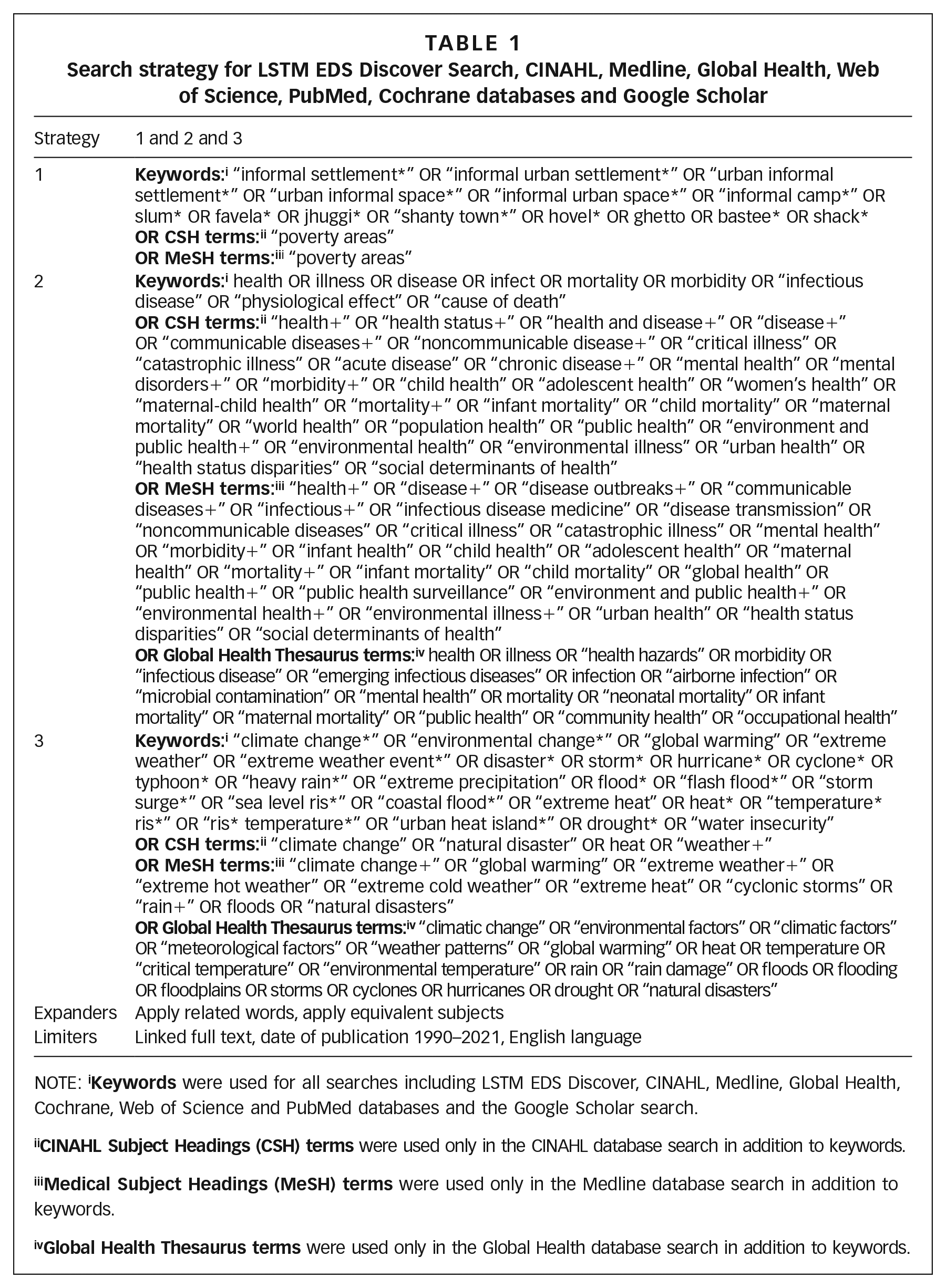
NOTE: i
The following inclusion criteria were used:
linked full-text available;
published between January 1990 to June 2021;
written in English;
studies, case reports or discussion papers containing primary research data from informal settlements, formally published in an academic journal;
specific to three main ideas: urban informal settlements, health, and extreme weather events related to climate change.
The following exclusion criteria were used:
published before January 1990;
not written in English;
theses, dissertations and books;
literature not containing empirical evidence or primary research data from urban informal settlements;
literature not covering all three key ideas named in the inclusion criteria;
literature about long-term climate change impacts; the science of climate change; or only about adaptation, mitigation and resilience.
After removing duplicates, all results were recorded in Excel files and titles and abstracts were screened for relevance, using the inclusion and exclusion criteria outlined above. This was followed by full-text screening of identified results, using the inclusion and exclusion criteria.
For data extraction, collection and analysis of included results, summary tables were created in an Excel file documenting study information, publication details, methods, main findings, and strengths and limitations. Strengths and limitations were considered to critically appraise and assess the quality, value and relevance of studies to determine the weight given to their findings in addressing the research questions.(29)
An adapted thematic analysis method as described by Aveyard(30) was used to guide the analysis and synthesis of literature. This included the use of summary tables, thematic coding using NVivo 11 software, and the development of a thematic framework. Themes naturally emerged from the literature and were continuously identified and adapted throughout the coding process. Codes were then organised into a framework of sub-themes and overarching themes which was used to structure results.
Iv. Results
a. Search results
The initial search produced 2,982 results, of which 2,795 were removed during initial screening. Of the remaining 187 studies, 133 were removed after screening the full text. The remaining 54 studies were deemed relevant and suitable for inclusion in the narrative review. A full list is provided in the supplementary material. Figure 1 provides an overview of the search results.(31)
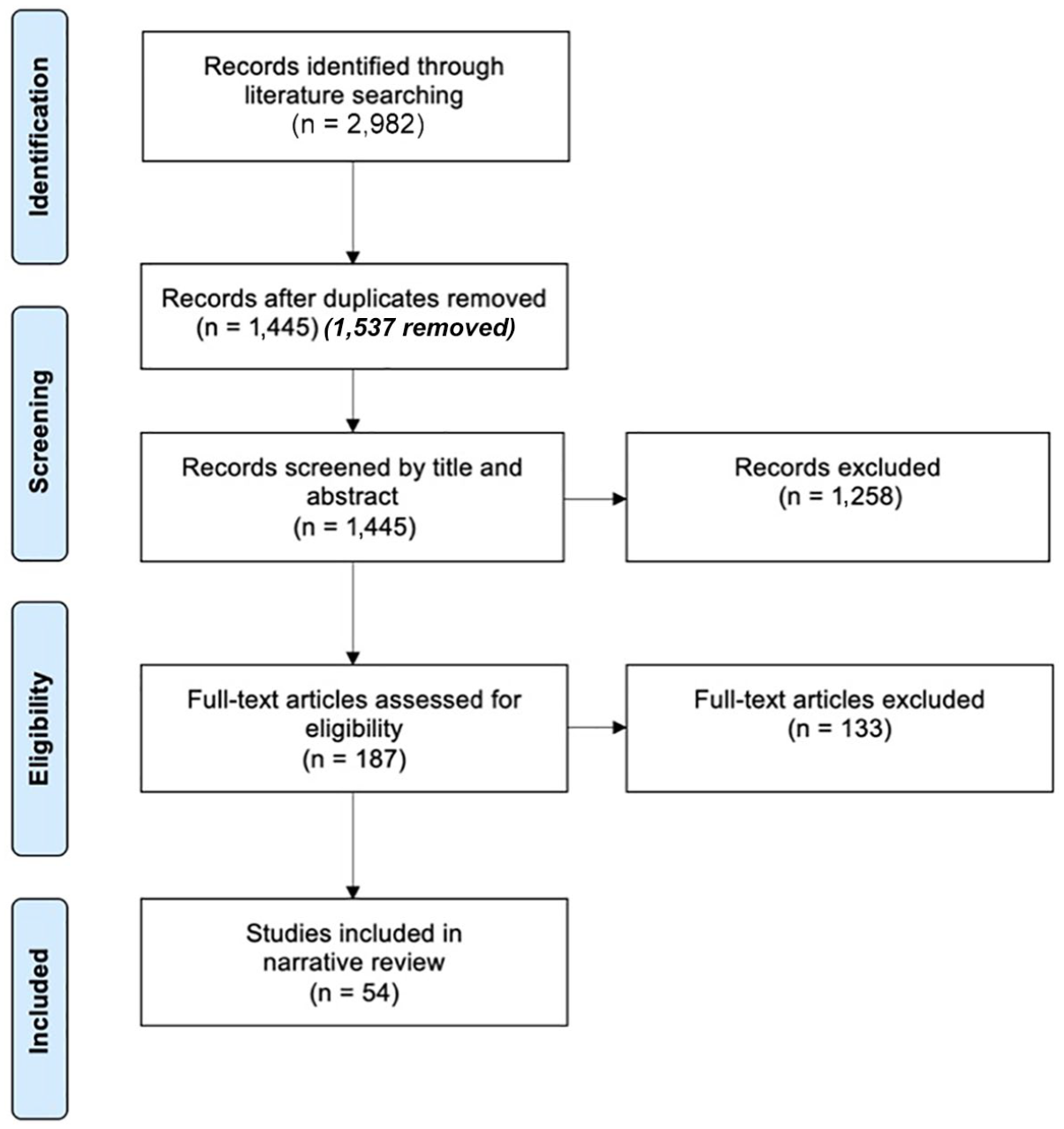
PRISMA flow diagram of search results
The majority of included results were primary research articles (n = 48) including cross-sectional studies (n = 33), longitudinal studies (n = 11), case-control studies (n = 2) and case reports (n = 2). Several discussion papers (n = 6) all included primary research data or primary research case studies (see supplementary material).
The reviewed studies were published between January 2000 and June 2021. Unsurprisingly, the publication rate has increased over time: 30 of the 54 studies have been published since 2015 and 12 since 2020. The increasing rate suggests ongoing evidence synthesis will be required.
Most studies were conducted in Asia (n = 26) and Africa (n = 20). A further seven studies were conducted in South America and one in North America (see supplementary material).
Most studies (n = 42) focused exclusively on informal settlements or slums while some (n = 12) also studied formal areas. Only 12 studies explicitly defined informal settlements or slums, most commonly using the UN Habitat definitions, although most mentioned characteristics such as lack of secure tenure without specifying a definition.
b. Extreme weather events
Flooding was the most discussed extreme weather event. Of the 54 studies, 40 discussed flooding and heavy rainfall events. This contrasts with Borg et al.,(32) who found temperature-related exposure to be the most common weather event discussed in their sample of 15 studies. The impacts of landslides were explored in two studies in our sample focused on flooding,(33) although the occurrence of landslides in informal settlements was more widely noted. Storms were discussed in four studies, although many of their health impacts were discussed in terms of the associated flooding. One of these four studies(34) discussed wind; however, intense wind was not more widely discussed. Although “storm”, “hurricane”, “cyclone” and “typhoon” were included in the search strategy, including the term “wind” in future reviews may be beneficial. Extreme temperatures were discussed in 19 studies; 12 focused on heat specifically, the remaining seven discussed other forms of extreme weather as well, including the impact of cold temperatures in three studies. Six studies discussed droughts and water scarcity, but not exclusively. While the occurrence of fires was noted,(35) surprisingly the relationship between fires and extreme weather events and the resulting impacts on health were not explored in depth. Again, future reviews may consider adding “fire” to their search terms.
While many studies suggested the more general health impacts of extreme weather events and climate change while emphasising the vulnerability of informal settlements, this analysis only includes the health impacts found in the studied informal settlements.
c. Health impacts of extreme weather events
Health impacts of floods
Seventeen studies found informal settlements were in areas exposed to flooding, including coastal areas, low-lying areas, floodplains, and near rivers and waterways. Immediate health impacts of floods included injuries and high mortality (see Table 2). During floods in Lagos, Nigeria in 2011, of 607 households surveyed in Badia informal settlement, 27 people reported the death of a household member.(36) In another study of the same settlement, 7.6 per cent of surveyed women (n = 262) reported the death of a household member and 14.1 per cent reported injuries sustained by household members. Women in more affluent areas reported no deaths or injuries.(37)
Health impacts of floods
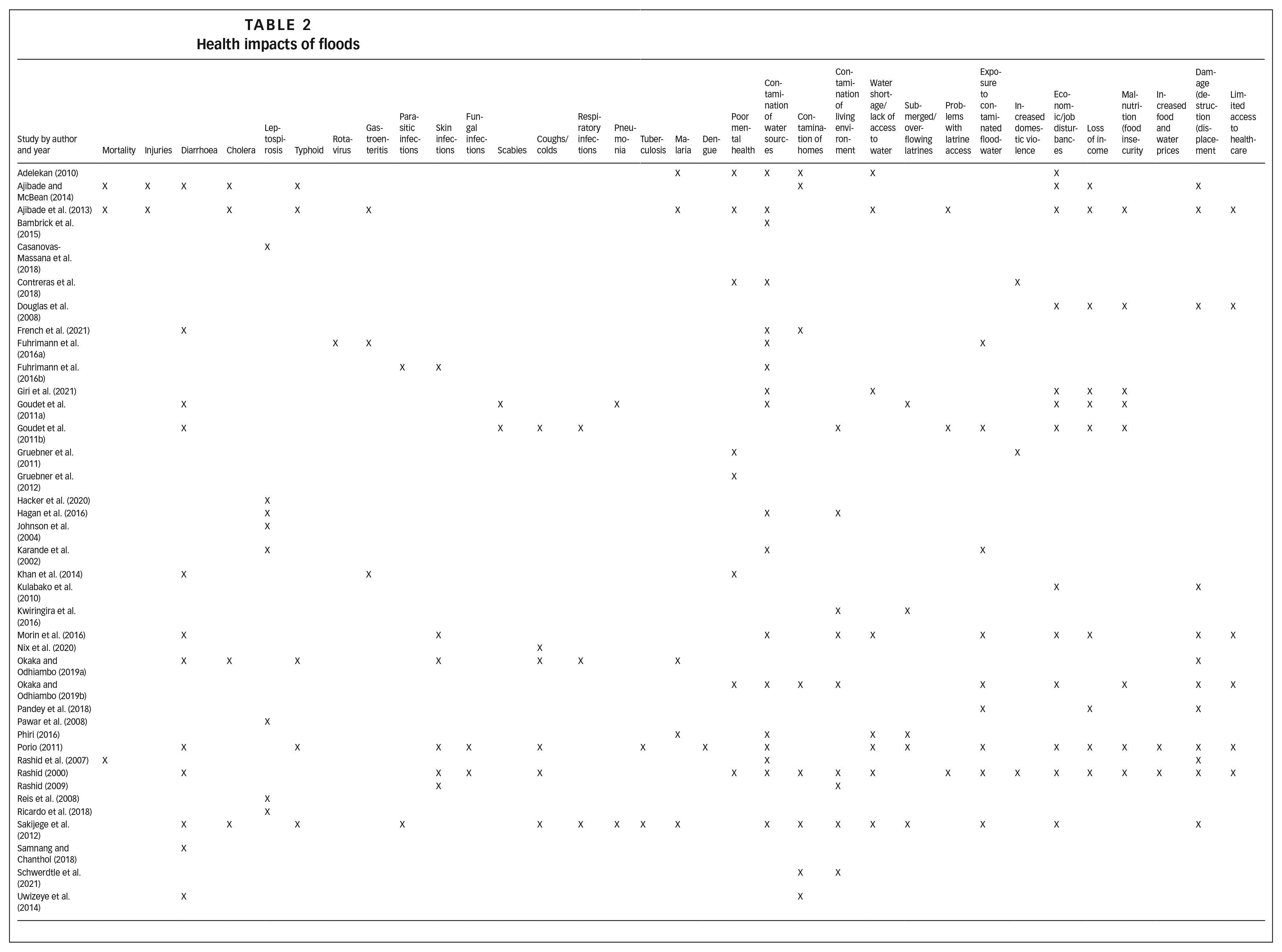
Studies also identified the contamination of water sources, homes and living environments during floods as a major health hazard (see Table 2). Several studies found that the contamination of water sources led to water shortages and limited access to safe water, resulting in worsened sanitation and hygiene. During floods, many pit latrines were submerged by floodwater and overflowed, and human waste spread into homes and around the settlements. Residents also reported problems in accessing latrines. In Lagos, Nigeria(38) and Dhaka, Bangladesh(39) for example, women were constrained by insecurity and lack of privacy during floods and had to relieve themselves at night or in their own homes. Limited access to sanitation facilities also affected bathing and personal hygiene. In an informal settlement in Kampala, Uganda, Kwiringira et al.(40) found that sanitation facilities overflowed, and were dirtier and more difficult to clean compared to the dry season. In these studies, the impacts of floods were shaped by existing inequities in access to water and sanitation facilities, including those related to gender. Both gender and provision of water and sanitation will be discussed further as determinants of vulnerability in Section IV d.
Many studies found that infectious disease burdens significantly increased during and after flooding events, including from water- and food-borne diseases (diarrhoea, typhoid, gastroenteritis, leptospirosis, cholera and rotavirus), skin problems, respiratory conditions and vector-borne diseases (see Table 2). Direct contact with dirty floodwater and contaminated drinking water sources increased the risk of disease during floods, especially for children who often played in contaminated floodwater.(41) Households at a lower elevation in informal settlements were more exposed to flooding and had increased risk of typhoid,(42) leptospirosis(43) and diarrhoea.(44)
Studies also found an increase in mental health problems associated with floods. In informal settlements in Mombasa, Kenya, 80.8 per cent of 390 households reported problems with mental health during the last flooding event, linked to the trauma of losing property and having nowhere to live.(45) In Lagos, Nigeria,(46) households reported the inability to sleep, loss of appetite, stress, and fear of future floods.
Women across informal settlements in Lima, Peru(47) and Dhaka, Bangladesh(48) reported an increase in domestic violence during floods. Women in Dhaka said this was due to increased stress on their husbands to provide for their families in times of financial hardship and unemployment.
Floods also had less direct impacts on health, related to changes in food consumption, food security, increased food and water prices, livelihood disruption and loss of income (see Table 2). Damage and destruction of homes and displacement added to both economic and health burdens.
Health impacts of extreme temperatures
Five studies described settlements in areas that were vulnerable to extreme temperatures. Cross-sectional studies in informal settlements in Nairobi, Kenya,(49) Kolkata, India(50) and informal townships in Gauteng and Mpumalanga, South Africa(51) found that populations there were exposed to temperatures over 40°C. Although the health impacts were not recorded, these temperatures exceeded the thresholds at which negative health impacts and increased mortality would be expected.(52) Three further studies in Nairobi, Kenya(53) and Ahmedabad, India(54) found associations between high temperatures and increased mortality in informal settlement populations, specifically in Egondi et al.(55) for children under four years of age and people with non-communicable diseases.
Populations living in informal settlements reported heat-related symptoms and serious impacts of heat including heat-related illness, infectious diseases, poor mental health and other non-communicable health problems (see Table 3). In three studies, people reported that heatwaves and hot summer temperatures affected their ability to work.(56)
Health impacts of extreme temperatures
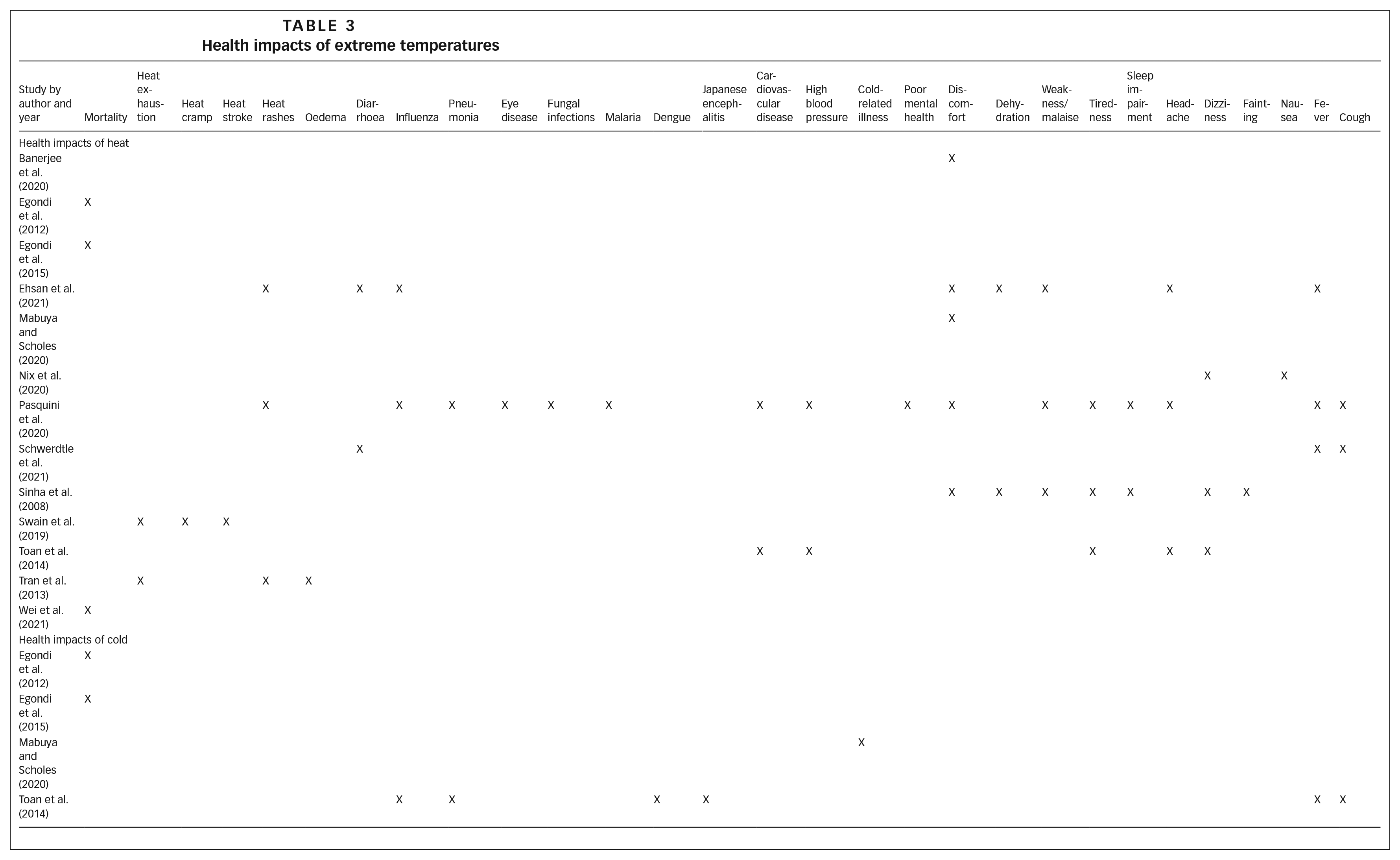
Four studies examined the effects of cold weather on health (see Table 3). Two studies in Nairobi found higher mortality rates in colder periods with high rainfall(57) and significant associations between lower temperatures and years of life lost.(58) “Shack dwellers” in townships in South Africa were found to be at higher risk of cold-related illness than people living in housing of better quality.(59) Informal settlement residents in Hanoi, Vietnam associated infectious diseases with cold weather.(60)
Health impacts of droughts and water scarcity
Few studies focused specifically on the health impacts of droughts and water scarcity; however, in informal settlements in Shasheme, Ethiopia,(61) residents experienced problems with washing and hygiene related to water shortages, and found malaria and typhoid were more common during the dry season, when temperatures were also higher. In informal settlements in Kampala, Uganda, Kwiringira et al.(62) observed that water scarcity during the dry season made it difficult to clean latrines. In Nairobi, Kenya, adolescents over the age of 10 and adults had three times the risk of typhoid after long periods without rain.(63) In four informal settlements in Dehradun, India, 25 per cent of 121 participants reported “health-related problems” due to droughts.(64)
Health impacts of storms
Shultz et al.(65) reported on the impacts of Hurricane Dorian in shanty towns in Marsh Harbour, Abaco Islands in the Bahamas in 2019. The study, mainly focused on mental health impacts, found the affected population suffered from acute psychological distress, acute grief reactions, major depression, generalised anxiety and post-traumatic stress disorder immediately after and in the months following the disaster. These responses were linked to loss, destruction, displacement, homelessness and unemployment resulting from the hurricane, which caused high mortality and severe injuries. In the aftermath of Typhoon Pedring in 2011, Morin et al.(66) identified vulnerability to typhoons and cyclones due to settlement location in Manila, mainly discussing the consequences of flooding and storm surges.
d. Determinants of vulnerability
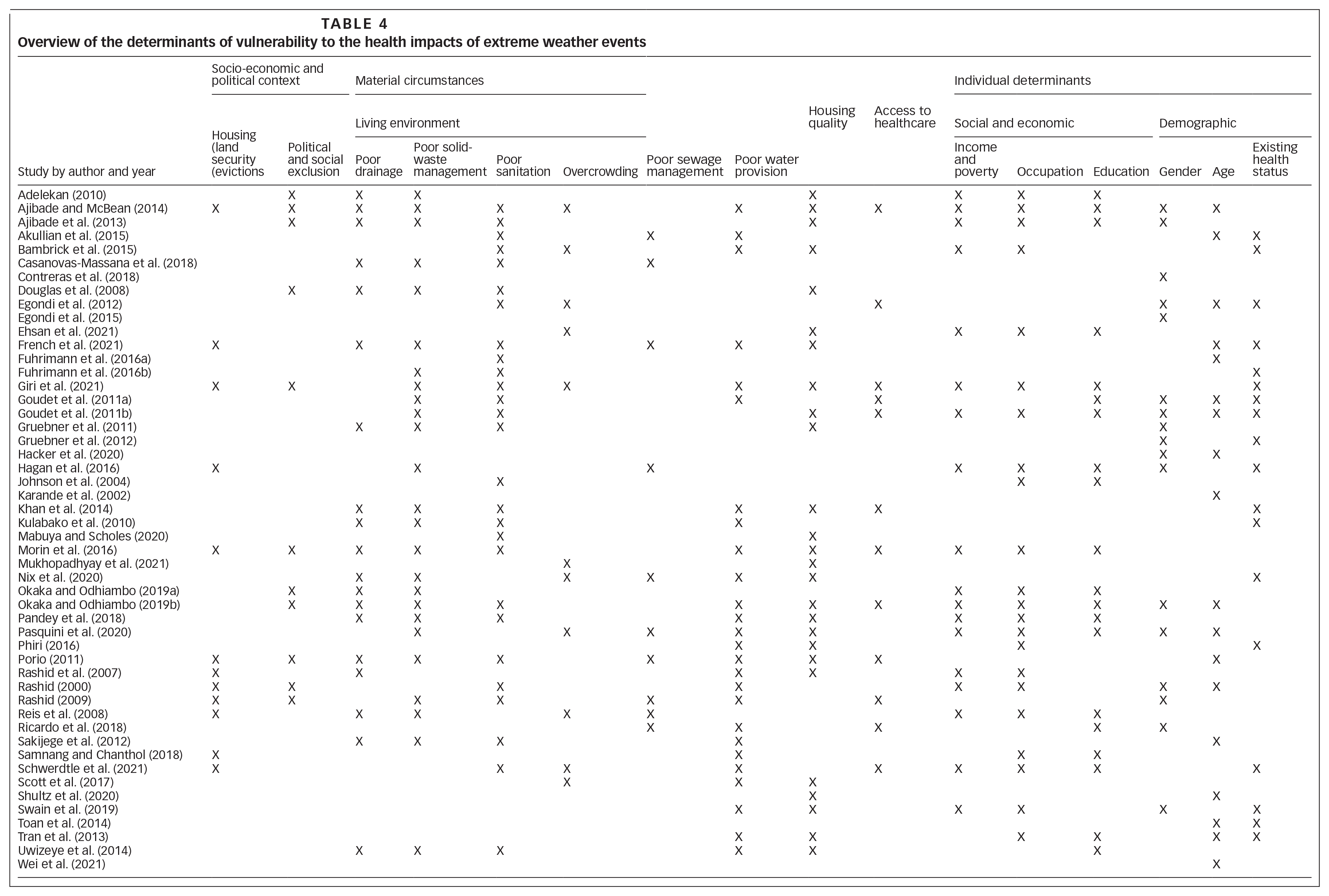
We examined the determinants mentioned in the studies to understand how the local context in informal settlements shapes vulnerability, including to the impacts of extreme weather events, and creates variation in health impacts. The overarching factors identified in the included studies are shown in Table 4 and are explored in more depth in the following section. We do not rigidly adhere to the broad categories of structural and intermediary determinants of health used in the SDH framework to structure our discussion. Instead, we consider specific determinants of health from the framework in the most logical sequence for this topic: beginning with the socio-economic and political context, then discussing material circumstances at settlement-level, and then individual-level determinants, including socio-economic status, demographic factors and health status.
Overview of the determinants of vulnerability to the health impacts of extreme weather events
Socio-economic and political context
In several informal settlements, the socio-economic and political context, including tenure insecurity and political and social exclusion, was found to contribute to the vulnerability to the health impacts of extreme weather events (see Table 4).
Housing rights, land security and evictions
Urban informal settlements are often considered illegal.(67) Studies noted that many residents have no legal title to their land and occupy marginal land including unauthorised governmental land.(68) As a result, many communities live under the threat of eviction and demolition.(69) Due to such threats, residents were reluctant to build more permanent and stronger housing structures that would provide them with more protection from extreme weather.(70) Samnang and Chanthol(71) also found that in informal settlements in Battambang, Cambodia, people were unable to relocate to safer land as they could not sell the land they currently lived on because they lacked formal land titles. Morin et al.(72) noted the occurrence of evictions following a typhoon. Okaka and Odhiambo(73) found fear of losing their homes stopped 4.3 per cent of respondents from evacuating during floods. The need to protect household belongings from theft was another reason for not evacuating.(74)
Political and social exclusion
Several studies suggested that governments refuse to provide infrastructure and services in informal settlements due to their illegal status. As a result, residents are often excluded from access to basic infrastructure and services, increasing their exposure and vulnerability to climate change impacts. In three studies in informal settlements in Lagos, Nigeria,(75) Accra, Ghana(76) and Mombasa, Kenya(77) participants believed poor planning and governmental exclusion and neglect increased the risk of flooding and flood impacts. Ajibade and McBean(78) found that households in Badia informal settlement in Lagos, Nigeria ignored government-issued typhoon warnings and did not evacuate because of distrust in the government, including fear of evictions.
In several studies, informal settlement residents reported receiving limited or no social and governmental support during and after extreme weather events. Morin et al.(79) found that although relief supplies and financial assistance were available for most typhoon-affected communities in Manila, there were many structural barriers to accessing this assistance. Many lacked the documents to apply for assistance and relocation and could not afford the fees to obtain them. Consequently, most households received relief supplies and financial assistance from families, friends and neighbours. Rashid(80) also found that flood-affected households helped each other. The absence or inadequacy of emergency responses(81) were also noted including the absence of emergency services.(82)
Studies in Dhaka, Bangladesh(83) and Lagos, Nigeria(84) found that the stigma attached to living in informal settlements limited the ability of women to find better jobs, increase their income, apply for loans and expand their social networks, thereby increasing their vulnerability during floods.
These wider social, economic and political factors, more difficult to research using conventional health research methodologies, are underexplored and significant knowledge gaps still exist, including limited community-level analysis of the contribution of socio-political marginalisation to vulnerability.
Material circumstances (physical environment)
Living environment
The living environment in informal settlements was found to contribute to increased risk of disease, flooding and the health impacts of floods and heat (see Table 4). Inequities in access to adequate water and sanitation shaped the health impacts of flooding for many. For example, in flood-affected informal settlements in Lagos, Nigeria,(85) Dhaka, Bangladesh(86) and Dar es Salaam, Tanzania,(87) floodwater was contaminated with human excreta from overflowing latrines, sewage and garbage and increased the risk of diarrhoea, typhoid and cholera. Several studies found increased risk of leptospirosis in households in closer proximity to open sewers.(88) Poor water supply and high water prices were identified as risk factors in many informal settlement communities.(89) Several studies found that wells, springs and other water sources were contaminated with faecal products, even without flooding. Phiri(90) found that wells built near latrines posed a great risk of contamination, especially during floods. A reliance on shallow wells, often submerged by floodwater, was also a risk.(91) Many people resorted to drinking dirty water during floods, increasing their risk of disease.(92) Goudet et al.(93) reported that even water in pipes became polluted during floods, increasing the risk of diarrhoea. Several studies found that the lack of access to safe drinking water increased the risk of diarrhoeal disease.(94) Water used for drinking(95) and bathing(96) was also identified as an important coping strategy against heat; however, this also relied on water availability.
Several studies identified health impacts related to crowding and population density. In an informal settlement in Dar es Salaam, Tanzania, participants noted that the high building density increased heat.(97) Ehsan et al.(98) also suggested that a densely populated environment adds to the urban heat island effect. Scott et al.(99) found significantly higher temperatures in the densely populated informal settlements in Nairobi than those recorded by the local weather station, especially at night. Mukhopadhyay et al.(100) found longer periods of dangerous heat stress in households with greater numbers of occupants in Kolkata, India. In Lagos, Nigeria,(101) Accra, Ghana(102) and Mombasa, Kenya,(103) informal settlement residents perceived overpopulation and overcrowding as causes of flooding.
Housing quality
In several informal settlements, poor-quality homes were more vulnerable to flooding and heavy rain (see Table 4). Morin et al.(104) found that during the 2011 typhoon in Manila, homes in informal settlements made from wood, sheet metal and plastic were often not strong enough to withstand storm surges. Several studies found that poor housing quality increased exposure to heat. Mabuya and Scholes(105) found that “shacks” made from corrugated iron, mud blocks, and other cheap materials were most vulnerable to high indoor temperatures and temperature fluctuations compared to houses made of more durable materials. Ehsan et al.(106) studied low-income neighbourhoods in Faisalabad, Pakistan and found that houses in the shade of trees or neighbouring buildings and with well-ventilated rooms had a lower heat discomfort index. Another study in two informal settlements in Kolkata, India, found longer periods of dangerous heat stress were positively associated with corrugated tin and asbestos sheet roofs, dwellings with only one room, and households with greater numbers of occupants.(107) Housing material may combine with other factors such as energy sources to increase the risk of fires. In Lagos, Ajibade and McBean(108) found that accidental fire outbreaks were related to wood construction and the use of kerosene lamps and candles. Accidental fires also undermined housing quality, increasing the impacts resulting from heavy rain.
Access to healthcare
In many informal settlements, access to healthcare was identified as a problem, both lack of provision(109) and affordability.(110) Participants in several studies associated this with the increased risk of illness.(111) A lack of access to healthcare was found to be exacerbated during floods.(112) Porio(113) found that in three informal settlements in Manila, those with lower incomes resorted to using traditional healers during floods. In Mombasa, Kenya, Okaka and Odhiambo(114) found that of 390 studied households, 22.3 per cent had to walk through floodwater to access healthcare services and 13.1 per cent found this difficult or impossible.
Individual determinants: social, economic and demographic determinants and health status
Several studies emphasised that poverty, low income, occupation, education, gender, age and existing health status shaped and diversified the vulnerability of informal settlement residents to health impacts of extreme weather events (see Table 4).
Income and poverty
While many studies described the greater exposure to environmental hazards of those who cannot afford to live in safer locations, only three studies discussed in depth how poverty increases exposure to environmental hazards and contributes to vulnerability.(115) For example, Hagan et al.(116) found that households in Salvador, Brazil with lower incomes lived at lower elevations and had greater exposure to contaminated soil, mud and water during floods, leading to higher leptospirosis infection risk.
Immediate coping strategies and longer-term adaptive capacity were also influenced by income. For example, in informal settlements in Dar es Salaam, Tanzania(117) and Bhubaneswar and Cuttack, India,(118) income limited adaptive responses to heat such as air conditioning and refrigeration. Rashid et al.(119) found that in informal settlements in Dhaka, financial constraints prevented people from flood-proofing their homes and adopting other effective adaptive responses. They also found that without significant economic incentives, participants chose not to relocate from flood-prone areas, partly due to moving costs. Ajibade et al.(120) found that after flooding in Lagos in 2011, women in informal settlements were more severely affected than women living in more affluent areas. They struggled to restart their businesses due to lack of capital and an inability to rebuild. Morin et al.(121) found that 45 per cent of typhoon-affected households in informal settlements had to take out loans to cope with the storm’s impacts. Okaka and Odhiambo(122) found that 73 per cent of 390 participants in flood-affected settlements in Mombasa would not evacuate, mainly due to financial constraints.
Occupation
Several studies found that the occupations of informal settlement residents often exposed them to climate hazards (see Table 4). In Mombasa, Okaka and Odhiambo(123) found that small traders were among those more vulnerable to the health risks of flooding but did not expand on reasons for this. Studies in Dar es Salaam, Tanzania,(124) Dhaka, Bangladesh(125), Bhubaneswar and Cuttack, India(126) and Ahmedabad, India(127) found increased vulnerability to heat exposure and related health impacts among residents who worked outdoors or in poorly ventilated areas. Poor job security made it impossible for participants in Dar es Salaam to reduce their hours to avoid the heat.(128) In an informal settlement in Manila, people received no compensation for missed days of work during the typhoon disaster, and some were fired.(129) Goudet et al.(130) found that rickshaw pullers in Dhaka could not work during floods, limiting their ability to buy food. Home-based work, common in informal settlements and particularly among women,(131) was found to be adversely affected by extreme weather.(132)
Education
Studies in Manila(133) and Mombasa(134) found that low educational status and illiteracy made households more vulnerable to the health impacts of floods. Low educational status and illiteracy were also linked to increased risk of leptospirosis in informal settlements Salvador, Brazil(135) and Iquitos, Peru,(136) a disease often exacerbated during floods. Morin et al.(137) found that during a typhoon disaster and subsequent floods in Manila, households with limited education could not read warning information and had limited access to post-disaster assistance due to the required paperwork.
Knowledge and awareness of information related to extreme weather were also found to be a determinant of vulnerability. Tran et al.(138) noted that those in Ahmedabad, India who sought information about heat illness had reduced odds of heat-related illness, possibly because they were more likely to avoid heat exposure. Several studies identified limited knowledge and poor awareness about climate change, risks and impacts(139) and limited disaster-related training.(140)
Gender
While women were generally considered to be more vulnerable to the impacts of climate change and extreme weather, few studies examined this in great depth (see Table 4). Pasquini et al.(141) found that women and children suffered more from heat exposure as they had to remain indoors at night due to safety concerns. Ajibade and McBean(142) and Okaka and Odhiambo(143) found that women were more vulnerable to the health impacts of floods but neither study expanded on this. Goudet et al.(144) found in two separate studies that during floods, mothers often significantly reduced their own food intake to feed their husbands and children. As discussed earlier, women suffered from domestic violence(145) and problems with sanitation during floods.(146) Gruebner et al.(147) noted that in flood-affected informal settlements in Dhaka, Bangladesh, men had better mental well-being, but did not explore this. Only one study provided an in-depth analysis of the gendered impacts of floods in an informal settlement. Ajibade et al.(148) found that in Badia informal settlement in Lagos, polygamy played an important role in shaping financial vulnerability and ability to recover from disaster. Because husbands could not provide for all their wives and children, women were obliged to generate additional income. Most women did not perceive flood impacts to be gendered, but researchers found that women suffered greater economic and material losses working from inside their homes, greater difficulty caring for their children, and more problems with sanitation, privacy and access to clean water.
On the other hand, in Salvador, Brazil(149) and Santa Fe, Argentina,(150) men faced a higher risk of leptospirosis. Ricardo et al.(151) suggested that in Santa Fe this was due to increased occupational exposure. Egondi et al.(152) identified higher cold-related mortality among men in a study from Nairobi but suggested no reason for this. Swain et al.(153) found that in Bhubaneswar and Cuttack, India, men were at higher risk of heat-related illness due to their occupations and outdoor activities.
Social class (beyond income), ethnicity, race and religion were not discussed as determinants of vulnerability in any of the included studies. The potential contribution of cultural influences, including health beliefs, climate change risk perception, traditions, gendered health inequalities and social structures, is also underexplored in the literature.
Age
Age was found to influence vulnerability to the health impacts of extreme weather events (see Table 4). Children had greater exposure to contaminated water during floods, increasing their risk of diarrhoea,(154) rotavirus,(155) leptospirosis,(156) water-borne infections,(157) dengue,(158) and respiratory infections.(159) Vulnerability also varied within the under-18 category. Akullian et al.(160) found that the risk of typhoid in children under 10 almost doubled for every 10-metre decrease in elevation of households in Kibera, Nairobi, Kenya; however, the risk of typhoid was not associated with elevation or location in adolescents and adults. In Makassar, Indonesia, French et al.(161) identified a higher prevalence of diarrhoea in children under five compared to older children and adults. Children were also vulnerable to malnutrition during floods.(162) Egondi et al.(163) found significant associations between child mortality and both increased and colder temperatures in two informal settlements in Nairobi.(164) Pasquini et al.(165) identified children as more vulnerable to heat but did not expand on this. In contrast, Shultz et al.(166) found that children showed fewer mental health impacts compared to adults in the aftermath of Hurricane Dorian in the Bahamas in 2019.
The elderly have also been identified as especially vulnerable to the health impacts of extreme weather. In Mombasa, Kenya, Okaka and Odhiambo(167) found adults over the age of 51 were among the most vulnerable to the health risks of flooding, but did not expand on this. In Ahmedabad, India, Tran et al.(168) noted increased odds of self-reported heat-related illness and symptoms among those over 60. Wei et al.(169) found people over 65 the most susceptible to heat mortality, while Egondi et al.(170) found those over 50 years most susceptible to cold temperatures.
Existing health status
Across different studied informal settlements, health status was found to be poor, with high burdens of infectious diseases (including diarrhoeal diseases and other food- and water-borne and water-related diseases), vector-borne diseases (including malaria and dengue), parasitic infections, pneumonia, tuberculosis, and HIV and AIDS, as well as malnutrition, poor mental health, and other non-communicable diseases (see Table 5).
Existing health status
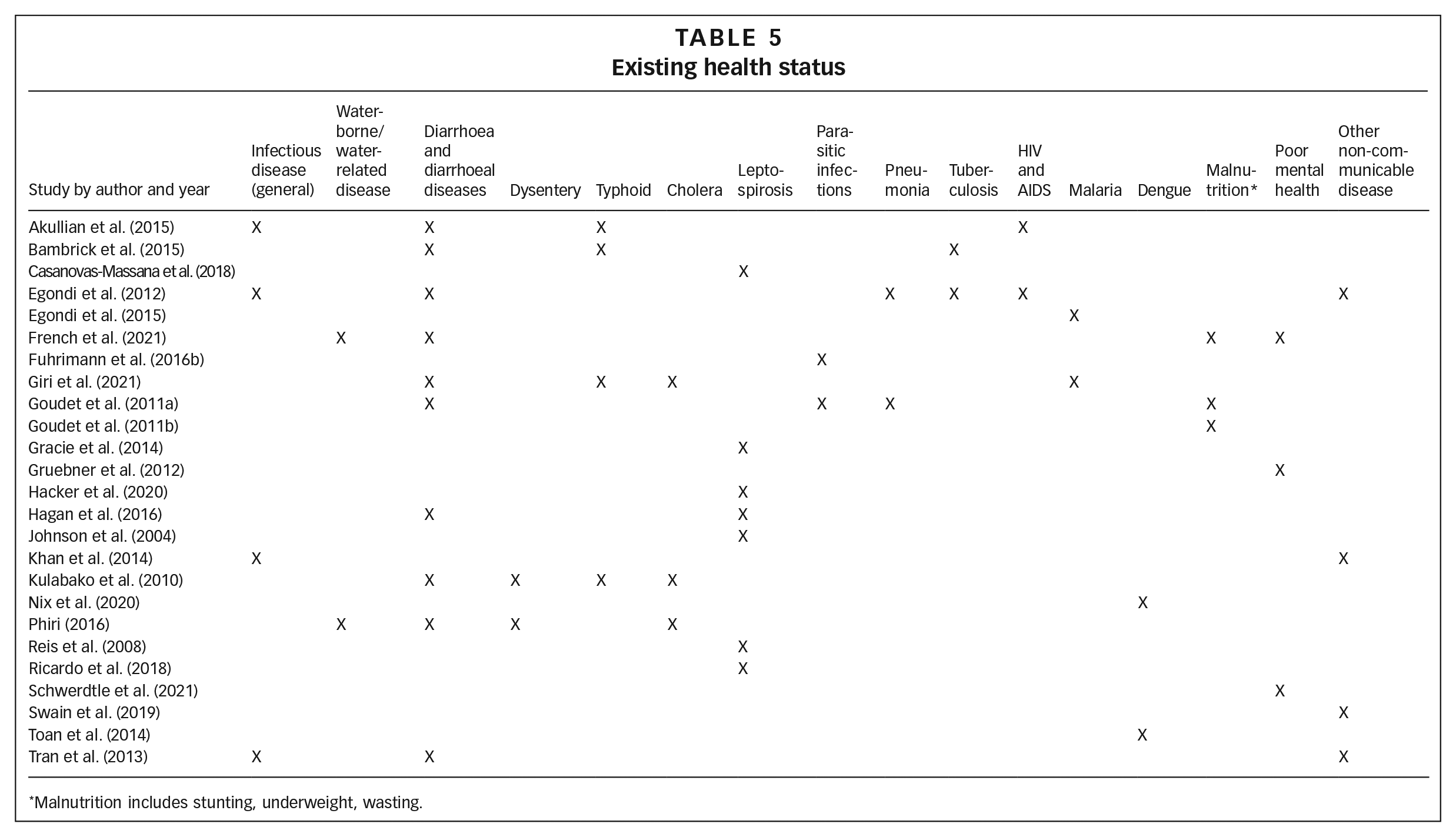
Malnutrition includes stunting, underweight, wasting.
Several studies found those with pre-existing disease to be more vulnerable to the health impacts of heat and flooding. Swain et al.(171) and Tran et al.(172) found in study sites in India that people with pre-existing chronic conditions and infectious diseases had an increased risk of developing heat-related symptoms and illness. Egondi et al.(173) identified significant associations between mortality and high temperatures among people with non-communicable diseases in Nairobi. A study in Mombasa found that households with a member with a chronic illness or disability were among those most likely to be highly vulnerable to the health impacts of flooding.(174) Only one other study mentions disability, but does not discuss this further as a determinant of vulnerability.(175)
Interactions between the determinants of vulnerability and health impacts of extreme weather events
Previous sections have demonstrated how each of these contextual factors shape the vulnerability of people living in informal settlements to the health impacts of extreme weather events. Although sometimes these factors contribute to vulnerability in isolation, often they overlap, influence each other, and shape vulnerability through a complex web of interactions and interdependencies, as exemplified in Figure 2. The complexity of these interactions creates variations and diversity in the vulnerability among individuals living in informal settlements.
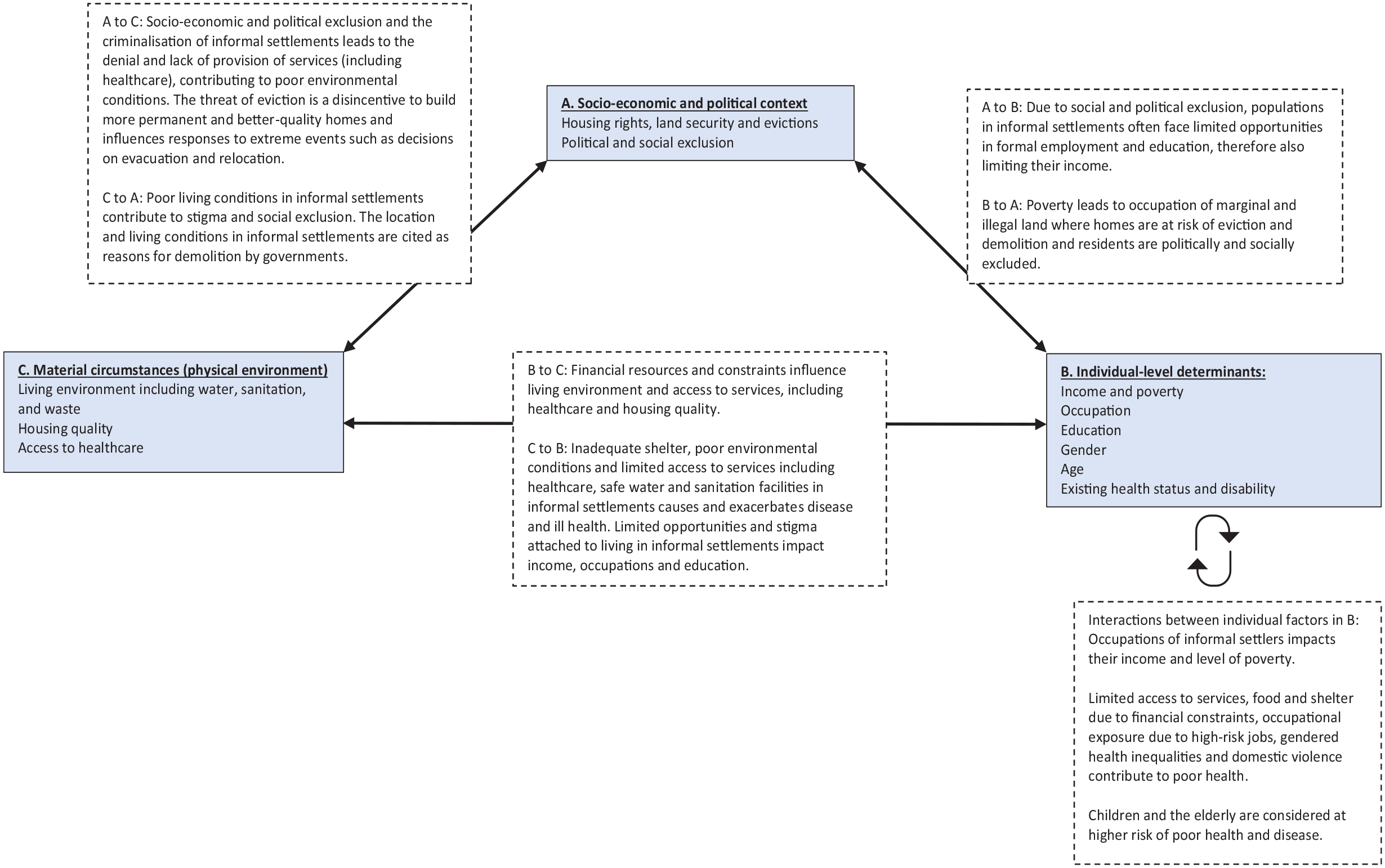
Interactions between the determinants of vulnerability to the health impacts of extreme weather events
A limitation of the use of the SDH framework to guide the analysis of this review is that it may lead to the erroneous understanding that determinants operate in isolation, whereas in reality they overlap both within and across structural, intermediary and individual levels. For example, the living environment is heavily determined by the inadequate service provision that is a product of the socio-economic and political context. Socio-economic factors, such as the inability to recover after floods, could be considered as both individual and community-level impacts with structural-level determinants. However, the SDH framework locates poverty at the individual level. To effectively respond to climate change, individual, social and economic determinants must be understood and addressed as products of larger, intersecting socio-economic and political systems of power.
V. Discussion and Conclusions
This paper presents the most comprehensive review to date of the literature on the health impacts of climate change in informal settlements, focusing specifically on extreme weather events. The narrative review has considered 54 studies, published between 2000 and June 2021. Our search results show that this is, unsurprisingly, an expanding body of research and that a continuing synthesis of findings will be required. Moreover, we found that the extent of the available research on extreme weather events varies by topic. While flooding is relatively well-studied within the sample, few studies consider water scarcity and drought, which is evidently an area for future research. Notably, only 12 of the 54 studies explicitly defined informal settlements/slums, most of these using UN Habitat definitions. Given the heterogeneity of these contexts, we recommend that future studies provide a detailed characterisation of their context with reference to existing definitions to enable more granular analysis of the way specific features relate to health impacts and their social determinants.
Our analysis of the 54 studies shows the wide-ranging health impacts of floods, extreme temperatures, droughts and storms in informal settlements. These include both direct impacts such as injury, disease and death, and the more indirect health impacts resulting from the effects on livelihoods, environmental conditions, access to healthcare, coping strategies and adaptive capacities. Importantly, when compared to the review by Borg et al.,(176) this review has drawn on a greater body of evidence on the mental health impacts of flooding, and indicates that other extreme weather events, including extreme temperatures and storms, can also negatively impact mental health.
The review of the health impacts, combined with the thematic analysis of their social determinants, highlights the fact that health impacts are not uniformly experienced within informal settlements, but are first shaped by the extent of the exposure, often influenced by location, including where people live within settlements. Then, individual characteristics and markers of disadvantage (including age, gender and socio-economic position) interact with material circumstances and access to healthcare influenced by the wider socio-economic and political context to shape adaptive capacity, causing variations in vulnerability to the impacts of climate change. For example, differing degrees of exposure related to location and the presence or lack of infrastructure and service provision, combine with individual vulnerabilities to determine the impacts of extreme weather events. However, some determinants of vulnerability to extreme weather have been insufficiently researched. For example, some aspects of health, such as disability, are rarely mentioned. Socio-economic characteristics including class, religion and culture or community dynamics such as social capital and community-level power inequities are not considered in the studies. Moreover, access to healthcare and the response of the health system during disasters has been relatively underexplored. These are all areas in need of further research.
These findings have clear implications for policy responses. First, responses need to consider variation in within-settlement vulnerabilities. Our review has reinforced the need identified by Sverdlik(177) for local governments to prioritise vulnerable groups and to be sensitive to “axes of difference” in their response to climate change, including age and gender. We have shown that the relationship between gender and vulnerability is not necessarily straightforward and needs to be understood in context. Strategies to minimise the impacts of climate change need to reflect and respond to these different vulnerabilities. To inform policy, further research into these other axes of difference is also required. This review has shown that for some factors, such as income, occupation and education, there is a small body of evidence, whereas other axes of difference such as religion, social capital and disability have not been explored.
Furthermore, intersectional analysis is required to identify how different axes of vulnerability – and the systems of power that underlie them – interact to intensify or mediate vulnerabilities in specific contexts. For example, gender, socio-economic status, age and (dis)ability all interact to create specific positionalities and thus vulnerabilities for individuals. These positionalities and vulnerabilities are shaped by dynamic intersections between systems of power, including patriarchy, ableism, class relations and the political economy of informality in specific contexts. To illustrate, when we combine the analyses of gender and occupation within the studies, it is clear that these two factors interact in context-specific ways, to shape vulnerabilities and ultimately the impacts of extreme weather events. Researchers and policymakers must take an intersectional approach, examining and responding to these intersecting identities and determinants. Here we can learn from and expand on existing intersectional analyses of the social determinants of health (such as that of Hogan et al.(178)) and of urban development (for example Rigon and Broto(179)).
Second, to adapt to and minimise the health impacts of climate change including extreme weather events in informal settlements, comprehensive multi-sectoral responses are required which address the wider social determinants of health. National and local governments must ensure that health services are physically and financially accessible at all times, including during extreme weather events. Actors from diverse sectors, representatives of grassroots organisations, and those living and working in informal settlements must be brought together to build climate-resilient health systems. Addressing health impacts requires not only improved access to healthcare, but also improvements in livelihoods, education and access to services including water and sanitation, with attention to government provision and health inequities.
The theory of syndemics, which analyses how diseases synergistically interact with each other and their social context to increase health burdens in specific populations, may have utility here.(180) The material conditions within informal settlements increase the risk of a range of diseases, which we have shown to be amplified by extreme weather events. Adaptive and coping strategies are constrained by the same material conditions, which share common socio-economic and political determinants. Individual vulnerabilities are further shaped by various intersecting axes of disadvantage and existing health status, both of which further interact. The health impacts of informality and climate change therefore cluster and reinforce each other in specific contexts. Many of the health impacts of climate change and poor health in informal settlements can be linked to the same root causes, embedded in contextual factors, that determine vulnerability. Addressing these health impacts therefore means addressing these root causes. For example, we found that the pre-existing risk of diarrhoeal diseases for informal settlement populations was exacerbated during floods. Increases in diarrhoeal diseases were found to exacerbate child malnutrition, showing the negative synergy between health impacts.(181) These synergistic health impacts occurred because floods exacerbated existing deficiencies in provision of sanitation and safe drinking water, and often in food security, which are underpinned by the political economy of informality. Promoting resilience to the health effects of climate change requires that these social determinants be tackled.
Overall, we must go beyond simply labelling informal settlements or even slums as “vulnerable to climate change”. As we have shown, vulnerabilities vary within and between settlements and are caused by multiple intersecting inequalities and determinants. Further detailed empirical research at the individual, household and community level, fully embedded in the wider social and political context, is needed to both understand and minimise the health impacts of climate change.
Supplemental Material
sj-pdf-1-eau-10.1177_09562478221083896 – Supplemental material for Climate change and health in informal settlements: a narrative review of the health impacts of extreme weather events
Supplemental material, sj-pdf-1-eau-10.1177_09562478221083896 for Climate change and health in informal settlements: a narrative review of the health impacts of extreme weather events by Emma Hambrecht, Rachel Tolhurst and Lana Whittaker in Environment & Urbanization
Footnotes
Funding
The research which informs this article was undertaken by the first author as part of their Master’s dissertation at the Liverpool School of Tropical Medicine (LSTM) and was supervised by the second and third authors. The second and third authors’ time for supervision and the writing of this article was supported by the Global Challenges Research Fund (GCRF) Accountability for Informal Urban Equity Hub (ARISE), which is a UK Research and Innovation (UKRI) Collective Fund award with award reference ES/S00811X/1.
Supplemental Material
Supplemental material for this article is available online.
4.
Direct effects are those resulting directly from changes in temperature and precipitation including extreme weather events which cause injuries, illness and death. Indirect effects include those caused by changes in natural systems such as vector-borne diseases and those shaped by social responses such as displacement. See Haines and Ebi (2019) and ![]() .
.
8.
12.
The United Nations Human Settlements Programme (UN Habitat, 2015) defines informal settlements as areas where residents have no tenure security, there is a lack of basic infrastructure and housing may not comply with regulations and be in hazardous locations. UN Habitat considers slums to be the most deprived and excluded forms of these settlements, with slum dwellers experiencing a lack of at least one of the following: improved water source, improved sanitation facilities, sufficient living area, housing durability and security of tenure. However, there is also great variation in informal settlements.
15.
23.
IPCC (2021); ![]() .
.
27.
31.
33.
53.
68.
69.
74.
Porio (2011); ![]() .
.
81.
109.
111.
115.
130.
132.
134.
144.
146.
147.
149.
152.
159.
Porio (2011); ![]() .
.
162.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.