
Abstract
Approximately half of all slums(1) in India are not recognized by the government. Lack of government recognition, also referred to as “non-notified status” in the Indian context, may create entrenched barriers to legal rights and basic services such as water, sanitation and security of tenure. In this paper, we explore the relationship between non-notified status and health outcomes in Kaula Bandar, a slum in Mumbai, India. We illustrate this relationship using the findings of a four-year long series of studies in the community. By comparing Kaula Bandar’s statistics with those from other Mumbai slums captured by India’s National Family Health Survey–3, we show that Kaula Bandar has relative deficiencies in several health and social outcomes, including educational status, child health and adult nutrition. We then provide an explanatory framework for the role that Kaula Bandar’s non-notified status may play in generating poor health outcomes, by discussing the health consequences of the absence of basic services. We also highlight the criminalization by the government of activities necessary for fulfilling access to fundamental needs such as water, toilets and shelter. We argue that the policy vacuum surrounding non-notified slums such as Kaula Bandar results in governance failures that lead to poor health outcomes. Our findings highlight the need for cities in India and other developing countries to establish and fulfill minimum humanitarian standards in non-notified slums for the provision of basic services such as water, sanitation, solid waste removal, electricity and education.
I. Introduction
India has the world’s second largest urban population and roughly 93 million Indians reside in urban slum conditions, which may adversely impact health.(2) Large-scale national datasets have highlighted the problem of intra-urban disparities in health and social indicators between slum and non-slum populations in India.(3) Fewer studies have explored the question of inter-slum disparities – the fact that even among different slums within a given city, there may be dramatic differences in access to resources and health outcomes.(4)
The variable legal status of different slums in the eyes of the government may be one factor that contributes to inter-slum health disparities. Each Indian state uses different policies to determine whether a community qualifies as being a legal slum. Being given legal recognition by the government is often a prerequisite to receiving municipal services such as piped water, toilets and electricity. Given the nature of the government’s selection criteria however, a de facto slum community may fail to secure de jure status. This categorization process results in two classes of slums: government-recognized slums (i.e. “notified” slums) and government non-recognized slums (i.e. “non-notified” slums). As per India’s 2008 National Sample Survey (NSS), approximately half of slums in India and 45 per cent of slums in Maharashtra (the state in which Mumbai is located) are non-notified.(5)
In this paper, we highlight the problem of inter-slum health disparities in Mumbai using the findings of a four-year series of studies of Kaula Bandar (known hereafter as KB), a non-notified slum. KB has a population of 10,000–12,000 people and is located on a wharf on Mumbai’s eastern waterfront (Photo 1). Originally established by Tamil migrants more than 50 years ago, KB has seen the arrival of migrants from north India in recent years. By comparing data from KB to statistics from Mumbai slums captured by India’s National Family Health Survey–3 (NFHS–3), we show that KB’s health indicators are relatively worse than those of other Mumbai slums. We then provide an explanatory framework for the role that KB’s non-notified status may play in generating poor health outcomes, and discuss the larger implications for governance and public health in slums.

Aerial view of Kaula Bandar: 10,000–12,000 people live on a wharf on Mumbai’s eastern waterfront
II. The Legal Backdrop
To appreciate the implications of non-notified status, the legal backdrop governing slums in Mumbai must first be understood. The rights of slum dwellers residing on city-owned land in Maharashtra are delineated in a 1995 addendum to the Maharashtra Slum Areas Act of 1971.(6) The addendum states that the city government must extend basic amenities (for example water and sanitation) to slum residents who have proof of residency prior to 1 January 1995. Such residents are also entitled to security of tenure and rehabilitation in formal housing in the event of displacement from their homes. While this addendum established entitlements for some slum dwellers, others who arrived in Mumbai after 1995, or who lack pre-1995 proof of residency, are barred from legally receiving basic amenities and security of tenure from the municipality.
Rare exceptions have been made to the “1995 rule”. For example, during expansion of the railway lines for the Mumbai Urban Transportation Project, all project-affected individuals were rehabilitated in new homes with no regard for any residency cut-off date.(7) In addition, certain projects designated as being of vital public importance have been allowed to use a more liberal cut-off date of 1 January 2000 for identifying families that should benefit from resettlement; however, every cut-off date modification requires extensive legal proceedings in court by the government of Maharashtra. Despite such rare exceptions, on the whole the “1995 rule” has created significant inequality in access to resources between and within slum communities, especially with regard to water and sanitation.
KB faces additional legal barriers to accessing resources, since it is located on land belonging not to the city government, the Municipal Corporation of Greater Mumbai (MCGM), but rather to a central (federal) government agency, the Mumbai Port Trust (MbPT). The Constitution of India places certain vicinities in Mumbai (including seaport, railway, airport and defence areas) under the legislative jurisdiction of the central government, which means that Maharashtra state government regulations do not apply in these areas. The state government therefore cannot engage in any activities (for example, extension of water and sanitation services to slums) on these lands without obtaining a document called a No Objection Certificate (NOC) from the respective central government agency responsible for that land.
Central government agencies are hesitant to provide NOCs, as they fear that extension of services by the state government may bolster slum dwellers’ claims to land tenure. Even though state government policies are not applicable, the central government has not formulated a coherent slum policy to fill this legal vacuum.(8) As a result, slums on central government land occupy a legal “no-man’s land”, whereby no government authority takes responsibility for providing access to basic services.
In addition to these well-defined legal barriers, we also argue that KB has been the victim of other, less tangible impediments to resource access. The “non-notified slum” label becomes a conceptual lens through which government officials view communities. This de-prioritization of non-notified slums may prevent extension of particular resources to these slums even when legal barriers technically do not exist or can be negotiated. To use Appadurai’s phrase, non-notified slum residents may be viewed as “citizens without a city” – residents who are deprived of their right to city resources not only on de jure but also on de facto grounds.(9)
III. Methods
a. Research collaboration
In 2008, researchers from Partners for Urban Knowledge, Action and Research (PUKAR), the Harvard School of Public Health (HSPH) and New York University (NYU) formed a collaboration to perform a series of public health studies in KB. Research units were formed across institutions to optimize skills sets. HSPH students collaborated with PUKAR’s research coordinators and “barefoot researchers”, who are Mumbai youth (many of whom are from KB) trained in data collection techniques by PUKAR. Ethics committees at PUKAR, HSPH or the Harvard Medical School approved all study protocols.
b. Data sources and statistical analysis
Data for this comparative study come from two sources, the datasets on KB from the PUKAR–HSPH–NYU collaboration and the datasets from India’s NFHS–3. Indicators from all datasets were summarized using STATA (v12, College Station, TX).
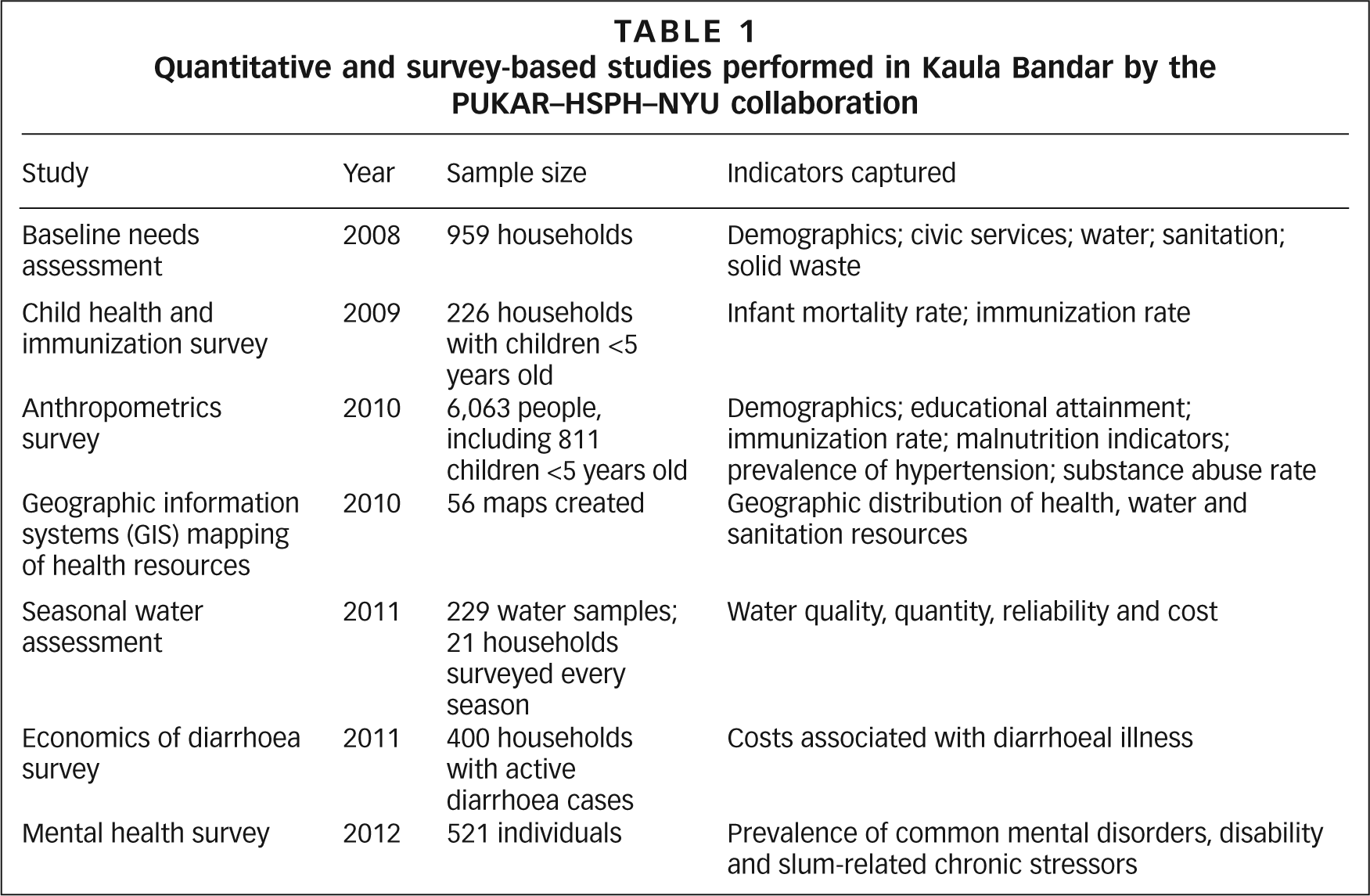
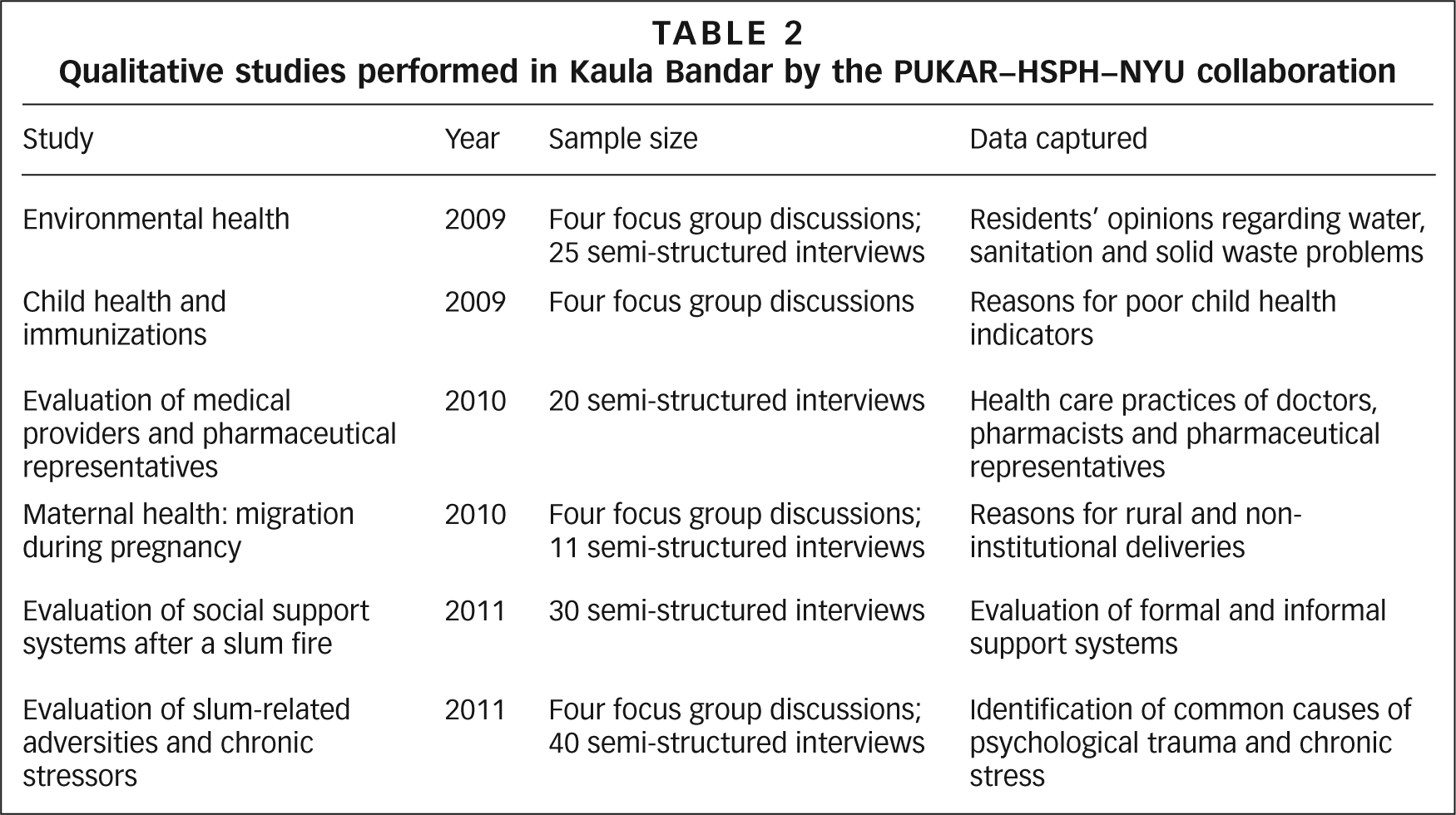
Tables 1 and 2 summarize the quantitative and qualitative studies performed by the PUKAR–HSPH–NYU collaboration. Studies evaluated “core” public health indicators (for example immunization rates) and less commonly studied issues (for example mental health). The findings of the 2010 anthropometrics survey are particularly relevant to our investigation of inter-slum disparities, so we will therefore briefly discuss the methods used in that study.(10)
Quantitative and survey-based studies performed in Kaula Bandar by the PUKAR–HSPH–NYU collaboration
Qualitative studies performed in Kaula Bandar by the PUKAR–HSPH–NYU collaboration
The anthropometrics survey collected health and social information (for example literacy and immunization history) as well as anthropometric measurements (for example height and weight). Instruments were harmonized with NFHS to allow for comparison. Every weekend from March 2010 to January 2011, a uniformly trained team of two physicians, four research coordinators and 20 “barefoot researchers” collected data from KB residents after obtaining informed consent. To facilitate participation, researchers visited each home at least three times for recruitment. Anthropometric measurements were collected at a central tent that was moved to different locations in the slum. In total, data were collected from 1,701 households and 6,063 individuals, including 811 children under the age of five.
As a comparison to our findings from KB, we analyzed raw datasets from the NFHS–3, a nationally representative survey of health in India conducted in 2005–2006. These data can be disaggregated to look at specific urban sub-populations such as slums. The NFHS–3 collected data from a representative sample of 1,104 households in Mumbai that are classified as being located in slums according to the 2001 Census of India (hereafter referred to as “NFHS slums”). The 2001 census classified a community as a slum if it was notified or recognized by the state or local government, or if it contained more than 300 people (i.e. 60–70 households) and had an environment subjectively assessed as being “congested”, “unhygienic” or lacking in key infrastructure.(11) Therefore, the comparative analysis that follows highlights inter-slum variability through a comparison of the “average” slum conditions in Mumbai (as represented by the NFHS slums) with the conditions of the particular slum of KB.
IV. Relative Deficiencies in Health and Social Outcomes in Kaula Bandar
Tables 3–5 present a comparison of demographic information, basic household information, basic services, educational status and child health indicators between KB and the NFHS slums.
Demographic information, basic household information and access to basic services for residents in Kaula Bandar vs. Mumbai slums in the NFHS–3(1)
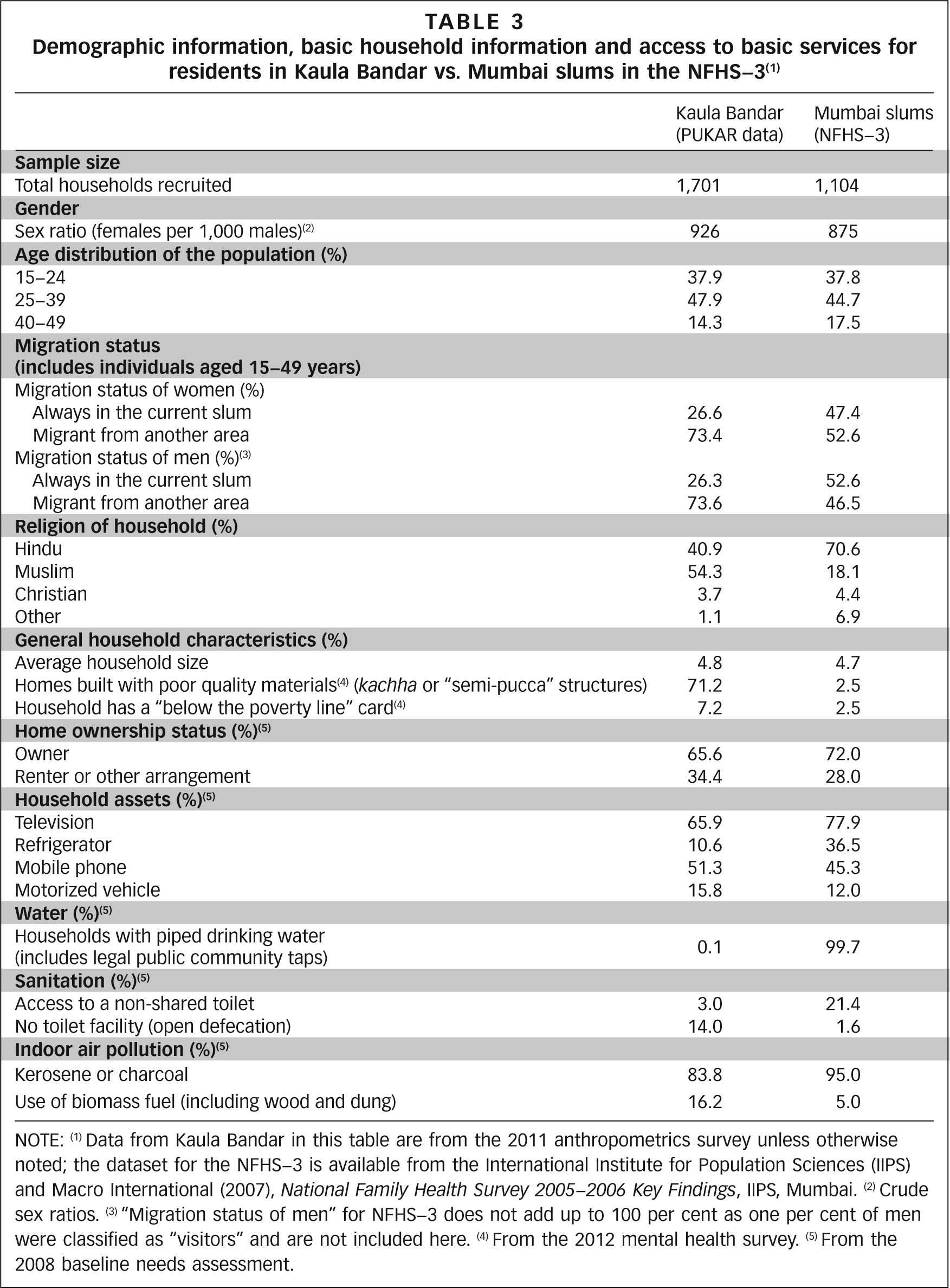
NOTE: (1) Data from Kaula Bandar in this table are from the 2011 anthropometrics survey unless otherwise noted; the dataset for the NFHS–3 is available from the International Institute for Population Sciences (IIPS) and Macro International (2007), National Family Health Survey 2005–2006 Key Findings, IIPS, Mumbai. (2) Crude sex ratios. (3) “Migration status of men” for NFHS–3 does not add up to 100 per cent as one per cent of men were classified as “visitors” and are not included here. (4) From the 2012 mental health survey. (5) From the 2008 baseline needs assessment.
Literacy and educational attainment for residents of Kaula Bandar vs. Mumbai slums in the NFHS–3(1)
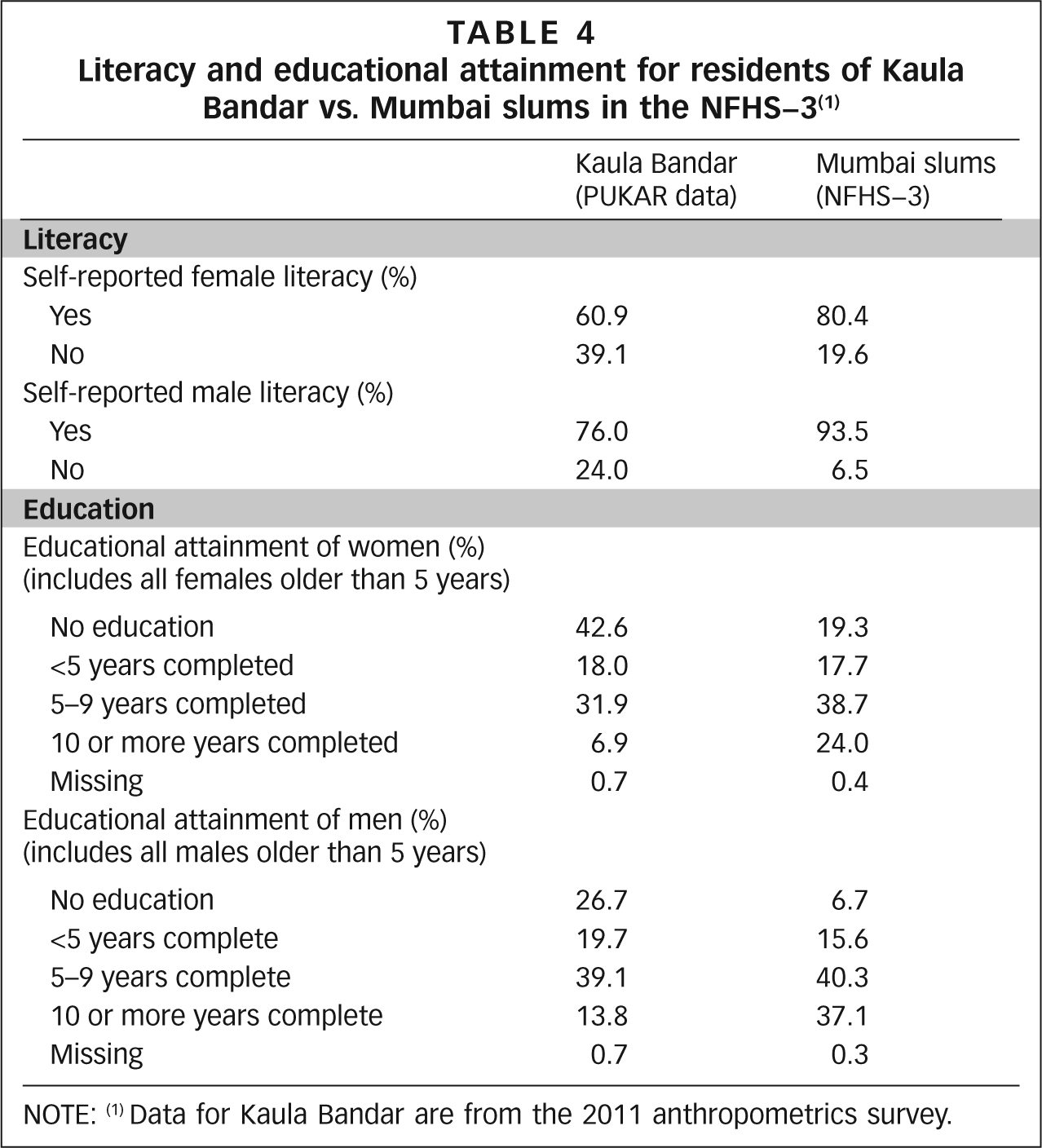
NOTE: (1) Data for Kaula Bandar are from the 2011 anthropometrics survey.
Child health indicators in Kaula Bandar vs. Mumbai slums in the NFHS–3(1)
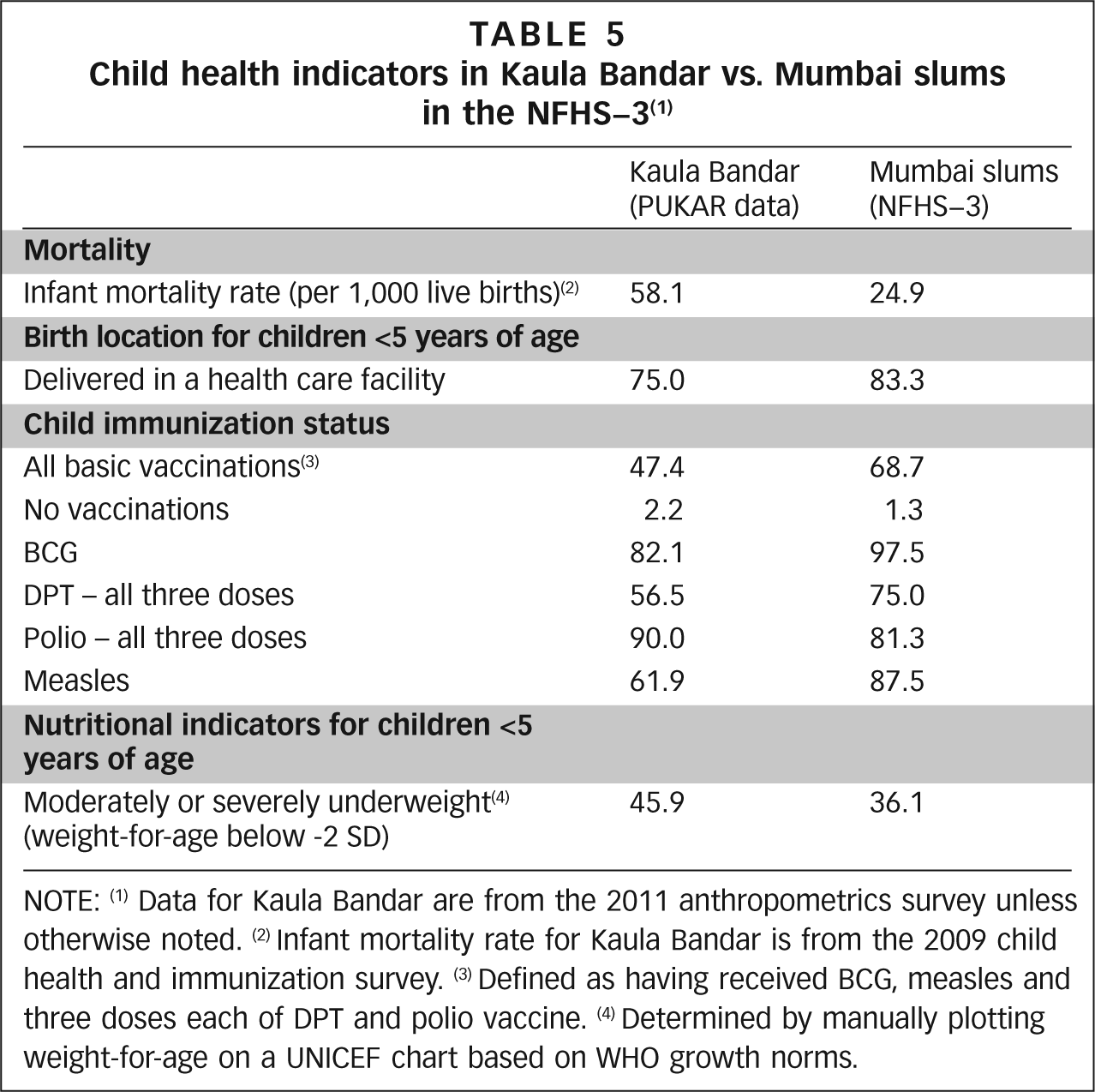
NOTE: (1) Data for Kaula Bandar are from the 2011 anthropometrics survey unless otherwise noted. (2) Infant mortality rate for Kaula Bandar is from the 2009 child health and immunization survey. (3) Defined as having received BCG, measles and three doses each of DPT and polio vaccine. (4) Determined by manually plotting weight-for-age on a UNICEF chart based on WHO growth norms.
Table 3 shows that the age distribution and mean household size in KB are very similar to those for the NFHS slums. KB has a higher proportion of migrants, a higher proportion of Muslims, a higher proportion of homes built with poor quality materials, a lower rate of home ownership and a lower rate of ownership of assets such as a refrigerator or television.(12)
Table 3 also highlights a significant gap in access to basic services. Access to piped water (through community or home water taps) is almost universal in the NFHS slums, while virtually no KB households have access to piped water. KB residents have a lower rate of access to a non-shared toilet and a higher rate of open defecation among adults. A higher proportion of KB households use biomass fuels for cooking, which is associated with an increased risk of lung disease.
Table 4 shows that the proportion of women who are illiterate and who have no education is twice as high in KB compared to NFHS slums. The education gap for men is even more dramatic, with the proportion of men who are illiterate or who have no education being more than three times higher in KB.
Table 5 shows that nearly every child health indicator in KB is worse than in the NFHS slums. Infant mortality is more than twice as high in KB; the rate of fully immunized children is substantially lower in KB; the percentage of children who are moderately or severely underweight is higher in KB; and the percentage of children born in a health care facility (i.e. institutional delivery) is lower in KB. The institutional delivery rate is a key indicator not only of child health but also of maternal health, since it is associated with decreased maternal mortality.
With regard to adult nutrition, KB has a relatively higher proportion of men who are underweight (32 per cent vs. 25.6 per cent in the NFHS slums). Interestingly, nutritional status in women exhibits a different pattern, with KB having a slightly lower proportion of women who are underweight (20.3 per cent vs. 23.1 per cent) and a higher proportion of women who are overweight or obese (37.1 vs. 25.1 per cent). This differential may partly be explained by differences in employment. Women in other slums are often employed as domestic workers, whereas KB has a low rate of female employment outside of the home, which may lead to a more sedentary lifestyle and increased obesity.
V. The Connection between Lack of Government Recognition and Health Outcomes
The comparative analysis above highlights just how large inter-slum health disparities can be. What accounts for KB’s disparate health outcomes? In this section, using data and observations from our studies, we argue that KB’s non-notified status is a major contributing factor to its relatively poor health and social indicators. Our argument focuses on the following issues: access to water, access to sanitation and solid waste removal, access to electricity, access to municipal schools, access to official documents, access to compensation following disasters, and forced eviction.
a. Lack of access to the municipal water supply
KB’s non-notified status precludes it from accessing the municipal water supply or taps (Table 3). Residents must instead purchase water through an informal distribution system managed by private vendors living in KB. Using motorized pumps, vendors extract water from underground water pipes that were originally placed by the fire brigade for emergency use in case of fires. This water is pumped through rubber hoses that travel hundreds of metres to reach community lanes, where residents pay monthly (and sometimes weekly) fees to vendors to receive and store water in their homes. Due to inconsistent supply, the majority of residents only access water every three or more days. A few times a year, government officials raid vendors’ motors, cutting off water access to all of KB’s residents. During these episodes of “system failure”, residents obtain water by rolling 300-litre drums up to two kilometres to a nearby community that has functioning water taps (Photo 2).

Girls from Kaula Bandar roll a barrel down the road to fill with water from a tap in the next community during a failure of the informal water distribution system. Residents cite the lack of a formal water supply as a barrier that sometimes prevents children from attending school
In the 2011 seasonal water assessment (Table 1), we performed an extensive study of the consequences of this informal water distribution system, the full results of which are described elsewhere.(13) In every season and during an episode of “system failure”, researchers collected water samples from several points along the water distribution system, while also administering a survey to, and testing water samples from, 21 KB households. Our findings reveal that this informal distribution system fails to fulfill the most basic standards for key health and social equity indicators, namely water quality, quantity, cost, accessibility and reliability.
In terms of water quality, we found that half of point-of-source water samples from vendors’ motors were contaminated with coliform bacteria during the monsoon. With regard to quantity, 95 per cent of households did not get enough water to meet the World Health Organization’s (WHO’s) recommended minimum usage of 50 litres per capita per day (LPCD), and 48 per cent of households did not even get 20 LPCD, a usage level associated with “high” health risk according to WHO.(14)
Poor water quality and inadequate quantity are independently associated with poor health outcomes, especially with regard to diarrhoeal illness.(15) Studies of slums globally have found diarrhoea to be one of the top two causes of mortality in children under the age of five.(16) Recurrent diarrhoea is a major contributor to child malnutrition and poor cognitive function, which result in decreased educational attainment.(17) Improvements in water quality and quantity have each been shown to reduce rates of diarrhoea by as much as 25–33 per cent.(18)
Water insecurity may also indirectly impact health by negatively affecting income, livelihood and education. In different seasons, the fee that KB residents pay to water vendors is 52–206 times the standard municipal water charge of 2.25 rupees per 1,000 litres of water that residents of notified slums pay. This represents 6–16 per cent of the average monthly household income, a spending level that in some cases could be catastrophic. Due to highly unpredictable water timings, 39 per cent of adults report that the water situation adversely affects their or their family members’ ability to go to work.
Livelihood is more severely affected during episodes of “system failure”, as described below by a 20-year-old north Indian male focus group discussion participant:
“Last week, I was in Goa for my job. My parents called me and told me to urgently come back because there was no water in KB. So I immediately left that job and came back home. I found that there was absolutely no water available. One of my friends in another community has a well near his home. I told him: ‘I am sending you a tanker to fill with water from your well. Then I will distribute that water’… On the third trip, the police stopped me… They fined me 1,800 rupees. They told me that it is illegal to bring water to this community… So the only remaining option is to pay 400 rupees and purchase water from the water vendors.”(19)
In the absence of a formal municipal water supply, the criminalization by local authorities of alternative modes of accessing water reinforces a cycle of poverty that may have several less immediately obvious long-term health consequences.
b. Lack of access to sanitation
KB’s non-notified status precludes it from getting government-built toilet blocks. Four small pay-for-use toilet blocks exist in KB, three of which were built by slum residents themselves with informal support from local politicians (although without formal government sanction). However, given the lack of reliable water supply, excessive use (due to high population density) and lack of maintenance, many of the toilets in these blocks rapidly become dysfunctional. There are in theory a total of 19 toilets seats for the entire population in these pay-for-use toilet blocks, but in fact there are fewer functioning seats. As a result, KB has a relatively high rate of open defecation among adults (Table 3) and it is universally practiced among children. Adults who regularly use toilets, especially women, often travel great distances to access pay-for-use toilets outside of KB.
Non-notified status also prevents the development of sewer infrastructure in KB. As a result, excreta from the pay-for-use toilet blocks in KB empties directly into the adjacent ocean. KB’s ocean water has a high fecal bacteria count in all seasons, and given that 31 per cent of residents report flooding of their homes with ocean water during the monsoon, much of the community is exposed to this excreta. The direct health consequences of inadequate sanitation are similar to those resulting from poor water access – increased diarrhoeal illness, child death, malnutrition and poor cognitive function.(20)
Our qualitative interviews highlight other indirect impacts of the lack of toilets on livelihood and income. Households report spending as much as 20–30 rupees per day and waiting for up to 60 minutes in queues at the pay-for-use toilets. For those who choose to defecate in the open, because of difficulties with the toilets, the criminalization of the practice by local authorities serves as a source of chronic stress. As described in this interview with a 30-year-old Tamilian male resident, the police harass adults who engage in open defecation:
“Sometimes, the police arrest people who defecate by the sea. Recently, they arrested more than 150 people… They took 50 to 150 rupees from each person and then let them go free. My children defecate by the sea, so each time they go there I’m scared they will get arrested. But my children go there because there is no other option. There are too many people at the toilets and it also costs too much money.”
As with water, criminalization of open defecation places additional financial constraints on already impoverished populations.
c. Inadequate collection of solid waste
Lack of government recognition also compromises solid waste collection. As per our qualitative interviews, solid waste collection in KB by the city government was minimal until a few years ago. As a result, residents have disposed of garbage in the surrounding ocean for the past few decades, and KB is now encompassed by a giant mass of refuse extending several metres out into the ocean at low tide (Photo 3). Over the last four years, a local corporator (an elected official) encouraged regular garbage removal through the Jawaharlal Nehru National Urban Renewal Mission, a central government initiative that provides external funding for social improvements.(21)

A child plays with a kite on a rubbish dump in Kaula Bandar at low tide; water hoses also run through the dump and open defecation takes place in the area
Despite this new effort, there are still limitations to KB’s garbage collection services. Municipal trucks do not travel the main road to collect waste from dumpsters located inside KB; instead, they only collect garbage from a single dumpster located immediately outside the slum.(22) Whether this failure is due to legal barriers to entering the slum or general unwillingness on the part of garbage collectors, the result has been that dumpsters in KB are persistently overloaded. Most residents therefore continue to dispose of their waste in the ocean.
Solid waste dumps negatively impact health by encouraging the proliferation of disease vectors such as rats, flies and mosquitoes. Proximity to garbage dumps in slums has been associated with increased rates of child diarrhoea, helminth infections, dengue fever and leptospirosis.(23)
d. Barriers to accessing the municipal electricity supply
Brihanmumbai Electricity Supply and Transport (BEST), a company managed by the city, provides electricity to many areas of Mumbai. In the past, BEST had been more liberal regarding providing electricity meters to KB residents and, as a result, some households established a reliable electricity supply for which they regularly pay the city. In recent years, however, BEST has refused to provide new electricity meters, citing legal barriers to providing this service on central government land. One 36-year-old Tamilian male resident describes the consequences of this:
“We applied to BEST for a proper electricity connection, but BEST told us that [KB] is [on MbPT] land. They told us that we first have to go to the [MbPT] officials to get a No Objection Certificate before they will provide us with electricity. In the past, a few people were able to get official meters… Now people are forced to steal electricity from whoever already has a meter. No one gets proper electricity in their homes because so many people are stealing electricity. Every month, BEST officials come just to cut [illegal] electricity connections and then leave. They never consider why people are forced to steal electricity in the first place.”
The health consequences of this situation arise largely from risks from illegal electricity wires, which cause electrocutions and overload fuse boxes. In our interviews, residents reported overloaded fuse boxes as being the most common cause of fires. One 42-year-old north Indian male resident describes the situation as follows:
“Many people who steal electricity often use a single meter and fuse box. There is too much load on that single fuse box. All my documents are ready and I keep them in a plastic bag. I am always ready at any time to run out with that bag if a fire breaks out.”
Another 30-year-old Tamilian male resident said: “We also fear that we will get shocked by these open connections. If you put your hand in the wrong place, that’s it, you’re finished.” This fear is not unfounded; at least two children died from electrocution in KB in 2011. In addition to the direct health consequences, poor access to electricity may indirectly affect health by adversely impacting livelihood opportunities and educational attainment, as lack of light inhibits studying.
e. Barriers to accessing municipal schools
In 1995, the government of India issued guidelines stating that government-run primary schools should be located within one kilometre for all children and that there should be at least one primary school per 3,000–4,000 people.(24) These basic educational standards have not been fulfilled in KB, and the nearest municipal primary school is more than two kilometres away. Given the population size of KB and other slums in its immediate vicinity, ideally there should be at least five primary schools within one kilometre of KB, as per government guidelines. The absence of a primary school in KB’s vicinity is odd, even in the context of India as a whole; since 1993, 94 per cent of India’s rural population has lived within one kilometre of a primary school.(25)
We argue that this gap in access to schools is largely a result of KB’s status as a non-notified slum. A UNESCO report evaluating primary education in Mumbai noted that the municipality has faced extensive difficulty in finding legal spaces to set up schools in slums on land owned by central government agencies such as the MbPT:
“[A] number of land-owning agencies of the central government in big cities, such as the Port Trust… allow slums to come up on their vacant lands, [but] are reluctant to permit the provision of basic services… The implication for locating schools near slum dwellings is obvious. If schools cannot be put where slums come up, the children of these colonies will be deprived of access to primary education. This is indeed the case in many areas of Mumbai, and parents and children have to fight hard to arrange for expensive transportation to the nearest schools.”(26)
Our interviews highlight the impact of inaccessibility to both schools and transportation to school in KB. One 48-year-old Tamilian female resident said:
“Every day we have to wake up at 5am to get [our child] out of here at 6am, so he can be at school at 7am. If the children show up more than five minutes late, they beat them and send them back home… If the schools were close by, we could at least walk there and easily make it on time. To get to this school he has to travel by train, and in the rainy season the train is often late. But they don’t listen to any of those excuses.”
The gap in school access may be one reason for the dramatic difference in literacy and educational attainment between KB and the NFHS slums (Table 4). Other resource limitations that result from non-notified status may have indirect impacts on education. Nine per cent of households reported that the water situation had a significant impact on their children’s ability to go to school. This is especially true when the informal water distribution system fails, since many children must miss school to roll drums back and forth to taps in other communities to fetch water (Photo 2).
Poor access to education has significant downstream health consequences. Studies from India, including an analysis of data from urban areas, have found that a mother’s educational attainment is one of the most important predictors of infant mortality, under-five child mortality, child nutritional status, immunization rates and institutional delivery rates.(27)
f. Difficulty in accessing official documents
Due to KB’s non-notified status, residents have difficulty accessing official documents that facilitate full civic rights. In contrast to residents of notified slums, KB residents have no possibility of obtaining home ownership documents that would establish security of tenure. Such exclusion from formal property rights may reinforce poverty by making people hesitant to upgrade their homes in the absence of legal protection against property loss.(28)
An even more fundamental document that KB residents have difficulty obtaining is a ration card. These facilitate access to subsidized goods such as wheat, rice, sugar, oil and kerosene through the government’s public distribution system, especially for families below the official poverty line. A ration card also serves as the most widely recognized form of proof of identity, which is sometimes required to access basic services, obtain formal employment and facilitate school enrolment.
In the 2008 baseline needs assessment (Table 1), we found that 33 per cent of households did not have a ration card. Vulnerable groups such as tenants (those renting living spaces) were significantly less likely to have a ration card. There is no specific regulation that prevents residents of non-notified slums from getting a ration card – however, the ration card application states that an applicant must supply some form of “residential proof”. Since KB’s residents live in a situation of informality, without official residential documents such as home ownership papers or rental agreements, providing appropriate paperwork is frequently impossible.
The lack of a ration card may affect child and adult nutrition indicators as they are unable to access subsidized food. The inability to get subsidized kerosene without a ration card may help explain the higher use of unhealthy biomass fuel in KB (Table 3). And as obtaining basic services and formal employment may be more difficult without a ration card, its lack may have an indirect impact on health by limiting livelihood options and deepening income poverty.
g. Discrimination in compensation provided after disasters and calamities
In February 2010, a fire broke out in KB that burnt down approximately nine per cent of homes in the slum (Photo 4). The government response to the fire shows how non-notified slum residents can be excluded from receiving meaningful compensation after a calamity. Since the central government does not have a policy of providing compensation to slum dwellers after disasters, the only monetary assistance that KB fire victims received came from the personal funds of local elected representatives. Every fire-affected family was supposed to be given 1,000 rupees per individual, up to a maximum of 5,000 rupees per household.

A family sits in the ruins of their home after the 2010 fire in Kaula Bandar
We subsequently evaluated the restitution process through interviews and an analysis of government records. Despite the fact that 251 households were affected (according to a census by PUKAR and community leaders), the government documents only listed 164 fire-affected homes. Of these, the records only noted providing compensation to 88 households (35 per cent of the fire-affected population). For the 164 households reported in the government documents, the total value of property lost by those residents was estimated at 8,729,500 rupees; however, only approximately 400,000 rupees was disbursed as compensation, which constitutes 4.6 per cent of the total estimated loss. Fire-affected families received no additional support for rebuilding their homes.(29)
The government response to a fire in the notified Mumbai slum of Behrampada contrasts greatly to the response in KB. In 2009, more than 1,100 shanties burned down in Behrampada, and the Maharashtra state government approved 65,000,000 rupees for rehabilitation, an amount per fire-affected household 37 times greater than that given to KB households.(30) In addition, the state government initiated the reconstruction of their homes on the same site within two weeks.(31) By contrast, fire-affected residents in KB had to muster the resources to re-build their homes themselves. Many of the tenants migrated out of the slum soon after the fire as they no longer had a place to live in KB.
Non-notified slums may be at increased risk of fires due to the presence of illegal electricity connections (see above) and the lack of a legal water supply, which makes fires difficult to control once they have started. Slum fires may have direct health consequences, including loss of life, burns and respiratory complications. Such calamities may have profound indirect impacts on health, by deepening asset poverty and negatively impacting mental health. Such consequences are likely more severe in non-notified slums such as KB, where government compensation after such calamities is minimal.
h. Forced eviction and loss of home
Residents of notified slums in Mumbai are protected from forced eviction. If displacement becomes necessary for redevelopment purposes, the government provides residents of notified slums with rehabilitation in formal housing. By contrast, KB residents have no legal protection against eviction or home demolition, and they have no right to rehabilitation in the event of displacement.
In our interviews, KB residents noted that the MbPT had been more aggressive in demolishing homes in the past. In the last two decades, most residents had not experienced forced eviction; however, many feared the possibility of this happening in the future, as they realized that they were unlikely to get any restitution. A small minority of residents who had arrived recently and had built homes on the few remaining open spaces in KB have faced recurrent demolition of their homes. At the time PUKAR researchers interviewed this 42-year-old north Indian man, the MbPT had demolished his home only four days before:
“[T]he [MbPT] broke down my home… In the past, they would come here and give us notice. They would tell us: ‘Leave your home in the next 40 days, otherwise we will break it down.’ This time, they came suddenly and just started breaking down my home… The [MbPT] took all our belongings… They told me that since my home was on Port Trust land, all the property inside of it belongs to the Port Trust. So they said: ‘We will give nothing back to you.’ I told them: ‘I am ready to pay you money to get my belongings back.’ But they refused.”
Such recurrent dispossession brutally reinforces poverty. People become unwilling to make long-term investments to upgrade the quality of their homes, as they fear that any such investment will be transient.(32) This logic may partly explain the dramatic difference in the proportion of homes built with poor quality materials in KB compared to the NFHS slums (Table 3). The KB resident interviewed above eloquently related this concern when describing his thoughts after the demolition:
“When they left, we immediately built our home once again on the same spot, using plastic. My home is still not completely proper. I have arranged four bamboo shoots and covered them with a plastic sheet. I spent 35,000 rupees to build that original home, for flooring and proper walls… I face great tension now. Do I make a new home or not? If I make a new home, I have no guarantee that they will not come again and break it down.”
It is likely that forced eviction has impacts on several health indicators, even though the precise associations may be difficult to measure. The effects on mental health may be profound, and the phenomenon of “root shock” in response to recurrent displacement has been described in the US setting.(33) After the demolition, the KB resident described his feelings of trauma and disillusionment:
“When my home was broken down it was traumatic. A home is a very beautiful place in our lives. I have a dream that one day I will eventually own my own home. I am an illiterate person but I know the importance of a good home. I lost everything. I will never forget that moment. It had an extremely difficult impact on my life.”
VI. The Structural Violence of Legal Exclusion in Indian Cities
“Structural violence… describes social structures – economic, political, legal, religious and cultural – that stop individuals, groups and societies from reaching their full potential… [and result in] the impairment of human life… Structural violence is often embedded in longstanding ‘ubiquitous social structures, normalized by stable institutions and regular experience’… Disparate access to resources, political power, education and health are just a few examples.”(34)
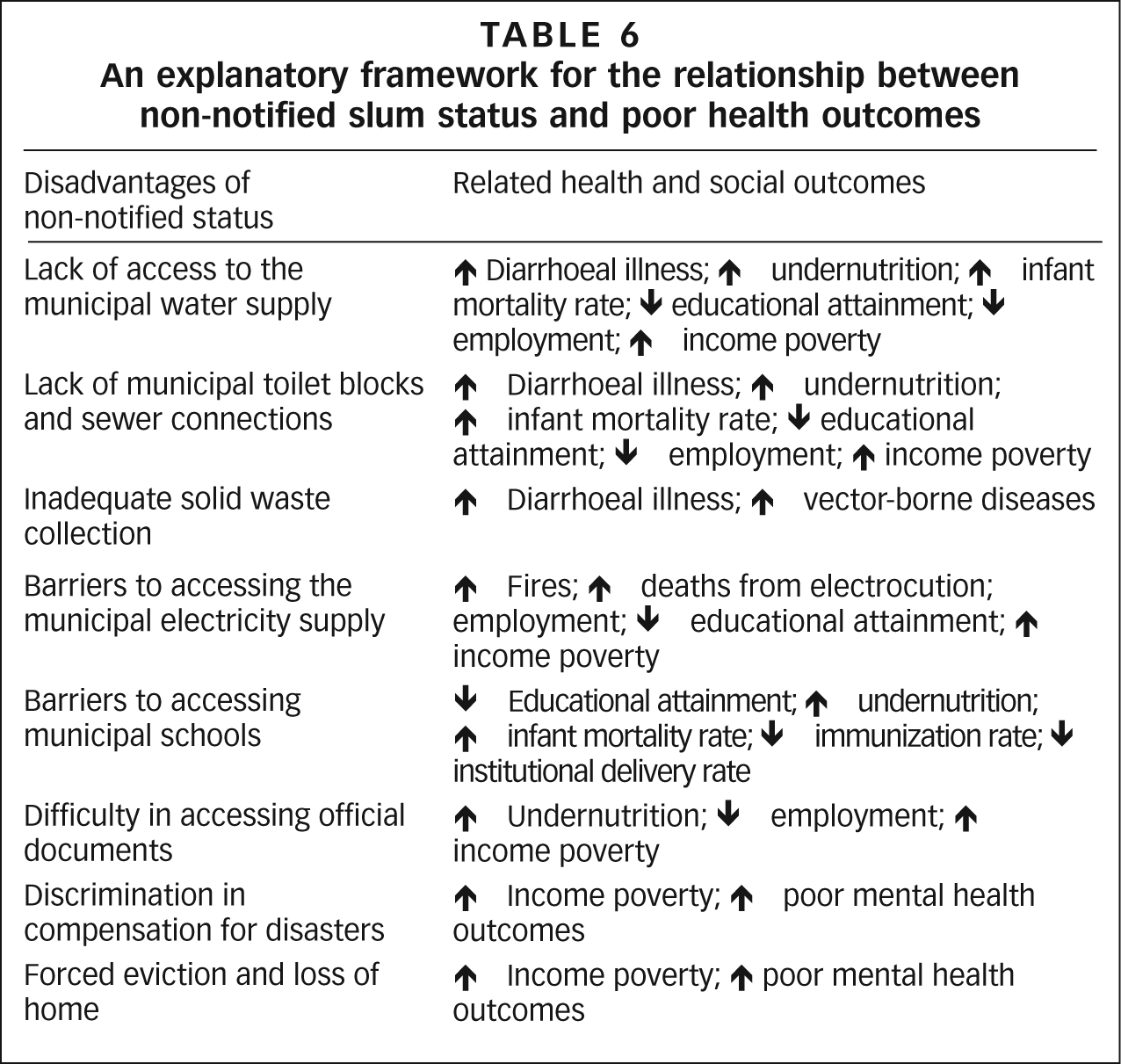
In this paper we have provided an explanatory framework for KB’s numerous health deficiencies relative to other Mumbai slums, by illuminating the larger social context of its status as a non-notified slum (Table 6). Based on four years of community-based research, we highlight the health consequences of widespread failures of basic entitlements that occur due to a legal vacuum. We also describe the way that activities required to fulfill basic human needs – water, toilets and shelter – are sometimes actively criminalized.
An explanatory framework for the relationship between non-notified slum status and poor health outcomes
We believe that our argument, although circumstantial, is persuasive. Residents of non-notified slums such as KB are subject to extensive structural violence from failures of governance. Social and legal exclusion become embodied in poor health outcomes; indeed, this structural violence takes its toll on the very lives and bodies of the urban poor.
In our argument, we focus on “proximal” causes of health outcomes (such as lack of access to water, solid waste collection and educational facilities) rather than on specific diseases (such as diarrhoea, leptospirosis and vaccine preventable infections), which represent the “distal” end causes of morbidity and mortality. Even more proximal to these failures of basic services is the policy framework that sanctions this system of exclusion. While provision of medical outreach services is crucial in addressing KB’s immediate health crisis, interventions focused on the proximal causes (for example provision of equitable water access) are equally crucial for a more comprehensive transformation of health.(35)
By focusing on the consequences of non-notified status, we do not intend to exclude completely other possible explanations for KB’s relative deficiencies in health outcomes. Since the NFHS–3 does not include income data, we were unable to compare the average household income in KB to that of the NFHS slums. However, differences in asset data (including the proportion of homes built with poor quality materials and ownership of a refrigerator, television or home) suggest that KB may be poorer on average than the NFHS slums.
While asset poverty may seem to be a simple alternative explanation for KB’s poor health indicators, we would argue that such an explanation does not minimize the influence of non-notified status on health. Our explanatory framework suggests that income and asset poverty in KB are themselves significantly influenced by lack of government recognition. For example, the threat and reality of home demolition may result in KB residents being hesitant to upgrade the quality of their homes; high spending on water as a proportion of monthly income reinforces income poverty; and a massive educational gap resulting from a lack of schools in the vicinity may adversely impact livelihood opportunities and income. Therefore, relative poverty alone is not a sufficient explanation for KB’s poor health status, given that income and asset poverty are also partly, if not largely, shaped by the slum’s non-notified status.
Another alternative explanation is that cultural differences between KB and other Mumbai slums may result in different health care-seeking behaviour. For example, KB’s low immunization rate could be due to cultural beliefs that inhibit mothers from seeking this care, rather than due to a resource gap in vaccine provision. In 2011, PUKAR advocated for outreach from the city government to provide immunizations through health camps in KB. These camps have witnessed a consistently strong response from mothers, which suggests that the primary barrier to child immunization was a resource gap rather than a cultural barrier. Indeed, overly focusing on “cultural difference” as a cause of ill-health in disadvantaged groups may cause us to overlook more glaring structural inequalities.(36)
VII. Conclusions
Kaula Bandar has very clearly been on the physical map of the city of Mumbai for more than 50 years. Indeed, it is located a mere 20 minutes away from India’s stock exchange, the literal epicentre of the country’s wealth. Over decades, KB residents have made meaningful contributions to the social and economic life of the city, often by serving in physically demanding occupations such as collecting garbage and disassembling decommissioned ships. KB also has thriving informal home industries producing low-cost goods that are largely consumed by more affluent Mumbai residents.
Despite their undeniable presence in the city, KB residents simultaneously occupy a legal “no-man’s land” – a zone absent of policies that address their existence as human beings and citizens of the city. In a conceptual and ethical sense, KB is therefore “off the map” of government officials, occasioning the denial and criminalization of access to basic services and entitlements. We argue that this legal vacuum results in structural violence that manifests itself in health indicators that are disproportionately worse than those of other slums in Mumbai. Our work highlights the problem of significant inter-slum variability in health outcomes within cities. Given the scale of the global slum population, creating methods for identifying the most vulnerable slums within cities will be critical for defining public health priorities equitably.(37)
We also believe that our findings emphasize the need to establish minimum humanitarian standards for non-notified slums with regard to access to basic services such as water, sanitation, solid waste collection and restitution after calamities. International guidelines, such as the Sphere charter that outlines minimum standards in disaster-affected areas, could provide a starting point for developing these criteria.(38) Until such an underlying policy framework is created, the health and livelihoods of residents of KB and other non-notified slums will continue to be “off the map”.
Footnotes
Acknowledgements
The Rockefeller Foundation was the primary funder for this project. The baseline needs assessment was funded by the Ford Foundation. Ramnath Subbaraman’s contribution was partly funded by numerous institutes of the National Institutes of Health through the Fogarty International Clinical Research Scholars and Fellows Programme at Vanderbilt University (R24 TW007988). Devorah Klein Lev-Tov facilitated transcription of dozens of hours of interviews. Sundar Burra of SPARC provided feedback on slum policy. We thank the residents of Kaula Bandar, who never hesitated to share their experiences with us. This paper is a tribute to their graciousness and perseverance.
The data analyzed in this paper were collected as part of a joint effort by researchers from Partners for Urban Knowledge, Action and Research (PUKAR), Mumbai, India; the Harvard School of Public Health (HSPH), Boston, USA; and New York University (NYU). The principal investigators were Arjun Appadurai (NYU), David E Bloom and Anita Patil-Deshmukh. In addition to the authors, the following researchers had a role in several of the studies: Prashant Kashid, Mahesh Nanarkar, Marjia Ozolins and Sima Shah; and the following researchers facilitated individual studies: Namrata Bagaria, Joya Banerjee, Laura Khan, Heather Lanthorn, Adriane Lesser, Ronak Patel, Kunal Sood, Hanni Stoklosa and Dana Thomson. Data collection for several studies was undertaken by PUKAR’s “barefoot researchers”, many of whom are youth living in Kaula Bandar.
1.
The term “slum” usually has derogatory connotations and can suggest that a settlement needs replacement or can legitimate the eviction of its residents. However, it is a difficult term to avoid for at least three reasons. First, some networks of neighbourhood organizations choose to identify themselves with a positive use of the term, partly to neutralize these negative connotations; one of the most successful is the National Slum Dwellers Federation in India. Second, the only global estimates for housing deficiencies, collected by the United Nations, are for what they term “slums”. And third, in some nations, there are advantages for residents of informal settlements if their settlement is recognized officially as a “slum”; indeed, the residents may lobby to get their settlement classified as a “notified slum”. Where the term is used in this journal, it refers to settlements characterized by at least some of the following features: a lack of formal recognition on the part of local government of the settlement and its residents; the absence of secure tenure for residents; inadequacies in provision for infrastructure and services; overcrowded and sub-standard dwellings; and location on land less than suitable for occupation. For a discussion of more precise ways to classify the range of housing sub-markets through which those with limited incomes buy, rent or build accommodation, see Environment and Urbanization Vol 1, No 2, October, available at ![]() .
.
2.
3.
Gupta, K, F Arnold and H Lhungdim (2009), Health and Living Conditions in Eight Indian Cities: National Family Health Survey (NFHS–3) 2005–2006, International Institute for Population Sciences, Mumbai, 113 pages.
4.
Osrin, D, S Das, U Bapat, G Alcock, W Joshi and N S More (2011), “A rapid assessment scorecard to identify informal settlements at higher maternal and child health risk in Mumbai”, Journal of Urban Health Vol 88, No 5, pages 919–932.
5.
6.
Government of Maharashtra (1971), Maharashtra Slum Areas (Improvement, Clearance and Redevelopment) Act of 1971, Addendum to Section 3–B, accessible at http://www.legalpundits.com/Content_folder/MahSlum260209.pdf; also see ![]() , Mumbai Development Control Rules, DCR–33 (10), Mumbai.
, Mumbai Development Control Rules, DCR–33 (10), Mumbai.
7.
Patel, S, C D’Cruz and S Burra (2002), “Beyond evictions in a global city: people-managed resettlement in Mumbai”, Environment and Urbanization Vol 14, No 1, April, pages 159–172.
8.
Gangan, S (2010), “Maharashtra C M Ashok Chavan to Centre: have a slum policy like we do”, DNA, 22 August 2010, accessible at http://www.dnaindia.com/mumbai/report_maharashtra-cm-ashok-chavan-to-centre-have-a-slum-policy-like-we-do_1426904; also Alternative Law Forum (2005), “Mumbai to Shanghai without slums–3: slum policies”, accessible at ![]() .
.
9.
Appadurai, Arjun (2001), “Deep democracy: urban governmentality and the horizon of politics”, Environment and Urbanization Vol 13, No 2, October, pages 23–43.
10.
Findings from the other studies are also included in this paper. Readers with questions about the methods underlying these studies should contact the authors.
11.
While we are assuming that the NFHS slums are a representative sample, there may be sampling biases deriving from the survey’s classification of communities as “slums” based on the 2001 census. According to a recent report, the 2001 census undercounted non-notified slums in many cities, such that “…the slum population of the country was grossly underestimated” (see reference 2, page 15). Given the possible omission of non-notified slums, the sample of NFHS slums used in this analysis may be skewed towards the population of notified slums in Mumbai, although the extent to which this is the case is unclear.
12.
Unlike notified slum residents, who are ensured security of tenure, no one in Kaula Bandar technically “owns” his or her own home. Rather, “ownership” in Kaula Bandar refers to someone having built his or her own living structure and therefore having the informal right to rent out the space.
13.
Subbaraman, R, S Shitole, K Sawant, T Shitole, D E Bloom and A Patil-Deshmukh (2011), “Failures in the quality, quantity and reliability of water provided through an informal distribution system in Mumbai, India”, [Abstract OS40.6], Paper presented at the 10th International Conference on Urban Health, 2–4 November 2011, Belo Horizonte, Brazil.
14.
Howard, G and J Bartram (2003), “Domestic water quantity, service level and health”, World Health Organization, Geneva, 33 pages.
15.
Hunter, P R, A M MacDonald and R C Carter (2010), “Water supply and health”, PLoS Medicine Vol 7, No 11, e1000361, pages 1–9.
16.
Kyobutungi, C, A K Ziraba, A Ezeh and Y Ye (2008), “The burden of disease profile of residents of Nairobi’s slums: results from a demographic surveillance system”, Population Health Metrics Vol 6, page 1; also Marsh, D, K Husein, M Lobo, M Shah and S Luby (1995), “Verbal autopsy in Karachi slums: comparing single and multiple cause of child deaths”, Health Policy and Planning Vol 10, No 4, pages 395–403.
17.
Guerrant, R L, R B Oria, S R Moore, M O Oria and A A Lima (2008), “Malnutrition as an enteric infectious disease with long-term effects on child development”, Nutrition Reviews Vol 66, No 9, pages 487–505; also Lorntz, B, A M Soares, S R Moore, R Pinkerton, B Gansneder, V E Bovbjerg, H Guyatt, A M Lima and R L Guerrant (2006), “Early childhood diarrhoea predicts impaired school performance”, Pediatric Infectious Disease Journal Vol 25, No 6, pages 513–520.
18.
See reference 15.
19.
Partners for Urban Knowledge, Action and Research (2011), “Mental health study phase 1: slum adversity qualitative interviews”, PUKAR, Mumbai, unpublished. All of the quotations from Kaula Bandar residents that follow throughout the remainder of this paper also come from this study.
20.
See reference 16, Kyobutungi et al. (2008); also see reference 16, Marsh et al. (1995); see reference 17, Guerrant et al. (2008); and see reference 17, ![]() .
.
21.
Personal communication from Corporator Mangesh Bansod to PUKAR researchers.
22.
See reference 21.
23.
Rego, R F, M L Barreto, R Santos, N F de Oliveira and S Oliveira (2007), “Rubbish index and diarrhoea in Salvador, Brazil”, Transactions of the Royal Society of Tropical Medicine and Hygiene Vol 101, No 7, pages 722–729; also Hayes, J M, E Garcia-Rivera, R Flores-Reyna, G Suarez-Rangel, T Rodriguez-Mata, R Coto-Portillo et al. (2003), “Risk factors for infection during a severe dengue outbreak in El Salvador in 2000”, American Journal of Tropical Medicine and Hygiene Vol 69, No 6, pages 629–633; and Reis, R B, G S Ribeiro, R D Felzemburgh, F S Santana, S Mohr, A X Melendez, A Queiroz, A C Santos, R R Ravines, W S Tassinari, M S Carvalho, M G Reis and A I Ko (2008), “Impact of environment and social gradient on Leptospira infection in urban slums”, PLoS Neglected Tropical Diseases Vol 2, No 4, e228, pages 1–10.
24.
Mathur, M, R Chandra, S Singh and B Chattopadhyaya (2007), “Norms and standards of municipal basic services in India”, National Institute of Urban Affairs, New Delhi, 38 pages.
25.
De, Anuradha and Jean Dreze (1999), Public Report on Basic Education in India, Oxford University Press, New York, 168 pages.
26.
Juneja, N (2001), Primary Education for All in the City of Mumbai, India: The Challenge set by Local Actors, UNESCO International Institute for Educational Planning, Paris, page 29.
27.
Agarwal, S and A Srivastava (2009), “Social determinants of children’s health in urban areas in India”, Journal of Health Care for the Poor and Underserved Vol 20, Supplement 4, pages 68–89; also Singh, A, P K Pathak, R K Chauhan and W Pan (2011), “Infant and child mortality in India in the last two decades: a geospatial analysis”, PLoS One Vol 6, No 11, e26856, pages 1–19.
28.
De Soto, Hernando (2000), The Mystery of Capital: Why Capitalism Triumphs in the West and Fails Everywhere Else, Basic Books, New York, 276 pages.
29.
Sawant, K, S Shitole, T Shitole, D E Bloom and A Patil-Deshmukh (2011), “Lean on me – inequities of formal support systems during disasters for the most vulnerable residents of an unregistered slum”, [Abstract OS1.4], Paper presented at the 10th International Conference on Urban Health, 2–4 November 2011, Belo Horizonte.
30.
Hameed, A (2009), “Rs 6.50 crore approved for rehabilitation of Behrampada fire victims”, Indian Muslim, 21 July, accessible at ![]() .
.
31.
Ashar, Sandeep (2009), “Behrampada hutments rise from the ashes”, DNA, 29 July, accessible at ![]() .
.
32.
See reference 28.
33.
Fullilove, M T (2001), “Root shock: the consequences of African–American dispossession”, Journal of Urban Health Vol 78, No 1, pages 72–80.
34.
Farmer, P E, B Nizeye, S Stulac and S Keshavjee (2006), “Structural violence and clinical medicine”, PLoS Medicine Vol 3, No 10, e449, pages 1686–1691 (e-article so no page number for quote).
35.
See reference 34.
36.
See reference 34.
37.
See reference 4.