
Abstract
The COVID-19 pandemic has made policy transfer imperative for countries in dealing with this unprecedented global crisis. Policy transfer is theoretically considered successful when an external policy is legally adopted into the recipient country’s legislation and achieves its intended goals. However, the definitions of policy transfer success and failure remain ambiguous, particularly when assessing the discrepancy between policy (non-)compliance and policy outcomes. Drawing on a unique case study of Vietnam’s policy on separating newborns from mothers with COVID-19 and the street-level bureaucrats’ non-compliance observed during the first delivery of an affected mother in the country, this paper demonstrates that non-compliance with transferred policies - driven by street-level bureaucrats’ pursuit of optimal policy outcomes and professional confidence - can result in both policy transfer failure and desirable policy outcomes. Accordingly, the paper proposes an analytical framework for evaluating policy transfer success and failure and policy outcomes that incorporates non-compliance as a key variable. It further examines the roles of street-level bureaucrats in policy transfer, as well as the contexts and motivations behind their non-compliance. It also offers practical implications for policymakers, emphasizing the need to anticipate potential non-compliance and ensure flexibility in policymaking and implementation in crisis conditions.
Keywords
Introduction
COVID-19 exposed countries worldwide to the same epidemiological problem, acting as a catalyst for policy learning and change. Policymakers embarked on a search for effective policy solutions across various areas to address the challenges posed by COVID-19, including contact tracing (Sideri and Prainsack, 2023), school closures (Giuliani, 2023), and social distancing (Mistur et al., 2023). A rigorous compilation of lessons in pandemic response from various countries has yielded a wealth of policy information for policymakers worldwide (Powell and King–Hill, 2020). Policy transfer, a process whereby policy knowledge and practices from one political system is utilized to inform and guide the formulation and development of similar policies in another political system ((Dolowitz and Marsh, 2000), became a quick and efficient tool for policymaking in turbulence. In times of crisis, policy transfer is used more often because policymakers need to resort to “quick fix” solutions that policy transfer can offer (Evans, 2009).
Theoretically, policy transfer is assessed as being successful when the policymakers achieve their aims when transferring the policies into their system (Dolowitz and Marsh, 2000). However, in reality, as policy transfer is not an “all-or-nothing” process (Dolowitz and Marsh, 2000: 13), the examination of policy transfer success and failure needs to be based on different levels or degrees of the transfer outcomes. Viewing from the policy transfer stages (Evans, 2009), policy transfer should be examined across multiple levels, encompassing its impact on the nature of policy debates during the pre-decision stage, its influence on policy design, selection, and options at the decision stage, and its effect on policy outcomes and efficiency in the post-decision stage. This highlights the importance of defining policy transfer success and failure in relation to policy implementation and its outcomes.
The existing literature has seen some efforts in establishing policy transfer success and failure. These focus mainly on policy adoption or non-adoption (Minkman et al., 2018), the transfer process itself (Dolowitz and Marsh, 2000), or the roles of learning to policy transfer success and failure (Giest, 2017; Stone, 2017). A few studies indicate the link between street-level bureaucrats’ policy (non-)compliance and policy transfer success and failure (Šimić Banović, 2015). There is a lack of rigorous research and an analytical framework to evaluate policy transfer success and failure in relation to street-level bureaucrats’ policy implementation and outcomes. Scholars have pointed out that the connection between policy transfer and its perceived success or failure is inherently complex, as determining what constitutes success or failure often involves multifaceted and nuanced considerations (James and Lodge, 2003; Matei et al., 2018). Therefore, evaluating policy transfer success and failure in relation to policy outcomes requires empirical studies that closely examine the (non-)compliance, particularly by street-level bureaucrats, with the transferred policy and its effectiveness.
Since 2014, Vietnam has adopted and integrated the World Health Organization’s Early Essential Newborn Care (EENC) intervention, regulating that babies must be kept with their mothers immediately after birth with prolonged skin-to-skin contact and early and exclusive breastfeeding (WHO, 2014). However, when the COVID-19 outbreak reached Vietnam in early 2020, the Ministry of Health (MoH), aligning with international practices on separating newborns from COVID-19-positive mothers (Murdoch Children’s Research Institute, 2023; WHO, 2021), mandated immediate postnatal separation to prevent transmission. Although the policy was formally integrated into Vietnam’s regulatory framework, it was not followed during the country’s first delivery involving a COVID-19-positive mother, reflecting a notable case of non-compliance.
By analysing the non-compliance of Vietnam’s policy regarding the separation of babies from their COVID-19 positive mothers by doctors and nurses at a district hospital in Danang City, this article will shed light on the significance of street-level bureaucrats’ policy non-compliance in policy transfer, examining its contradictory influences on the success and failure of policy transfer and policy outcomes. The findings from this empirical research suggest directions for rethinking policy transfer success and failure, offering an emergent analytical framework for examining policy outcomes in relation to policy (non-)compliance. The study also proposes approaches for assessing street-level bureaucrats’ roles, considering contextual influences, motivations, and professional confidence in shaping their non-compliance.
This article is organised into five sections. The first section reviews key concepts related to policy transfer success and failure, policy non-compliance, and policy outcomes. It defines policy success and failure, examines how success and failure are evaluated in policy transfer, and considers the role and consequences of non-compliance in shaping outcomes. This review reveals a gap in the literature concerning the relationship between street-level bureaucrats’ non-compliance and policy transfer outcomes. The second section outlines the research methodology, detailing case selection and the use of qualitative methods. The third section presents the empirical case. The fourth section discusses theoretical and practical implications, particularly regarding street-level actors. The final section concludes with key findings, limitations, and directions for future research.
Policy transfer success and failure, policy non-compliance and policy outcomes
The ambiguity of policy transfer success and failure
To evaluate policy transfer success and failure, it is crucial to consistently define policy transfer and distinguish it from similar concepts. Policy transfer is defined by Dolowitz and Marsh (2000: 5) as “the process by which knowledge about policies, administrative arrangements, institutions and ideas in one political system (past or present) is used in the development of policies, administrative arrangements, institutions and ideas in another political system”. It is a “generic concept” that “encompasses a range of related concepts” but is distinct from similar terms such as policy diffusion, policy learning, and lesson drawing (Stone, 1999: 52; Evans and Davies, 1999: 363). For example, policy learning (May, 1992) and lesson drawing (Rose, 1991) describe the process of acquiring knowledge about policies implemented elsewhere. While policy learning and lesson drawing can be components of policy transfer, they do not necessarily lead to policy adoption (Casady and Parra, 2021), as policymakers may also learn from the mistakes of others and decide what not to adopt (Rose, 1991). This article applies Dolowitz and Marsh’s conceptualization of policy transfer, specifically referring to the adoption of policies in the recipient country.
As a process, policy transfer has a beginning and an end with different stages of development (Evans and Davies, 1999; Rose, 2005). Theoretically, the process of voluntary policy transfer consists of multiple stages, some of which can occur simultaneously or recur. These stages include identifying problems, exploring policy solutions, assessing the feasibility of transfer, implementing transfer activities, and adopting the transferred policy, as illustrated in Figure 1. Evans and Davies (1999: 379) insisted that a policy “can ultimately only be said to have been transferred if it is carried out” and “the analysis of policy transfer is incomplete without reference to implementation”. Since implementation determines whether a policy has actually been transferred, this article adopts the perspective that policy transfer encompasses both policy adoption and implementation. Policy transfer stages. Source: Duong (2022a).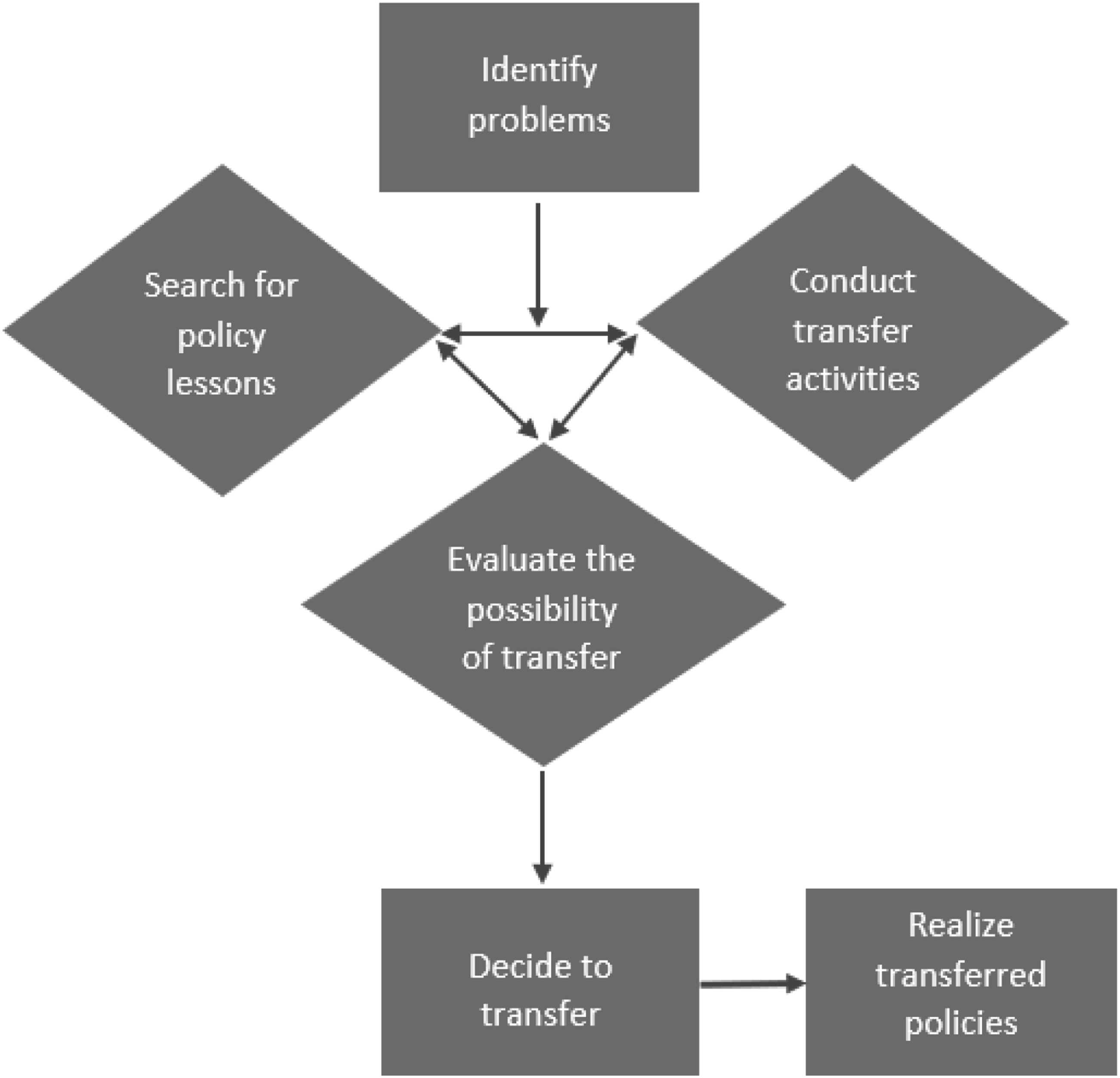
While research on policy transfer has developed significantly, the study of policy transfer success and failure is still under-explored. Some studies evaluate policy transfer success and failure based on whether the external policy is adopted or not and to what degree. For example, according to Minkman et al. (2018: 234), successful adoption is when the policy is adopted upon the completion of the transfer process and non-adoption occurs when a policy was “considered but never initiated” or was “initiated but aborted along the way”. Meanwhile, formal adoption refers to the condition in which the policy is formally adopted but is not implemented (Minkman et al., 2018). This shows an unclear line between the success and failure of policy transfer. Other scholars evaluate the transfer process itself. Dolowitz and Marsh (2000) categorize policy transfer failure into uninformed transfer, incomplete transfer, and inappropriate transfer. However, these classifications do not account for the implementation of the transferred policy. A limited number of studies examine policy transfer success and failure in relation to policy outcomes, considering these outcomes across three dimensions: process, programs, and politics (Matei et al., 2018).
Nevertheless, in assessing policy outcomes and efficiency, there has been no agreement on the definition of policy success and failure because policy success and failure can be viewed from different perspectives (McConnell, 2010). One common criterion that has been widely used to assess policy success and failure is the extent to which the goals of the policymakers are achieved and the absence of opposition and non-compliance with the policy. For example, McConnell (2010: 351) insists that “a policy is successful if it achieves the goals that proponents set out to achieve and attracts no criticism of any significance and/or support is virtually universal”. The evaluation of policy success and failure becomes more complicated when being considered in relation to policy transfer. For instance, in urgent situations where governments seek an immediate solution, policy transfer is often regarded as successful if the external policy is adopted “virtually unamended” because policymakers are perceived as decisive; however, this approach may lead to policy challenges in the future (Marsh and Sharman, 2009: 283).
Another issue in defining policy success and failure is about answering the question “success and failure for whom?”. It is because the evaluation of policy outcomes “may reflect power relations and be different for different individuals/groups” (Marsh and Sharman, 2009: 284). Consequently, policy evaluation “has multiple dimensions, often succeeding in some respects but not in others, according to facts and their interpretation” (McConnell, 2010: 345). In addition, policy success and failure are multidimensional. McConnell (2010) categorises policy success and failure into three dimensions, including process, program, and politics. Accordingly, the judgment of policy success and failure can be plural as a policy can be seen as being successful programmatically but not politically and vice versa (McConnell, 2010), or “a policy can “succeed” on one dimension, or for one set of people, while “failing” on another dimension, or for another set of people” (Marsh and Evans, 2012: 4). This is why policy success and failure is seen as a “slippery concept” (Baldwin et al., 2019: 171), which makes the evaluation of policy transfer success and failure with regards to policy outcomes far from being a simple task.
Policy non-compliance and policy transfer success and failure
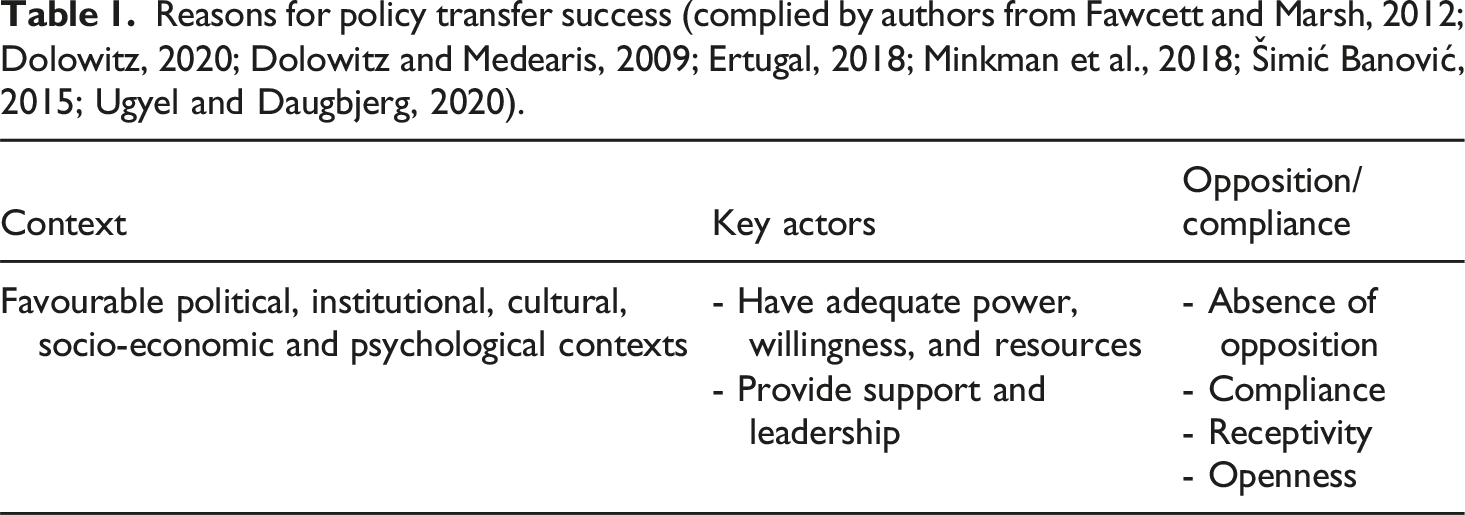
Reasons for policy transfer success (complied by authors from Fawcett and Marsh, 2012; Dolowitz, 2020; Dolowitz and Medearis, 2009; Ertugal, 2018; Minkman et al., 2018; Šimić Banović, 2015; Ugyel and Daugbjerg, 2020).
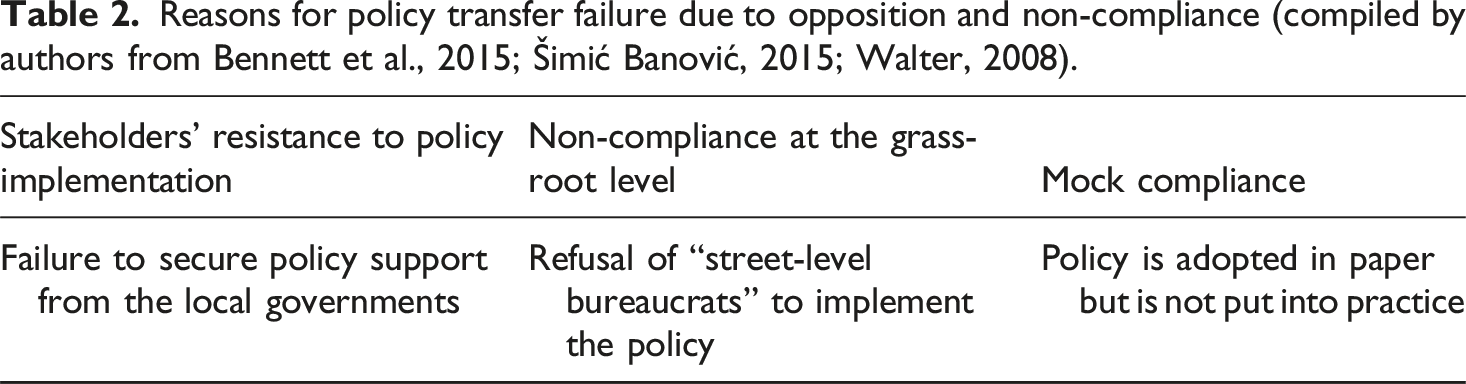
Reasons for policy transfer failure due to opposition and non-compliance (compiled by authors from Bennett et al., 2015; Šimić Banović, 2015; Walter, 2008).
What needs to be addressed?
While the justification of policy transfer success or failure may depend on the subjective perspective adopted by evaluators (Dolowitz and Marsh, 2000), there is a strong link between policy (non-)compliance and policy transfer success or failure. Furthermore, since policy success can be defined as the achievement of policy goals and the absence of resistance to the policy (McConnell, 2010), policy (non-)compliance and its outcomes play a crucial role in determining policy success or failure. This suggests a causal relationship between policy transfer, policy (non-)compliance, and policy success or failure.
Despite this connection, the literature lacks sufficient theorization and empirical research on the relationship among the three variables. In addition, although street-level bureaucrats’ resistance to, or non-compliance with, policy implementation has been documented in both routine and crisis contexts (Cox et al., 2021; Mavrot and Hadorn, 2023), there remains a gap in understanding why and how such non-compliance influences policy transfer and policy outcomes. Several key questions remain unanswered: (1) How does street-level bureaucrats’ policy non-compliance affect policy transfer success and failure?; (2) How are the success and failure of policy transfer and policy outcomes evaluated in relation to policy (non-)compliance?; and (3) Can policy transfer failure still lead to policy success (or failure) in the context of street-level bureaucrats’ policy non-compliance, and why? Answers to these questions are important because desirable policy outcomes, especially in urgent or high-stakes contexts like pandemics, depend not only on the formal adoption of transferred policies but also on how frontline actors interpret and implement them. Addressing these issues may prevent misdiagnoses of non-compliance and support more accurate, context-sensitive evaluations of policy transfer and implementation.
Methodology
This research utilizes the qualitative case study method, employing the non-compliance of the policy to separate babies born to COVID-19 mothers in Vietnam as a case to study the success and failure of policy transfer and its outcomes. This method helps to explore “why” and “how” such an event happened and the relevance of contextual conditions (Yin, 2018). While this approach limits generalizability, it enables close attention to processual detail and context-specific dynamics that are often obscured in large-N studies.
To construct a plausible and evidence-informed account of how non-compliance occurred and was interpreted, this study employed a combination of document analysis, self-reflection, and semi-structured in-depth interviews. The documents analysed include official decisions, regulations, reports issued by the MoH and relevant hospitals, media articles, and publications from the World Health Organization (WHO). Notably, the research was informed by the documentary Mầm sạch (Clean Sprout), aired on Da Nang Television and awarded the Gold Medal at the 2020 Vietnam National Television Festival. Statements from the documentary were quoted with attribution and cited under the documentary’s credited authors.
This research made extensive use of self-reflection as a methodological tool to enhance the credibility and transparency of the research process. Self-reflection enables researchers to move beyond technical execution and engage as reflective practitioners capable of constructing meaning from the case under investigation (Mortari, 2015: 1). Dr. Hoang Thi Tran, Vice Director of Danang Hospital for Women and Children, who led the delivery team at Hoa Vang Medical Centre, contributed a detailed reflection on her professional role, decision-making processes, and experiences during the care of newborns delivered by COVID-19-positive mothers. In addition to her responsibilities at Hoa Vang, Dr. Tran was tasked with overseeing similar cases across Danang City during the pandemic. Her dual role as practitioner and researcher offered a unique perspective. The reflection was structured around guiding questions and is cited in this paper with clear attribution.
Purposive sampling was employed to select interview participants directly involved in the delivery of the first COVID-19-positive mother at Hoa Vang Medical Centre. Conducted between July and September 2023, the interviews involved four key respondents: the Director of Hoa Vang Medical Centre (also Director of the Hoa Vang Field Hospital during the pandemic), and three members of the delivery team, including doctors and nurses. All interviews were conducted in Vietnamese, adhering to the principle of anonymity. Responses were translated into English and transcribed verbatim to ensure accuracy and fidelity to participants’ intended meanings.
The data were analysed manually using a thematic analysis approach informed by established literature on policy transfer and street-level bureaucracy. The analysis aimed to identify key dimensions relevant to understanding policy non-compliance and transfer outcomes, including contextual factors (e.g., crisis pressures), street-level bureaucrats’ motives (e.g., ethical reasoning), professional justifications (e.g., medical expertise), specific instances of non-compliance (e.g., decision-making processes), and reported policy outcomes. Interview transcripts, self-reflections, and documents were reviewed iteratively to identify patterns and contrasts. Codes and categories were developed inductively and refined through ongoing analysis, with themes organised around the central research questions, allowing theories to emerge from the data collected.
COVID-19 hot spot and Vietnam’s policy
The Early Essential Newborn Care (EENC) guideline, issued by the World Health Organization in 2014, recommended immediate and prolonged skin-to-skin contact between mothers and newborns, as well as early and exclusive breastfeeding, to ensure optimal maternal and neonatal outcomes (WHO, 2014). Vietnam formally adopted this guideline through Decision No. 4673/QD-BYT, issued by the Ministry of Health (MoH) on 10 November 2014. This policy remained unchanged until the onset of the COVID-19 pandemic. By March 2020, Vietnam had recorded nearly 170 confirmed COVID-19 cases, with no reported deaths, ranking 84th among 200 countries affected (Ministry of Health, 2020). The country’s initial success was attributed to strict national quarantine and lockdown measures. In this context, MoH issued Decision No. 1271/QD-BYT on 21 March 2020, mandating the immediate postnatal separation of babies born to COVID-19-positive mothers, aligning with global efforts to curb viral transmission through patient isolation.
The Hoa Vang Medical Centre, a 170-bed district-level hospital in Danang City, was among a few hospitals assigned the responsibility of treating COVID-19 patients during the pandemic outbreak by the Danang Municipal government. The first delivery of a woman infected with COVID-19 in Vietnam occurred at this medical centre. At the time of the woman’s labour, Decision No. 1271/QD-BYT was in effect, and its regulations were required to be strictly followed nationwide as mandated by law.
The story of the delivery of the first COVID-19 infected mother in Vietnam
The 35-year-old woman tested positive to COVID-19 at 34 weeks and 4 days of her pregnancy. She had a caesarean section at 36 weeks with mild COVID-19 symptoms at Hoa Vang Medical Centre on 15 August 2020. Dr. Tran recalled the situation at that time: “When COVID-19 hit the world, Danang became a hot spot of the pandemic…. Our health sector had to face many difficulties and challenges… There was one case at Hoa Vang Medical Centre that I will never forget in my career life - a pregnant woman contracted COVID-19 very close to her due date.” (Lan et al., 2020)
The doctors and nurses at Hoa Vang Medical Centre faced a difficult struggle to make the best medical decision. Being aware of the benefits of EENC and the risks of COVID-19 transmission, “we are put in a dilemma situation… my hardest question is that should we separate the baby from her mother to avoid the risk or to keep the baby with her mother to prevent possible diseases and death?” said Dr. Tran. “I had to struggle with many different thoughts. I had to decide the best treatment option for the mother and the baby. I was obsessed with the innocent eyes of the babies, and the desire to protect them…”, she added (Lan et al., 2020).
The COVID-19 infected woman was also confused about the medical decision and did not know which was best for her and her baby: “At first, I was told that after birth, my baby would be separated from me and transferred to another hospital. However, after that, the doctor told me that it was not necessary to separate the baby from me. Actually, at that time, I was really worried. I was anxious that my daughter would get COVID-19 if she was kept with me” (Lan et al., 2020).
After a thorough discussion, the medical team decided not to separate the baby from her mother. “We decided that the baby must be kept with her mother for skin-to-skin contact and early breast-feeding”, said Dr. Tran (Lan et al., 2020). Consequently, the delivery was successful when the baby was free from COVID-19 and received both skin-to-skin contact and breastfeeding. “I am very happy that my daughter did not contract COVID-19 from me”, said the mother (Lan et al., 2020). The decision not to separate the baby from her mother contradicted the MoH’s policy, representing a case of policy non-compliance.
Non-compliance with baby-mother separation policy and policy transfer success and failure
A case of policy transfer
Measures to prevent the risks of transmission of COVID-19 from mothers to babies were taken by many countries and were advocated by medical experts. In February 2020, China strictly applied the separation policy to COVID-19 mothers giving birth in hospitals, followed by South Korea in early March (Chen et al., 2020; Yeo et al., 2020). In April 2020, the American Academy of Pediatrics (AAP) recommended temporarily separating newborns from mothers with COVID-19 (Downey, 2020b).
Despite WHO’s recommended guidelines of EENC for babies of COVID-19 infected mothers (WHO, 2020), and AAP’s withdrawal from their previous recommendation in July 2020 (Downey, 2020a), most babies born to mothers with COVID-19 worldwide were separated from their mothers after birth. An international study conducted by Murdoch Children’s Research Institute, and the European Society of Paediatric and Neonatal Intensive Care, found that in 10 countries, including Brazil, France, Italy, and the US, 54% of newborns were separated from their mothers (Murdoch Children’s Research Institute, 2023). Another study of 20 clinical guidelines from 17 countries during the pandemic found that one-third recommended the separation of mothers and newborns if the mothers had or may have had COVID-19 (WHO, 2021). A global survey of thousands of neonatal healthcare providers also revealed that two-thirds of healthcare workers in 62 countries reported that they did not allow mothers with confirmed or suspected COVID-19 to practice skin-to-skin contact (Rao et al., 2021).
Vietnam is no exception: the issuance of Decision No. 1271/QD-BYT by MoH followed this practice. In the first policy draft prepared by MoH Maternal and Child Health Department, they did not recommend separating newborns from COVID-19-positive mothers, except in severe cases. However, when the draft was sent to relevant hospitals for comments, some major hospitals insisted on separation. For example, the National Children’s Hospital strongly advocated for separation. Three out of the four references they cited to support their proposal were based on Chinese research. As a result, MoH adopted the newborn separation policy. Being among the reviewers of the first policy draft, Dr. Tran insisted: “This policy may have been adopted with reference to China’s policy”.
Timeline for the adoption and removal of newborn separation policy.
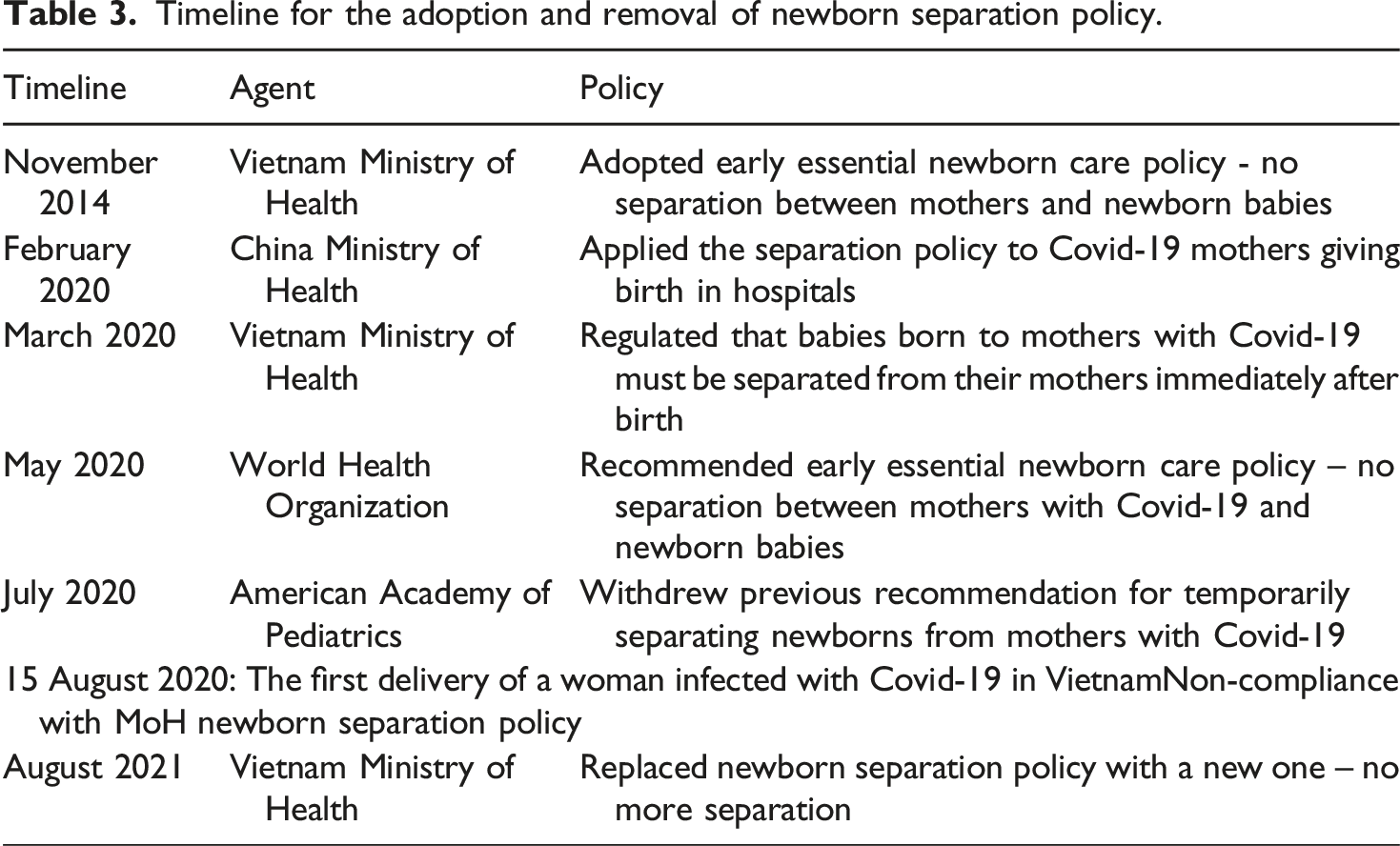
The external policy was transferred to Vietnam unamended and adopted successfully into Vietnam’s legal system. It served the policymakers’ goals of containing and minimizing COVID-19 transmission. Importantly, it is a manifestation of the government’s active and timely response in emergencies. Vietnamese policymakers engaged in policy change prior to experiencing the cases of delivery of mothers with COVID-19, which helped them to be prepared for dealing with possible risks. This type of “anticipatory” or “preventive” policymaking is among public health best practices (Crow et al., 2022), but can lead to trade-offs if the risks of compliance outweigh the risks of non-compliance.
Policy non-compliance: Rationales and outcomes
Clinical and medical considerations, as well as concerns about the safety and benefits for both the baby and the mother, were the driving factors behind the non-compliance with the mother-baby separation policy. The delivery team at Hoa Vang Medical Centre aimed to achieve two goals: preventing the transmission of COVID-19 from the mother to the baby and minimizing the health risks for the newborn. “Our most important goal is that the baby does not get COVID-19 from her mother and at the same time can benefit the most from skin-to-skin contact and early breastfeeding”, said Dr. Tran (Lan et al., 2020). There was careful examination and study of the pros and cons of separating the baby from her mother. A delivery team member said: We studied MoH’s guidelines and other international studies and found that babies with COVID-19 do not develop complicated symptoms. Therefore, after discussing with Dr. Tran, we compared the benefits and the risks of separating the baby from her mother. Being away from her mother immediately after birth, the baby will be more vulnerable to the risks of hypothermia, hypoglycaemia and infection. Meanwhile, the possibility of getting COVID-19 from her mother without separation is not confirmed. Therefore, if we keep the baby with her mother and practice strict transmission prevention measures, the outcomes will be better. This is also beneficial to the mother’s mental well-being, aiding in a speedy recovery from the illness (Author interview, 20 July 2023).
This view was shared by all the delivery team members who specialize in Obstetrics and Gynecology. “The separation of the baby from their mother, even during COVID-19, has numerous consequences. It further burdens medical staff, exacerbating the issue of personnel shortage during the pandemic. The separation also means that the baby does not receive early breast-feeding and is exposed to the risks of formula milk” (Author interview, 15 August 2023). The team conducted many consultations before making the medical decision. “We had so many discussions and consultations to decide the best solution for both the mother and the baby”, said Dr. Tran. The decision was made with the support and confidence of the whole delivery team. “I believe in Dr. Tran’s and my colleagues’ decision, and I was not anxious about this”, said a team member (Author interview, 5 August 2023).
However, as COVID-19 was hitting the country so hard, this clinical justification was not without doubt at that time. The uncertainty was most apparent on the side of the mother. “The mother also wanted to have some ways to separate the baby from her, such as putting the baby into the incubator. However, with scientific evidence, we advised the mother about the benefits of keeping the baby with her, at the same time with strict measures to prevent the transmission”, said a team member (Lan et al., 2020). In this case of an emergency, the medical team’s trust and confidence came from medical expertise, not from fear or coercion. “Being a doctor trained in Obstetrics and Gynecology, I understand the benefits of skin-to-skin contact. However, with a COVID-19 mother, we need careful consideration and consultation”, as explained by a doctor in the team (Author interview, 28 July 2023). The decision was made based on quick research of scientific evidence, which served as a catalyst for making sound judgments in turbulence. A team member revealed that “in an emergency, we searched the internet and read reliable journals. We need to decide quickly based on consultation and discussion. There has been no precedent in Vietnam” (Author interview, 20 July 2023). Dr. Tran elaborated: “We referred to WHO guidelines and other medical documents to confirm the benefits of skin-to-skin contact and the risk of COVID-19 transmission in this practice. Based on the practical evidence, we found that the risks associated with COVID-19 in babies are much lower than the risks of not applying skin-to-skin contact and early breastfeeding for the newborn. Therefore, we decided to follow the WHO guidelines”.
The decision not to separate the baby from her mother means non-compliance with the government’s policy, particularly when earlier MoH requested Danang to strictly follow their regulations (Truong, 2020). This non-compliance may entail accountability consequences; however, these were not the concern of the medical team at that time. The concern about more favourable outcomes for the baby and the mother outweighed the fear of responsibility and the consequences of non-compliance with the national regulations. “According to the regulations, we have to separate the baby from her mother. In the case that we do not follow the regulations and the baby is infected with COVID-19, then we have to take responsibility for our decision. Nevertheless, if we separate the baby from her mother, the baby can face the risks of low temperature and low blood sugar due to no breastfeeding after birth, and the risk of infections. These risks can lead to more diseases and deaths than COVID-19”, said Dr. Tran.
Moreover, the concern about the mother’s physical and mental health urged the doctors to reject the regulation. “I think we all overcome the fear of not complying with the regulations to minimize the disadvantages for the mother and the baby. This is because giving birth in the isolated hospital and the short gap between life and death in the pandemic is a burden for both of them” (Author interview, 1 September 2023). The medical team acted according to the medical ethics in which the health of the patients was given the priority. “From the bottom of our heart, we decide and act with the responsibility of doctors. We only think for the patient, not anything else” (Author interview, 20 July 2023).
After difficult discussions and consultations, the medical team decided to keep the baby close to her mother, with strict measures applied to prevent COVID-19 transmission. The outcomes of the decision were desirable. The mother and the baby were healthy and were discharged a week later. A team member recalled: “The mother and the baby were well and came home, especially the baby, who did not get COVID-19. This is a great success for our team and for the health sector. For me, this is an unforgettable experience” (Author interview, 28 July 2023). The successful outcomes strengthened the doctors’ confidence in medical and clinical evidence. Particularly, this created a precedent for the following delivery cases. “This builds up my confidence in medical evidence and it is a good start for applying skin-to-skin contact for other deliveries of COVID-19 infected mothers” (Author interview, 1 September 2023). This also served as a good reason for calling for the revision of the transferred baby-mother separation policy. It is confirmed that “EENC… remains feasible during the pandemic and should be prioritized by policymakers and programme managers” (Tran et al., 2021: 1993).
After this successful case, Dr. Tran stated, “we reported it to the Ministry of Health. In Danang, this practice was implemented for all deliveries involving mothers with confirmed and suspected COVID-19”. One year later, in August 2021, MoH replaced Decision No. 1271/QD-BYT with a new one, resuming EENC in Vietnam’s medical system. Along with WHO guidelines, the success of the non-separation practice in Danang with its positive outcomes served as important evidence for the MoH to consider policy change (Author interview, 15 August 2023). Policy non-compliance produced better outcomes and played a significant role in driving policy change.
Discussion
Evaluating policy transfer success and failure in relation to (non-)compliance
The case study demonstrates that the incorporation of an external policy into the legal system of the recipient country does not guarantee successful policy transfer. The option of the mother – baby separation policy shows that Vietnamese policymakers were quick in responding to the threats posed by COVID-19, but non-compliance created obstacles in the implementation stage. This highlights the significance of considering the various stages of the transfer process when evaluating the success and failure of policy transfer. Given the complicated nature of the transfer processes, policymakers may be successful in the formation of the policy, but may face obstacles and even opposition in the implementation stage that can alter their original ideas (Dolowitz et al., 2020).
This shows that the term “successful adoption”, as defined by Minkman et al. (2018: 234), does not equate to successful policy transfer. Instead, the implementation of an adopted policy is crucial in determining whether a policy transfer process is complete and successful. Conceptually, policy transfer is deemed successful when the enacted policy produces outcomes aligned with the objectives of policymakers. Conversely, failure to implement a transferred policy constitutes policy transfer failure. Thus, the evaluation of policy transfer success or failure must consider both policy adoption and implementation. It is insufficient to assess success solely based on the formal incorporation of external policy into domestic legislation. This research underscores the importance of policy (non-)compliance in shaping transfer outcomes. Compliance, where the transferred policy is effectively enacted, signals success, whereas non-compliance, formal adoption without practical execution, indicates transfer failure.
Evaluating policy success and failure in relation to (non-)compliance
Policy (non-)compliance holds important implications for policy outcomes. The primary aim of the MoH’s decision was to prevent the transmission of COVID-19 from infected mothers to their newborns. However, strict compliance with this policy could have introduced health risks due to the absence of immediate skin-to-skin contact and early breastfeeding. A genuinely successful policy should aim to maximise overall infant well-being, ensuring both protection from infection and the promotion of healthy development. In this case, policy non-compliance arguably contributed to achieving these dual objectives. This complicates the assessment of policy success and failure. If success is defined as both faithful implementation and goal attainment, then non-compliance may represent partial failure in design fidelity but partial success in outcome realisation.
On the other hand, if policy success is defined by maximizing benefits for recipients, then non-compliance can represent policy success when it produces better outcomes than strict adherence. Thus, compliance alone does not guarantee success. Instead, improved outcomes resulting from non-compliance should be recognized as central to evaluating policy effectiveness. This challenges the conventional assumption that compliance equates to success and highlights the need for a more flexible, comprehensive approach. Evaluations should consider not only whether policy outcomes align with policymakers’ goals (McConnell, 2010) but also whether they deliver tangible benefits to those affected (Baldwin, 2000). Ultimately, policy outcomes shaped by (non-)compliance may be assessed differently depending on whether they are deemed desirable or undesirable, complicating the classification of success or failure.
Figure 2 presents an empirically grounded analytical framework for evaluating policy transfer success and failure by integrating policy (non-)compliance as a central variable. Policy transfer success depends on whether the adopted policy is effectively implemented or resisted. Non-implementation due to opposition constitutes policy transfer failure, while adherence and faithful implementation indicate transfer success. The framework also links (non-)compliance to its consequences, recognising that policy outcomes shape assessments of policy success or failure. Non-compliance that results in desirable outcomes may contribute positively to policy success, whereas compliance producing adverse outcomes does not guarantee success. This framework may be further refined and expanded in future research by incorporating additional variables. Analytical framework for evaluating policy transfer success and failure.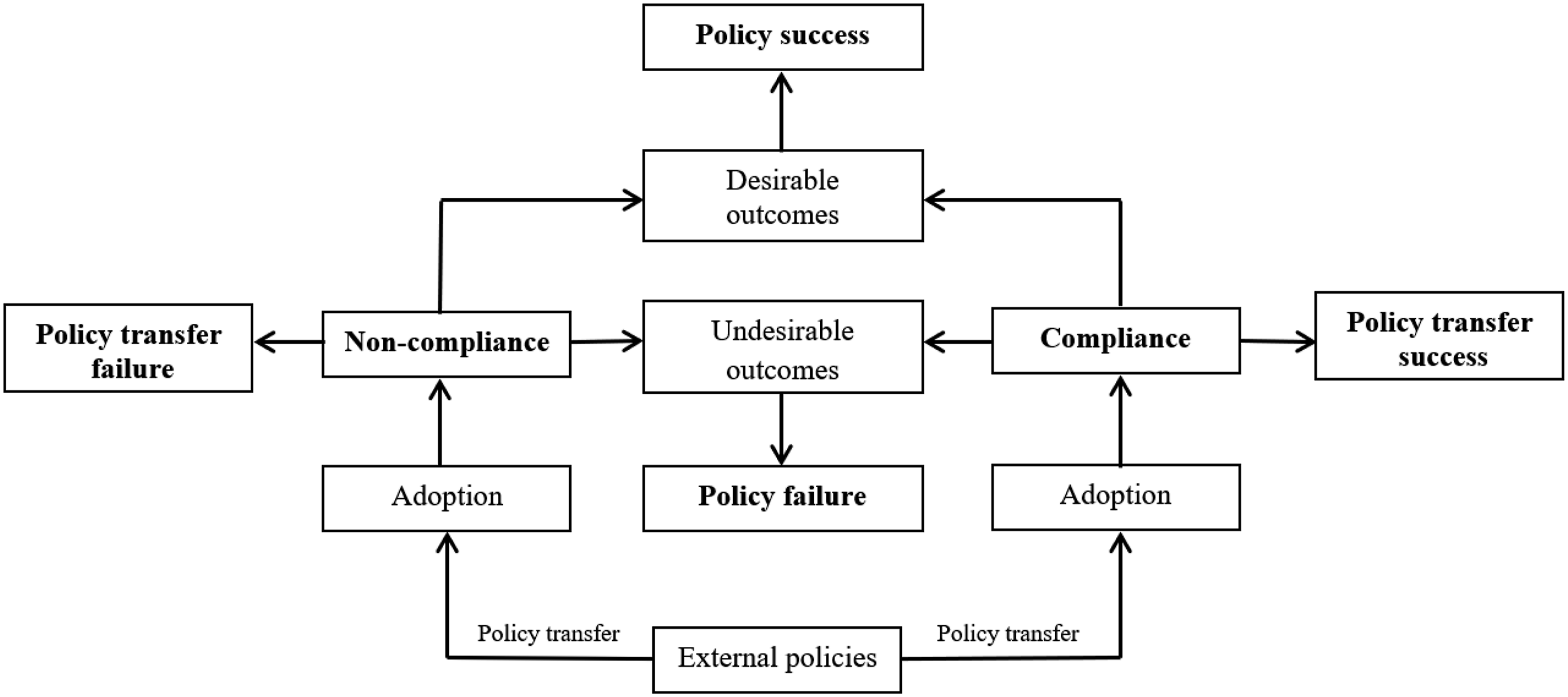
Street-level bureaucrats and policy (transfer) success and failure
The study highlights the crucial role of street-level bureaucrats in policy transfer and their impact on the success and failure of policy transfer, and policy outcomes. Street-level bureaucrats, as defined by Lipsky (1980), are frontline public servants responsible for policy implementation. They are professionals with discretionary power, enabling them to “exercise discretionary judgment in their field” (Lipsky, 1980: 14). While the role of street-level bureaucrats has traditionally been associated with policy delivery, existing research has increasingly recognised their involvement in policymaking, particularly in shaping policy design and solutions (Cohen and Klenk, 2019; Durose, 2007). This study demonstrates that street-level bureaucrats played a pivotal role in adopting the mother-baby separation policy in Vietnam, as their recommendations, informed by external experiences, influenced the Ministry of Health’s initial response. Moreover, their (non-)compliance with transferred policies can affect policy transfer success, failure, and outcomes. In this case, the Danang delivery team’s non-compliance resulted in policy transfer failure but ultimately improved outcomes, prompting a policy overhaul. Figure 3 illustrates their dual influence on policy transfer and delivery. Street-level bureaucrats’ roles and non(compliance).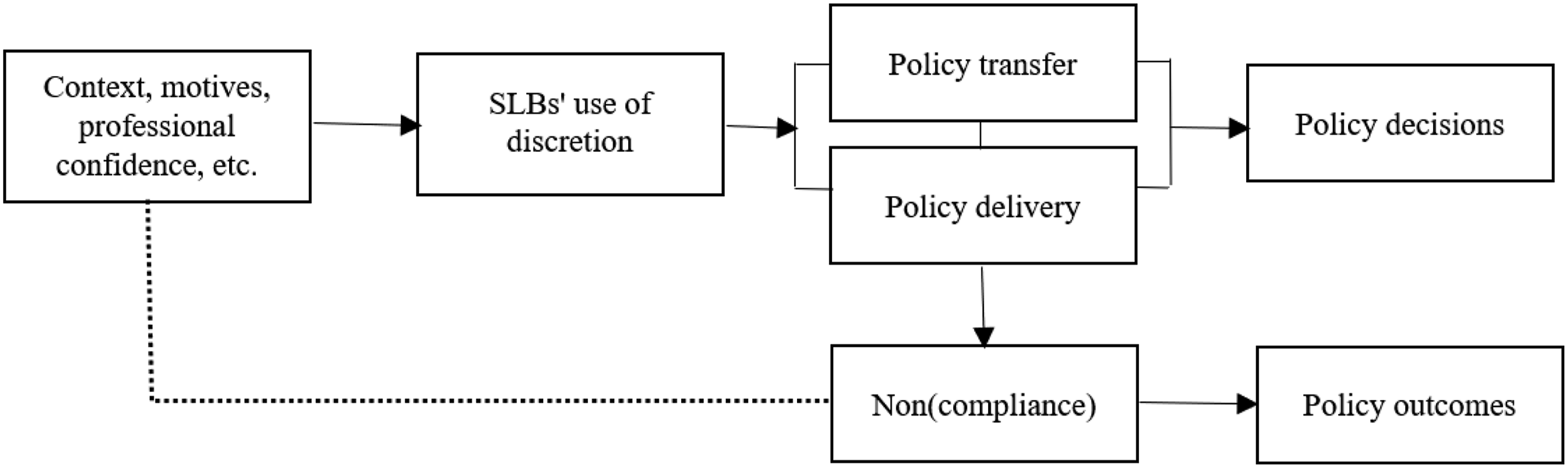
Evans (2020: 2) argues that the street-level bureaucracy literature “is too broad-brush and cannot capture the range of ideas of compliance in public services” because it “tends to see non-compliance as endemic in the use of discretion”. This study addresses this issue by demonstrating that non-compliance, as a result of street-level bureaucrats’ discretionary decisions, should be analysed in relation to context, motives, and approaches. The unprecedented pandemic compelled countries to learn from one another, but the key to successful policy adoption and implementation lay in adapting foreign policies to fit local contexts (Islam et al., 2020; Mistur et al., 2023). In this process, street-level bureaucrats played a crucial role in ensuring that policies were effectively tailored to meet local needs.
A key aspect of non-compliance with the mother-baby policy is that street-level bureaucrats’ decisions to deviate are made promptly yet grounded in professional guidelines, scientific evidence, and expertise, with careful consideration of risks and benefits for both mother and infant. While non-compliance with COVID-19 measures may result from factors such as low governmental trust (Nivette et al., 2021), individual perceptions or lack of resources (Ege et al., 2024), this case demonstrates that it can also reflect street-level bureaucrats’ confidence in their expertise and commitment to optimal outcomes. Given the role of professional knowledge in enabling discretionary flexibility and contextual adaptation (Larsen et al., 2025), such non-compliance may, under certain conditions, enhance policy outcomes and success. This highlights the need for nuanced evaluations of (non-)compliance as it “needs to be sensitive to different types of public services and the subsequent variety of commitments and concerns of street-level bureaucrats in those public services” (Evans, 2020: 2). Figure 3 illustrates this dynamic, emphasizing contextual, motivational, and professional influences on non-compliance.
Policy implications
The findings suggest that policy transfer and outcomes were shaped more by frontline actors’ real-time justifications and non-compliance than formal policy design. While other factors, such as organizational culture, leadership, resource constraints, and oversight, cannot be ruled out, this case highlights the critical role of discretion, adaptability, and flexibility during crisis implementation, with important implications for practitioners. Firstly, the presence of a high level of heterogeneity in the implementation of crisis-response policies, due to the discretion of local governments and the central government’s inability to assess external lessons (Mattei and Vigevano, 2021), poses a challenge for policymakers in monitoring the implementation of transferred policies at the local level. This case study illustrates that the crisis conditions prevented MoH from thoroughly assessing policy lessons from diverse sources and international norms set by WHO, and from anticipating non-compliance at the local level. This limitation is observed in many other health systems, as the pandemic has exposed their shortcomings in dealing with the unprecedented impact of an emerging virus (Gostin, 2022; Parmet, 2022). Furthermore, in the context of a pandemic, governments may perceive risks differently due to various factors (Egger et al., 2021), which can influence their ability to learn from other countries. Therefore, the broader participation of policy actors, including street-level bureaucrats, in all stages of policymaking and policy transfer is crucial, as it enhances preparedness and facilitates the exploration of alternative solutions.
Secondly, findings from this case study suggest that relying solely on top-down policy action may not always lead to successful outcomes of policy transfer, especially in turbulent contexts. Policies adopted at the central government level may not be implemented at the local level due to non-compliance. Non-compliance with transferred policies can arise when policy transfer is used as a quick-fix solution. While these observations may not generalize to all settings, they underscore the need to give careful consideration to potential non-compliance and the potential side effects of the transferred policy in emergency contexts. Moreover, this case highlights the importance of examining the underlying motives and outcomes of non-compliance. Policy non-compliance does not necessarily indicate an intention to defy the will of policymakers; instead, it may be driven by a desire to seek optimal solutions to policy issues. The logic of consequentiality (Nakrošis and Bortkevičiūtė, 2022) plays a significant role in understanding compliance or non-compliance, particularly when professionals are involved in policy implementation.
Thirdly, while barriers to policy transfer in times of crisis are deeply rooted in political and cultural contexts (James, 2023), professional barriers, such as resistance from street-level bureaucrats, also influence the success or failure of policy transfer. It may be beneficial for policymakers to anticipate the possibility of non-compliance, remain open to innovative approaches to policy implementation, and consider timely policy adjustments when there is evidence, however context-specific, that non-compliance may contribute to positive outcomes. During a crisis, the creativity and efforts of local governments and street-level bureaucrats play a significant role in addressing crisis-related issues (Ahmad et al., 2022; Carlitz et al., 2021). In some contexts, non-compliance or alternative approaches by local governments and street-level bureaucrats may enhance outcomes for policy recipients. Although not universally applicable, this highlights the potential benefit of flexible policy design and enforcement to strengthen resilience in emergency management (Radburn et al., 2023) and increase the likelihood of achieving more favourable policy outcomes.
Conclusion
Policy success and failure must be assessed based on the interpretation of the beholders depending on many factors, including their perception, beliefs, and objectives (Fischer, 2003). This perspective can also be applied to evaluating policy transfer success and failure. From the multidimensional view (McConnell, 2010), the transfer of the mother-baby policy during COVID-19 in Vietnam represents a process failure - while the policy was successfully adopted into legislation, its implementation was rejected due to non-compliance. Therefore, the definition of policy transfer success and failure must consider both policy adoption and implementation. Policy implementation should not be treated as “a presupposed residual in goal achievement” because this undermines the significance of ambiguity, conflict, and resistance during this important stage of the policy transfer process (Hupe and Hill, 2016: 103). (Non-)compliance plays a decisive role in determining the success or failure of policy transfer.
While non-compliance with public health measures during COVID-19 can stem from different reasons (Achimescu et al., 2021; Nivette et al., 2021), this research identifies key reasons for non-compliance with the transferred policy: concern for policy outcomes affecting recipients and professionals’ confidence in medical evidence. In this case, non-compliance led to optimal outcomes for both the mother and baby, ensuring the prevention of COVID-19 transmission while also safeguarding their overall well-being. Although a common critique of the policy transfer literature is its lack of “independent reasons for outcomes based on features of transfer processes” (James and Lodge, 2003: 179), this research contributes to a deeper understanding of the relationship between policy transfer and policy success or failure by positioning non-compliance as a decisive factor.
This research offers a perspective that may inform future efforts to reconceptualize the relationship between non-compliance, policy transfer success and failure, and policy outcomes. While non-compliance inherently leads to policy transfer failure - since it contradicts policymakers’ intentions to implement the policy - it does not necessarily result in policy failure. This is because policy success or failure is ultimately determined by the desirability of its outcomes. The assessment of these outcomes depends on for whom they are beneficial and in what context they are evaluated. Accordingly, the proposed framework underscores the necessity of a critical and multidimensional analysis rather than a one-sided assessment in evaluating both policy transfer and policy outcomes.
While there is limited research on policy transfer during COVID-19 that provides an in-depth analysis of policy performance and policy success or failure, this study enhances our understanding of the factors influencing policy transfer success and failure, with non-compliance as a crucial variable. It also highlights the role of street-level bureaucrats in policy transfer and their impact on policy transfer success, failure, and ultimately, policy outcomes. Furthermore, it advocates for the inclusion of contextual factors, motivational drivers, and professional credentials in analysing street-level bureaucrats’ non-compliance in policy implementation. While based on a single case study, this research offers tentative practical implications for practitioners, highlighting the potential importance of considering non-compliance and maintaining flexibility in policy adoption and enforcement, particularly in emergency contexts. The article suggests that using policy transfer as a “quick fix” for emerging issues in turbulent situations should be thoroughly assessed and carefully consulted.
In the context of authoritarian regimes such as Vietnam, policy compliance is strictly enforced, especially with Vietnam’s stringent measures in response to COVID-19. Therefore, this occurrence of non-compliance presents an intriguing case for analysing policy transfer, and policy success and failure, thereby contributing to the existing literature on public policy. However, this research does have certain limitations. As health policies and strategies are closely linked to the competence, trustworthiness, and accountability of governments (Baggott, 2012), non-compliance with health policies can serve as an indicator of political success and failure. This aspect is not analysed in this article and therefore requires further research to provide a solid assessment. Future studies can investigate whether policy non-compliance holds meaning for political goals and the political success and failure of policymaking bodies.
Importantly, a single case study is insufficient to generalize policy non-compliance within similar contexts. The phenomena under investigation, policy non-compliance following transfer and its associated outcomes, are inherently complex, especially in crisis settings that are dynamic and vary across time and space. Therefore, the insights presented here should be viewed as exploratory and illustrative rather than definitive. Alternative explanations, such as institutional implementation challenges, actor-specific preferences, and resource constraints, may also account for observed outcomes. This is particularly relevant in creeping or evolving crises, where compliance patterns can shift. Further comparative, multi-case research is necessary to assess broader applicability.
In conclusion, this case study highlights that during periods of turbulence, governments may turn to rapid policy transfer to address emerging challenges. However, the formal adoption of external policies does not guarantee successful implementation, as non-compliance may arise at the street level. When guided by professional judgment and a pursuit of contextually appropriate solutions, such non-compliance can, in some cases, lead to more desirable outcomes. These findings suggest the need to incorporate non-compliance into analyses of policy transfer, while recognizing the context-specific nature of these dynamics.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.