
Abstract
Values are seen as important in both interorganizational networks and wicked problems. However, in both academia and practice the exact implications of these values remain unclear. In this article we examine the role of values in interorganizational networks dealing with wicked problems, by conducting a case study in a pregnancy and childbirth network. Our analysis identified both actor and network values, three value tensions among actors, and a variety of coping strategies to deal with these tensions. The findings indicate that value differentiation in networks should not be only seen as a problem, but also as an important ingredient for the achievement of network goals. Furthermore, our study revealed functional-structural and cognitive-cultural coping strategies to respond to value tensions among actors, applied by both the network administrative organization and the individual actors in the network. Lastly, we elaborate on the position and skill set of the network leader. We leverage these research results to formulate insights and recommendations for network practice.
Introduction
One of the core features of wicked problems is that entrenched value differences are regularly involved in many problem areas (Rittel and Webber, 1973). In this light, Head and Alford (2015: 713) point out that “many difficult policy problems of the modern era” should be understood as “grounded in competing value frameworks.” Bannink and Trommel (2019: 198–200) argue that the main characteristic of wicked problems is that “they show conflict on the normative dimension next to complexity on the factual dimension.” In other words: “Wicked problems are wicked because the factual and normative aspects of the issues are intertwined at actor-level.” This observation is shared by Vangen and Huxham (2012), who consider that the actors in interorganizational networks responding to wicked problems bring different values to the table, and may be even uncertain about what these actually are. This value differentiation may often occur in these networks, and is particularly relevant in the governance of wicked problems.
Value differentiation is seen as a core attribute of both wicked problems and interorganizational networks, suggesting that more insight into values helps us better understand how interorganizational networks address wicked problems. These insights could help organize more appropriate governance arrangements in these networks. Various efforts to order and analyze the complexity of governance in networks have led to a growing body of knowledge. Several well-known articles provide insight into key features and aspects (Ansell and Gash, 2008; Bryson et al., 2015; Emerson et al., 2012), structures, regimes, partner decision, and modes of governance (Klijn and Koppenjan, 2015; Provan and Kenis, 2008; Van der Heijden, 2022), and the effectiveness of interorganizational governance networks (Kenis and Raab, 2020; Provan and Kenis, 2008; Provan and Milward, 2001; Raab et al., 2015). This has resulted in useful models and typologies, which are used in academia and in practice. However, in the existing literature, there is a lack of information about the exact role and implications of values. When values, and especially value differentiation, are mentioned, different views about how to deal with them exist. Some approaches assume that collaborating actors must reconcile their values or work toward shared values for successful collaboration. Klijn and Koppenjan (2015: 7), for example, state that governance in networks is about “reconciling different values as well as the different actors representing those values.” Ansell and Gash (2008) see the identification of common values as an important step toward a shared understanding in multi-party networks. However, other lines of reasoning do not strive toward the integration of values. Emerson et al. (2012: 14), state that instead of sharing a specific understanding, “mutual understanding” between actors may be more important: “the ability to understand and respect others’ positions and interests even when one might not agree.”
This article attempts to fill that gap by examining the role of values in interorganizational networks dealing with wicked problems, without assuming a priori that shared values are necessary for successful collaboration. We aim to contribute to the existing literature on the network response to wicked problems by introducing an additional perspective focusing on the values and normative considerations of actors in the network. A decentered actor perspective will give us insight into the values, viewpoints, understandings, and perspectives of individual actors in the network. Therefore, it is relevant to investigate possible tensions between these values, and how the actors in the network cope with these tensions (Huxham and Beech, 2003; Van Duijn et al., 2021).
The case study on which this article is built concerns an interorganizational pregnancy and childbirth network that aims to improve quality of care, to tackle the perinatal mortality in the Netherlands, which is very high compared to other European countries (Schölmerich et al., 2014). To improve quality-of-care services, various policies have been implemented to stimulate collaboration between actors and the integration of services (Struijs et al., 2020). These policies aim to tackle a common wicked problem in many countries: fragmentation of care, which is a result of several other issues, such as insufficient alignment of care services, the lack of a shared language, inappropriate governance mechanisms, and hindering policies and payment arrangements. Hence, as with any other wicked problem, it could be seen as a symptom of other problems in the system. Furthermore, it can be an enduring, complex societal problem for which there is no definitive formulation (Head and Alford, 2015; Shaw and Rosen, 2013). Besides the high perinatal mortality, it has many negative implications, such as low patient satisfaction, increasing complexity of the care system, and cost-ineffectiveness. As a response to this, the pregnancy and childbirth network aims to integrate different care services: perinatal, birth, and maternity care.
The objective of this study is to advance the understanding of the role of values in the network response to wicked problems. The main research questions of this study are: (1) What values do the different actors in the network find important? (2) What value tensions arise? (3) How do the actors in the network cope with these value tensions?
Theory
Values play an important role in our everyday behaviors and decisions, but are also abstract and intangible. When looking at the work developed by sociological and psychological theorists, values can be defined as “conceptions of the desirable” (Kluckhohn, 1951) or “standards of preferences” (Rokeach, 2008). As Hitlin and Piliavin (2004) state, values describe a preferred outcome of a particular situation. They can be seen as beliefs that function as moral compasses (Spates, 1983) that form the core of our identity (Hitlin, 2003). Schwartz and Bilsky (1987) made the concept of values more concrete by formulating five core characteristics of values. Values (1) are concepts or beliefs, (2) refer to desirable goals, behaviors, or end states (3) transcend specific situations or objects, (4) are the guiding principles for actions and behaviors, and (5) are ordered by relative importance. In nonprofessionals terms, values are what we see as important and what we want to pursue.
Values theory distinguishes multiple types of values. First, a distinction between individual and supra-individual values can be made. With individual values, the personal values of people are meant (Schwartz, 1992). As mentioned above, a characteristic of values is that they are ordered by relative importance. People may often differ as to things’ relative importance; this is called their personal value hierarchy (Schwartz, 2012). People and groups of people often relate their value hierarchies to their own identity and group membership. For example, friends and co-workers often share values. The construction of these value hierarchies is both determined by personal aspects and internalization. Research shows that age, family background, and sex have an influence on the values of people (Kalleberg and Marsden, 2019). Similarly, experiences related to certain events or professional and cultural development also influence the priority values of people (Suar and Khuntia, 2010). Thus, values develop throughout peoples’ education, careers, and lives. Values theory also mentions so-called supra-individual values, going beyond individual values of people, such as societal and organizational values (Rokeach, 2008). Societal values refer to values that are deeply rooted in societies. For example, individualism, personal freedom, and self-reliance are considered as important in some societies and cultures, while other societies attach less importance to them (Hofstede, 2011). When looking at organizational values, a shared set of values within an organization is often mentioned, displaying the organization’s identity and culture. The importance of aligning individual values of employees with the supra-individual values of an organization is often emphasized in the literature (Sullivan et al., 2001).
Values theory distinguishes terminal and instrumental values. While terminal values are end goals or end states, instrumental values represent modes of behavior by which these goals should be achieved. Terminal values are nouns—for example, safety or sustainability, whereas instrumental values are adjectives—for example, safe or sustainable. Sustainability is an end goal to pursue (terminal), and a process could be organized in a sustainable way (instrumental) (Rokeach, 2008). In this study we look at terminal and instrumental values, because both may play an important in network collaboration.
Values in public policy and interorganizational networks
The concepts of “value” and “values” are gaining greater attention in public policy and administration literature. First, a stream of literature addresses public value. These articles focus on public management and how this may contribute to society (Crosby et al., 2017; Moore, 1995; O’Flynn, 2007). Second, several studies focus on public values, looking at what citizens find important and to what extent there is public consensus about these values (Bozeman, 2007, 2019). Third, many articles about public policy pay attention to conflicting values underpinning policies, value trade-offs, and how to make policy decisions (Meijer and De Jong, 2020; Oldenhof et al., 2014). In this study, we take a decentered actor perspective by focusing on the values of individual actors in a specific context: an interorganizational network.
The interorganizational network context is specific, because different organizations collaborate and often aim to integrate services. We should therefore look more deeply into the role of values in both differentiation and integration in interorganizational networks (Kenis and Raab, 2020). By “differentiation,” we mean the differences between the actors in the network. We define integration as the inclusion of actors within an organizational network to produce a collective output. Raab (1998) distinguishes two categories of differentiation: (1) functional differentiation, defined as the different functions of actors—in other words, the division of labor; and (2) structural differentiation, defined as the different structural positions of actors. In addition to these dimensions, this paper focuses on value differentiation, which can be defined as the different values or value hierarchies of actors (Schwartz, 2012). When looking from a differentiation point of view, interorganizational care networks often consist of a variety of people and organizations with different functions, roles, values, cultures, professional backgrounds, and perceptions (Bardach, 2001; Klijn and Koppenjan, 2015). Examples of participating actors are doctors, care providers, hospitals, governments, and insurers. In a recent study, Zonneveld et al. (2022) demonstrated the extent of value differentiation between actors in care integration.
The literature presents many mechanisms that could enhance integration. Roughly two groups of integrative mechanisms can be distinguished: (1) functional or structural mechanisms of integration, and (2) cognitive–cultural or normative mechanisms of integration (Raab, 1998; Valentijn, 2015). Functional and structural mechanisms of integration refer to connecting actors through structural coordination patterns, such as communication, payments (Stokes et al., 2018; Tsiachristas, 2016), information provision (Kenis and Raab, 2020), information exchange technology (Cameron et al., 2014), organizational ingredients (Minkman, 2012), and governance models (Ansell and Gash, 2008; Emerson et al., 2012). Besides these functional mechanisms, there is a growing attention for cognitive–cultural integration mechanisms based on a common orientation toward values, cultures, goals, and purpose (Valentijn, 2015). These cognitive–cultural integration mechanisms are particularly important in interorganizational care networks, since a formal hierarchy is often absent and top-down steering is often not suitable in these networks (Axelsson and Axelsson, 2009; Raab, 1998).
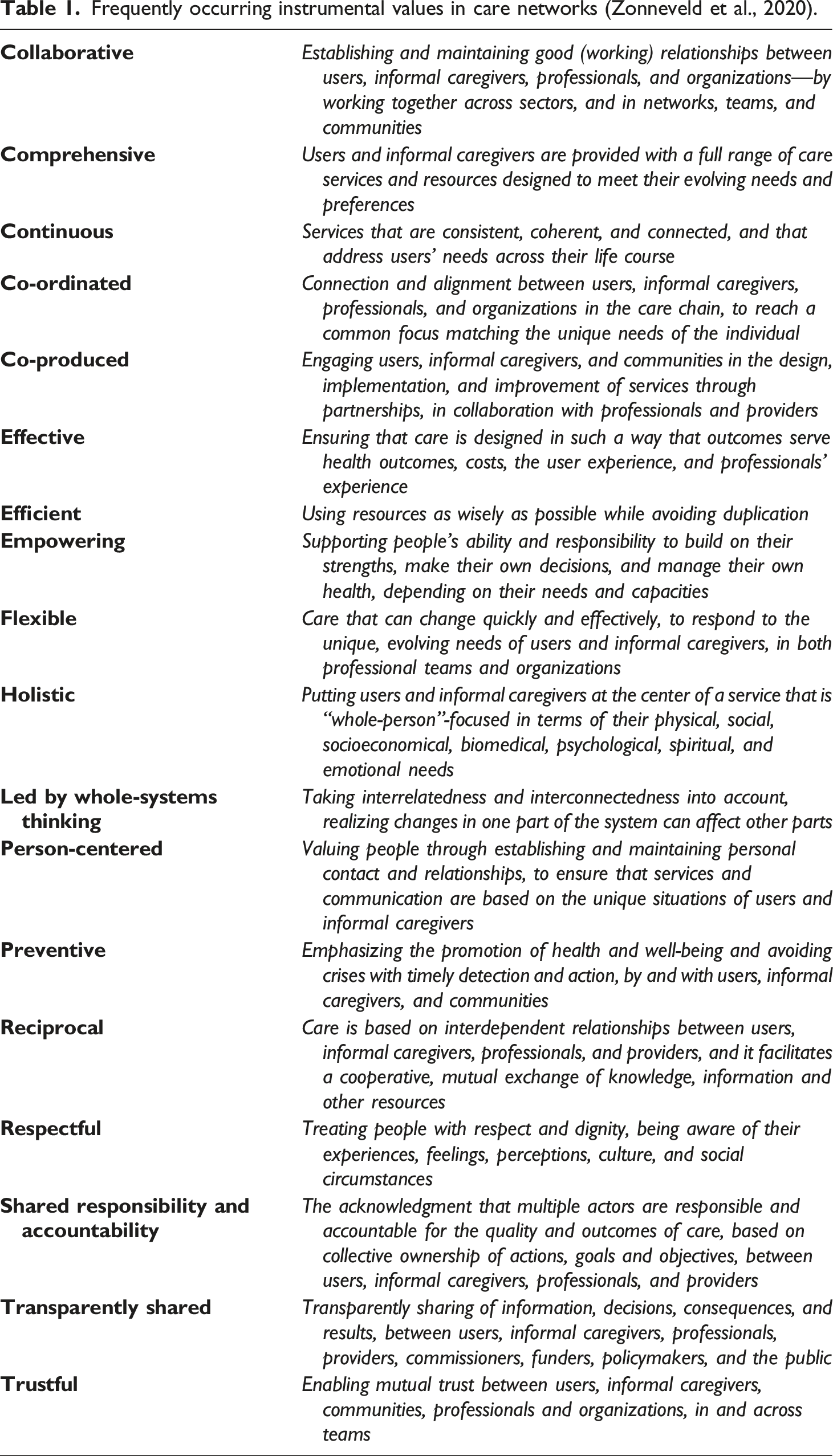
Values associated to care networks
Frequently occurring instrumental values in care networks (Zonneveld et al., 2020).
Application of theory in this study
The concept of values is abstract and intangible, and the definition of values relates to several other concepts such as beliefs, goals, views, and principles. Because these concepts are often intertwined in practice, it is difficult to precisely isolate or separate the concept of values from the other concepts in this study. This is important to consider when interpreting the results of our case study.
Another point to consider is the possible intertwinement of different types of values. In this study, we examine what values network actors find most important (1) as themselves as individual actors in the network, and (2) for the care network as a whole. We must be aware that people develop values throughout their lives, influenced by experiences such as childhood, education, or the organization they work for. Hence, actor values could be a combination of their personal, organizational and network values. It is therefore important to consider that it is difficult to precisely isolate these different types of values from each other.
Methods
Case study and data collection
This article draws on a case study of an interorganizational pregnancy and childbirth network in the Netherlands. Historically, the Netherlands has a higher perinatal mortality than other European countries (Schölmerich et al., 2014). To improve the quality of care, the actors work together in a network pursuing the integration of perinatal, birth, and maternity care services, both in primary care and in the hospital (Struijs et al., 2020). Hence, the case in this study could be seen as a care services network.
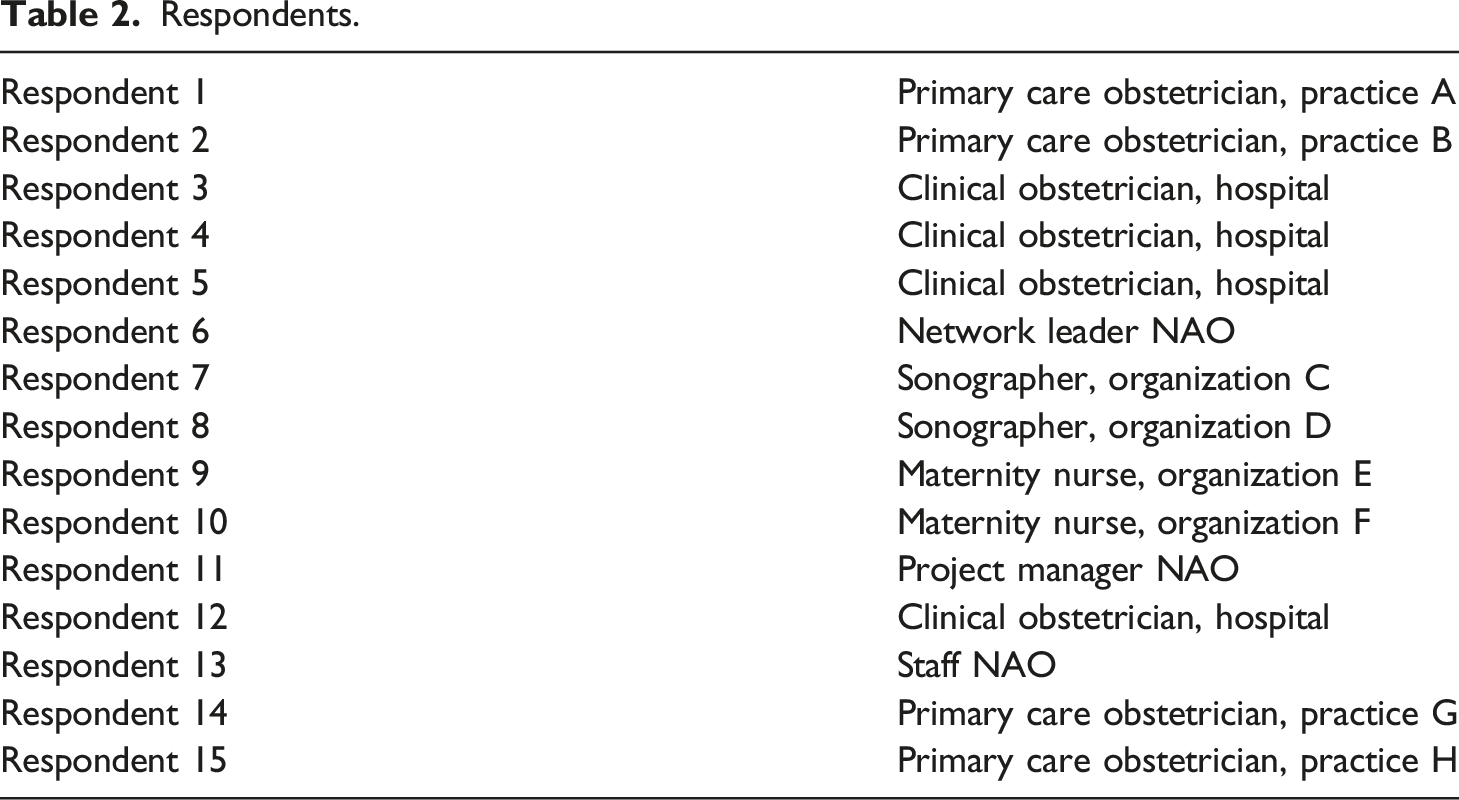
The care network consists of 13 organizations, including a hospital, primary obstetrician practices, maternity care agencies, and ultrasound practices. Several professionals from these different organizations work together in practice. Examples of these professions are medical doctors, nurses, obstetricians, gynecologists, maternity nurses, and sonographers. The collective mission of the collaborating organizations is “putting the (future) pregnant woman, her partner, and the (unborn) child in the center of all services.” The network has also formulated three overarching core values: broad scope on physical, medical, psychical, and social aspects of life (holism); prevention; and empowerment. Recently, the governance form of the network has evolved from shared governance (participant-governed network) to a network–administrative organization network (NAO) (Provan and Kenis, 2008)
Respondents.
Analysis
For the analysis of the data, we followed an abductive approach. All interviews were coded through thematic analysis using MaxQDA software. To ensure quality we have used the systematic data analysis method of Corley and Gioia (2004). As a start, we identified first-order codes (concepts), which reflect the voice of the respondent (Corley and Gioia, 2004). After that, second order codes (themes) were assigned, reflecting the understanding of the researcher. For the second order coding, we used our set of 18 values as a basis (Zonneveld et al., 2020). As a last step, we grouped similar codes into overarching dimensions. The analysis was conducted by one researcher, supervised by three other researchers. Any disagreements were resolved through discussion.
Findings
The analysis of 15 interviews resulted in 357 coded text fragments, of which 301 related to values, tensions and coping strategies, and 56 to contextual information. In this section we present our findings. The coding structure is shown in Figure 1. Coding structure.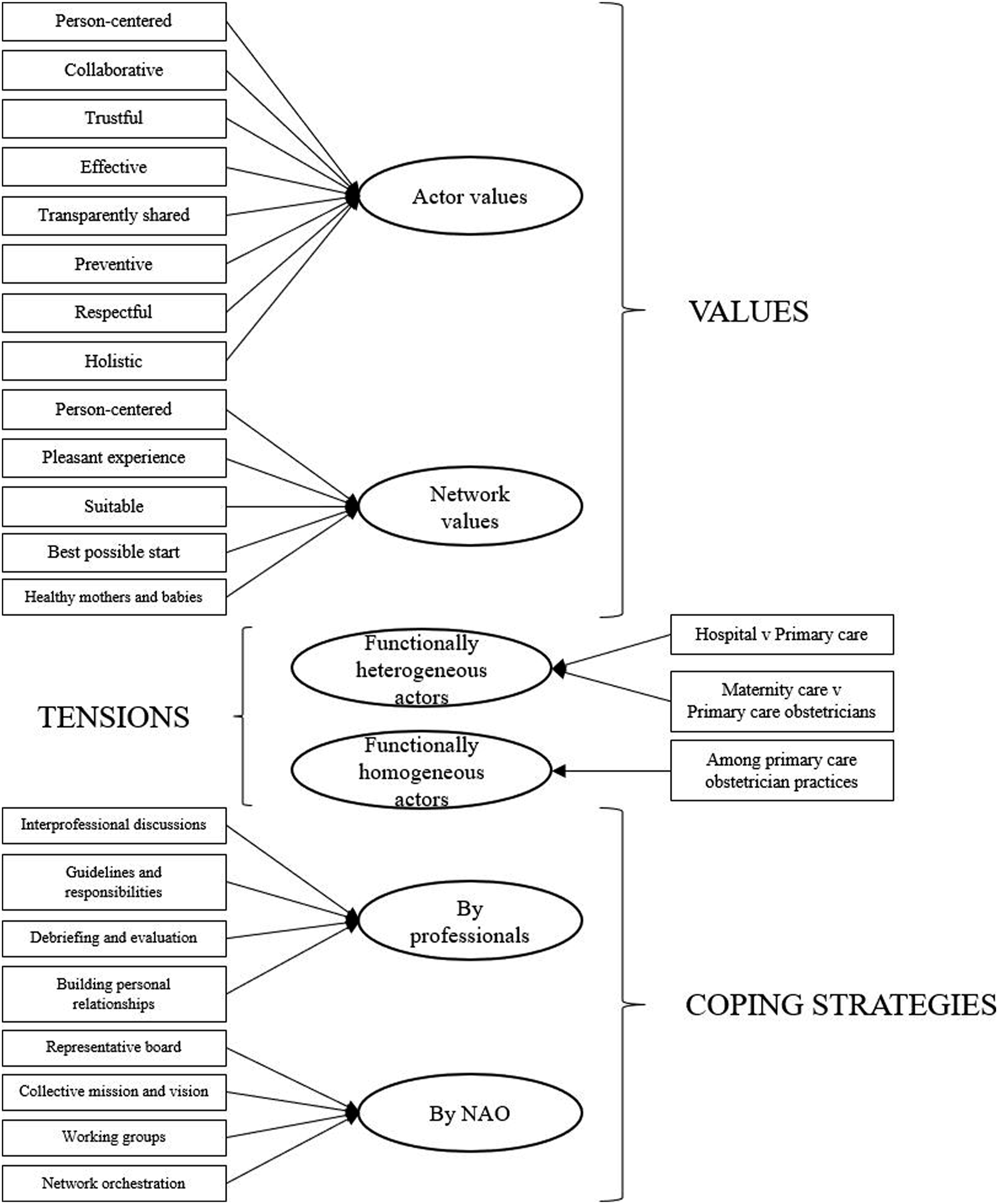
Values
Our analysis revealed (1) values that actors find important as individual professionals, and (2) values that are seen as collective network values by the respondents.
Actor values
When looking at what values respondents find important as an individual professional, several values emerged from the data. First, “For each patient, we have to look what care is needed, and what place is the best for the patient.” ( “I think you should be able to estimate what someone needs and what is going well at that moment. That is the same when I work at someone’s home and I know in advance that there are, for example, mental issues or a challenging history. You must take that into account; you have to be able to engage with that when you talk to people.” (
Second, many respondents indicated that they find “So, from that perspective, we make sure that we collaborate well and that we arrange that together in the best way possible for the customer with their baby.” (
Furthermore, “Referrals have to be done well, you have to trust each other, so yes, that is very important.” (
Especially clinical obstetricians, working in the hospital, found the value “It just must be effective. Chop, chop, chop; that lady has to come for a check-up....I think very much, in that regard, black and white. The care question is: [respondent name], come and help me, because I think this child is in need. Then there is really only one solution: that child must be born.” ( “I don’t like that ECG [heart monitoring], I really want that baby to be born soon.” (
The value “But it is precisely the transparency between such a maternity nurse and such an obstetrician and then finding a good solution together for both parties, that is the most important.” (
A respondent indicates that transparency in the network is also an issue that should be considered as a point of improvement: “Then of course you also sign that we may exchange data with each other for better care. But we still don’t know [referring to a lack of information]. And then they’re like, hello, I’ve discussed all this. Why should I discuss that with you again?....I don’t think this works well between us and the obstetricians.” (
Furthermore, “During pregnancy you also work partly preventive, either to be ahead of things, to inform women.” (
Other respondents also mentioned “I think, above all, whether you like them or not where you’re working at the time, that’s beside the point. You just must always respect each other and be able to discuss and solve that together, so to speak, if there is something. Well, you don’t hear often, but I think you’re in people’s houses, so you must adapt.” (
Finally, “When you work at people’s homes because they have just had a baby, you see the whole picture. You see how the feedings are going, how the nights are going. How’s mother? How’s the baby? All that sort of things. An obstetrician who comes by and is there for ten minutes. She does the checks: is the temperature going well? Those kinds of things. And then that’s it. We see the rest. (
Network values
When asked for the most important collective values in the network, respondents mentioned five overarching themes. First, respondents mentioned “The pregnant woman and her unborn child or now-born child are in the center. Her wishes and needs are in the center.” (
Second, the professionals in the network stated that “We simply want to create the most pleasant experience for them.” (
A respondent emphasized that, although the interpretation may differ among the collaborating actors, a pleasant experience is the shared objective of the collective network: “Of course we all want a client to have a pleasant experience, that she feels heard and that we do what is necessary. Whether this should be done through way A or way B; in the end it comes down to the same. Not everyone will interpret it the same, but I do think that the outcome will be the same—or at least we try it to be the same.” (
Third, respondents mention the most “Sure, I think we all have the goal in mind: to be able to provide the best suitable care for the client.” (
When asked for network value, respondents also mentioned two network objectives, referring to desirable end goals. First, respondents referred broadly to a “Our [the network’s] common goal is caring for mother and child, and the best possible start to a new life.” (
Lastly, “We all have the same end goal, don’t we? Healthy mother, healthy child.” (
Value tensions
Our analysis identified three types of value tension. First, we describe value tensions between functionally heterogeneous actors in the network: between hospital and primary care obstetricians regarding joint births, and between maternity care and primary care obstetricians. After that, we describe a tension between functionally homogeneous actors in the network: the value tensions among different primary care obstetrician practices.
Value tensions between functionally heterogeneous actors
Hospital versus primary care: joint births
A value tension has emerged from the data between the clinical obstetricians working in the hospital on the one hand, and the obstetricians working in primary care on the other hand. In the interviews, clinical obstetricians have a more medically oriented value orientation, focusing on avoiding and excluding medical risks for mother and baby. In technical jargon, this is called “pathology.” Obstetricians working in primary care take a different starting point: having confidence in the human body and a successful natural birth, without medical intervention. This is called focusing on “physiology” in technical jargon. As a primary care obstetrician put it: “What I stand for the most is for monitoring physiology. We are healthy when we are pregnant. Of course, there will be particularities—we will have to look at that, and we will work on that at that time—but the basis is still that we are built for this and that we can do this.” (
This difference in value orientation may have grown because of different experiences during the careers of both clinical and primary obstetricians. A clinical obstetrician stated: “I think as a primary care obstetrician, you work from physiology. So, you always assume that everything will go well, unless....As a clinical obstetrician you usually treat people, pregnant women, or women in maternity with a medical indication. So, there is something pathologic going on: it can be a very mild pathology or it can be a very severe pathology. Because you’re so used to that pathology, I think you’re also more likely to see pathology in physiological deliveries. And vice versa.” (
These tensions are especially reflected when clinical and primary obstetricians work together during a so-called “joint birth.” Although these value differences sometimes may complicate the collaboration, both clinical and primary obstetricians also emphasize the added value of a joint birth. Both professionals have different knowledge, expertise, and a different relationship with the client. The primary care obstetricians, for example, have already developed a deeper relationship with the client A clinical obstetrician stated: “I think two always know more than one. Those patients have known that primary care obstetrician for much longer. She [the primary care obstetrician] has already guided a lot of that birth, and then you join her as a new person....And they sometimes have a different relationship with those people, so that together you can get the best out of such a patient and her partner....We rate the heart film of course, that’s something we do every day and what they see every now and then. And I think they [the primary care obstetricians] guard the physiology a little more now.” (
A primary care obstetrician says: “Studies have simply shown that if a woman is continuously guided, it brings benefits for childbirth, so in that sense it is of course not pleasant if a pregnant woman sees four faces during childbirth. You prefer to have just one or at most two if there is no other option, so that is the advantage of being allowed to do a joint birth [with the clinical obstetrician] and that you could finish something under the supervision of a clinical obstetrician.” (
Maternity care versus primary care obstetricians: an extra pair of eyes
Besides value tensions between obstetricians in primary care and the hospital, the data also revealed a tension between maternity care nurses and primary care obstetricians. Maternity care nurses come into the picture shortly before the birth of a baby. After the child is born, they deliver a maximum of 80 h of care in 10 days. Maternity care nurses have a broad value orientation, taking care at the whole household and social network: father, mother, possible other children, family and other relatives, or friends. Primary care obstetricians only have shorter contact moments with the client and focus on the health of newborns. These differences may sometimes lead to tensions at a home of a client. As a maternity nurse stated: “Because you don’t see each other’s entire picture, it can sometimes differ how you think about it. Those are things that you sometimes think: yes, easy to talk to if you come by for ten minutes, but we are sitting here with a very tired crying mother who is broken, so to speak....For example, some [mothers] are just overtired. Then the obstetrician can say, for example: ‘just go to sleep and skip a feeding.’ While I am are just trying to get it all going....Sometimes that is difficult; if you’ve made a plan and it just gets messed up.” (
Similarly, the respondents acknowledge that these differences may also complement each other. Because of their broad view, maternity nurses form an extra pair of eyes for the primary care obstetricians. As a primary care obstetrician states: “We do not necessarily come to people’s homes, and sometimes maternity care still has information for us even during the pregnancy that we did not know ourselves yet. For example, sometimes maternity care goes on a home visit somewhere and afterwards calls us with, “there are actually very few things there, are you aware of the financial situation?” In fact, they are the first to come into someone’s home situation, and you can get a lot of information from a home situation about the financial resources or hygiene, etc. That’s always very important information for us. And certainly, also during the maternity week they are there all day, of course we visit a few times during the maternity week, but we are there for about half an hour, then we see so much less than the maternity care sees during the day, so no, I wouldn’t know.” (
This was also indicated by a maternity nurse during the interviews: “Well, I think maternity care brings a unique piece, which is that we work behind those people’s front doors for eight days. And there we are with maternity nurses who really use those eyes and ears to see: what do I see and what is happening here? What worries me and what do I share with an obstetrician?” (
Value tensions between functionally homogeneous actors
Different values among primary care obstetrician practices
The last value tension that emerged from the data, is a tension among the different primary care obstetrician practices in the network. Although these practices do the same work in a functional way, they may have different values and visions. These differences may for example relate to the extent of a physiological view. As the network leader stated: “I see a lot of differentiation between practices....For example, [practice X], which really works from a certain physiological view, is very close to the people and takes a lot of time for that. While [practice Y] is really different.” (
As a reason for these differences, the competition between primary care obstetrician practices is mentioned. In contrast to the hospital, for example, primary care obstetrician practices are small businesses owned by independent entrepreneurs. According to a primary care obstetrician, they must differentiate themselves to survive: “You must distinguish yourself as an obstetric practice, so we have a certain vision. I think every obstetric practice has a certain vision of what they think is important, what should work well for a client, but also should work well for her or his team....Yes, people ask for evening consultations. If one does and the other doesn’t, then you may have lost that client.” (
These differences among primary care obstetrician practices may lead to tensions. Collaboration partners, such as the clinical obstetricians in the hospital, must cope with the different values of primary care obstetricians. Some primary care practices have value orientations that are relatively more aligned with the hospital than others. As a clinical obstetrician put it: “Of course there is always a difference in practices, also in their vision, for sure....One moves much more along with the patients, even if they want to receive care outside the guidelines. Some practices are very easy [with moving along], because they believe that all this should be possible, and it is very physiologically oriented. Other practices follow the guidelines a bit more and look more for a compromise with a patient, for example....In every network there are [primary care] obstetrician practices of which I think: what the heck are you doing?” (
Similarly, this differentiation between primary care obstetrician practices is also seen as an asset. Because of their different visions and identity, clients in the region can choose the practice that suits them best. There is a broad and balanced range of primary care obstetrician practices to choose from. As a project manager of the network stated: “Well, the primary care practices are not aligned, let me put it this way. And that’s also a bit of balancing, because that’s not a bad thing, because we don’t want to make it one-size-fits-all. It’s good that all those practices have their own identity and really differ from each other and that they run their own business operations, but the moment that gets in each other’s way because, well, there are different ideas, that makes it a bit difficult.” (
Coping strategies
The analysis identified strategies to cope with value tensions applied by both professionals and the NAO. First, we will elaborate on the strategies applied by professionals. Thereafter, we will present the coping strategies used by the NAO.
Coping strategies by professionals
In their daily work in the network, the professionals apply several coping strategies to deal with value tensions in practice. First, professionals have “During that delivery [joint birth] we had so many discussions: Should we try that for a while? Shall we press on a different attitude for a moment? And then finally that child was born without artificial redemption. And yes, that was really just a nice collaboration.” (
Another example of such interprofessional discussions are exchanges between maternity nurses and primary care obstetricians, as illustrated by this respondent: “We have learned not to let it escalate, but to call each other [the maternity nurses and primary care obstetricians] at an early stage, to inform and discuss: What is going well here, what is going wrong here? What can we do to prevent it from happening again?” (
Besides interprofessional discussions, professionals also apply “There is always a captain on the ship. We do have several situations, a bit of a gray area, in which case the primary care obstetrician can finish the delivery, but I have the final responsibility.” (
Third, after a collaboration such as a joint birth, professionals in the network “What has also been agreed is debriefing after the birth: What went well and what went wrong? And what can we learn from this? That’s how you try to contribute to quality across the network” (
Another respondent also stated that this debriefing and evaluation also contributes to mutual understanding between professionals with different backgrounds: “It is important to briefly discuss, actually debrief, after such a birth: What did I think about it? Because there is not always room to discuss everything next to a patient....It’s really good to discuss that. Then you just understand a little more what the thinking of the other party was, so to speak.” (
Lastly, professionals indicated that they actively “And especially now in [network name], it is clear, you know each other. And we sometimes have meetings [to coordinate], because you know the faces. We’ve just had a great symposium, including social services, so we’re also working on getting to know each other better.” (
It was also stated that a lack of personal relationships may complicate the collaboration: “We work with many practices. And there are a lot of regulars in those practices. But there are also a lot of changing observers....And that’s a tricky one, isn’t it? For example, if I hand over a joint birth and it’s a familiar face to me, I’d rather say: “Please keep me posted. If I can do something…” And if it is an unknown observer to me of whom I do not know how she works, I find it more difficult to just bear the responsibility and not be present in that room.” (
Coping strategies by NAO
Besides the professionals applying coping strategies, the NAO also develops activities to stimulate smooth collaboration between professionals. First, the NAO compiled a board with representatives of each of the disciplines in the work. This “I made sure I had, well, enough flavors on the board....I think we now have a really nice representation of primary care partners.” (
The role of the board members is to ensure support of the different participating organizations. This must result in a broadly supported annual plan with intended activities, the network leader said: “Once we receive what the board members have collected from their organizations and what they consider important for the coming year, we process that into an annual plan.” (
The board also monitors the achievement of these activities and compliance with the agreements that have been made.
Second, the actors agreed on a “Well [our individual visions] became a collective vision, which we also put on paper with each other. We really discussed with the primary care obstetricians, the clinical obstetricians, etc., ‘What is our collective vision concerning birth care?’” (
This mission and vision are communicated in the annual plan by the NAO board members. “We always make an annual plan with the NAO, with a mission and a vision. That is what the members of the NAO board do. They are really very committed to that.” (
The collective mission and vision are underpinned by certain overarching values, related to the needs of the service user, as stated by this respondent: “It is in all our heads: it [the care service] must contribute to the [care of the] pregnant women. That is so ingrained in all of us....It’s a common thread throughout the organization [NAO]” (
Third, within the NAO there are several “There’s the board and later there are working groups such as Care, Quality, and Innovation. Then you have an umbrella working group in which I work. So, the issues that come from the board go to that overarching working group to see who will take care of it....In each group there are one or two representatives per primary care obstetricians, clinical obstetricians in the hospital, gynecologists. Let’s say all those working groups are staffed by all disciplines.” (
Finally, the “It is mainly about being in connection, in listening, in taking it along, in picking it up again and showing each other’s perspectives....I think that’s my role. Show each other the vision and perspective of the other in the conversations....So yes, a chameleon.” (
Besides showing the perspectives of other actors, the network leader also empowers the organizations to take the initiatives, as is illustrated in this example: “I think you are much stronger if you make sure that others always ‘walk with the flowers’ [take the credit]. So that people say, after you have whispered ten times, ‘Maybe this is a good idea,’ say: I have such a good idea.” (
The central position of the network leader between the different actors is also recognized by other professionals in the network, as is stated by a professional: “She [the network leader] is really just the spider in the web; the one with the helicopter view who does not deliver care, but who knows what is going on everywhere. And of course, she has a lot of experience from the other [networks].” (
Discussion and conclusion
In this study, we examined the role of values in the response of an interorganizational care service network to wicked problems. We have identified both instrumental values, referring to modes of behavior, and terminal values, referring to end goals to pursue. We found that particular values such as “person-centered,” “collaborative,” and “trustful” were often seen as important by multiple individual actors in the network. There was less consensus among the individual actors about other values, for example “effective,” “transparently shared,” and “preventive.” No clear hierarchy among these values was found. Subsequently, the respondents mentioned overarching values when asked for the most important collective values for the network as a whole. Only some of these supra-individual network values clearly overlap with frequently mentioned individual values of the respondents, such as “person-centered.” Other network values refer to health outcomes or patient satisfaction. Examples are “healthy mothers and babies” and “a pleasant experience.” These findings demonstrate that, in this case, although actors agree on certain overarching network values, value differentiation does indeed exist and persist.
Our analysis revealed three value tensions among actors in the network. These tensions may complicate the collaboration between the actors in the network. However, each of these tensions also leads to value-creation for the service user, contributing to the overarching goals of the network. First, the value differentiation among obstetrician practices may lead to different ways of working among these practices, making collaboration complex for the other partners. However, this differentiation also leads to a varied range of obstetric practices in the region, with different identities and values. Service users have a broader range of practices from which to choose, which may contribute to more suitable care. Second, although close collaboration between clinical and primary care obstetricians during joint births may lead to value tensions, the values of both professionals are also complementary. While a clinical obstetrician has a pathology-related focus, primary care obstetricians base their work on physiology values and clients’ relationships. Hence, this combination of values may result in greater person-centeredness, which is an overarching network goal. Finally, our study revealed value tensions among maternity care professionals and primary care obstetricians. Again, the values of both professionals are complementary, focusing on different aspects of the family that they are supporting at home. While obstetricians focus on the health of mother and baby, maternity care professionals see the bigger picture of the whole household and social network. The three value tensions identified exist between separate (groups of) actors. This demonstrates value differentiation among actors on a network level (actor–actor). Our findings do not explicitly show value tensions between actors and the network as a whole (actor–network). However, this does not mean that value tensions between individual actors and an alliance of actors or the NAO could not arise on particular topics.
The study findings show that, in this case, value differentiation among actors is needed to pursue overarching network goals. Although value differentiation may lead to tensions in practice, it creates significant value for service users. The representative board of the NAO formulated a shared mission underpinned by a broad frame of overarching values on which each of the partners could agree, leaving enough space for value differentiation among the actors. This suggest that value differentiation in service networks should not only be seen as a problem that must be solved, but also as an important ingredient to achieve network goals. In the network governance literature, the importance of shared or common values among actors is often stressed. Our study adds to this by demonstrating that, besides agreeing on overarching network values, value differentiation among individual actors is needed to add value for service users. Our findings suggest that we do not have to reconcile different values in networks dealing with wicked problems (Klijn and Koppenjan, 2015: 7), but rather let them coexist. Nevertheless, it is crucial to understand and be aware of each other’s values, which is also advocated by Emerson and colleagues (2012: 14).
Understanding that value differentiation could also be seen as an important element, it is relevant to know how to cope with value tensions in practice. Our study uncovered coping strategies to deal with value tensions between actors, applied by both the professionals themselves and the NAO network. These strategies could be distinguished in two categories (1) functional–structural strategies, referring to structural coordination patterns, and (2) cognitive–cultural strategies, referring to a common orientation toward values, culture, and goals.
In the center of Figure 2, in the middle of the four categories, we have positioned “network orchestration,” referring to the role of the network leader. Orchestrational work in networks can be defined as creating value by bringing previously separate activities together through coordination and structuring (Bartelings et al., 2017; Paquin and Howard-Grenville, 2013). In this case, the network leader plays an important role by connecting different activities and actors in the network. The network leaders bridge the gap between the NAO network and the professionals, by for example composing a representative board. The network leader uses both functional–structural and cognitive–cultural strategies to integrate actors and activities. In this light, network orchestration could be seen as both a functional-structural and a cognitive–cultural undertaking. The network leader could be seen as both a function in the NAO network and an individual with cognitive–cultural competencies. These study findings align with the work of O’Leary et al. (2012), who argue that leaders in collaborative networks need interpersonal and group process skills. As O’Leary et al. (2012: s81) state: “People, process, and communication skills are not enough. In addition, successful collaboration requires an individual with an intricate set of relational attributes.” This balance between functional–structural and cognitive–cultural skills on the one hand, and the individual actors and the network as a whole on the other hand, makes network orchestration a complex task, comparable to “walking a tightrope.” Coping strategies.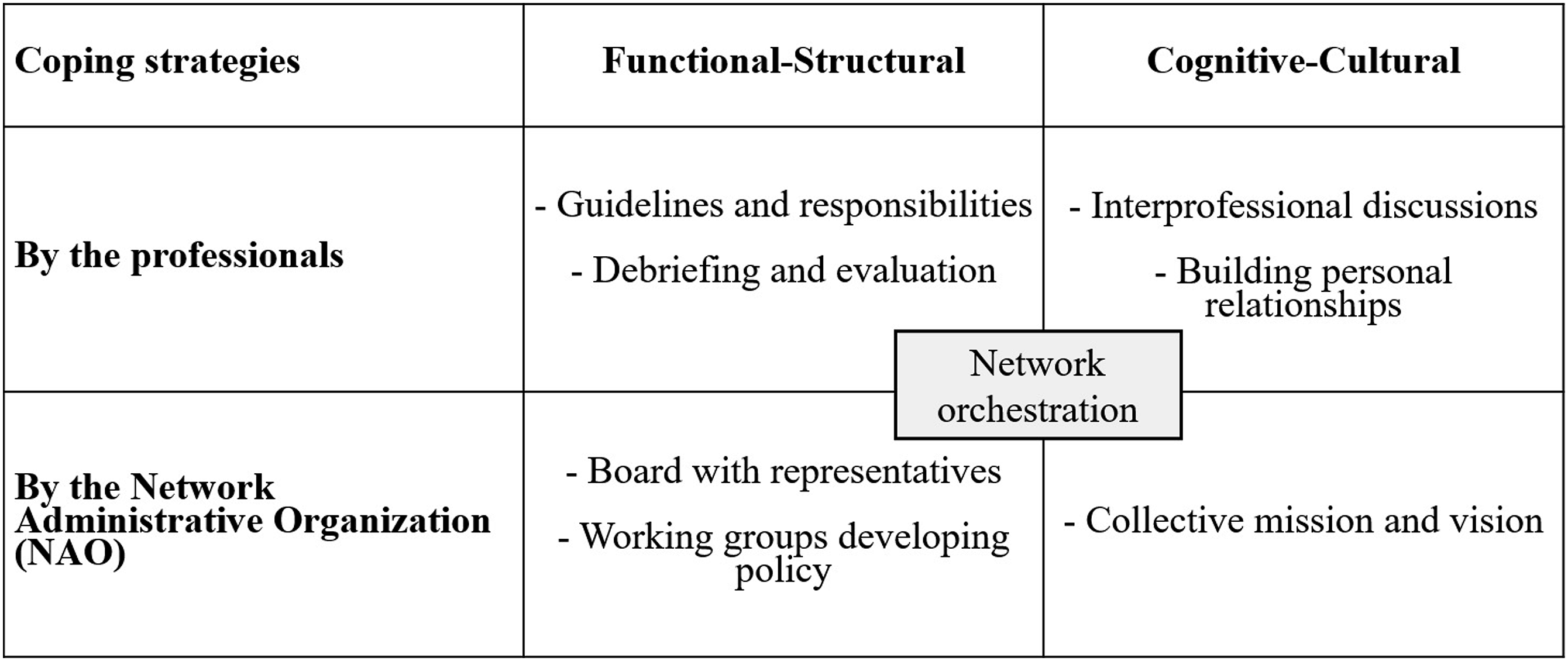
Strengths and limitations
This study illustrates how values play a role in the response of a care network to a wicked problem, why value differentiation is an important attribute in networks instead of only a difficulty, and how the actors cope with value tensions. A strength of this study is its in-depth qualitative research design, which provided rich and detailed information. Second, the analysis has been built on a systematic qualitative method (Corley and Gioia, 2004) and a systematically developed set of values (Zonneveld et al., 2020). These qualitative results add to previous quantitative work on values (Zonneveld et al., 2022). Although the study took place in a specific context, its findings contribute to our understanding of the role of values in networks responding to wicked problems. Acknowledging the limitations of generalizability, its insights in value differentiation in service networks could be relevant to other settings and policy fields.
Practice implications
This study has several implications for practice. First, it implies that value differentiation within a collaborative network should not be seen as a problem only, but also as a vital component of working together in networks—at least, when the appropriate coping strategies are applied. Public professionals need to be aware of this and learn to resist the urge to reduce value differentiation. Methods such as serious gaming, for example, offer the opportunity to experience both the challenges and importance of value differentiation: how can we work together despite our different values? Second, it demonstrates that orchestrational work in networks is all about the balance between making room for value differentiation among actors on the one hand, and connecting actors by applying integration strategies on the other hand. Our study identifies both functional–structural and cognitive–cultural strategies. Finally, the role of values on individual, organizational, and network-level deserve more attention in education and training of public professionals acting in interorganizational networks.
Future research
Multiple recommendations for future research can be made. First, it would be relevant to conduct multiple case studies in care service networks with different objectives, target groups disciplines, other policy contexts, or other value compositions. This may provide information about the influence of these contextual characteristics. For example, what value tensions arise when a network provides services for different target groups? Do less complex target groups need a lower level of value differentiation among professional actors to achieve network goals? Qualitative Comparative Analysis (QCA) could be a promising methodology for the analysis of these multiple cases and may help explain why some cases are successful and others are not. Second, it would be interesting to specifically investigate governance modes in relation to value differentiation. The care network investigated in this case study, transformed from a participant-governed network to an NAO network (Provan and Kenis, 2008). What would the results have looked like if the network still used a shared governance approach, or if it was coordinated by a lead organization? What would be the implications for the coping mechanisms identified?
Footnotes
Acknowledgements
We would like to thank the study respondents for their participation and time.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Vilans, National Centre of Expertise in Long Term Care in The Netherlands.