
Abstract
Much has been written about co-production in mainstream services but less is known about its applicability to service users with severe and multiple disadvantages (SMD). Given the sometimes-precarious relationship between providers and users with SMD, the paper argues that co-production should not be approached in the same way as conventional user engagement because of the degree of marginalisation, stigma and exclusion users with SMD face. Through a thematic analysis of evidence systematically collated via a rapid evidence assessment, the author proposes a co-production framework comprising a series of organisational principles to create an enabling environment for co-production with vulnerable service users. The application of the model is encouraged across a range of sectors and settings so that all service users can become empowered participants in the design and delivery of services that affect their lives.
Introduction
Co-production is situated within the field of citizen participation and public management where collaboration is promoted as a means to enhance service quality (Park, 2020; Brandsen and Honingh, 2015). It has been associated with a range of outcomes, including enhanced effectiveness and efficiency, increased user satisfaction, and improved user–provider relationships (Bovaird and Loeffler, 2013; Alford, 2014). First introduced to policy and academic fields in the 1970s, Ostrom defined co-production as ‘the potential relationships that could exist between the “regular” producer (street-level police officers, schoolteachers, or health workers) and “clients” who want to be transformed into safer, better educated, educated, or healthier persons’ (1996, 1079). Ostrom identified a series of conditions necessary for the promotion and achievement of co-production. These included a synergy between the different contributors where ‘each has something the other needs’ (1996, 1082), options available to both partners, credible commitment based on reciprocal and mutual contributions, and incentives to encourage and enable inputs from officials and citizens.
Inspired by Ostrom, the co-production literature has evolved with a revival of scholarly interest over the last two decades (Bovaird et al., 2019; Sicilia et al., 2019; Osborne et al., 2021; Park, 2020). This interest has primarily been inspired by shifting paradigms of public management that have moved away from New Public Management (NPM) ideologies of the 1980s and 1990s which applied private sector techniques to achieve greater value and efficiency (Hood, 1991). New Public Governance and more recently Public Service Dominant Logic evolved in reaction to the unsuitability of the product dominant, private value logic of earlier paradigms and ushered in a recognition of the increasingly multi-sectoral nature of governance where public services are based on inter-organisational relationships, networks, collaborative partnerships, and other forms of multi-actor policy making and public action (Anttiroiko and Valkama, 2016).
The shifts in ideology towards public value creation have cemented the popularity of co-production amongst the non-profit sector actors, think tanks, and policymakers to enhance the value of public services. Whilst public value remains something of a catch-all phrase for multiple aspirations about public service, its defining features comprise what the public values and, what adds value to the public sphere (Benington, 2011). In the UK, co-production has secured cross-party appeal; first as part of the political discourse under Labour Party control in the early 2000s, and subsequently through the 2010 coalition government’s flagship ‘Big Society’ policy and the Conservative government civil society strategies (Lowndes and Pratchett, 2012). Public servants across a range of service areas have faced a renewed drive to develop co-produced, innovative delivery models triggered by the recognition that publicly desirable outcomes rely on the contributions of multiple stakeholders, not just those of providers. Furthermore, fiscal constraints resulting from the global financial crisis have renewed interest in co-production as a means to compensate for reductions in investment in public services by leveraging civil society resources and capacity (Liddle and Murphy, 2012).
The inclusion of service users has become an integral element of the development and delivery of public services. Advocates argue that co-production is greater than citizen participation and to achieve a truly co-produced service, service users must be involved at all stages of the service planning, commission, implementation, and monitoring cycle (Bovaird and Loeffler, 2013). Several studies refer to the activation of the service users’ untapped or sleeping resources in the co-production process (Palumbo, 2016; Palumbo et al., 2018; Cavallone and Palumbo, 2019). In this manner, the literature conceptualises service users as experts based on their lived experience (Brandsen and Honingh, 2015). The activation of their assets and resources enables them to become valued and valuable partners in public service delivery, rather than being mere consumers of it.
Needham and Carr (2009) emphasised the importance of power-sharing in co-production whereby citizens are afforded real decision-making power. To be genuinely transformative ‘requires a relocation of power and control, through the development of new user-led mechanisms of planning, delivery, management and governance’ (p. 6). Co-operation in these phases has been labelled ‘co-planning’, ‘co-delivery’ and ‘co-monitoring’ (Bovaird and Loeffler, 2013: 1124), and co-production is used in this paper to cover all forms of co-operation, unless otherwise specified.
Turning to service co-production with disadvantaged service users, Ostrom considered co-production as ‘crucial for achieving higher levels of welfare … particularly for those who are poor’ (Ostrom, 1996: 1083). More recent studies have similarly prioritised the urgency of including those who have most at stake and encourage the inclusion of service users with ‘lived experience’ in service design and delivery alongside professionals (Habermehl and Perry, 2021). In this manner, co-production challenges the assumption that service users are passive recipients of care and recognises their contribution to successful service delivery. However, service user involvement requires them to have the resources, skills and capabilities to enable active participation. Research from the health sector exploring the self-management of long-term health conditions identified the skills and capabilities deemed necessary for user engagement in the co-production process. Skills included problem solving, decision making, resource utilisation, developing effective partnerships with providers and acting to make behavioural changes (Wilson, 2001). For those who experience societal disadvantage, the availability of these skills and capabilities may be limited and awakening those sleeping resources will require greater effort and support from providers. Societal disadvantage can refer to a wide-ranging set of concerns across education, health, employment, income, social support, and housing whereby disadvantaged or vulnerable groups are identified according to various socio-economic factors. This paper is focused on a particular conceptualisation that explores the extreme margins of social disadvantage, as this is where there appears to be the most profound evidence gap (Bramley et al., 2015). The paper adopts Bramley et al.’s definition of severe and multiple disadvantage that signifies the complex problems faced by individuals involved in one or more domains of disadvantage (specifically homelessness, substance misuse, offending), where mental ill-health is a common, complicating factor (Bramley et al., 2015: 6).
There is a high degree of stigma attached to people caught up in the homelessness, substance misuse or criminal justice systems (Shelton et al., 2010). This dislocation from societal norms that these intersecting experiences represent serves to push people to the extreme edges of mainstream society (McNaughton, 2009). Wider research evidence shows that often citizens with SMD fall between the gaps in policy and provision and fail to receive the personal and integrated care they need (Fitzpatrick et al., 2013). In these circumstances co-production is likely to be increasingly challenging. Added to this - within public services in the social care field – there is a dominant tradition prioritising service providers as responsible for and accountable to the needs and demands of their communities (Park, 2020). The model has remained provider-driven across many disciplines, with mental health care models in particular criticised for being service-led rather than service-user-led (Thom and Burnside, 2018; Park, 2020). Reviews of the empirical evidence have observed that the term co-production is often absent, with a stronger focus on peer support initiatives (Slay and Stephens, 2013) or on approaches that adopt a paternalistic approach to service user involvement (Bradley, 2015). As such, less is known about how co-production applies, successfully or otherwise, to support those who experience SMD (McNaughton, 2009).
This paper seeks to address that gap by achieving two aims. Firstly, to collate and explore the empirical evidence on co-production as a means to enhance service quality for those experiencing SMD. Secondly to apply that evidence to a propose a framework that can be applied by service providers seeking to develop co-produced models of service delivery with individuals with SMD. The framework contributes to the advancement of knowledge on this topic and its testing and refinement of framework is encouraged in future research studies.
The following section presents the methodological approach. The findings are then presented organised around the core themes identified in the analysis. The discussion highlights the implications for theory and practice and a framework for co-production is proposed for service users with SMD. Limitations of the research are considered with suggestions for future research.
Methodology
The expansion of evidence-based practice has led to an increasing variety of review types (Grant and Booth, 2009; Gough et al., 2012; Varker et al., 2015). The suitability of several approaches was considered in order to select an appropriate method to meet the research aims. For rigour, the review needed to apply a systematic approach and so methods that were less systematic (such as a scoping review) were discounted. A full systematic review of the literature adheres to strict guidelines to ensure transparency but adopts a realist philosophy in the a priori gathering of empirical data to test theories and predefined concepts using what Gough describes as an ‘aggregative’ logic (2012, p. 3). As such the application of this methodology was considered less suited to this study that seeks to generating emerging concepts and theories through a more iterative approach.
A rapid evidence assessment (REA) was selected which combined the principles of a systematic literature review with one that allows a ‘configuring logic’, one that is trying to explore, interpret and understand the world through the arranging of information and developing of concepts (Gough et al., 2012: 3). This enabled the review to be more exploratory and, whilst a general protocol for how the review would be carried out was developed, the detail was allowed to evolve iteratively which enabled different stages to be refined, even repeated to ensure the process remained capable of answering the research question.
Given the multidisciplinary nature of the topic, the search strategy embraced multiple academic databases including IBSS, APA, Scopus, Web of Science and PubMed that were included for their breadth and depth of peer-reviewed literature across the fields of science, technology, medicine, social sciences, and arts and humanities. The database searches used combinations of two groupings of search terms. The primary search applied a narrow focus on co-production with service users with SMD. This followed Bramley et al.’s (2015) domains of severe and multiple disadvantage: homelessness, substance misuse, mental health, and offending behaviours as this particular set of experiences resonates in service users with multiple and complex needs and are likely to facing chronic exclusion (Rosengard et al., 2007; Hampson, 2010). The search employed the terms service co-production OR service co-design OR service co-delivery alongside the Boolean operator AND with the terms complex needs OR homeless* OR mental health OR substance misuse OR offend*. The narrow search string yielded 18 results across the databases. Following an iterative process to meet the aim of developing a framework for providers, a wider search string was applied. This employed the terms service co-production OR service co-design OR service co-delivery to the Title – Abstract which yielded 332 results across the databases.
The titles and authors of each of the 350 studies were scanned for duplication and an initial 152 studies removed. The titles and abstracts of the remaining 198 papers were then screened and a decision to obtain the full text was made according to the inclusion criteria: (1) Context: service co-production. (2) Setting/population focus: service users connected to mental health, offending behaviour, homelessness, and substance misuse services following the Bramley et al. (2015) definition of SMD. (3) Date: the popularity of co-production forms part of wider theoretical developments in public management that adopt a more relational approach to service design and delivery over the last two decades (Osborne, 2006; Anttiroiko and Valkama, 2016). As such the search was restricted to a 20-year period from 2000 onwards to ensure articles reflected this renewed drive. (4) Language: only articles published in English were included to enable replicability of the study and to ensure all the records included in the analysis had an international audience. (5) Source: attention initially focused on international peer-reviewed journal articles, which provided higher levels of reliability to the findings of this study. Only original research and review articles were involved in the analysis; other contributions such as editorials, book chapters and letters to the editor were ignored. Both conceptual and empirical papers were included.
Where the abstract met the criteria, the full paper was retrieved and screened for relevance. Not all the abstracts contained information on all the inclusion criteria (this is a problem with electronic searching). In these cases, a decision was made on whether to include the study based on the information available. In cases of doubt or lack of information, the study was included. In total, 50 of the papers met the inclusion criteria. The full text of the papers was then reviewed which resulted in a further 19 being removed often due to context and population focus issues, leaving 31 to be included in the critical appraisal. Here the quality of the studies was assessed against a set of criteria to identify those of suitable quality and relevance. Gough (2007) points to three main dimensions of in the appraisal of studies: (1) the methodological quality of the study being considered; (2) the appropriateness of that research design for answering the research question(s); and (3) the relevance of the study focus for answering the research question. Drawing on Gough (2007), the researcher developed a framework to make explicit decisions on focus, quality of execution and appropriateness of design. The researcher summarised details in an appraisal table recording details of each study’s: (1) purpose/focus, (2) research design including number of participants/sample size, (3) key findings and summary of conclusions, (4) methodological approach and limitations to assess the strength of the evidence. Seven articles were removed, leaving 24 papers to be included in the research synthesis. The process of selection has been summarised in Figure 1. Flowchart of the research selection strategy. Source: Author’s own.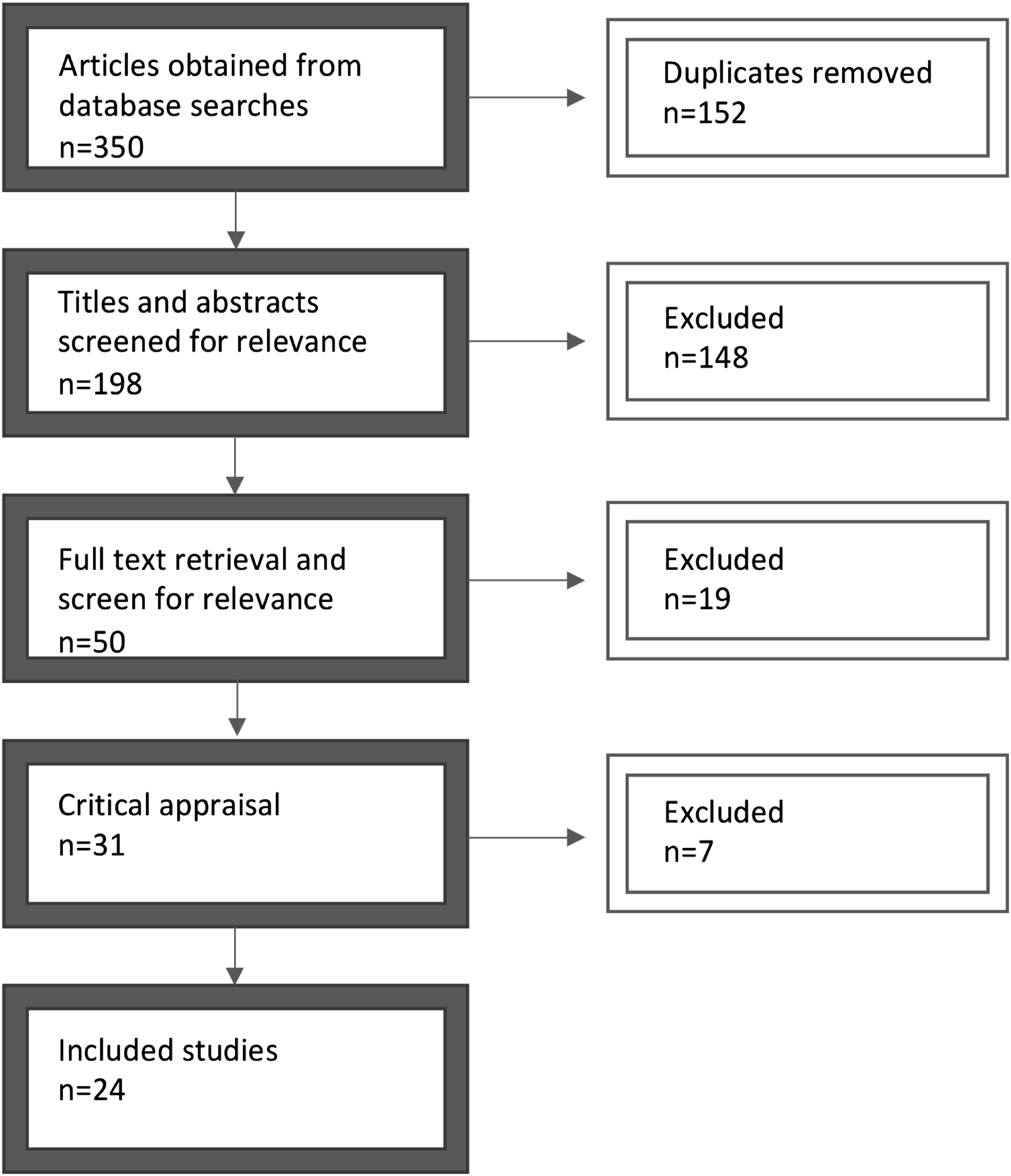
Given the scarcity of papers specific to the research aims, the iterative design enabled purposive sampling to be applied to the evidence synthesis which involved using recommendations, conducting citation forward searches in conjunction with the more traditional database searches.
Synthesis of research evidence
The low number of papers generated by the narrow search string in particular - supported by the findings from the expanded search - demonstrates that co-production with SMD is an under-researched area. The narrow search string revealed a lack of empirical evidence published in peer-reviewed journals on the subject. Of the body of 24 papers initially reviewed, only nine focused specifically on co-production with vulnerable service users including those with SMD of which six related to mental health services. The wider studies included in the review were situated in the context of public service co-production (11 papers) including community development projects, and education initiatives; and public health co-production (four papers) where it was felt transferable lessons might lie.
To meet the aim of developing a framework for service co-production with users with SMD, the review sought to identify crucial factors from the evidence base that enabled or hindered service co-production. The analysis involved the organisation and coding of papers using thematic analysis whereby themes were coded under a series of macro headings. The narrative that follows is organised following these four themes: motivation; trust and empowerment; organisational structure and culture; and staff as catalyst and change agents. Given that most papers reviewed took a wider focus, the discussion also considers how these themes apply or otherwise to the context of working alongside service users with SMD.
Motivation
Co-production relies on the individual’s motivation to take part in the process; a service user’s readiness to accept a more engaged role in the relationship with the professional is imperative. Graffigna et al.’s (2020) research on co-production with those recovering from mental ill health identifies that the service user needs to have a level of resilience with the clinical condition to develop the motivation, skills, and competence to change their behaviours and attitudes toward their life. For those with SMD, mental ill health will feature alongside other challenging needs related to their offending behaviour, homelessness and substance misuse. This combination is likely to comprise a set of mutually reinforcing causal inter-relationships that serve to push people to the extreme edges of mainstream society (Bramley et al., 2015). In this context, the resilience, or capacity of these individuals to overcome adversity, and thrive despite their challenges and trauma are likely to be lower (Luthar et al., 2000) and there will likely be a lack of motivation to engage in service provision at all, let alone in co-production. As such, a consideration of the factors that motivate individuals to engage in co-production in order to identify ways to encourage disengaged users is necessary.
It is commonly assumed that engagement is driven by material self-interest. Inspired by public choice theory, Verschuere et al.’s (2012) review of co-production of public services regarded people as “benefit maximisers who will only co-produce when benefits outweigh costs” (p.1087). This self-interest implies co-production is extrinsically motivated and enabled through tangible rewards. Others encourage a focus on intrinsic rewards and observe that when co-production results from extrinsic motivations, such as material rewards or even the fear of sanctions, it is less likely to lead to outcomes such as self-efficacy (Bradley, 2015; Fledderus, 2015; Farooqi, 2016). Alford (2014) emphasises that service providers should direct users’ attention to what co-production can offer them. By heightening the benefits that they will receive from the service, the model taps into other motivations such as personal achievement, growth, or a sense of accomplishment.
Cavallone and Palumbo’s (2019) review of co-production of community projects warns that citizens can bring selfish motivations when they engage in public service co-production, and this could result in what Palumbo and Manna (2018) describe as co-destruction where the process has negative outcome. Staff may also act out of self-interest and be unwilling to engage users in the co-production of services. This reluctance may be the result of their desire to maintain control over the dynamics of service delivery, or the consequence of their limited confidence in the citizens’ contribution to the process.
Motivation to engage will be more challenging for service users with SMD who are marginalised by society. Barriers to participant engagement, such as the lack of awareness, accessibility and acceptability, are likely to disproportionately affect disadvantaged and vulnerable people who are faced with multiple adversities and complex needs (Bramley et al., 2015). As such, providers looking to engage vulnerable users in co-production will need to tailor strategies for motivating user engagement to overcome these additional barriers.
One option is to start with individual co-produced activities. Bovaird et al.’s (2016) research exploring co-production through citizen panels supports this idea. They found an apparent difference in motivation levels depending on whether co-production was a collective or individual effort. Citizens were more motivated to engage when the actions involved were relatively easy and could be carried out individually rather than in groups. Collective co-production was dependent on the efforts of fellow users which added greater complexity to the process and impacted on the attainment of user outcomes.
For service users with SMD, consideration of the ease of getting involved in co-production is needed. Reflection on the particular barriers these individuals face and consideration of the activities they will participate in will be essential. Providers also need to identify the importance of the service to the users and convey the value or benefit co-production will bring.
Trust and empowerment
The review found that engagement in co-production is reliant on the users’ external efficacy – that is their trust in the provider to offer meaningful opportunities for engagement, and their internal efficacy - or perception of their personal competences and resources (Alford, 2014; Farooqi, 2016; Van Eijk and Steen, 2016). The greater the level of trust, the more likely they are to cooperate and engage in co-production (Ostrom, 2014). The findings of the review, however, highlight that the establishment of trust is problematic within services that support marginalised groups including those with SMD (Bramley et al., 2015; Strokosch and Osborne, 2016). Service users experience mistrust that may stem from previous poor experiences or negative perceptions of public service providers. Engagement in co-production should therefore be situated in the context of the service user’s broader experiences of engaging with services recognising that these may not have been positive. Establishing trust between provider and service user was identified as crucial to building initial relationships. Strokosch and Osborne refer to an initial ‘moment of truth’ when the service user first engages that offers a crucial opportunity to build trust (2016: 687).
Similarly, staff distrust in co-production can stem from previous experience of service user engagement. Service users’ lack of commitment to plans or rules can result in a disregard of their claims or ideas (Park, 2020). Bradley’s (2015) review of carers and co-production found that mental health professionals were persistently criticised for not adequately involving service users and carers in care planning. Mental health workers were often unwilling to trust the views and preferences of patients, particularly in relation to their treatment preferences. As a result, users often perceived such approaches as stigmatising, manipulative and coercive.
This results in a power imbalance between service provider and user which inhibits co-production. As such, the sharing or redistribution of power and responsibility offers a means to build trust. The review identified a disconnect between theory and reality. In his conceptual paper, Park (2020) highlights examples from health and social care where staff hold primary decision-making authority as they attend to the complex problems of service users, who are often stigmatised. He argues that in this relationship there is a danger of user inclusion becoming a tokenised practice with little substantive collaboration. As a result, scholars have expressed concern that co-production can simply become another form of paternalism that restricts service users’ autonomy by offering nominal user engagement opportunities to legitimatise provider-driven solutions (Brudney and Lantos, 2011).
Thom and Burnside’s (2018) review of power sharing through co-production in New Zealand’s criminal justice system illustrates this point. The qualitative study focused on examining offenders’ understanding and actualisation of co-production and found co-production was often seen as a tick-box exercise where the power structures of the prison would never truly allow for co-production within the overwhelming ethos of control and punishment. There was no real opportunity given to prisoners in this study to influence planning or evaluation within or beyond their sentence.
Palumbo’s (2016) review identified information asymmetry as a barrier to trust in health care co-production. Health professionals having more, or better information prevented information exchange between providers and users and, as a result, undermined mutual understanding between the health care professionals and the patients, resulting in the discouragement of patients to engage.
Several of the studies that focused on citizens with lived experience provided some insight into how trust could be fostered to address the power imbalance. Strokosch and Osborne’s (2016) empirical study of asylum seekers in Glasgow suggested that allowing service users to shape their own services was dependent upon the development of a close but professional relationship between user and provider. They observed that this worked best when the asylum seekers were viewed as “experts in their own lives, with valuable knowledge and experience … and therefore, in a position to make important service contributions” (Strokosch and Osborne, 2016: 684). Channelling the knowledge and resources of the service users could be challenging and was dependent on a continuous and equal dialogue between the service user and provider. The COCO framework developed by Graffigna et al. (2020) offers a valuable tool to monitor the extent to which patients, together with other stakeholders, are involved in co-productive processes in mental health to address the power imbalance.
Following earlier points on motivation, the engagement of service users initially in individual co-production appears to build trust as users develop an increased perception of control and influence over the service. In their study of work-integration programmes for young people not in education, employment, or training (NEET), Hazenberg et al. (2014) identified the creation of a supportive and structured environment as vital to the success in assisting NEET individuals. The allocation of a coach was seen as important in developing trust, as was jointly agreeing a structured programme. When undertaking collective co-production, Aiken and Bode’s study (2009) of back-to-work programmes to support socially excluded people found that joint interests and common backgrounds between the groups of service users led to higher levels of trust and engagement; for example being from the same neighbourhood or having the same socio-economic status.
Organisational structure and culture
The review highlighted that developing supportive organisational structures and culture were key enablers for managing effective co-production (Bovaird and Loeffler, 2013; Alford, 2014). According to Jaworski and Kohli (1993, as cited in Alford, 2014), organisational structures should be characterised by low centralisation and high connectedness. Bauer et al. (2019) similarly found flat organisational hierarchies were a key factor in creating effective co-production processes in mental health recovery programmes. Fledderus (2015) also recognised that managers who were personally involved with activities with users and whose leadership style was less hierarchical were more able to create the feeling of reciprocity among service users that is essential to co-production. Flat organisational hierarchies appear to encourage greater focus on building relationships with service users which is essential for trust building in co-production. They also afford staff at lower levels of the organisation greater autonomy in decision-making, empowering them to make judgements on the spot and coordinate appropriate responses to service users’ needs. These are all essential components of working with service users with SMD to engender trust and address the power imbalance.
Another supporting factor of co-production was an organisational culture that valued user engagement as an integral part of the service. At the strategic level, this required staff to have adequate levels of autonomy and resources to devise appropriate strategies aimed at engaging service users (Gill et al., 2011). Studies have found that in embracing this culture, the organisation provides a protected niche for the development and implementation of new ideas generated through the co-production process. In Farmer et al.’s study (2017, 2018) for example, the rural community health initiative had strategic buy-in, alongside human and financial resources which allowed experimentation to occur in relatively unthreatened and stable circumstances.
Echoing earlier observations, the adoption of co-production is often dependent on the disposition of service managers and front-line staff towards the concept. Farooqi’s (2016) study exploring community co-production initiatives in Pakistan found that a change in attitude and acceptance towards co-production amongst staff was responsible for wider institutional changes. These included structural and resource changes to create mechanisms that encouraged the involvement of local communities in service co-production. Aiken and Bode’s (2009) research on back-to-work programmes in Germany and the UK notes that non-profit organisations are often better placed to foster a culture of co-production and service user engagement because of their focus on social goals. Bauer et al.’s (2019) research exploring the characteristics of effective recovery-orientated mental health initiatives similarly identifies strong social value and process rather than performance orientation as essential characteristics, a view endorsed further by Strokosch and Osborne’s (2016) paper on asylum seekers in Glasgow. This is significant in the context of supporting people with SMD where service provision is often delivered by non-profit organisations who embrace social value.
On a related point, the findings of the review offer caution against the adoption of managerialist structures and cultures in the sector that risks converting non-profit organisations into performance orientated, “just in time” deliverers of poor programme outcomes. Eikenberry and Kluver’s (2004) article on marketisation in the non-profit sector explain that a focus on efficiency and achieving value for money has meant that those organisations contracted to deliver public services have been pressured to reduce costly activities that do not add measurable economic value. Park’s study (2020) on patient-centred care similarly recognised the impact of bureaucratisation on co-production. Dependence on external funding incentivises service organisations to adjust their priorities to correspond to funders’ preferences which might reduce their focus on the views of service users and wider community members.
Staff as catalyst and change agents
The research clearly shows that staff play an integral role within organisations seeking to adopt a co-production model. Farmer et al.’s (2017, 2018) exploration of community health services found a supportive policy and practice environment to be crucial to the development and implementation of co-production. They suggested that to gain acceptance, co-produced ideas and innovations must negotiate a political as well as practice-based landscape. Dominant political interests tended to resist change inspired by others, and co-produced innovations diffused only when they were considered compatible with the prevailing regime. In this context, staff played a critical role as agents of change. Acting as boundary spanners, they were able to connect people within and outside their organisation to ensure co-produced ideas were progressed. Staff re-interpreted and promoted new ideas to fit the language and direction of the existing regime so that the initiatives were regarded as desirable. Palumbo and Manna’s (2018) exploration of co-production in health care similarly identifies staff as key facilitators of co-production. When interacting with patients, health care professionals played two complementary roles. Firstly, they were patient enablers who encouraged the engagement of patients in the provision of care; secondly, as patient catalysts, they stimulated the patient’s enthusiasm to be involved in their care provision.
In the context of service users with SMD, the findings imply that co-production is not something that anyone can facilitate and sustain. To act as change agents, staff need training and support to develop the range of skills and knowledge required to build and sustain these relationships with complex service users and other providers. This will include guidance on developing a trusting environment, and tools for engaging and empowering service users to contribute and share their experiences.
Discussion: Implications for theory and practice
With its roots in public choice theory and appeals to self-help (Ostrom and Ostrom, 1971), co-production is still regarded as an innovative approach to public service provision. The focus on communities as a source of ideas and action echoes a trend in social theory that emphasises dispersed agency over centralised social structures (Eversole, 2011). This paper had two aims: (1) to explore the empirical evidence on service co-production as it applies to those experiencing SMD and (2) to use that knowledge to propose a framework to support providers seeking to develop such an approach with service users with complex needs.
On the first aim, the review demonstrates that while scholars have widely discussed the theoretical and conceptual building blocks of public service co-production, there is a lack of empirical, peer-reviewed studies that have focused on its application to those with more complex needs. Studies that do exist tend to be conceptual with a lack of comparative, empirical evidence comparing different sites or service types. To address the second aim, the search terms were widened to capture a broader body of relevant materials on co-production. The wider evidence advocates for an asset-based approach where the service users’ resources are valued and combined with those of the service provider to enhance service quality and outcomes thus achieving greater public value. However, the findings of the review found little mention of an asset-based approach. Rather than being considered as valuable assets in an approach that encourages dispersed agency over hierarchical structures, the review found that service users continue to experience a ‘provider knows best’ approach with attempts to engage service users restricted by organisational structure, culture and poor staff buy-in. This results in a tokenistic and paternalistic adoption of co-production principles and a model that remains provider-driven rather than user-led (Thom and Burnside, 2018; Park, 2020).
For those with complex needs, the theoretical paradigm has not swung far from the traditional dependency culture produced by the welfare state. Strokosch and Osborne (2020) debated the reasons for the failure of active citizen participation in service delivery and highlighted the linear nature of service production models to be partly to blame. These models routinely cast public service providers in the role of design and delivery and service users as service consumers. For service users with SMD, co-production needs a rethink in recognition that these groups of citizens will be distinguishable from those experiencing other forms of social disadvantage because of the degree of stigma and dislocation from societal norms that their intersecting experiences represent. The association with perceived behavioural ‘deviance’ or ‘transgression’ (Fitzpatrick and Stephens, 2014), means that a particularly high degree of stigma is attached to people caught up in the homelessness, substance misuse or criminal justice systems (Bramley et al., 2015). This serves to push people to the extreme edges of mainstream society; as such they tend to be underrepresented in services and less likely to engage in interventions (McNaughton, 2009).
A thematic analysis identified four macro factors that underpin the co-production process, and these have been considered specifically from the perspective of working with service users with SMD. The analysis reveals there will be additional barriers and challenges to surmount to ensure these service users are included in the process of co-production. Given the sometimes-precarious relationship between providers and users with SMD, the application of co-production needs to be applied more sensitively to ensure users are not coerced into the process or disengaged further by it. Co-production should not be approached in the same way as conventional user engagement because of the degree of marginalisation, stigma and exclusion users with SMD face.
To encourage the move away from a linear, consumer centric model that is failing service users with SMD, the factors identified in the review have been synthesised into a framework that depicts a circular, inclusive co-produced approach to supporting those with complex needs. The framework (see Figure 2) provides a major contribution to bridge the gap in knowledge on the empowerment and engagement of the most vulnerable citizens in service co-production. A framework for complex needs co-production. Source: Author’s own.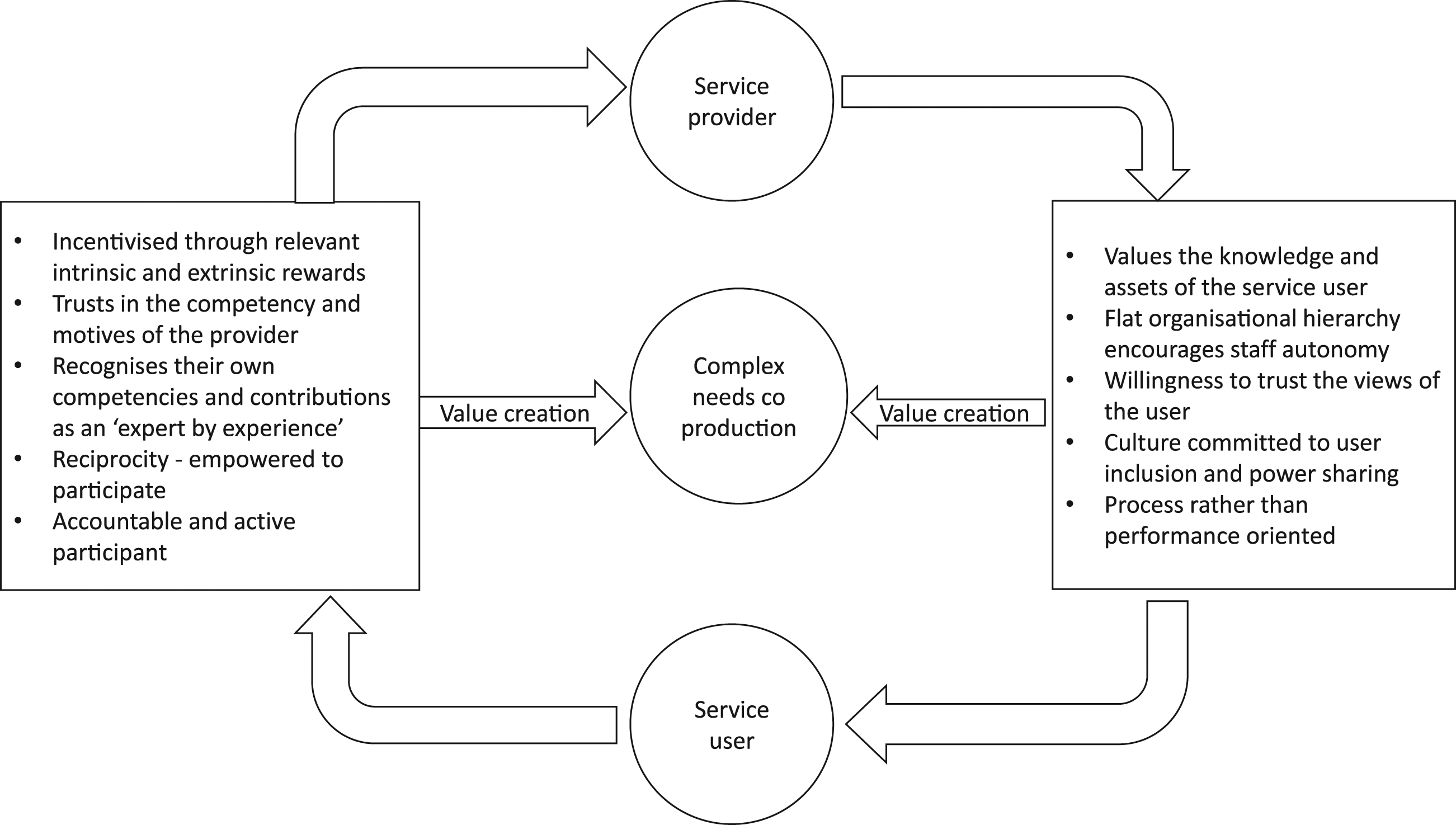
The framework depicts the enabling environment that underpins a shared and meaningful approach to co-production. The model can be applied as a series of operating principles aimed at supporting service providers to make the shift towards embedding co-production within their service to empower users with SMD to influence the health and social services upon which they heavily depend.
The adoption of the framework by professionals working with service users with SMD is encouraged and it can be applied in a variety of ways. Across the organisation, staff could be asked to evaluate current practice against each of the principles to identify areas of a good practice and explore areas for development. The ‘provider enablers’ on the right of the framework could form part of a joint exercise involving staff and service users to gauge how the organisation is perceived. The findings could then inform the co-design of approaches that activate and value the knowledge and resources of the service users. Consideration of how users’ voices are heard and represented with the organisational hierarchy will help to address power imbalances.
Similarly, staff and users can apply the ‘service user enablers’ on the left of the framework to reflect on how current policies and procedures incentivize the engagement of service users in co-production. Developing a greater understanding amongst staff of the impact of trauma and adversity faced by users with SMD will be key to unlocking methods to motivate individuals to engage in co-production. Building trust slowly and jointly finding ways to enable service users to contribute meaningfully to decisions that affect their lives through regular support sessions will engender a sense of reciprocity and empowerment amongst users.
Despite its contributions, there are some limitations to the reliability of this study that should be noted. Although multiple citation databases were used to conduct the review, there is the potential that literature not catalogued on the databases will have been missed. The subject matter of this REA also means that the literature is dispersed through many academic fields making it harder to search for and review literature from so many different disciplines. The search criteria used to collect relevant articles will have impacted the breadth of the research strategy. This was deliberate to maintain the focus of the review and ensure articles were relevant to the topic, but the inclusion of alternative terms may return different results. Future studies might incorporate other approaches to community-driven development such as asset-based community development in the search strategy which would widen understanding of the application of these approach to co-production. In a REA, the quality assurance of evidence is carried out by a single researcher compared with a systematic review in which evidence will be assessed by two or more researchers who come to a consensus on the strength of the evidence presented in each study: this could increase the reliability of the findings. To mitigate any bias in selection, an objective and easily replicable research design was applied.
Conclusion
Service design for vulnerable users has been identified as a key area for development in public management and co-production offers a means to enhance quality. The majority of studies on co-production focus on mainstream service users and fail to consider how the process might work with citizens with SMD who are often stigmatised and dislocated from societal norms. This paper achieves two aims. A thorough assessment of the evidence on service co-production involving those experiencing SMD discovered a lack of empirical evidence. Given the degree of marginalisation and exclusion they face, the study argues that co-production with complex service users should not be approached in the same way as mainstream user engagement processes and highlights the need for greater empirical research to identify the differences from generic service user engagement in co-production.
Drawing on an expanded knowledge base to achieve the second aim, the paper summarises a series of factors that provide valuable, insightful and helpful lessons on the potential benefits and pitfalls of co-production with extremely marginalised service users. This framework is offered as a tool for service providers looking for new approaches. Its application and testing are encouraged across a range of different services that support citizens with SMD including those in the housing, substance misuse and criminal justice sectors where the review found a lack of empirical evidence. Given the identification of a culture founded on social values as an enabling factor and concerns of the marketisation of public services, it would also be useful to compare its application in different provider settings notably contrasting voluntary sector with local authority provision.
Through these refinements, based on empirical application, the framework can empower complex service users to become experts in their own circumstances. It is hoped that will shift the paradigm from a paternalistic, linear approach that promotes dependency towards one that recognises the traumatic life experiences of those with SMD and adapts co-production to engender a joint responsibility for the improvement of their health and life outcomes.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article. The research underpinning the paper received some funding from The Y, Leicester, a charity supporting young homeless people. They had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.